
Abstract
Aortic valve sclerosis (AVS) is defined as calcified and thickened aortic leaflets without restriction of leaflet motion. We have not found any studies that previously assessed the effect of AVS on myocardial functions with three dimensional-speckle tracking echocardiography (3D-STE). Therefore, we aimed to identify any early changes in left atrial (LA) myocardial dynamics and/or left ventricular (LV) systolic functions in patients with AVS using 3D-STE. Seventy-five patients with AVS and 80 age- and gender-matched controls were enrolled into the study. The baseline clinical characteristics of the study patients were recorded. Conventional 2D echocardiographic and 3D-STE analyses were performed. The LV-global longitudinal strain (LV-GLS) and LV-global circumferential strain (LV-GCS) were significantly decreased in the AVS (+) group than in the control group (p < 0.001 and p = 0.013, respectively). In multivariate logistic regression analysis; LV-GLS (p < 0.001, odds ratio (OR) = 3.16, 95% confidence interval (CI) 1.42–5.63) and Triglyceride (TG) (p = 0.033, OR = 1.29, 95% CI 1.11–1.72) were found to be independent predictors of AVS. ROC analysis was performed to find out the ideal LV-GLS cut-off value for predicting the AVS. A LV-GLS value of > − 18 has 85.8% sensitivity, 67.5% specificity for the prediction of the AVS. Our results support that subjects with AVS may have subclinical LV deformation abnormalities even though they have not LV pressure overload. According to our findings, patients with AVS should be investigated in terms of atherosclerotic risk factors, their dysmetabolic status should be evaluated and closely followed up for their progression to calcific aortic stenosis.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Aortic valve sclerosis (AVS) is defined as thickened and calcified aortic valvules without restriction of leaflet motion [1]. This abnormality occurs in 30% of people who are older than 65 years of age [2]. Inflammatory process, oxidation, endothelial damage, lipid accumulation, extracellular matrix degradation, and calcification are involved in the pathogenesis of AVS [3]. AVS is a common echocardiographic finding, and it has been considered a progressive process with aging [4, 5]. However, current several data suggest that sclerosis of aortic valve is not simply a consequence of aging, but is also associated with an increased risk of acute coronary syndrome, ischemic heart disease, congestive heart failure, cerebrovascular disease, and cardiovascular mortality [6,7,8]. So, it is considered an atherosclerosis-like process [9]. Although sclerotic aortic valve does not cause aortic transvalvular pressure gradient, its effects on outcomes in cardiovascular diseases are not clear.
Left ventricular ejection fraction (LVEF) as a conventional echocardiographic parameter is routinely used to evaluate the left ventricular (LV) myocardial systolic function in clinical practice; but to detect the early-stage of myocardial dysfunction, it is not sensitive enough. In recent years, advanced strain echocardiography techniques provides reliable and extensive assessment of myocardial dynamics. Three dimensional-speckle tracking echocardiography (3D-STE) gives clinicians a new noninvasive tool in characterizing and understanding preclinical myocardial involvement via 3D strain analysis [10]. 3D-STE is considered a validated technique for LA and LV quantification as compared to two dimensional-speckle tracking echocardiography (2D-STE) [11, 12].
Aortic stenosis (AS) leads to adverse LV remodeling and myocardial dysfunction due to LV pressure overload. But, the effects of AVS on LA mechanics and LV dynamics are uncertain. To identify the early subclinical LV myocardial dysfunction in subjects with AS, several impressive clinical studies have been done using 2D-STE and 3D-STE. However, we couldn’t find any studies that previously evaluated the effect of AVS on myocardial functions with 3D-STE. Therefore, we aimed to identify if any early alterations in LA myocardial dynamics and/or LV functions in patients with AVS by 3D-STE.
Materials and methods
Study population
A total of 155 subjects who were admitted for routine check-up and examined at outpatient clinics were enrolled into this cross-sectional study between May 2016 and January 2018. The patient group [AVS (+) group] consisted of 75 patients with AVS. The control group [AVS (−) group] included 80 age- and gender-matched healthy subjects. AVS was identified according to criteria described by Otto et al. [3] as non-uniform thickening or spotty calcified areas of the aortic valve leaflets without a significant transvalvular aortic gradient (maximum aortic velocity < 2.5 m/s). The exclusion criteria of the current study were history of atherosclerotic heart diseases (myocardial infarction, percutaneous coronary intervention, and/or coronary artery by-pass graft), rheumatic heart disease, bicuspid aortic valve, aortic and mitral insufficiency due to any cause, significant aortic stenosis, atrial and ventricular arrhythmias, heart failure, cardiac pacemaker, LVEF < 55%, inflammatory and/or infectious diseases, chronic kidney and liver insufficiency, uncontrolled hypertension, thyroid dysfunction, and inadequate image quality for speckle-tracking analysis. The local ethics committee approved the present study. An informed and signed consent form was obtained from all study patients.
2D-echocardiographic and 3D-STE evaluation of LA and LV
2D and 3D-STE assessment of all patients were performed by an experienced cardiologist in the 3D strain analysis. Measurements and data obtaining were based on the recommendations of the American Society of Echocardiography and the European Association of Echocardiography [13]. Echocardiographic evaluations were performed with an easily accessible echocardiographic system (Vivid E9; GE Healthcare, Horten, Norway). Following the recording of 2D images, 3D full-volume data sets of the LA and LV were obtained. In the present study, 12 patients who had poor 3D image quality were excluded from the study. LVEF was obtained automatically with 4D auto LVQ. The stored echocardiographic data were exported to a separate workstation for off-line analysis. The endocardial border of the LV cavity was automatically detected by the software in 3D. If the auto endocardial border detection was judged as inaccurate by the examiner, the left atrial/ventricular endocardial borders were manually adjusted in multiplanar layout with a point-click method, immediately followed by secondary automated refinement of boundary detection according to the results. LV-global longitudinal strain (LV-GLS), LV-global circumferential strain (LV-GCS), LV-global area strain (LV-GAS), and LV-global radial strain (LV-GRS) of the left ventricul were obtained for the strain analyses.
In the current study, to assess the left atrial mechanics; LA reservoir, contractile, and conduit functions were evaluated. The reservoir function of LA was evaluated using the left atrial strain-reservoir (LAS-r), and left atrial emptying fraction (LAEF) in 3D. The contractile function of LA was evaluated using LAS-active: LA strain at the onset time of the P wave, and LAEF-active: (LA volume at the onset time of the P wave − LA minimum volume)/LA volume at the onset time of the P wave. The conduit function of LA was evaluated by using LAS-passive: (LAS-r) – (LAS-active), and LAEF-passive: (LA maximum volume − LA volume at the onset time of the P wave)/LA maximum volume [14].
Measurement reproducibility
The ICC for interobserver comparisons of 3 dimensional left atrial volume, LAS, LAS-active, GLS, GCS, GAS, and GRS were 0.89 (95% CI 0.85–0.92), 0.85 (95% CI 0.82–0.90), 0.91 (95% CI 0.87–0.95), 0.93 (95% CI 0.91–0.96), 0.88 (95% CI 0.85–0.90), 0.84 (95% CI 0.81–0.86), and 0.92 (95% CI 0.89–0.95), while the intraobserver comparisons were 0.87 (95% CI 0.83–0.92), 0.77 (95% CI 0.75–0.81), 0.89 (95% CI 0.86–0.94), 0.93 (95% CI 0.90–0.96), 0.89 (95% CI 0.87–0.92), 0.93 (95% CI 0.89–0.95), and 0.88 (95% CI 0.86–0.92), respectively.
Statistical analysis of the study
For variable analysis, SPSS 25.0 program (IBM Corp., Armonk, NY, USA) was used. Normally distributed parameters were expressed as mean ± standard deviation, and non-normally distributed parameters were expressed as median (minimum–maximum). The categorical variables were expressed in numbers and percentages. The Shapiro–Wilk test was used to examine the homogeneity and normal distribution of the variables. The Independent-Sample T test was used to analyze the parametric variables, and the Mann–Whitney U test was used to analyze nonparametric variables. Pearson chi-square and Fisher Exact tests were tested to compare categorical variables. To identify independent predictors of AVS, multivariate logistic regression analysis was used. To analyze the sensitivities of the strain results to predict the presence of AVS, receiver operator characteristic curves (ROCs) were used. Variables were examined at 95% confidence level. A p-value < 0.05 was considered as statistically significant.
Results
A total of 155 subjects were enrolled into the current study [75 subjects in AVS (+) group and 80 subjects in the AVS (−) group]. The clinical characteristics and laboratory results of the patients are presented in Table 1. The mean age of the study population was 54.9 ± 8.3 years, and 68.3% of the patients were male. The mean BMI was significantly higher in the AVS (+) subjects than in the AVS (−) subjects (p = 0.005). The frequency of HLP was higher in the AVS (+) group than in the controls (p = 0.028), and the mean TG level was significantly higher in the AVS (+) subjects than in the control group (p = 0.002). There were not any significant differences between groups in terms of age, gender, systolic and diastolic blood pressure (BP), smoking, heart rate, fasting glucose, creatinine, TC, LDL-C, HDL-C, and history of HT and DM (Table 1).
Peak transaortic velocity was higher in the AVS (+) patients than the controls (p = 0.007), other than this, there were not any significant differences between the two groups regarding the 2D-echocardiographic results. 2D-echo couldn’t identify differences between the groups in left cardiac chamber size or in parameters of diastolic function (Table 2).
3D strain analysis of the study population
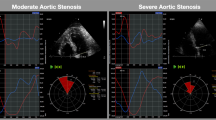
The LA and LV 3D-STE results are shown in Table 3. The LV-GLS and LV-GCS were significantly depressed in the AVS (+) group than in the AVS (−) subjects (p < 0.001 and p = 0.013, respectively) (Table 3; Fig. 1).

Depressed LV-GLS (a) and LV-GCS (b) of a patient with AVS, and sclerotic aortic valve image (c) in parasternal long axis
We couldn’t find any significant differences between the groups regarding LV-GAS, LV-GRS, LAS-r, LAS-active, LAS-passive, LAEF, LAEF-active, and LAEF-passive (p = 0.562, p = 0.255, p = 0.606, p = 0.413, p = 0.388, p = 0.194, p = 0.265, and p = 0.912, respectively) (Table 3).
In multivariate analysis; LV-GLS (p < 0.001, Odds ratio (OR) = 3.16, 95% Confidence interval (CI) 1.42–5.63), and TG (p = 0.033, OR = 1.29, 95% CI 11–1.72) were found to be independent predictors of AVS (Table 4).
To find out the ideal LV-GLS cut-off value for predicting the AVS, ROC analysis was performed. A LV-GLS value of > − 18 has 85.8% sensitivity, 67.5% specificity for the prediction of the AVS [AUC 0.754, (p < 0.001)] (Fig. 2).

ROC curve of LV-GLS for predicting AVS
Discussion
In the current study, using 3D-STE, we aimed to assess whether or not there are LA and/or LV alterations in patients with AVS. The findings of the present study demonstrated that AVS led to impairment of the left ventricular dynamics. To our knowledge, this study is the first to evaluate the LA and LV functions in subjects with AVS by performing 3D-STE.
AS is the third cause of death among cardiovascular diseases, and morbidity with AS has been rapidly increasing for recent years [15, 16]. AS represents the narrowing of the aortic leaflets, which causes an obstruction of the LV outflow and eventually developing symptoms of the disease. Several recent studies suggest that aortic stenosis is not a passive degenerative process resulting from decades of repetitive mechanical stress, but rather an active disease that involves the interaction of several pathways, including chronic inflammation, lipid infiltration, osteoblastic activation, and active mineralization within the aortic valve [17]. AVS, as the initial phase of AS, occurs in the early stages of this active disease. In addition, this process is similar to the pathophysiology of atherosclerosis. It is known that there are subclinical LV myocardial impairments in AS. The question of whether there are subclinical myocardial dysfunctions in AVS, which is at the beginning of this process, directed us to investigate this relationship.
Characterization of myocardial mechanics and dynamics through the echocardiographic assessment of myocardial deformation might provide a more thorough representation of LV contractile function [18]. Alterations in LV contractile function are evaluated as longitudinal, circumferential and radial strain according to the location of myofibrils by strain analysis. In the presence of subendocardial ischemia, LV-GLS is generally the first to be depressed, due to the longitudinal arrangement of LV endocardial myofibers [19]. AS causes LV pressure overload. Progressive increases in afterload lead to LV remodeling and an alteration in coronary flow reserve. These changes may cause subendocardial ischemia and fibrosis and may gradually affect LV myocardial systolic function [20, 21]. In addition, subclinical LV dysfunction may occur in dysmetabolic states such as obesity without manifest left ventricular mechanical stress. Obesity is closely linked to myocardial remodeling accompanied by structural and functional abnormalities. It seems to contribute to inflammation, oxidative stress, apoptosis, interstitial fibrosis, and lipotoxicity. In our study, the presence of subclinical LV myocardial dysfunction in subjects with AVS without LV pressure overload may be due to the accompanying dysmetabolic state.
Previous studies suggest that metabolic syndrome is associated with a twofold increase in the relative risk of coronary heart disease and thromboembolic events [22]. Recently, metabolic syndrome has also been linked to increased prevalence of AVS, and faster progression of calcific AS [23,24,25]. Capoulade et al. examined the relationship between metabolic syndrome and progression of aortic stenosis, and also the effects of aging and statin treatment on aortic stenosis progression [26]. They demonstrated that metabolic syndrome is an independent predictor of faster AS progression, with more pronounced impact in younger patients. Considering the components of the metabolic syndrome, in our study, we found that the mean BMI was significantly higher in the AVS (+) subjects than in the controls. Also, the frequency of HLP was higher in the AVS (+) patients than in the AVS (−) subjects, and the mean TG level was significantly higher in the AVS (+) subjects compared to the AVS (−) subjects. Our findings support the literature by showing that increased BMI and hyperlipidemia are related to the pathophysiology of AVS.
Insulin resistance (IR), as a key mediator of obesity and metabolic syndrome, is thought to be associated with pathogenesis of calcific aortic valve disease and altered LV function and structure. Utsunomiya H et al. demonstrated that IR is associated with subclinical abnormalities of LV function assessed by 2D-STE in patients with AVS [27]. They found that LV-GLS, strain rate (SR), and early diastolic SR were significantly lower in the AVS+IR group than in the AVS−IR group and in control subjects; and they showed that IR is a powerful independent predictor of subclinical LV myocardial dysfunction regardless of concomitant visceral obesity and LV hypertrophy. This study is important for investigating subclinical LV dysfunction in AVS. However, as they mentioned, their study has the expected limitations of 2D-STE, such as longer examination times, miss-tracking, and angle dependence. They also did not evaluate whether or not there was an impairment on left atrial functions. 3D-STE provides a more precise representation of myocardial deformation. In the current study, we demonstrated that the LV-GLS and LV-GCS were significantly depressed in the AVS (+) group than in the AVS (−) group. However, we couldn’t find any significant differences between two groups in terms of left atrial 3D-STE results. We did not find any studies that previously assessed the effect of AVS on myocardial functions with 3D-STE.
In the current study, we showed that left ventricular functions, rather than the left atrial mechanics, were impaired subclinically in subjects with AVS. The vulnerability of LV endocardium to ischemic/nonischemic oxidative stress and changes in extracellular matrix may be pathophysiological processes in the development of subclinical ventricular myopathy in early stage compared to atrial tissue. Our results support that subjects with AVS may have subclinical LV deformation abnormalities even though they have not LV pressure overload. In the line of these findings, we can say that subjects with AVS should be investigated for comorbidities leading to atherosclerosis, their dysmetabolic status should be evaluated and these patients should be followed up more closely.
Limitations
This study had several limitations. There were a limited number of patients in the study. The cross-sectional design of the current study precluded the demonstration of a causality relationship. Patients were not examined for CAD, which could affect strain parameters. In addition, we did not evaluate calcific load in AVS with computed tomography.
Conclusions
The current study is the first to assess the LA and LV myocardial dynamics in the subjects with AVS by performing 3D-STE. We demonstrated that the LV-GLS and LV-GCS were significantly depressed in the AVS (+) subjects than in the AVS (−) subjects. However, we showed that the left atrial 3D values were similar in both groups. According to these findings, patients with AVS should be investigated in terms of atherosclerotic risk factors, their dysmetabolic status should be evaluated and closely followed up for their progression to calcific AS. There is a need for prospective studies with a greater number of patients investigating the interaction between AVS and subclinical LV dysfunction and examining the pathophysiological relationship.
References
Otto CM, Lind BK, Kitzman DW, Gersh BJ, Siscovick DS (1999) Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N Engl J Med 341:142–147
Poggio P, Branchetti E, Grau JB, Lai EK, Gorman RC, Gorman JH et al (2014) Osteopontin-CD44v6 interaction mediates calcium deposition via phospho-Akt in valve interstitial cells from patients with noncalcified aortic valve sclerosis. Arterioscler Thromb Vasc Biol 34:2086–2094
Otto CM, Kuusisto J, Reichenbach DD, Gown AM, O’Brien KD (1994) Characterization of the early lesion of ‘degenerative’ valvular aortic stenosis. Histological and immunohistochemical studies. Circulation 90:844–853
Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE et al (1997) Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study J Am Coll Cardiol 29:630–634
Boon A, Cheriex E, Lodder J, Kessels F (1997) Cardiac valve calcification: characteristics of patients with calcification of the mitral annulus or aortic valve. Heart 78(5):472–474
Chandra HR, Goldstein JA, Choudhary N, O’Neill CS, George PB, Gangasani SR et al (2004) Adverse outcome in aortic sclerosis is associated with coronary artery disease and inflammation. J Am Coll Cardiol 43:169–175
Shah SJ, Ristow B, Ali S, Na BY, Schiller NB, Whooley MA (2007) Acute myocardial infarction in patients with versus without aortic valve sclerosis and effect of statin therapy (from the Heart and Soul Study). Am J Cardiol 99(8):1128–1133
Aronow WS, Ahn C, Shirani J, Kronzon I (1999) Comparison of frequency of new coronary events in older subjects with and without valvular aortic sclerosis. Am J Cardiol 83:599–600
Gharacholou SM, Karon BL, Shub C, Pellikka PA (2011) Aortic valve sclerosis and clinical outcomes: moving toward a definition. Am J Med 124:103–110
Kleijn SA, Aly MF, Terwee CB, van Rossum AC, Kamp O (2011) Comparison between direct volumetric and speckle tracking methodologies for left ventricular and left atrial chamber quantification by three-dimensional echocardiography. Am J Cardiol 108:1038–1044
Mochizuki A, Yuda S, Oi Y, Kawamukai M, Nishida J, Kouzu H et al (2013) Assessment of left atrial deformation and synchrony by three-dimensional speckle-tracking echocardiography: comparative studies in healthy subjects and patients with atrial fibrillation. J Am Soc Echocardiogr 26:165–174
Nemes A, Domsik P, Kalapos A, Lengyel C, Orosz A, Forster T (2014) Comparison of three-dimensional speckle tracking echocardiography and two-dimensional echocardiography for evaluation of left atrial size and function in healthy volunteers (results from the MAGYAR Healthy Study). Echocardiography 31:865–871
Lang RM, Badano LP, Tsang W, Adams DH, Agricola E, Buck T et al (2012) American Society of Echocardiography; European Association of Echocardiography. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. J Am Soc Echocardiogr 25:3–46
Sugimoto T, Robinet S, Dulgheru R, Bernard A, Ilardi F, Contu L et al (2018) Echocardiographic reference ranges for normal left atrial function parameters: results from the EACVI NORRE study. Eur Heart J Cardiovasc Imaging 19(6):630–638
Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ et al (2017) 2017 ESC/EACTS Guidelines for the management of valvular heart disease. The task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 38:2739–2791
Novo G, Fazio G, Visconti C, Carità P, Maira E, Fattouch K et al (2011) Atherosclerosis, degenerative aortic stenosis and statins. Curr Drug Targets 12:115–121
Freeman RV, Otto CM (2005) Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation 111:3316–3326
Amzulescu MS, De Craene M, Langet H, Pasquet A, Vancraeynest D, Pouleur AC et al (2019) Myocardial strain imaging: review of general principles, validation, and sources of discrepancies. Eur Heart J Cardiovasc Imaging 20:605–619
Mizuguchi Y, Oishi Y, Miyoshi H, Iuchi A, Nagase N, Oki T (2008) The functional role of longitudinal, circumferential, and radial myocardial deformation for regulating the early impairment of left ventricular contraction and relaxation in patients with cardiovascular risk factors: a study with twodimensional strain imaging. J Am Soc Echocardiogr 21:1138–1144
Dusenbery SM, Lunze FI, Jerosch-Herold M, Geva T, Newburger JW, Colan SD et al (2015) Left ventricular strain and myocardial fibrosis in congenital aortic stenosis. Am J Cardiol 116:1257–1262
Weidemann F, Herrmann S, Stork S, Niemann M, Frantz S, Lange V et al (2009) Impact of myocardial fibrosis in patients with symptomatic severe aortic stenosis. Circulation 120:577–584
Gami AS, Witt BJ, Howard DE, Erwin PJ, Gami LA, Somers VK et al (2007) Metabolic syndrome and risk of incident cardiovascular events and death: a systematic review and meta-analysis of longitudinal studies. J Am Coll Cardiol 49:403–414
Katz R, Wong ND, Kronmal R, Takasu J, Shavelle DM, Probstfield JL et al (2006) Features of the metabolic syndrome and diabetes mellitus as predictors of aortic valve calcification in the Multi-Ethnic Study of Atherosclerosis. Circulation 113:2113–2119
Katz R, Budoff MJ, Takasu J, Shavelle DM, Bertoni A, Blumenthal RS et al (2009) Relationship of metabolic syndrome to incident aortic valve calcium and aortic valve calcium progression: the Multi-Ethnic Study of Atherosclerosis. Diabetes 58:813–819
Briand M, Lemieux I, Dumesnil JG, Mathieu P, Cartier A, Després JP et al (2006) Metabolic syndrome negatively influences disease progression and prognosis in aortic stenosis. J Am Coll Cardiol 47:2229–2237
Capoulade R, Clavel MA, Dumesnil JG, Chan KL, Teo KK, Tam JW et al (2012) Impact of metabolic syndrome on progression of aortic stenosis: influence of age and statin therapy. J Am Coll Cardiol 60(3):216–223
Utsunomiya H, Yamamoto H, Kunita E, Hidaka T, Kihara Y (2014) Insulin resistance and subclinical abnormalities of global and regional left ventricular function in patients with aortic valve sclerosis. Cardiovasc Diabetol 13:86
Funding
This work did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dogdus, M., Yildirim, A., Kucukosmanoglu, M. et al. Are there any subclinical myocardial dysfunctions in subjects with aortic valve sclerosis? A 3D-speckle tracking echocardiography study. Int J Cardiovasc Imaging 37, 207–213 (2021). https://doi.org/10.1007/s10554-020-01977-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-020-01977-4