
Abstract
This study evaluated the role of psychiatric morbidity in relation to a history of suicidal behavior, with a particular focus on attention-deficit/hyperactivity disorder (ADHD). Suicidality and psychiatric diagnoses were assessed in 370 incarcerated male juvenile delinquents from Northern Russia using the semi-structured K-SADS-PL psychiatric interview. A lifetime history of suicidal ideation only (24.7 %) and suicidal ideation with suicide attempts (15.7 %) was common. Binary logistic regression analysis was used to assess the role of ADHD and other psychiatric disorders in suicidal ideation and suicide attempts. A history of suicidal ideation and of suicide attempts were associated with higher rates of psychiatric morbidity and with the number of comorbid psychiatric disorders. An ADHD diagnosis was associated with an increased risk for both suicidal ideation and for suicide attempts. The comorbidity of ADHD with drug dependence further increased the risk for suicidal ideation, while ADHD and alcohol dependence comorbidity increased the risk for suicide attempts. Our findings highlight the importance of adequately detecting and treating psychiatric disorders in vulnerable youths, especially when they are comorbid with ADHD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Suicide is the third leading cause of death in youth [1]. Despite its public health and clinical importance, the prediction of suicidal behavior in adolescents still poses substantial clinical difficulty for mental health professionals [2]. The challenge for effective suicide prevention is to identify the most vulnerable individuals and the circumstances that represent an increased risk for suicidal behavior, and then to intervene effectively [3]. From this perspective, mental health problems and institutional placement have long been considered as major risk factors for suicidal behavior. Considering that suicide is often the most common cause of death in correctional settings [3], delinquent adolescents constitute a highly vulnerable population, with the prevalence of lifetime suicidal ideation in delinquent youth ranging from 16.9 to 59 % [4], while the suicide rate for incarcerated youth is 3–18 times higher than in the age-matched general population [5, 6]. However, as the individuals in prisons and correctional facilities often share characteristics that traditionally represent a higher risk for suicide, such as being young and male, having mental health problems and substance use disorders, as well as being socially isolated and disenfranchised [3], many characteristics of suicidal delinquents may also be shared by non-suicidal inmates. It is therefore crucial to identify the specific factors that can distinguish those at risk for suicide from the non-suicidal in these settings. Previous US studies of delinquent youth [7–9] have linked suicidal behavior to serious mental health problems, such as depression, posttraumatic stress disorder and substance abuse [e.g. 4].
Although research on the association between attention-deficit/hyperactivity disorder (ADHD) and suicidal behavior among delinquent youth has been somewhat limited to date, there is some evidence that ADHD symptoms might also be associated with an increased risk for suicidal behavior among incarcerated youths [e.g. 10, 11]. Moreover, the results from these studies concur with those among youth in the general population which have clearly demonstrated that ADHD may represent one of the major mental health risk factors for suicidal behavior [12, 13]. Prospective research on children with ADHD has shown for example, that the disorder is associated with an increased risk for suicidal ideation, attempts and completed suicide by young adulthood [14–16], while population-based research among adults has indicated that the comorbidity of ADHD with other psychiatric disorders may provide an additional and substantial risk for suicide [17]. In contrast, other research has suggested that the association between ADHD and suicidal behavior may be fully mediated by other psychiatric disorders [18]. Hence, it remains unclear whether ADHD constitutes an independent and additional risk for suicide after controlling for comorbidity or whether certain combinations of ADHD with other psychiatric disorders may represent a potential risk for suicide.
The purpose of the present study was to evaluate what types of psychiatric disorders are associated with suicidal ideation and suicide attempts in a group of Russian male juvenile delinquents. Previous research has demonstrated that the prevalence of psychiatric disorders in Russian juvenile delinquents tends to be similar to that in other countries and is substantially higher than that observed in the general population (see for example [19]). In addition, considering the comparative lack of research about the role of ADHD and its comorbidity for suicide, the study also aimed to determine whether a diagnosis of ADHD in this group constitutes an additional risk factor for suicidal behavior, over and above the risks posed by other psychiatric disorders, as well as explore whether a combination of ADHD with any other psychiatric diagnosis would further increase the risk for suicidal behavior.
Materials and Methods
Participants
The study was undertaken in the Arkhangelsk region of Northern Russia. This area has a population of 1.5 million people, approximately 98 % of whom are ethnic Slavs. Over a period of 6 months delinquent subjects were voluntarily recruited into the study from a correctional facility for approximately 300 male adolescent inmates who had been court-sentenced to the only juvenile correction center in the region. Most of the delinquents had been convicted multiple times for offenses that included property crimes (theft, car theft, etc. −51 %), violence-related crimes (e.g. fighting, robbery −38 %), and in a smaller number of cases, rape or sexual violence (6 %) and murder (5 %). In general, those sentenced to correction for theft had displayed a pattern of repeat offending (stealing), with numerous convictions, with sentencing to the facility occurring only after a repeat conviction during parole. At the time of the study the mean official sentence length was 3.98 ± 1.61 years, with the total number of adjudications ranging between 1 and 4 (M = 1.81 ± 0.64). The participants were aged from 14 to 19 years old (M = 16.36 ± 0.84).
The study was approved by the Institutional Review Board of the Arkhangelsk State Medical Academy. All subjects were informed that participation was voluntary and that any information they provided would remain confidential. Specifically, they were assured that the institutional staff would not have access to the information they provided. Potential participants were provided with detailed descriptive information about the study and any questions they had about the study and their involvement in it were answered. At this stage, among those approached eight stated that they did not want to provide personal information and refused to participate.
In order to assess the prevalence of psychiatric diagnoses according to DSM-IV, a semi-structured psychiatric interview, the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL) [20], was conducted with 370 delinquent youths. As recruitment stretched over a period of 6 months during this period some youths were released from the facility while others entered. This meant that the interviewed group was larger than the total population of the institution at any one time. The psychiatric assessment was conducted with each participant individually.
Instruments
Lifetime Suicidal Ideation and Suicide Attempts
The affective disorders module of the K-SADS-PL [20] contains 4 items assessing suicide ideation and attempts (thoughts of death and/or wish to die; thinking about killing oneself with or without a specific plan; attempt to kill oneself and wish to die during the attempt; seriousness and severity of the attempt) both current and in the past (lifetime). Subjects who reported never having thoughts of death were categorized as belonging to the non-suicidal group (NS). Individuals who had thought of suicide, but never attempted it, were assigned to the suicidal ideation group (SI). Those who had suicidal thoughts and who had also attempted suicide were considered as the suicide attempt group (SA). As there is some evidence that youth may more readily report on suicidal ideation when providing self-reports rather than in interviews [21, 22], items from two self-reports were also used: “I think about suicide” (Youth Self-Report (YSR) [23]) and any of three statements on suicidal thoughts from the Beck Depression Inventory (BDI) [24]. Individuals who reported suicidal ideation on either self-report (BDI or YSR), but not during the interview were also included in the SI group.
Psychopathology
To obtain information on current and past diagnoses, including ADHD diagnosis, we also used the K-SADS-PL. This is a semi-structured psychiatric interview that has been extensively validated and has high inter-rater diagnostic reliability, with interrater agreement in scoring screens and diagnoses ranging from 94 to 100 % [20]. The measure has been used with the Russian youth previously [e.g. 25]. For a diagnosis to be assigned, clinically significant diagnosis-specific impairment had to be present [26]. Two psychiatrists conducted the interviews with diagnoses being assigned using DSM-IV criteria [27]. As the aim of the present study was to assess the relationship between a lifetime history of suicidality and psychopathology, lifetime rates of psychiatric diagnoses were used in the analyses. No information on the total number of previous suicide attempts was obtained.
Translation
The translation of these scales into Russian followed established guidelines, including the use of independent back translations [28]. Russian translations made by the first author were reviewed by other native Russian-speaking mental health colleagues. An official interpreter made independent back translations. The obtained versions were reconciled, analyzing and correcting inconsistencies. Translation of the K-SADS was done at the Department of Psychology, Moscow State University, following the above-mentioned procedure.
Statistical Analysis
Chi square tests were used as appropriate to examine differences between the subgroups (NS vs. SI and NS vs. SA). Binary logistic regression analysis was used to assess the association between psychiatric diagnoses and the risk of suicidal ideation and suicide attempts. Using the suicide group variable (NS vs. SI and NS vs. SA) as an outcome, a logistic regression analysis was conducted. In the first step, age and all the psychiatric diagnoses (except for ADHD) were included in the analysis. In step two (while controlling for all other psychiatric diagnoses), ADHD diagnosis was included. Finally, in order to assess whether a combination of ADHD and each of the other diagnoses would further increase the risk for suicide, over and above the individual risk associated with each particular disorder, interaction terms were created for ADHD and each individual psychiatric diagnosis, which were included in the analysis at step three. The data were analyzed using the Statistical Package for the Social Sciences (SPSS-21.0). The level of statistical significance was p < 0.05.
Results
Prevalence of Suicidal Ideation and Suicide Attempts
The psychiatric interview revealed that a lifetime history of suicidal ideation only [91 subjects (24.7 %)] and suicide attempts (with a history of suicidal ideation) [58 subjects (15.7 %)] were common, while 220 subjects (59.6 %) reported neither. Those who reported suicidal ideation through self-reports only (YSR or BDI; 56 subjects) and those who reported ideation both during the interview and through self-reporting (35 subjects) had similar rates of psychopathology, which, however, differed significantly from the NS group.
Demographic Information Related to Suicidal Ideation and Suicide Attempts
The participants in the three groups did not differ significantly on their family constellation prior to incarceration (55.9 % in NS, 50.6 % in SI and 53.2 % in SA, χ 2 = 0.62; ns, coming from complete families or families with remarried parents, as opposed to single-parent families or other family constellation). There was no significant difference between the three groups on the level of their parents’ education (27.3 % in NS, 30.6 % in SI and 40.0 % in SA, χ 2 = 2.68; ns, and 39.0 % in NS, 37.7 % in SI and 35.4 % in SA, χ 2 = 0.21; ns reported that their fathers and mothers, respectively, completed college/professional education or higher). The participants in the SA group were slightly older (16.7 ± 0.79 years) than those in the NS (16.3 ± 0.89 years) or the SI group (age = 16.3 ± 0.74 years), F = 2.62, p < 0.05. Hence, binary regression analyses were conducted controlling for age.
There was a higher prevalence of psychiatric treatment received prior to the incarceration among those reporting suicidal ideation or suicide attempts (34.3 % in NS, vs. 45.0 % in SI vs. 51.0 % in SA, χ 2 = 5.53; p < 0.05). In addition, they more frequently reported relatives’ substance abuse (14.8 % in NS, vs. 32.1 % in SI vs. 28.6 % in SA, χ 2 = 11.25; p < 0.01) or some kind of psychiatric contact by their relatives (4.7 % in NS, vs. 7.5 % in SI vs. 16.3 % in SA, χ 2 = 7.45; p < 0.05). The prevalence of violent forms of crime among the participants did not differ significantly between the three groups (58.9 %, 58.9 %, and 60.3 %, respectively, ns).
In addition, compared to the NS group, the SI group and especially the SA group more frequently reported a previous history of non-suicidal self-injurious behavior (11.4 %, 23.1 % and 36.8 %, respectively, χ 2 = 21.66; p < 0.001).
Psychopathology
The prevalence of the most common comorbid psychiatric diagnoses in the NS, SI and SA groups are presented in Table 1. The SI and SA groups generally had higher rates of psychopathology than the NS group. Significant differences between the groups were obtained for lifetime rates of major depression, PTSD, anxiety disorder, ADHD, and alcohol dependence, but no differences were found in the rates of drug dependence. In addition, the number of comorbid diagnoses was tallied for each subject (no psychiatric diagnosis, 1–2 psychiatric diagnoses and 3 or more psychiatric diagnoses). The SA group had the highest rate of comorbid psychopathology (63.8 % having 3 or more diagnoses), as compared to the SI group (51.6 %) and the NS group (29.5 %) (χ 2 = 31.68; p = 0.001).
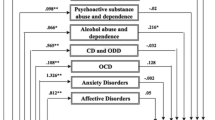
Finally, as described above, a series of binary logistic regression analyses was conducted, using the suicide group variable as an outcome. Two separate analyses were conducted, with the NS versus SI groups and the NS versus SA groups, as the outcome variables (Table 2). When comparing the NS and SI groups, the diagnosis of CD appeared as a significant predictor for SI in the first step, explaining 6.6 % of the variance. In step two, having an ADHD diagnosis was a significant predictor for SI, even after controlling for comorbidity, and explained additional 5.6 % of the variance. Finally, in step 3, the interaction effect for ADHD by drug dependence appeared as significant predictor for SI (explaining additional 4.4 % of the variance). Hence, all psychiatric disorders combined explained 16.6 % (Nagelkerke R2) of the difference between the NS and SI groups.
When comparing the NS and SA groups (Table 2), age and the diagnoses of alcohol dependence and PTSD appeared as significant predictor for SA in the first step, explaining 16.3 % of the variance. In step two, having an ADHD diagnosis was a significant predictor for SA, even after controlling for comorbidity, and explained additional 7.5 % of the variance. At this stage, age was no longer a significant predictor. Finally, in step 3, the interaction effects for ADHD by alcohol dependence appeared as significant predictors of SA (explaining additional 4.4 % of the variance). Hence, all psychiatric disorders combined explained 30.3 % (Nagelkerke R2) of the difference between the NS and SA groups.
Discussion
The purpose of the present study was to evaluate the impact of mental health problems on the risk for suicide in a group of delinquent adolescents, who, according to previous research, represent a high risk group for suicidal behavior. The study further aimed to evaluate whether having only ADHD or ADHD combined with other psychiatric disorders would pose an additional risk for suicidal behavior, over and above that of other mental health problems.
The results of this study indicate that suicidal ideation and suicide attempts are common in Russian delinquent youth and that their lifetime prevalence is comparable to that found in other studies with juvenile delinquents [e.g. 4]. A total of 40.4 % of the participants reported a history of either suicidal ideation only or both suicidal ideation and attempts. This suggests that juvenile detention and correctional facilities must systematically screen for suicide risk and that psychiatric services in such facilities must be increased.
This study found that juvenile delinquents with a history of suicidal thoughts and of attempted suicide differed significantly from the non-suicidal delinquents in terms of experiencing higher rates of major depression, posttraumatic stress disorder, conduct disorder, ADHD, anxiety disorders, and alcohol dependence. These differences are all relatively well described in the literature and have been demonstrated previously both in the general population and among delinquent youths [8, 29, 30]. In addition, a greater number of comorbid psychiatric diagnoses substantially increased the risk for suicidal behavior in our sample. This finding concurs with the results from previous research that comorbidity tends to increase the risk for both attempted and completed suicide [31]. Finally, those with a history of suicidal thoughts and especially, of attempted suicide, differed significantly from the non-suicidal delinquents in terms of their previous contact with psychiatric services, and in terms of the self-reported history of psychiatric and substance abuse problems in their relatives.
Until recently, there has been comparatively little focus on the association between ADHD and suicidal behavior [32]. As juvenile delinquents represent a high risk group with respect to both the prevalence of suicidal behavior and of ADHD [e.g. 33], evaluating this association in delinquent youths may provide an important insight into suicidal behavior in youth. Our study found that ADHD poses an increased risk for suicidal behavior. In addition, and in line with recent register- and population-based studies, the association between ADHD and suicidal behavior remained robust even after controlling for the presence of comorbid mental disorders [34, 35]. These findings also support the results from the somewhat limited previous research suggesting that ADHD represents an important risk factor for suicidal behavior in delinquent youth [10, 11].
Several mechanisms have been proposed in order to explain the association between ADHD and an increased risk of suicidal behavior, focusing on the role of the core ADHD symptoms. In particular, a strong link has been established between impulsivity, one of the main clinical characteristics of ADHD, and an increased risk for suicidal behavior both in the general population [36] and in individuals with ADHD [e.g. 37], reflecting a tendency to act quickly without forethought and with little regard for the consequences [27]. Likewise, impulsive-aggressive behavior (with an emotional impulsiveness at its core) has been linked to an increased risk for suicide [38]. It has been further suggested that emotion dysregulation, previously linked to suicidal behavior in adolescents [39], might be considered as one of the central components in ADHD [40].
As described above, the results from this study show that ADHD in combination with alcohol and drug dependence further increased the risk for suicidal ideation and suicidal acts, respectively, as compared to the risk posed by each individual disorder. It is well-documented that children with ADHD are at a greater risk of developing psychiatric problems, such as depression, conduct problems and substance abuse [41], which in turn, are strongly associated with suicide in adolescence. Some authors have suggested that comorbidity between ADHD and other psychiatric disorders amplifies the risk for poorer outcomes [42] and even, that ADHD makes the clinical outcome of comorbid disorders worse in every respect [43], possibly as a result of greater psychosocial adversity, such as peer rejection, school problems and conflictual relationships in the family [e.g. 44, 45]. Both alcohol and drug dependence seem to further impact the general vulnerability associated with ADHD symptoms and potentiate the risk for suicidal behavior, possibly by further decreasing cognitive control and increasing impulsivity. Along these lines, some studies [46] have found that ADHD may have an indirect effect on suicidal ideation through emotion regulation deficits, which are also typical for traumatic reactions [47] and which tend to be further exacerbated under the influence of substances [48].
This research has the usual limitation of any study that uses cross-sectional data i.e. that it was not possible to determine causal relationships. The study also relied on self-reports of suicidal behavior and was limited by its retrospective assessment of lifetime psychopathology. Although the prevalence of suicidal ideation and suicide attempts in our population was similar to that in other studies of juvenile delinquents, given the stigma attached to mental health problems, including suicide, it is possible that subjects might have responded in a socially desirable manner, hence biasing results. This seems particularly plausible, considering that while using different data sources for identifying the SI group, we found a discrepancy in the figures between the reporting methods. In addition, although we were able to use data from different sources for SI, we could not do this for SA which is therefore more likely to be underestimated. Finally, the findings were generated from a sample of incarcerated delinquent youth from Northern Russia and additional studies are needed in other samples and cultures in order to determine whether these findings are more generally representative.
Clinical Implications
The results from the present study support previous findings that suicidal behavior is common in delinquent populations and is strongly associated with psychopathology. Consequently, thorough psychological assessment of these youngsters is essential. These findings are also important for the field of forensic psychiatry, as they demonstrate high lifetime history rates of suicidal ideation/attempts in juvenile delinquents, with particularly high rates of psychopathology in youth who have such a history.
The finding that an ADHD diagnosis by itself, as well as in combination with alcohol and substance dependence, increases the risk for suicide ideation and suicide attempts has further important research and clinical implications. It underlines the need for more research on the association between ADHD and suicidal behavior in other groups; in particular, in general population samples in order to better understand the factors associated with it. The study also highlights the importance of adequately detecting and treating ADHD, and of making health care professionals aware that there might be an increased risk of suicidal behavior among delinquent youths with ADHD.
Summary
Despite its public health and clinical importance, the prediction of suicidal behavior in adolescents still poses a substantial clinical challenge for mental health professionals. Delinquent adolescents constitute a highly vulnerable population, with the prevalence of lifetime suicidal ideation and suicide rates being several times higher than in the age-matched general population. This study evaluated the role of psychiatric morbidity in relation to a history of suicidal behavior in Russian juvenile delinquents with a particular focus on ADHD. Suicidality and psychopathology were assessed in 370 incarcerated male juvenile delinquents from Northern Russia using a semi-structured psychiatric interview. A lifetime history of both suicidal ideation only and suicidal ideation with suicide attempts was common. An ADHD diagnosis increased the risk for suicidal behavior, both as a separate risk factor, as well as in combination with drug dependence and alcohol dependence. Our findings highlight the importance of adequate detection and treatment of psychiatric disorders, especially ADHD, in vulnerable youths and of making health care professionals aware that there might be an increased risk of suicidal behavior among delinquent youths with ADHD. The study further underlines the need for more research on the association between ADHD and suicidal behavior in other groups; in particular, in general population samples.
References
Center for Disease control and Prevention (2013) Injury prevention and control: web-based injury statistics query and reporting system. http://www.cdc.gov/injury/wisqars/index.html
Gould MS, Shaffer D, Fisher P, Kleinman M, Morishima A (1992) The clinical prediction of adolescent suicide. In: Maris RW, Berman AL, Maltsberger JT, Yufit RI (eds) Assessment and prediction of suicide. Guilford Press, New York, pp 130–143
World Health Organization (2007) Preventing suicide in jails and prisons. WHO Press, Geneva
Casiano H, Katz LY, Globerman D, Sareen J (2013) Suicide and deliberate self-injurious behavior in juvenile correctional facilities: a review. J Can Acad Child Adolesc Psychiatry 22:118–124
Gallagher CA, Dobrin A (2006) Facility-level characteristics associated with serious suicide attempts and deaths from suicide in juvenile justice residential facilities. Suicide Life Threat Behav 36:363–375
Fazel S, Benning R, Danesh J (2005) Suicides in male prisoners in England and Wales, 1978–2003. Lancet 366:1301–1302
Abram KM, Choe JY, Washburn JJ, Teplin LA, King DC, Dulcan MK (2008) Suicidal ideation and behaviors among youths in juvenile detention. J Am Acad Child Adolesc Psychiatry 47:291–300. doi:10.1097/CHI.0b013e318160b3ce
Kempton T, Forehand R (1992) Suicide attempts among juvenile delinquents: the contribution of mental health factors. Behav Res Ther 30:537–541
Rohde P, Seeley JR, Mace DE (1997) Correlates of suicidal behavior in a juvenile detention population. Suicide Life Threat Behav 27:164–175
Steiner H (2007) Suicidality, psychopathology, and gender in incarcerated adolescents in Austria. J Clin Psychiatry 68:1593–1600
Putnins AL (2005) Correlates and predictors of self-reported suicide attempts among incarcerated youths. Int J Offender Ther Comp Criminol 49:143–157
Impey MI, Heun R (2012) Completed suicide, ideation and attempt in attention deficit hyperactivity disorder. Acta Psychiatr Scand 125:93–102. doi:10.1111/j.1600-0447.2011.01798.x
Nigg JT (2013) Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin Psychol Rev 33:215–228
Barbaresi WJ, Colligan RC, Weaver AL, Voigt RG, Killian JM, Katusic SK (2013) Mortality, ADHD, and psychosocial adversity in adults with childhood ADHD: a prospective study. Pediatrics 131:637–644
Barkley R, Fischer M. (2005) Suicidality in children with ADHD. ADHD Rep 13:1–4
Hinshaw SP, Owens EB, Zalecki C, Huggins SP, Montenegro-Nevado AJ, Schrodek E, Swanson EN (2012) Prospective follow-up of girls with attention-deficit/hyperactivity disorder into early adulthood: continuing impairment includes elevated risk for suicide attempts and self-injury. J Consult Clin Psychol 80:1041–1051. doi:10.1037/a0029451
Agosti V, Chen Y, Levin FR (2011) Does Attention Deficit Hyperactivity Disorder increase the risk of suicide attempts? J Affect Disord 133:595–599. doi:10.1016/j.jad.2011.05.008
Park S, Cho MJ, Chang SM, Jeon HJ, Cho SJ, Kim BS, Bae JN, Wang HR, Ahn JH, Hong JP (2011) Prevalence, correlates, and comorbidities of adult ADHD symptoms in Korea: results of the Korean epidemiologic catchment area study. Psychiatry Res 186:378–383
Vermeiren R (2003) Psychopathology and delinquency in adolescents: a descriptive and developmental perspective. Clin Psychol Rev 23(2):277–318
Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, Ryan N (1997) Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36:980–988
Kaplan ML, Asnis GM, Sanderson WC, Keswani L, De Lecuona JM, Joseph S (1994) Suicide assessment: clinical interview vs. self-report. J Clin Psychol 50:294–298
Velting DM, Rathus JH, Asnis GM (1998) Asking adolescents to explain discrepancies in self-reported suicidality. Suicide Life Threat Behav 28:187–196
Achenbach TM. Manual for the youth self-report and 1991 profile. Burlington: University of Vermont Department of Psychiatry, 1991
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:561–571
Ruchkin VV, Schwab-Stone M, Koposov R, Vermeiren R, Steiner H (2002) Violence exposure, posttraumatic stress, and personality in juvenile delinquents. J Am Acad Child Adolesc Psychiatry 41:322–329. doi:10.1097/00004583-200203000-00012
Gould MS, King RA, Greenwald S, Fisher P, Schwab-Stone M, Kramer R, Flisher AJ, Goodman S, Canino G, Shaffer D (1998) Psychopathology associated with suicidal ideation and attempts among children and adolescents. J Am Acad Child Adolesc Psychiatry 37:915–923
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4th edn. APA, Washington, DC
Sartorius N, Kuyken W (1994) Translation of Health Status Instruments. In: Orley J, Kuyken W (eds) Quality of life assessment: international perspectives. Springer, Berlin-Heidelberg, pp 3–18
Brent DA, Perper JA, Moritz G et al (1993) Psychiatric risk factors for adolescent suicide: a case-control study. J Am Acad Child Adolesc Psychiatry 32:521–529
Shaffer D, Gould MS, Fisher P, Trautman P, Moreau D, Kleinman M, Flory M (1996) Psychiatric diagnosis in child and adolescent suicide. Arch Gen Psychiatry 53:339–348
Lewinsohn PM, Rohde P, Seeley JR (1995) Adolescent psychopathology III: the clinical consequences of comorbidity. J Am Acad Child Adolesc Psychiatry 34:510–519
Barkley RA (2014) ADHD and injuries: accidental and self-inflicted. ADHD Rep 22:1–8
Scott M, Underwood M, Lamis DA (2015) Suicide and related-behavior among youth involved in the juvenile justice system. Child Adolesc Soc Work 32:517–527. doi:10.1007/s10560-015-0390-8
Ljung T, Chen Q, Lichtenstein P, Larsson H (2014) Common etiological factors of attention deficit/hyperactivity disorder and suicidal behavior: a population-based study in Sweden. JAMA Psychiatry 71:958–964
Stickley A, Koyanagi A, Ruchkin V, Kamio Y (2016) Attention-deficit/hyperactivity disorder symptoms and suicide ideation and attempts: findings from the adult psychiatric morbidity survey 2007. J Affect Disord 189:321–328. doi:10.1016/j.jad.2015.09.061
Mann JJ, Oquendo M, Underwood MD, Arango V (1999) The neurobiology of suicide risk: a review for the clinician. J Clin Psychiatry 60(Suppl 2):7–11
Furczyk K, Thome J (2014) Adult ADHD and suicide. Atten Defic Hyperact Disord 6:153–158
McGirr A, Turecki G (2007) The relationship of impulsive aggressiveness to suicidality and other depression-linked behaviors. Curr Psychiatry Rep 9:460–466
Weinberg A, Klonsky ED (2009) Measurement of emotion dysregulation in adolescents. Psychol Assess 21:616–621
Martel MM (2009) Research review: a new perspective on attention-deficit/hyperactivity disorder: emotion dysregulation and trait models. J Child Psychol Psychiatry 50:1042–1051
Willcutt EG, Pennington B (1999) Psychiatric comorbidity associated with DSM-IV ADHD in a non-referred sample of twins. J Am Acad Child Adolesc Psychiatry 38:1355–1362
Renaud J, Brent DA, Birmaher B, Chiappetta L, Bridge J (1999) Suicide in adolescents with disruptive disorders. J Am Acad Child Adolesc Psychiatry 38:846–851
James A, Lai FH, Dahl C (2004) Attention deficit hyperactivity disorder and suicide: a review of possible associations. Acta Psychiatr Scand 110:408–415
August GJ, Realmuto GM, Macdonald AW III, Nugent SM, Crosby R (1996) Prevalence of ADHD and comorbid disorders among elementary school children screened for disruptive behavior. J Abnorm Child Psychol 24:571–595
Kuhne M, Schachar R, Tannock R (1997) Impact of comorbid oppositional or conduct problems on attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 36:1715–1725
Van Eck K, Ballard E, Hart S, Newcomer A, Musci R, Flory K (2015) ADHD and suicidal ideation: the roles of emotion regulation and depressive symptoms among college students. J Atten Disord 19:703–714. doi:10.1177/1087054713518238
Frewen PA, Lanius RA (2006). Toward a psychobiology of posttraumatic self-dysregulation: reexperiencing, hyperarousal, dissociation, and emotional numbing. Ann NY Acad Sci 1071:110–124. doi:10.1196/annals.1364.010
Wilens TE, Martelon M, Anderson JP, Shelley-Abrahamson R, Biederman J (2013) Difficulties in emotional regulation and substance use disorders: a controlled family study of bipolar adolescents. Drug Alcohol Depend 132:114–121. doi:10.1016/j.drugalcdep.2013.01.015
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ruchkin, V., Koposov, R.A., Koyanagi, A. et al. Suicidal Behavior in Juvenile Delinquents: The Role of ADHD and Other Comorbid Psychiatric Disorders. Child Psychiatry Hum Dev 48, 691–698 (2017). https://doi.org/10.1007/s10578-016-0693-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-016-0693-9