
Abstract
Antibodies and oxidative stress are hallmarks of multiple sclerosis (MS) lesions. We aimed to clarify the relation between them, their role in MS patients and to investigate their specificity, comparing MS with classical neurodegenerative diseases (ND). Brain samples from 14 MS cases, 6 with ND and 9 controls (without neurological diseases). Immunohistochemistry assays were used to detect oxidized lipids (EO6), IgG and IgM, oligodendrocytes (Olig2), axons (NF, neurofilament) and cellular (TUNEL) and axonal damage (APP, amyloid precursor protein). We did not observe EO6 in controls. All samples from MS patients showed EO6 in oligodendrocytes and axons within lesions. We did not detect co-localization between EO6 and antibodies. Neither did we between EO6 and TUNEL or APP. 94.4% of TUNEL-positive cells in normal appearing white matter were also stained for IgG and 75.5% for IgM. IgM, but not IgG, co-localized with APP. EO6 was associated with axonal damage in amyotrophic lateral sclerosis (ALS). We did not observe association between antibodies and cellular or axonal damage in ND patients. MS patients showed a higher number of B cells and plasma cells in the lesions and meninges than controls. The number of B cells and plasma cells was associated with the presence of antibodies and with the activity of the lesions. We observed a main role of B lymphocytes in the development of MS lesions. Antibodies contribute to the oligodendrocyte and axonal damage in MS. Oxidative stress was associated with axonal damage in ALS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is the most common chronic inflammatory demyelinating disease of the Central Nervous System (CNS). One of the main features observed in the CNS of MS patients is the presence of IgG, IgM and IgA antibodies on degenerating myelin sheaths (Lucchinetti et al. 1996; Storch et al. 1998), oligodendrocytes and axons (Sádaba et al. 2012; Zhang et al. 2005) located in demyelinated lesions. IgG and IgM were also detected in new forming lesions (Barnett and Prineas 2004; Gay et al. 1997) and normal appearing white matter (Sádaba et al. 2012) and were associated with activated complement factors and foamy macrophages (Breij et al. 2008; Storch et al. 1998; Sádaba et al. 2012).
The source of these antibodies is unknown, but it have been described as follicle-like structures in the meninges of MS patients (Magliozzi et al. 2007; Prineas 1979; Serafini et al. 2004), plasma cells in the lesions (Esiri 1977) and increased activated and memory B cells in the CSF (Haas et al. 2011). In addition, clonal expansion of these cells in brain lesions has been demonstrated, indicating that an antigen-driven immune response could be present (Baranzini et al. 1999) B lymphocytes also have antibody-independent effector functions. They present antigens to T lymphocytes, express in the membrane co-stimulatory molecules and secrete cytokines that regulate the activation of the latter (Ireland et al. 2012).
Nevertheless, it cannot be excluded that additional or other primary mechanisms may be involved in the pathogenesis of MS. Demyelinated plaques show oxidation of different molecules, such as DNA (Vladimirova et al. 1998), proteins (Bizzozero et al. 2005; Cross et al. 1998; Diaz-Sanchez et al. 2006; Liu et al. 2001) and lipids (Haider et al. 2011), which is related with demyelination and neurodegeneration (Haider et al. 2011). A marker of oxidative stress was observed in oligodendrocytes and axons located predominantly in actively demyelinating white matter and cortical lesions (Fischer et al. 2013), indicating that oxidative stress is related to the activation of macrophages and astrocytes (Fischer et al. 2012; Liu et al. 2001).
Moreover, inflammation and oxidative stress are not specific hallmarks of MS lesions, which makes it difficult to evaluate their role in the pathophysiology of the disease. Mutations in copper/zinc ion-binding superoxide dismutase and enzymes, which regulate the oxidation/reduction balance, have been detected in a relatively low percentage of Amyotrophic Lateral Sclerosis (ALS) patients (Kiernan et al. 2011; Rosen et al. 1993). Different studies performed in this disease have also demonstrated immunoglobulin (Engelhardt and Appel 1990) and complement (McGeer et al. 1991) deposition in the CNS of these patients and the presence of serum antibodies to voltage-gated calcium channels (Engelhardt et al. 1995; Kimura et al. 1994). Biochemical analyses have demonstrated increased lipid oxidation in astrocytes located in temporal lobe samples from frontotemporal dementia (FTD) patients (Martínez et al. 2008). Other groups detected antibodies in the cerebrospinal fluid of the latter (Kankaanpää et al. 2009).
Studies of Parkinson's disease (PD) have demonstrated that glutathione concentration is decreased in the substantia nigra (Jenner et al. 1992), and rats inoculated with IgG purified from these individuals showed destruction of the substantia nigra (Chen et al. 1998).
In these neurological diseases, there are specific targets that are damaged. Demyelination and axonal damage are the main targets of damage in MS patients (Stadelmann et al. 2011), while motor neurons are damaged in ALS patients (Kiernan et al. 2011), and the main target in PD disease is dopaminergic neurons (Moore et al. 2005). FTD is tau-associated dementia (Irwin 2016).
In this paper, we analysed the relation between antibodies and oxidative stress and their role in MS patients. We also aimed to investigate their specificity, comparing MS with classical neurodegenerative diseases (ND).
Materials and Methods
Tissue Specimens
MS brain tissues were obtained from the UK Multiple Sclerosis Tissue Bank, the Thomas Willis Oxford Brain Collection (now the Oxford Brain Bank), or Neuro Resource, University College London, Institute of Neurology and Banco de Tejidos CIEN, Instituto Carlos III. The former also donated the samples from patients with ALS, FTD and PD. Control samples were donated by the Departamento de Anatomía, Universidad San Pablo CEU. All subjects, or their close relatives, gave informed consent for brain donation after their deaths. The study was approved by the Ethical Committee of the Universidad San Pablo CEU (113/16/05).
We studied 96 formalin-fixed, paraffin-embedded tissue blocks from neurologically normal controls (n = 9) and patients with ALS (n = 2), FTD (n = 2), PD (n = 2) and MS (n = 14) patients. The demographic and clinical data and the type of samples analysed are summarized in Table 1.
The age at death of MS patients ranged from 26 to 69 and the disease duration from 6 months to 42 years. One case was primary progressive, 2 were acute MS, 9 showed a secondary progressive course and in 2 cases the evolution was not available.
Lesional Staging
Consecutive sections from MS tissue blocks were stained with hematoxylin-eosin to identify areas of hypercellularity or hypocellularity and with Luxol fast blue (LFB) to show the demyelinated areas. In order to characterize the lesion activity, we also performed immunohistochemistry with anti-CD68 antibody to detect macrophages. The protocols were used in previous works (Ferguson et al. 1997; Tzartos et al. 2008; Sádaba et al. 2012).
MS lesions were ordered as follows: (1) chronic inactive: lesions showing demyelination, hypocellularity, low number of inflammatory infiltrates and absence or marked scarcity of CD68-positive cells; (2) chronic active: lesions presenting hypercellularity and many macrophages at the edge of chronic lesions; (3) acute: lesions showing a high degree of inflammatory cell infiltration, including macrophages, some of which contained cytoplasmic Luxol fast blue-reactive fragments of myelin in the lesion. The 62 blocks from MS patients included 17 chronic inactive, 29 chronic active and eleven acute lesions; all the 30 blocks from patients without neurological disease were classified as control NAWM.
Then, we used immunohistochemistry assays (Sádaba et al. 2012) to classify the MS lesions regarding the presence of IgG or IgM (Supplementary Data 1).
Corresponding stains were performed to stage samples from patients with neurodegenerative diseases. We analysed samples from 2 Parkinson disease patients. All samples showed characteristic histological alterations (loss of dopaminergic neurons and aggregation of the protein α-synuclein into ubiquitin-positive Lewy bodies). We analysed samples from 2 patients with frontotemporal dementia. Samples from patient 1 showed classical histological alterations, gliosis (as it is observed in Fig. 3), neuronal loss and ballooned neurons. Samples from patient 2 did not show these characteristic histological alterations. We analysed samples from 2 patients with amyotrophic lateral sclerosis. Samples from patient 1 showed loss of upper motor neurons and associated astrogliosis. Samples from patient 2 did not show these classical histological alterations.
Immunohistochemistry
Sections (6 μm) of formalin-fixed and paraffin-embedded samples from the central nervous system were deparaffinised with Hemo-De solution (manufacturer, Scientific Safety Solvents, Fort Worth, Tex.; distributor, Fisher Scientific Co.) and rehydrated in ethanol and PBS. EDTA 2 mM, Tris 50 mM pH 90.0 buffer and microwave heating was used for retrieval of antigen as previously described (Kim et al. 2004). Consecutive sections were stained with mouse anti-IgM (Santa Cruz Biotechnology, Inc.,) diluted 1:10, mouse anti-IgG (AbD Serotec) diluted 1:50, mouse anti-EO6 (Avanti Polar Lipids) diluted 1:400, rabbit anti-APP (Sigma-Aldrich) diluted 1:200, rabbit anti Olig2 (oligodendrocyte transcription factor 2, Chemicon) diluted 1:250 overnight at 4 °C, anti CD79 diluted 1:40 (donated by Margaret Jones) and anti CD138 diluted 1:50 (Abd Serotec). Staining was developed with Dako Real Envision Detection System (Dako) as described previously (Tzartos et al. 2008).
Immunofluorescence
We used double-immunofluorescence to study the target of IgM and IgG antibodies and oxidative stress. Tissue sections were fixed as described above and then incubated with anti-IgM or anti-IgG or anti-EO6 at 1:10 or 1:200 or 1:100 dilution, respectively, overnight at 4 °C. Staining was developed using Tyramide signal amplification Kit with Alexa Fluor 488 (Invitrogen). After washing, slides were incubated overnight with a second antibody: mouse anti-EO6 at 1/100 dilution, rabbit anti-Olig-2 (EMD Millipore) at 1:250 dilution, rabbit anti-NF (neurofilament, AbD Serotec) at 1:300 dilution and rabbit anti-APP at 1:100 dilution. Appropriate secondary antibodies included anti-mouse-HRP or anti-rabbit-HRP. Samples were stained with Tyramide signal amplification kit with Alexa Fluor 568 (Invitrogen). When primary antibodies were all mouse monoclonal antibodies we used Vector M.O.M immunodetection kit (Vector Laboratories) to block the first antibody. As negative controls for each double label, the same procedure as above was followed except that one of the primary antibodies was omitted. No staining was seen in these sections. Positive control for IgM and IgG consisted of paraffin-embedded tonsillar tissue.
TUNEL Assay
Terminal deoxynucleotidyl transferase dUTP nick end labelling (TUNEL) assay was performed in order to analyse the oligodendrocyte damage and the relation of the latter with the oxidative stress or humoral immune response. Tissue sections were fixed, deparaffinised and rehydrated as described above. After peroxidase blocking, samples were incubated with TdT Reaction Buffer for 10 min. After washing, samples were incubated with TdT reaction mixture (Enzyme Reagent + Label Reagent) for 2 h at room temperature. Samples were washed with Stop Wash Buffer solution for 10 min. After washing, slides were incubated with the samples with streptavidin-HRP diluted 1:1000 for 20 min at room temperature. When immunohistochemistry assays were developed, DAB was used as chromogen. Tyramide-Alexa Fluor 568 was used when double-immunofluorescence labelling was performed.
Cell Quantification
To determine the number of cells in different areas, we marked out the area of lesions, NAWM and meninges using the ImageJ software (National Institutes of Health, Bethesda, MD). To identify the lesional area, we used hematoxylin staining to identify areas of hyper or hypocellularity. To assess the accuracy of the measurement of the area of the lesions and NAWM, we also calculate the lesional area in serial samples stained with Luxol or anti-CD68. Then, we counted manually the number of CD79- or CD138-positive cells using the same software.
Data Acquisition
When using diaminobenzidine immunohistochemistry, digital images of tissue sections were captured using a Scanner Leica SCN4000. For immunofluorescence, sections were examined with a fluorescence microscope (Leica fluorescence microscope CTR6000). Images were captured using Leica camera DFC345FX. ImageJ software (National Institutes of Health, Bethesda, MD) was used to manage the images.
Results
Study of Oxidative Stress in Samples from Patients with Neurological Diseases
We did not detect oxidized lipids (EO6) in normal brain tissue from normal controls. However, we could detect oxidative stress in tissue from all MS patients analysed. The presence of oxidized lipids was observed in patients ranging from 6 months to more than 40 years of disease duration and EO6 was detected in patients with secondary progressive MS and acute disease.
We did not observe EO6 staining in NAWM samples from MS patients nor in chronic inactive lesions, except in one sample from an acute MS patient. However, all chronic active and acute lesions analysed were positive for EO6. Oxidized lipids were observed in the cytoplasm of foamy macrophages, cells resembling oligodendrocytes and in axon-like structures, located mainly in the edge of the lesions (Fig. 1).

Analysis by immunohistochemistry of oxidative stress (EO6) in MS patients. Serial sections of a sample from control group (a, c) and chronic active lesions (b, e–f) and NAWM (d) from a MS patient. EO6 labelling (a, c, d, e, f) and Luxol Fast Blue (b) staining. No EO6-positive staining was observed in control group (c) or NAWM (d) from MS patient. e The picture shows EO6-positive oligodendrocyte-like cells and EO6-positive foamy macrophages. f Representative example of EO6-positive axon-like structures. a, b scale bar= 4 mm. c–f scale bar=25 µm
We also detected EO6-positive axon-like structures in all samples analysed from patients with ALS or FTD (Fig. 2a–d). However, we did not observe EO6-positive oligodendrocyte-like cells in this patients. No lipid oxidation was observed in PD samples analysed (Fig. 2e).

Analysis by immunohistochemistry of oxidative stress (EO6) in patients with neurodegenerative diseases. Samples from patients with ALS (a, b), FTD (c, d) and Parkinson (e, f). Representative images from patients with ALS (a) and FTD (c) showing positive staining for EO6. Magnifications from previous pictures showed axon-like structures labelled for EO6 in samples from patients with ALS (b) and FTD (d). No positive staining for EO6 were detected in patients with Parkinson (e). a, c, c scale bar= 4 mm. b, d, f scale bar = 25 µm
To demonstrate if oxidative stress affected oligodendrocytes and axons in patients with MS, ALS and FTD, we developed double-immunofluorescences (EO6/Olig2, EO6/NF, IgG/Olig2, IgG/NF, IgM/Olig2, IgM/NF). In MS patients, we observed oligodendrocytes (Olig2+ cells) and axons (NF+) stained for EO6 (Supplementary Data 2).
To study the specificity of these results, we also analysed the presence of E06 in patients with neurodegenerative diseases. Lipid oxidation affected NF-positive structures in patients with ALS or FTD (Supplementary Data 3).
Study of Antibody Deposits in Samples from Patients with Neurological Diseases
To analyse the specificity of antibody deposits and their role in the physiopathology of MS, we analysed the presence of IgG and IgM in samples from patients with ALS, FTD and PD. The study showed IgG on neurons in ALS patients (Fig. 3a, b) and on cells resembling astrocytes in FTD specimens (Fig. 3c, d). However, we did not detect IgG deposits in PD samples nor IgM in any case analysed (Fig. 3e–l). In summary, the antibody deposit pattern was different from that observed in tissue from MS patients, where antibodies were located on axons and oligodendrocytes and included IgM as well as IgG.

Analysis by immunohistochemistry of IgG and IgM deposits in patients with neurodegenerative diseases. Serial sections of samples from ALS (a, b, g, h), FTD (c, d, i, j), Parkinson (e, f, k, l). Labelling for IgG (a–f) and IgM (g–k). Positive staining for IgG was observed in samples from ALS (a, b) and FTD (e, f). Magnification of these pictures showed IgG deposits on neurons in ALS (b) and on astrocyte-like cells in FTD (d) brain samples. IgG deposits were not observed when brain samples from Parkinson (e, f) were analysed. Immunohistochemistry analysis did not demonstrate IgM deposits in samples from ALS (g, h), FTD (i, j) and Parkinson (k, l) patients. a, c, e, g, i, k Scale bar= 4 mm. b, d, f, h, j, l scale bar = 25 µm
Relation Between Oxidative Stress and Antibody Deposits in MS Patients
We have observed EO6/Olig2 double-positive cells and EO6-positive axons in this study (Suplementary Data 2). He have also observed IgG/Olig2 and IgM/Olig2 double-positive cells and IgG and IgM around axons (Supplementary Figure 4) in this study. In summary, EO6 and antibodies label the same structures, oligodendrocytes and axons (the same pattern). For this reason, we investigated whether oxidative stress and humoral immune responses were related. Consecutive immunohistochemistry demonstrated EO6-positive cells in IgG−/IgM−, IgG+/IgM− and IgG+/IgM+ lesions. Then we developed EO6/IgG and EO6/IgM double-immunofluorescence. However, we did not find IgG/EO6 or IgM/EO6 double-positive cells or axons in lesions (Fig. 4).

Relation of oxidative stress and IgG or IgM deposits in MS lesions. Representative images from the edge of chronic active lesions from MS patients. Staining for IgG (a, g, green), IgM (d, j, green) and lipid oxidation (EO6, b, e, h, k, red). Overlays did not show double-positive cells for EO6 and IgG (c) nor EO6/IgM double staining (f). Double-immunofluorescence did not demonstrate IgG/EO6 nor IgM/EO6 double-positive axons. Scale bar = 25 µm
Relation Between Oxidative Stress, Antibody Deposits and Tissue Damage in Patients with MS, FTD and ALS
Once we had demonstrated that oxidative stress and antibodies did not co-localize, first, we studied the role of oxidative stress and antibodies in the injury of oligodendrocytes in MS patients.
We developed an immunohistochemistry technique to detect damaged cells (TUNEL+) and we analysed white matter samples from these individuals and a control group.
We did not observe TUNEL-positive cells in the control group, but we detected TUNEL-positive cells in lesions and NAWM samples from MS patients (Fig. 5a–c).

Relation of IgG or IgM deposits and oligodendrocyte injury. Representative images from control group (a), and chronic active lesions (b, d–f) and NAWM (c, g–l) samples from MS patients. Diaminobenzidine (DAB) labelling for TUNEL (a–c). Fluorescence staining for EO6 (d, green), TUNEL (e, h, k, red), IgG (g, green) and IgM (j, green). Immunohistochemistry showed positive TUNEL cells in lesions (b) and NAWM (c). Double-positive EO6/TUNEL cells were not detected (f). Double-immunofluorescence demonstrated that most of the TUNEL-positive cells were also IgG positive (94.4%) (i). Most of the TUNEL cells were also IgM-positive (75.5%) (l). Scale bar = 25 µm
Following on from this observation, we performed EO6/TUNEL, IgG/TUNEL and IgM/TUNEL double-labelling to analyse the relation between these factors and cell damage. We did not observe EO6/TUNEL double-positive cells in any case (data not shown).
To clarify the role of antibodies in the oligodendrocyte damage in MS patients, we studied NAWM samples because, as described above, we did not detect oxidative stress nor inflammatory infiltrate in this area. We observed that most TUNEL-positive cells were also stained for IgG (94.4%) or IgM (75.5%) (Fig. 5d–l).
We further proposed to study if oxidative stress or immunoglobulin deposits were related with axon injury in patients with MS, ALS and FTD. To achieve this goal, first, we developed peroxidase staining on consecutive slides analysed previously to detect amyloid precursor protein (APP).
We did not observe APP deposits in samples from the control group or NAWM samples from MS patients, but we detected APP deposits in axons located in the centre and edge of chronic active lesions and also in acute lesions (Fig. 6a–c).

Study of axonal damage in MS patients. Serial sections of samples from control group (a), and NAWM (b) and chronic active lesion (c-l) from MS patient. DAB staining for APP (a-c) and fluorescent labelling for EO6 (e, green), IgG (g, green), IgM (j, green) and APP (e, h, k, red). The picture showed axons positively stained for APP in chronic active lesion from MS patients (b), but not in the control group (a) or NAWM from MS patients (c). Double-immunofluorescence showed that neither EO6 (f) nor IgG (i) co-localized with APP on axons. Overlays (l) demonstrated double-positive axons for APP and IgM. Scale bar = 25 µm
Then, we performed EO6/APP, IgG/APP and IgM/APP double-immunofluorescence on samples from MS patients to clarify the role of oxidative stress and antibodies in the damage of neurons and axons. We did not detect EO6/APP nor IgG/APP co-localization on axons in demyelinated areas from those samples (Fig. 6d–i). However, most of the APP-positive axons were also IgM-positive (Fig. 6j–l) in MS patients.
We did not observe IgG/APP co-localization on neurons in ALS patients (data not shown). However, contrary to MS, we found EO6/APP double-positive axons in samples from ALS and FTD patients (Fig. 7).

Study of axonal damage in brain samples from ALS (a–c) and FTD (d, f) patients. Fluorescent labelling for EO6 (e, d, green) and APP (b, e, red). Overlays demonstrated the presence of double-positive axons for APP and EO6 in samples from ALS (c) and FTD (f). Scale bar 25 μm
In summary, in MS patients, IgG and IgM were associated with oligodendrocyte damage and only IgM was linked with axonal damage. However, oxidative stress was related to axonal damage in patients with ALS and FTD.
Relation Between MS Lesion Activity and the Presence of B Lymphocytes and Plasma Cells in the Central Nervous System
To further investigate the role of the humoral immune response in the MS tissue damage, we analysed the presence of B lymphocytes and plasma cells in lesions (parenchyma and perivascular space) and the meninges regarding the activity of the lesions (Fig. 8a–f). Data are summarized in Table 2.

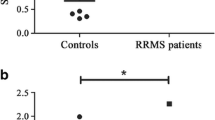
Relation between the number of B cells or plasma cells and the activity of the lesions. A Representative pictures of the presence of B cells (CD79 +) (a-c) and plasma cells (CD138 +) (d-f) in the perivascular space of chronic inactive (a, d), chronic active (b, e) and acute (c, f) lesions. g number of B cells. b Number of plasma cells. Bars represent mean ± 2xSEM (standard error of the mean). Right axis represent the number of cells in the lesions and left axis represent the number of cells in the meninges. NAWM normal appearing white matter. CI chronic inactive lesion, CA chronic active lesion, AC acute lesion, PV perivascular space, PAR parenchyma, MEN meninges, Scale bar: 25 µm
Chronic inactive (I) (p = 0.001), Chronic active (A) (p = 0.002) and Acute (C) lesions (p < 0.0001) showed a higher density of B lymphocytes in the perivascular spaces than NAWM. Acute lesions also had a higher density of these cells in the perivascular spaces than Chronic inactive lesions (p < 0.0001) or Chronic active. (p = 0.045) lesions. No statistical differences were observed between Chronic inactive and Chronic active lesions. The analysis of the parenchyma also demonstrated similar results. Chronic inactive (p = 0.013), Chronic active (p = 0.002) and Acute (p < 0.0001) lesions showed a higher density of B cells in the lesion parenchyma than NAWM. In addition, the parenchyma of active lesions also showed a higher density of these lymphocytes than the parenchyma of chronic inactive lesions (p = 0.041). The number of B cells in the parenchyma was similar when I and A or A and C lesions were compared. In summary, all types of MS lesions showed higher number B lymphocytes than NAWM, as a consequence of the increased number in both compartments, perivascular space and parenchyma. The analysis of the meninges around the NAWM or demyelinated areas only demonstrated significant differences in the number of B lymphocytes between AC lesions and NAWM (p = 0.031) (Fig. 8g).
All type of lesions also showed a higher number of plasma cells than NAWM consequence of the increased number of these cells in the perivascular space and parenchyma (Table 1). We observed an increased number of plasma cells in the perivascular space of I (p = 0.008), A (p = 0.002) and C (p = 0.026) lesions when compared with NAWM. In the parenchyma, I (p = 0.036), A (p = 0.02) and C (p=0.005) lesions also showed increased number of these cells than NAWM. No statistical significance difference in the number of plasma cells was detected among the different type of lesions. I (p = 0.019) and A (p = 0.030) lesions showed a higher number of plasma cells in the meninges than NAWM (Fig. 8h).
To study the role of B cells and plasma cells in the development of the lesions, we also compared the number of B lymphocytes and plasma cells in different type of lesions. I and A lesions showed a similar number of B and plasma cells in both areas, in perivascular spaces and parenchyma. However, the number of B cells was higher than the number of plasma cells lesions in both compartments of C lesions, in perivascular spaces (p < 0.003) and meninges (p < 0.012).
Relation Between the Presence of Antibody Deposits and the Number of B Lymphocytes and Plasma Cells in the Central Nervous System
To clarify the source of IgG and IgM deposits observed in MS patients, we analysed the presence of B lymphocytes and plasma cells in the lesions (parenchyma and perivascular spaces) and in the meninges surrounding the brain areas analysed regarding the presence of immunoglobulin deposits (Table 2).
Lesions showing IgG deposits had a higher number of B lymphocytes in the perivascular space (p = 0.002), parenchyma (p < 0.0001) and meninges (p = 0.029) than those areas without deposits. No significant differences in the number of B lymphocytes were detected when the meninges were analysed (Fig. 9a). IgG-containing areas also contained a higher number of plasma cells, in the perivascular spaces (p < 0.0001) and parenchyma (p = 0.001) compared with IgG-negative ones. No significant differences were detected between negative and positive IgG areas in the number of plasma cells in the meninges (Fig. 9b).

Relation between the number of B cells or plasma cells and the presence of IgG or IgM deposits. Bars represent mean ± 2xSEM (standard error of the mean). Right axis represent the number of cells in the lesions and left axis represent the number of cells in the meninges. a Number of B cells (CD79 +) in lesions with (IgG+) or without (IgG−) IgG deposits. b Number of CD79+ positive cells in lesions with (IgM+) or without (IgM−) IgM deposits. c Number of plasma cells (CD138 +) in IgG− and IgG+ lesions. d Number of CD138 cells in IgM− and IgM+ lesions. NAWM: normal appearing white matter. CI chronic inactive lesion, CA chronic active lesion, AC acute lesion, PV perivascular space, PAR parenchyma, MEN meninges
A similar number of B cells was observed when negative and positive IgM lesions were analysed (Fig. 9c). However, IgM-positive lesions showed a higher number of plasma cells in the perivascular space (p = 0.001), parenchyma (p = 0.003) and meninges (p = 0.015) than those without IgM (Fig. 9d).
Discussion
Intrathecal IgG synthesis is a hallmark for the diagnosis of MS (Andersson et al. 1994; Masjuan et al. 2006; Poser et al. 1983; Villar et al. 2005a) and oligoclonal IgM antibodies against lipids restricted to cerebrospinal fluid is an unfavourable prognostic marker of the disease (Villar et al. 2005b,2008). We observed previously IgG and IgM deposits on oligodendrocytes and axons located in demyelinating lesions of MS patients and on oligodendrocytes in the NAWM. Antibody deposits co-localized with complement and foamy macrophages (Sádaba et al. 2012). All these data support the suggestion that antibodies are a main mechanism of tissue damage in MS.
Nevertheless, it cannot be excluded that other mechanisms may be involved in this disease, for example, oligodendrocyte apoptosis (Lucchinetti et al. 2000) or oxidative stress (Bizzozero et al. 2005; Haider et al. 2011). Mitochondrial dysfunction that is related with axonal (Dutta et al. 2006; Mahad et al. 2009) and oligodendrocyte (Haider et al. 2011; Mahad et al. 2008), damage could play a main role in both cases. Different findings provide evidence that the oxidation of proteins or lipids could result in the generation of neo-epitopes, which in turn could lead to an immune response (Binder et al. 2002). About 40% of MS patients show IgM antibodies to phosphatidylcholine in the cerebrospinal fluid and in atherosclerosis IgG and IgM antibodies that recognize OxLDL (Tsimikas et al. 2007) have been described.
In addition, oxidative stress and humoral immune responses are not confined to MS among CNS diseases. Increased oxidative stress has been detected in CNS tissue from patients with ALS(Kiernan et al. 2011; Rosen et al. 1993), FTD(Martínez et al. 2008) and PD (Jenner et al. 1992), and antibodies to components of the CNS have been detected in patients with ALS(Engelhardt et al. 1995; Kimura et al. 1994), and PD (Chen et al. 1998).
Consequently, we proposed to analyse the relation between antibodies and oxidative stress and their role in MS patients. We also aimed to investigate their specificity, comparing MS with classical neurodegenerative diseases (ND).
We did not observe lipid oxidation in brain samples from controls without neurological diseases. However, we detected oxidized phosphatidylcholine in all MS patients analysed. Oxidative stress was independent of the clinical disease type or the disease duration. We did not observe lipid oxidation in chronic inactive lesions, but we detected oxidized phosphatidylcholine in chronic active (mainly in the edge of the lesion) and acute lesions. Contrary to previous observations when the presence of IgG of IgM in the CNS was analysed (Sádaba et al. 2012), we did not detect lipid oxidation in NAWM samples from MS patients. All these data suggest that oxidative stress is related to lesion activity, corroborating previous results (Haider et al. 2011). Lipid oxidation was observed in oligodendrocytes, foamy macrophages and axons located in lesions. These results corroborate those published by Haider et al. (2011) who observed oxidized phospholipids in the cytoplasm of oligodendrocytes located in active multiple sclerosis lesions, but we also discovered axons containing oxidised lipids.
We did not detect oxidative stress in samples from patients with PD. Although the number of samples analysed was not very high, this observation is consistent with a recent study describing increased oxidation in serum but not in cerebrospinal fluid of these patients (Wei et al. 2018). These results indicate that oxidative stress is unlikely to be a main mechanism in most cases of PD (Moore et al. 2005). Further studies are required to extend these observations.
However, we observed oxidative stress affecting axons in samples from ALS.
We also observed oxidized lipids on axons in FTD patients, data consistent with biochemical analysis (Martínez et al. 2008).
To clarify the specificity of the IgG and IgM deposits observed in MS patients (Barnett and Prineas 2004; Gay et al. 1997; Lucchinetti et al. 2000; Storch et al. 1998; Sádaba et al. 2012) we analysed these immunoglobulins in patients with neurodegenerative diseases.
We did not detect IgM in any case with neurodegenerative disease, demonstrating that this immunoglobulin is specific to MS patients. In MS cases we observed IgG on oligodendrocytes and axons. However, we detected IgG on neurons in samples from ALS cases, corroborating previous results (Engelhardt and Appel 1990). In samples from FTD individuals, we detected IgG deposits on cells resembling astrocytes. In summary, IgG deposits on oligodendrocytes are specific to MS patients when these individuals were compared with those suffering from classical neurodegenerative disease.
We have described above the presence of oxidised lipids on oligodendrocytes and axons in samples from MS patients, a similar distribution pattern to that observed when IgG and IgM was analysed previously (Sádaba et al. 2012). Consequently, we explored the relation between oxidative stress and the humoral immune response. We detected oxidative stress in lesions showing antibodies as well as in samples in which antibodies were not detected. Moreover, double-immunofluorescence showed that lipid oxidation did not co-localize with IgG or IgM. We have only analysed lipid oxidation but previous studies have shown that cells showing lipid oxidation are also exposed to the oxidation of different molecules (Haider et al. 2011). These data suggest that, in this case, a humoral immune response is not the main factor that elicits the production of free radicals, or in reverse, the oxidative stress does not trigger the humoral immune response either.
We also studied the role of oxidative stress and antibodies in axonal damage. We did not detect evidences of axonal damage in NAWM samples from MS patients or in the normal control group as previously described (Ferguson et al. 1997). We detected APP positive damaged axons in chronic and acute lesions but it was not solely related to inflammation because we detected positive axons for APP in the centre of chronic active lesions, a finding that differs from a previously published study (Ferguson et al. 1997). Probably, the discrepancy is for the reason that we used a highly sensitive immunohistochemistry technique. This finding supports the suggestion that humoral immune responses can trigger damage to axons because in these areas of chronic active plaques there is not a high number of inflammatory cells.
Next, we studied the role of oxidative stress and antibodies in oligodendrocyte and axonal damage. Double-immunofluorescence did not demonstrate an association between lipid oxidation and oligodendrocyte damage, suggesting that oxidative stress does not trigger demyelination. Probably, it is a secondary mechanism consequent upon the inflammatory process and cell injury. However, IgG or IgM-positive oligodendrocytes were also positive for a cell marker used to detect cell death. This evidence suggests that antibody could play a main role in the development of new forming lesions as previously suggested (Barnett and Prineas 2004; Gay et al. 1997).
Double-immunofluorescence also revealed that APP positive axons did not present oxidized phosphatidylcholine. Surprisingly, we did not detect IgG deposits on damaged axons, but APP positive axons were also IgM positive, indicating that these antibodies, but not IgG or oxidative stress, play a main role in axonal damage. These data clarify the poor outcome of MS patients with oligoclonal IgM bands in the cerebrospinal fluid (Villar et al. 2002a, 2002b, 2003).
Antibodies can trigger oligodendrocyte and axonal damage because they activate the complement cascade and macrophages, both of which are present in the lesions of these patients (Sádaba et al. 2004).
However, the pathological mechanism concerning axonal damage in patients without IgM remains to be elucidated. Regarding this, demyelination induces a reorganization of Na+ channels along the axon, which cause increased energy demand (England et al. 1990). However, mitochondrial damage has been described in the lesions (Mahad et al. 2008,2009) which could explain the decreased ATP production observed in samples from MS patients (Sádaba et al. 2016).
Contrary to MS cases, this study demonstrates that increased oxidative stress was observed in ALS and correlated with axonal damage. These findings represent, to our knowledge, the first evidence of the pathological role of this factor in ALS, at least in some patients. We realize that this observation is preliminary and needs to be confirmed in greater numbers of cases. Similar results were obtained when samples from FTD were analysed, and oxidative stress was related with axonal damage.
To study more deeply the role of the humoral immune response we analysed the number of B lymphocytes and plasma cells in the different MS lesions.
The number of B cells in the meninges surrounding the lesions was similar among I, A and NAWM, but, the highest number of B lymphocytes observed in C lesions was associated with an increased number of these cells in the meninges surrounding these type of lesion. In addition, the number of B lymphocytes was higher than the number of plasma cells in the lesions and meninges of C lesions. All these data demonstrate that the inflammatory demyelinating phase of MS lesions is related with the number of B lymphocytes. Moreover, meninges can be a main source of B lymphocytes during the inflammatory phase, corroborating previous results (Lovato et al. 2011; Obermeier et al. 2011). However, I and A lesions showed a high number of plasma cells in the lesions, especially in the perivascular spaces. As I lesions do not show inflammatory infiltrate (macrophages or T lymphocytes), the presence of plasma cells could be a main mechanism to maintain the lesions along the time. In addition, our findings support the important role of the perivascular space as a reservoir of plasma cells in A and I lesions.
The main mechanism, as described above, to provoke the tissue damage is the production of antibodies. Regarding this, we observed that IgG positive lesions showed a higher number of B lymphocytes in the lesions and meninges than those negative for this antibody. Moreover, IgG positive lesions also had a higher number of plasma cells in the lesions.
In line with this, immunoglobulin recombination was described in the B lymphocytes of the CNS (Baranzini et al. 1999), and B cell maturation was described as taking place in lymphoid nodules of the central nervous (Corcione et al. 2004) system and also in follicle-like structures in the meninges (Magliozzi et al. 2007).
IgM-positive lesions also showed a higher number of plasma cells in the meninges than IgM negative lesions. These data are relevant to previous results demonstrating a similar oligoclonal bands pattern in the cerebrospinal fluid during the evolution of the disease (Villar et al. 2008). Taking into account that IgM antibodies are related with axonal damage, these data explain that increased numbers of plasma cells in cerebrospinal fluid are related to tissue damage.
Of particular interest, these data are clinically relevant because they explain the results obtained with immunosuppressant treatments. Natalizumab decreases the number of relapses and the progression of the disability (Polman et al. 2006) and the therapy with anti-CD20 also decreases the number of lesions (Hauser et al. 2008). But they do not cure the disease, probably because they do not eliminate the production of intrathecal IgG or IgM antibodies (Piccio et al. 2010; Villar et al. 2012). For these reasons, it would be of great interest to develop a therapy against plasma cells.
In summary, our work draws attention to the main role of IgG and IgM in newly forming lesions in MS. In addition, we provide a novel role for IgM antibodies in axonal damage, which may account for patients with IgM antibody in cerebrospinal fluid having a poor prognosis (Villar et al. 2002a, b, 2003). However, we obtained preliminary evidence that oxidative stress is related to axonal damage in ALS. Thus, this study demonstrates differing pathophysiology between MS and the classical neurodegenerative diseases of ALS and FTD. It would be of great interest to clarify the causes of these differing pathological mechanisms in order to provide novel therapeutic strategies to limit neurological disability in all these patients.
Data Availability
The corresponding authors will provide anonymized data of this study on reasonable request from any qualified investigator, following relevant data protection regulations.
References
Andersson M, Alvarez-Cermeño J, Bernardi G, Cogato I, Fredman P, Frederiksen J, Fredrikson S, Gallo P, Grimaldi LM, Grønning M (1994) Cerebrospinal fluid in the diagnosis of multiple sclerosis: a consensus report. J Neurol Neurosurg Psychiatry 57:897–902. https://doi.org/10.1136/jnnp.57.8.897
Baranzini SE, Jeong MC, Butunoi C, Murray RS, Bernard CC, Oksenberg JR (1999) B cell repertoire diversity and clonal expansion in multiple sclerosis brain lesions. J Immunol 163:5133–5144
Barnett MH, Prineas JW (2004) Relapsing and remitting multiple sclerosis: pathology of the newly forming lesion. Ann Neurol 55(4):458–468
Binder CJ, Chang MK, Shaw PX, Miller YI, Hartvigsen K, Dewan A, Witztum JL (2002) Innate and acquired immunity in atherogenesis. Nat Med 8:1218–1226. https://doi.org/10.1038/nm1102-1218
Bizzozero OA, DeJesus G, Callahan K, Pastuszyn A (2005) Elevated protein carbonylation in the brain white matter and gray matter of patients with multiple sclerosis. J Neurosci Res 81:687–695. https://doi.org/10.1002/jnr.20587
Breij EC, Brink BP, Veerhuis R, van den Berg C, Vloet R, Yan R, Dijkstra CD, van der Valk P, Bö L (2008) Homogeneity of active demyelinating lesions in established multiple sclerosis. Ann Neurol 63:16–25. https://doi.org/10.1002/ana.21311
Chen S, Le WD, Xie WJ, Alexianu ME, Engelhardt JI, Siklós L, Appel SH (1998) Experimental destruction of substantianigra initiated by Parkinson disease immunoglobulins. Arch Neurol 55:1075–1080. https://doi.org/10.1001/archneur.55.8.1075
Corcione A, Casaza S, Ferretti E, Giunti D, Zappia E, Pistorio A, Gambini C, Mancardi GL, Uccelli A, Pistoia V (2004) Recapitulation of B cell differentiation in the central nervous system of patients with multiple sclerosis. ProcNatlAcadSci USA 101:11064–11069. https://doi.org/10.1073/pnas.0402455101
Cross AH, Manning PT, Keeling RM, Schmidt RE, Misko TP (1998) Peroxynitrite formation within the central nervous system in active multiple sclerosis. J Neuroimmunol 88:45–56. https://doi.org/10.1016/s0165-5728(98)00078-2
Diaz-Sanchez M, Williams K, DeLuca GC, Esiri MM (2006) Protein co-expression with axonal injury in multiple sclerosis plaques. ActaNeuropathol 111:289–299. https://doi.org/10.1007/s00401-006-0045-0
Dutta R, McDonough J, Yin X, Peterson J, Chang A, Torres T, Gudz T, Macklin WB, Lewis DA, Fox RJ et al (2006) Mitochondrial dysfunction as a cause of axonal degeneration in multiple sclerosis patients. Ann Neurol 59:478–489. https://doi.org/10.1002/ana.20736
Engelhardt JI, Appel SH (1990) IgG reactivity in the spinal cord and motor cortex in amyotrophic lateral sclerosis. Arch Neurol 47:1210–1216. https://doi.org/10.1001/archneur.1990.00530110068019
Engelhardt JI, Siklós L, Kömüves L, Smith RG, Appel SH (1995) Antibodies to calcium channels from ALS patients passively transferred to mice selectively increase intracellular calcium and induce ultrastructural changes in motoneurons. Synapse 20:185–199. https://doi.org/10.1002/syn.890200302
England JD, Gamboni F, Levinson SR, Finger TE (1990) Changed distribution of sodium channels along demyelinated axons. ProcNatlAcadSci USA 87:6777–6780. https://doi.org/10.1073/pnas.87.17.6777
Esiri M (1977) Immunoglobulin-containing cells in multiple-sclerosis plaques. Lancet 310:478–480. https://doi.org/10.1016/S0140-6736(77)91603-8
Ferguson B, Matyszak MK, Esiri MM, Perry VH (1997) Axonal damage in acute multiple sclerosis lesions. Brain 120:393–399. https://doi.org/10.1093/brain/120.3.393
Fischer MT, Sharma R, Lim JL, Haider L, Frischer JM, Drexhage J, Mahad D, Bradl M, Van Horssen J, Lassmann H (2012) NADPH oxidase expression in active multiple sclerosis lesions in relation to oxidative tissue damage and mitochondrial injury. Brain 135:886–899. https://doi.org/10.1093/brain/aws012
Fischer MT, Wimmer I, Höftberger R, Gerlach S, Haider L, Zrzavy T, Hametner S, Mahad D, Binder CJ, Krumbholz M et al (2013) Disease-specific molecular events in cortical multiple sclerosis lesions. Brain 136:1799–1815. https://doi.org/10.1093/brain/awt110
Gay FW, Drye TJ, Dick GWA, Esiri MM (1997) The application of multifactorial cluster analysis in the staging of plaques in early multiple sclerosis: identification and characterization of the primary demyelinating lesion. Brain 120:1461–1483. https://doi.org/10.1093/brain/120.8.1461
Haas J, Bekeredjian-Ding I, Milkova M, Balint B, Schwarz A, Korporal M, Jarius S, Fritz B, Lorenz HM, Wildemann B (2011) B cells undergo unique compartmentalized redistribution in multiple sclerosis. J Autoimmun 37:289–299. https://doi.org/10.1016/j.jaut.2011.08.003
Haider L, Fischer MT, Frischer JM, Bauer J, Hoftberger R, Botond G, Esterbauer H, Binder CJ, Witztum JL, Lassmann H (2011) Oxidative damage in multiple sclerosis lesions. Brain 134:1914–1924. https://doi.org/10.1093/brain/awr128
Hauser SL, Waubant E, Arnold DL, Vollmer T, Antel J, Fox R, Bar-Or A, Panzara M, Sarkar N, Agarwal S et al (2008) B-cell depletion with rituximab in relapsing-remitting multiple sclerosis. N Engl J Med 358:676–688. https://doi.org/10.1056/nejmoa0706383
Ireland SJ, Blazek M, Harp CT, Greenberg B, Frohman EM, Davis LS, Monson NL (2012) Antibody-independent B cell effector functions in relapsing remitting multiple sclerosis: clues to increased inflammatory and reduced regulatory B cell capacity. Autoimmunity 45:400–414. https://doi.org/10.3109/08916934.2012.665529
Irwin DJ (2016) Tauopathies as clinicopathological entities. Parkinsonism RelatDisord 22(Suppl 1):S29-33. https://doi.org/10.1016/j.parkreldis.2015.09.020
Jenner P, Dexter DT, Sian J, Schapira AH, Marsden CD (1992) Oxidative stress as a cause of nigral cell death in Parkinson’s disease and incidental lewy body disease the royal Kings and Queens Parkinson’s disease research group. Ann Neurol 32(Suppl):S82-87. https://doi.org/10.1002/ana.410320714
Kankaanpää J, Turunen SP, Moilanen V, Hörkkö S, Remes AM (2009) Cerebrospinal fluid antibodies to oxidized LDL are increased in Alzheimer’s disease. Neurobiol Dis 33:467–472. https://doi.org/10.1016/j.nbd.2008.12.001
Kiernan MC, Vucic S, Cheah BC, Turner MR, Eisen A, Hardiman O, Burrell JR, Zoing MC (2011) Amyotrophic lateral sclerosis. Lancet 377:942–955. https://doi.org/10.1016/s0140-6736(10)61156-7
Kim SH, Kook MC, Shin YK, Park SH, Song HG (2004) Evaluation of antigen retrieval buffer systems. J MolHistol 35:409–416. https://doi.org/10.1023/B:HIJO.0000039854.17808.e0
Kimura F, Smith RG, Delbono O, Nyormoi O, Schneider T, Nastainczyk W, Hofmann F, Stefani E, Appel SH (1994) Amyotrophic lateral sclerosis patient antibodies label Ca2+ channel alpha 1 subunit. Ann Neurol 35:164–171. https://doi.org/10.1002/ana.410350207
Liu JS, Zhao ML, Brosnan CF, Lee SC (2001) Expression of inducible nitric oxide synthase and nitrotyrosine in multiple sclerosis lesions. Am J Pathol 158:2057–2066. https://doi.org/10.1016/s0002-9440(10)64677-9
Lovato L, Willis SN, Rodig SJ, Caron T, Almendinger SE, Howell OW, Reynolds R, O’Connor KC, Hafler DA (2011) Related B cell clones populate the meninges and parenchyma of patients with multiple sclerosis. Brain 134:534–541. https://doi.org/10.1093/brain/awq350
Lucchinetti CF, Bruck W, Rodriguez M, Lassmann H (1996) Distinct patterns of multiple sclerosis pathology indicates heterogeneity on pathogenesis. Brain Pathol 6:259–274. https://doi.org/10.1111/j.1750-3639.1996.tb00854.x
Lucchinetti CF, Brück W, Parisi JE, Scheithauer B, Rodriguez M, Lassmann H (2000) Heterogenity of multiple sclerosis lesions: implication for the pathogenesis of demyelination. Ann Neurol 47:707–717. https://doi.org/10.1002/1531-8249(200006)47:6%3C707::aid-ana3%3e3.0.CO;2-q
Magliozzi R, Howell O, Vora A, Serafini B, Nicholas R, Puopolo M, Reynolds R, Aloisi F (2007) Meningeal B-cell follicles in secondary progressive multiple sclerosis associate with early onset of disease and severe cortical pathology. Brain 130:1089–1104. https://doi.org/10.1093/brain/awm038
Mahad D, Ziabreva I, Lassmann H, Turnbull D (2008) Mitochondrial defects in acute multiple sclerosis lesions. Brain 131:1722–1735. https://doi.org/10.1093/brain/awn105
Mahad DJ, Ziabreva I, Campbell G, Lax N, White K, Hanson PS, Lassmann H, Turnbull DM (2009) Mitochondrial changes within axons in multiple sclerosis. Brain 132:1161–1174. https://doi.org/10.1093/brain/awp046
Martínez A, Carmona M, Portero-Otin M, Naudí A, Pamplona R, Ferrer I (2008) Type-dependent oxidative damage in frontotemporal lobar degeneration: cortical astrocytes are targets of oxidative damage. J NeuropatholExpNeurol 67:1122–1136. https://doi.org/10.1097/NEN.0b013e31818e06f3
Masjuan J, Alvarez-Cermeño JC, García-Barragán N, Díaz-Sánchez M, Espiño M, Sádaba MC, González-Porqué P, Martínez San Millán J, Villar LM (2006) Clinically isolated syndromes: a new oligoclonal band test accurately predicts conversion to MS. Neurology 66:576–578. https://doi.org/10.1212/01.wnl.0000198253.35119.83
McGeer PL, McGeer EG, Kawamata T, Yamada T, Akiyama H (1991) Reactions of the immune system in chronic degenerative neurological diseases. Can J NeurolSci 18:376–379. https://doi.org/10.1017/S0317167100032479
Moore DJ, West AB, Dawson VL, Dawson TM (2005) Molecular pathophysiology of Parkinson’s disease. Annu Rev Neurosci 28:57–87. https://doi.org/10.1146/annurev.neuro.28.061604.135718
Obermeier B, Lovato L, Mentele R, Brück W, Forne I, Imhof A, Lottspeich F, Turk KW, Willis SN, Wekerle H et al (2011) Related B cell clones that populate the CSF and CNS of patients with multiple sclerosis produce CSF immunoglobulin. J Neuroimmunol 233:245–248
Piccio L, Naismith RT, Trinkaus K, Klein RS, Parks BJ, Lyons JA, Cross AH (2010) Changes in B- and T-lymphocyte and chemokine levels with rituximab treatment in multiple sclerosis. Arch Neurol 67:707–714. https://doi.org/10.1001/archneurol.2010.99
Polman CH, O’Connor PW, Havrdova E, Hutchinson M, Kappos L, Miller DH, Phillips JT, Lublin FD, Giovannoni G, Wajgt A et al (2006) A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med 354:899–910. https://doi.org/10.1056/nejmoa044397
Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA, Ebers GC, Johnson KP, Sibley WA, Silberberg DH, Tourtellotte WW (1983) New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Ann Neurol 13:227–231. https://doi.org/10.1002/ana.410130302
Prineas JW (1979) Multiple sclerosis: presence of lymphatic capillaries and lymphoid tissue in the brain and spinal cord. Science 203:1123–1125. https://doi.org/10.1126/science.424741
Rosen DR, Siddique T, Patterson D, Figlewicz DA, Sapp P, Hentati A, Donaldson D, Goto J, O’Regan JP, Deng HX (1993) Mutations in Cu/Zn superoxide dismutase gene are associated with familial amyotrophic lateral sclerosis. Nature 362:59–62. https://doi.org/10.1038/362059a0
Serafini B, Rosicarelli B, Magliozzi R, Stigliano E, Aloisi F (2004) Detection of ectopic B-cell follicles with germinal centers in the meninges of patients with secondary progressive multiple sclerosis. Brain Pathol 14:164–174. https://doi.org/10.1111/j.1750-3639.2004.tb00049.x
Stadelmann C, Wegner C, Brück W (2011) Inflammation, demyelination and degeneration - recent insights from MS pathology. BiochimBiophysActa 1812:275–282. https://doi.org/10.1016/j.bbadis.2010.07.007
Storch MK, Piddlesden S, Haltia M, Iivanainen M, Morgan P, Lassmann H (1998) Multiple sclerosis: in situ evidence for antibody- and complement- mediated demyelination. Ann Neurol 43:465–471. https://doi.org/10.1002/ana.410430409
Sádaba MC, González Porqué P, Masjuan J, Alvarez-Cermeño JC, Bootello A, Villar LM (2004) An ultrasensitive method for the detection of oligoclonalIgG bands. J Immunol Methods 284:41–145. https://doi.org/10.1016/j.jim.2003.09.018
Sádaba MC, Martín-Estal I, Puche JE, Castilla-Cortázar I (2016) Insulin-like growth factor 1 (IGF-1) therapy: mitochondrial dysfunction and diseases. BiochimBiophysActa 1862:1267–1278. https://doi.org/10.1016/j.bbadis.2016.03.010
Sádaba MC, Tzartos J, Paíno C, García-Villanueva M, Alvarez-Cermeño JC, Villar LM, Esiri MM (2012) Axonal and oligodendrocyte-localized IgM and IgG deposits in MS lesions. J Neuroimmunol 247:86–94. https://doi.org/10.1016/j.jneuroim.2012.03.020
Tsimikas S, Brilakis ES, Lennon RJ, Miller ER, Witztum JL, McConnell JP, Kornman KS, Berger PB (2007) Relationship of IgG and IgM autoantibodies to oxidized low density lipoprotein with coronary artery disease and cardiovascular events. J Lipid Res 48:425–433. https://doi.org/10.1194/jlr.m600361-jlr200
Tzartos JS, Friese MA, Craner MJ, Palace J, Newcombe J, Esiri MM, Fugger L (2008) Interleukin-17 production in central nervous system-infiltrating T Cells and glial cells is associated with active disease in multiple sclerosis. Am J Pathol 172:146–155. https://doi.org/10.2353/ajpath.2008.070690
Villar L, García-Barragán N, Espiño M, Roldán E, Sádaba M, Gómez-Rial J, González-Porqué P, Alvarez-Cermeño J (2008) Influence of oligoclonalIgM specificity in multiple sclerosis disease course. MultScler 14:183–187. https://doi.org/10.1177/1352458507082046
Villar LM, García-Sánchez MI, Costa-Frossard L, Espiño M, Roldán E, Páramo D, Lucas M, Izquierdo G, Álvarez-Cermeño JC (2012) Immunological markers of optimal response to natalizumab in multiple sclerosis. Arch Neurol 69:191–197
Villar LM, Masjuan J, González-Porqué P, Plaza J, Sádaba MC, Roldán E, Bootello A, Alvarez-Cermeño JC (2002a) IntrathecalIgM synthesis in neurologic diseases: relationship with disability in MS. Neurology 58:824–826. https://doi.org/10.1212/wnl.58.5.824
Villar LM, Masjuan J, González-Porqué P, Plaza J, Sádaba MC, Roldán E, Bootello A, Alvarez-Cermeño JC (2002b) IntrathecalIgM synthesis predicts the onset of new relapses and a worse disease course in MS. Neurology 59:555–559. https://doi.org/10.1212/wnl.59.4.555
Villar LM, Masjuan J, González-Porqué P, Plaza J, Sádaba MC, Roldán E, Bootello A, Alvarez-Cermeño JC (2003) IntrathecalIgM synthesis is a prognostic factor in multiple sclerosis. Ann Neurol 53:222–226. https://doi.org/10.1002/ana.10441
Villar LM, Masjuan J, Sádaba MC, González-Porqué P, Plaza J, Bootello A, Alvarez-Cermeño JC (2005a) Early differential diagnosis of multiple sclerosis using a new oligoclonal band test. Arch Neurol 62:574–577. https://doi.org/10.1001/archneur.62.4.574
Villar LM, Sádaba MC, Roldán E, Masjuan J, González-Porqué P, Villarrubia N, Espiño M, García-Trujillo JA, Bootello A, Alvarez-Cermeño JC (2005b) Intrathecal synthesis of oligoclonalIgM against myelin lipids predicts an aggressive disease course in MS. J Clin Invest 115:187–194. https://doi.org/10.1172/jci22833
Vladimirova O, O’Connor J, Cahill A, Alder H, Butunoi C, Kalman B (1998) Oxidative damage to DNA in plaques of MS brains. MultScler (Houndmills, Basingstoke, England) 4:413–418. https://doi.org/10.1177/135245859800400503
Wei Z, Li X, Liu Q, Cheng Y (2018) Oxidative stress in Parkinson’s disease: a systematic review and meta-analysis. Front MolNeurosci 11:236. https://doi.org/10.3389/fnmol.2018.00236
Zhang Y, Da RR, Hilgenberg LG, Tourtellotte WW, Sobel RA, Smith MA, Olek M, Nagra R, Sudhir G, van den Noort S et al (2005) Clonal expansion of IgA-positive plasma cells and axon-reactive antibodies in MS lesions. J Neuroimmunol 167:120–130. https://doi.org/10.1016/j.jneuroim.2005.05.006
Acknowledgements
We acknowledge the Oxford Brain Bank, supported by the Medical Research Council (MRC), Brains for Dementia Research (BDR) (Alzheimer Society and Alzheimer Research UK), Autistica UK and the NIHR Oxford Biomedical Research; Banco de Tejidos CIEN, Instituto Carlos III and Departamento de Anatomía de la Facultad de Medicina de la Universidad San Pablo CEU for providing human tissue; Dr. José Paredes, Dr. Silvano Heras and Dr Francisco J. García for providing tissue samples and Angelica Acebedo and Susana Arahuetes for technical help.
Funding
This work was supported by grants from the Instituto de Medicina Molecular Aplicada, Universidad San Pablo CEU (USP-BS-PPC16/2012 and MEMERG-1) and grant from the Universidad San Pablo CEU-Banco Santander (PI14/01620) to Dra. Úrsula Muñoz and by UK National Institute for Health Research (NIHR) through the Oxford Biomedical Research Centre (UK) to Professor Margaret Esiri. Cristina Sebal was supported by a fellowship grant from the Instituto de Medicina Molecular Aplicada, Universidad San Pablo CEU (Spain).
Author information
Authors and Affiliations
Contributions
UM, MCS and ES: conception and design of the study; CS, JT and CSl: acquisition and analysis of data and MCS, UM, ME, and ES: drafting a significant portion of the manuscript or figures.
Corresponding authors
Ethics declarations
Conflict of interest
Nothing to report.
Ethical Approval
The study was approved by the Ethical Committee of the Universidad San Pablo CEU (113/16/05). All the patients signed Informed consent. The donation of samples were approved by Committee of the Universidad San Pablo CEU, Instituto de Salud Carlos III (ISCIII) and Oxford University.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Muñoz, U., Sebal, C., Escudero, E. et al. Main Role of Antibodies in Demyelination and Axonal Damage in Multiple Sclerosis. Cell Mol Neurobiol 42, 1809–1827 (2022). https://doi.org/10.1007/s10571-021-01059-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10571-021-01059-6