
Abstract
To evaluate diagnostic impact of clinical use of coronary computed tomography angiography (CCTA) in patients with suspected stable coronary artery disease (CAD) and its consequences in daily practice for patient management, depending on stress test results in daily practice. Between 2009 and 2014 of a total population of 1352 patients of the German Cardiac Computed Tomography (CT) Registry who had previously undergone stress tests, CCTA visualizations were carried out on the coronary arteries with suspected stable CAD. Patients were divided into three groups according to stress test results: Group 1 with inconclusive (n = 178, 13.2%), Group 2 with ischemia in stress test (n = 372, 27.5%) and Group 3 without ischemia in stress test (n = 802, 59.3%). The test of preference was the stress electrocardiogram (ECG), which was performed more frequently in patients without ischemia in stress test as compared to those with ischemia (96.3% vs. 93.0%, p = 0.015). The incidence of detected obstructive CAD was lower in patients with suggested ischemia in stress test as compared to patients with inconclusive results (14.1% vs. 21.1%, p = 0.037). There was no difference in the incidence of an obstructive CAD in patients with and without ischemia in stress test (14.1% vs. 15.8%, p = 0.440). CCTA is a reliable, non-invasive option for ruling-out obstructive CAD irrespective of the stress test result.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Coronary computed tomography angiography (CCTA) is a broadly accepted modality for the non-invasive workup of selected patients with suspected stable coronary artery disease in clinical practice [1,2,3,4,5,6,7]. In some healthcare settings, CCTA is considered a first-line diagnostic test for patients with angina chest pain [8]. Current European Society of Cardiology (ESC) guidelines recommend further testing in patients with suspected stable coronary artery disease (SCAD) based on the pre-test probability (PTP). In order to obtain optimal results and to avoid overestimation of coronary stenoses, CCTA should be performed in patients with a low intermediate pre-test probability (PTP 15–50%). If Duke Criteria indicate a high risk patient, patients with stress-induced ischemia should be considered for coronary angiography. In cases of an inconclusive stress test results, further testing is recommended depending on patient characteristics and preferences [9].The German Cardiac CT Registry provides information about the indications, procedural data and clinical results of cardiac computed tomography in a routine clinical setting. The aim of our current analysis was to evaluate the influence of prior stress test results in cases of suspected stable coronary artery disease on the results of CCTA and the diagnostic impact of CCTA.
Materials and methods
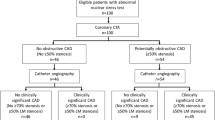
The German Cardiac CT Registry has records of 7061 cardiac CT examinations using at least 64-slice CT at 12 expert centers conducted between 2009 and 2014. 1352 patients with suspected stable coronary artery disease (CAD) who were undergoing CCTA for imaging of the coronary arteries with prior stress tests were included in our analysis and comprise the study population. Patients with other indications (e.g. no prior stress test, imaging of the pulmonary veins, clarification of cardiac mass, TAVI-procedure, valvular heart disease, history of CAD or evaluation of an implant) were excluded (n = 5709). Patients were divided into three groups depending on their stress test results: Group 1 with inconclusive stress test (i.st), Group 2 with ischemia in stress test (st+) and Group 3 without ischemia in stress test (st−) (Fig. 1). The CT scan was performed either as CCTA only or as a combined calcium scan using prospective triggering and retrospective acquisition with and without tube current modulation. Interpretation and reporting of the CT scan was performed by a cardiologist or radiologist or by a consensus reading. At the time of examination, data were collected including patient demographics, medical history, and standardized cardiovascular risk factors as determined by a structured patient interview in a web based electronic case report forms (CRFs). Detailed information regarding indication for cardiac CTA, study results (including results of coronary calcification exam and coronary CTA), diagnostic impact, procedures avoided by CT and recommended procedures were also collected via a structured data base.

Coronary CT in patients with suspected stable coronary artery disease for detection and/or exclusion of coronary artery stenoses. All patients (n = 1.626) were divided into two groups: group 1 with inconclusive or no stress test and group 2 with conclusive stress test. CAD coronary artery disease, CT computed tomography, PTP pre-test probability, TAVI transcatheter aortic valve implantation
A patient was considered to be hypertensive if he or she had received such a diagnosis on the basis of persistently elevated systemic blood pressure greater than 140/90 mmHg. Criteria for diabetes was based on the patient having increased levels of plasma glucose in oral glucose tolerance test, after fasting or elevated glycated hemoglobin (A1C). The cardiovascular risk factor cigarette smoking was divided into three categories: smoker (smoking during the last 2 month), former smoker (smoker who quit smoking at least 1 month ago) and non smoker. Patients whom had stopped smoking more than 20 years ago were not considered to have smoking as a risk factors. Family history was defined as coronary heart disease or stroke in first- or second-degree relatives under the age of 65 (females) and 55 (males). Symptoms of chest pain were divided into typical, atypical and non-anginal chest pain according to the ESC guidelines [9]. Typical angina meets all three of the following characteristics: (1) substernal chest discomfort of characteristic quality and duration, (2) provoked by exertion or emotional stress and (3) relieved by rest and/or nitrates within minutes. Atypical angina meets only two of these characteristics, while non-angina chest pain lacks or meets only one of the characteristics. The pre-test probability (PTP) was determined according to the updated CAD consortium model [10] by age, gender and the nature of symptoms [9] for all patients. Information regarding indications for the cardiac CT examination, scan parameters and contrast protocol, study results (including coronary CT angiography), complications and consequences were collected via a structured data base. The following parameters of our study population (n = 1352) were analysed in each group: patient characteristics, procedural characteristics, detection of obstructive coronary stenosis (as defined by the presence of coronary stenosis) equal to or greater than 50%, exclusion of CAD (as defined by the absence of plaques and stenosis), cardiovascular risk factors, referring physician, indication for CT scan, symptoms, previous stress test results, diagnostic and clinical impact of the CT scan.
Statistical analysis
Quantitative variables were expressed as mean ± standard deviation or median and interquartile range. Qualitative data (nominal or ordinal scale) were given as frequencies and rates. For comparison between subgroups, the classic Chi-squared-test or Kruskal–Wallis test were used. P-values of 0.05 or less were considered significant. Data analysis was performed at the Institute for Myocardial Infarction Research Foundation using SAS statistical analysis software, version 9.3 (SAS Institute, Inc., Cary, North Carolina, USA).
Results
Patient characteristics and risk factors
Mean patient age was 58.1 ± 11.3 years. The mean body mass index (BMI) was 26.9 ± 4.4 kg/m2. 47.8% (646/1352) were female. The mean PTP was 38.0% (28.0, 59.0). 14.9% (202/1352) of the patients met all three of the angina characteristics, 69.0% (933/1352) two and 16.1% (217/1352) only one criterion. 13.2% (178/1352) of the patients had an inconclusive stress test, while 86.8% (1174/1352) had a conclusive stress test. Conclusive stress tests include those with positive (n = 372, 27.5%) and negative results (n = 802, 59.3%).
Patients with ischemia in stress test had a lower pre-test probability than those without ischemia in stress test (st+: 37.5% vs. st−: 38.0%, p = 0.019) and with an inconclusive stress test (st+: 37.5% vs. i.st: 47.0%, p = 0.007). I Patients with ischemia in stress test were more likely female as compared to those without ischemia in stress test (st+: 54% vs. st−: 42.1%, p < 0.001). All groups did not differ in body mass index (i.st: 26.8 ± 4.3 kg/m2 vs. st+: 26.8 ± 4.5 kg/m2 vs. st−: 26.8 ± 4.2 kg/m2, p = 0.700), diabetes (i.st: 11.4% vs. st+: 8.5% vs. st−: 9.8%, p = 0.760), family history of myocardial infarction (MI), coronary artery bypass graft (CABG) and/or sudden death (i.st: 38.6% vs. st+: 21.9% vs. st−: 37.2%, p = 0.120) and hypertension (i.st: 65.0% vs. st+: 60.6% vs. st−: 59.7%, p = 0.680). The total number of cardiovascular risk factors were less frequent in patients with ischemia in stress test as compared to those without (st+: 2.0 vs. st−: 3.0, p < 0.001). Patient characteristics are shown in Table 1.
Clinical symptoms
Patients with an inconclusive stress test met more often all three criteria of angina as compared to those with ischemia in stress test (i.st: 25.3% vs. st+: 14.0%, p = 0.001). Patients with ischemia in stress test had more often dyspnea during exercise as compared to those without ischemia in stress test (st+: 33.2% vs. st−: 22.3%, p < 0.001). The stress test of preference was the stress electrocardiogram (ECG), which was performed more frequently in patients without ischemia in stress test as compared to those with ischemia in stress test (96.3% vs. 93.0%, p = 0.015). Further details are listed in Table 2.
Procedural characteristics and results of the CT scan
An additional assessment of coronary artery calcification was performed more frequently in patients without ischemia in stress test as compared to those with ischemia (st−: 91.0% vs. st+: 85.8%, p = 0.006). For patients with a conclusive stress test the median total Agatston-score was 55.0 (interquartile range [IQR] 13.0, 169.0; stress test with ischemia 48.0, IQR 14.0, 144.0; stress test without ischemia 59.0, IQR 12.9, 178), whereas the total Agatston-score for patients with inconclusive stress test was 77 (IQR 10.0, 178.0). Obstructive CAD was detected less frequently in patients with ischemia in stress test as compared to those with inconclusive stress test results (st+: 14.1% vs. i.st: 21.1%, p = 0.037), while there was no difference in the incidence between patients with ischemia in stress test and without (st+: 14.1% vs. st−: 15.8%, p = 0.0440, Table 3).
Clinical consequences
For all groups, there was no difference in the diagnostic impact of the CCTA (Table 4) regarding a completely new diagnosis (i.st: 1.2% vs. st+: 1.4% vs. st−: 1.4%, p = 0.540), an additional diagnosed aspect (i.st: 3.6% vs. st+: 4.3% vs. st−: 3.2%, p = 0.920) or for exclusion/confirmation of the suspected diagnosis (i.st: 95.2% vs. st+: 94.2% vs. st−: 95.5%, p = 0.800). As a consequence of CCTA, invasive coronary angiography could be avoided more frequently in patients with ischemia in stress test as compared to those without ischemia in stress test (st+: 59.8% vs. st−: 52.5%, p = 0.029).
Discussion
The German Cardiac CT Registry provides a large database regarding the clinical use of CCTA. This data provide valuable insights into daily routine in contrast to randomized trials, as it highlights the challenges of treating patients with prior diagnostic ambiguity from previously performed test. In contrast to patients without ischemia in stress test, those with ischemia were more likely to be female with a lower number of classic risk factors and a significantly lower pretest probability. This population also suffered less frequent from typical stable angina as compared to patients with an inconclusive stress test. For this reason, a CAD was uncommon in this subgroup.
Non-invasive testing for ischemia is recommended in patients with an intermediate PTP (15–85%) [9]. Alternatively, coronary CT angiography can be performed in patients who are at low intermediate PTP (15–50%), if left ventricular ejection fraction is > 50% and provided that adequate technology and expertise are locally available [9]. For the majority in all groups, a stress ECG was the preferred diagnostic method and was performed more often in patients with indications of ischemia in stress test compared to those with an inconclusive stress test results. The frequency of this sort of testing is presumably due to its simple nature and widespread availability, in addition to demonstrating low pretest probability. Surprisingly, there is a very high proportion of patients in the registry who had a previous conclusive stress test and were nevertheless subsequently examined with a CCTA. The proportion of patients in this group meeting the Duke criteria (Duke Treadmill Score) with respect to risk stratification is unknown. This missing risk stratification for previously performed stress test in high, intermediate and low cardiovascular (CV) mortality risk is also a frequently observed problem in daily practice. Many times, the assessment is based solely on the clinical evaluation of the referring physician. Since a CCTA was performed in this group, it is presumed that these patients presented with an intermediate or low CV mortality risk. Of these patients with a conclusive stress test, CCTA demonstrated no difference in the incidence of obstructive CAD between patients with suspected ischemia in stress test and those characterized by the absence of ischemia in the previous stress test. This is mainly caused by a low sensitivity and specificity in the chosen stress test (stress ECG). Another cause for this surprising correlation might be the variables in interpretation of stress test results, which are suspected to be mainly false-positive results. The attending physicians may have had doubts about the specificity of the chosen stress test, since the result was in contradiction to their clinical assessment. This factor is taken into account in the consensus recommendations of the German Radiology Society (DRG), the German Cardiac Society (DGK) and the German Society of Pediatric Cardiology (DGPK) on the use of cardiac imaging with computed tomography [11], which corresponds more to what is experienced in daily practice on this point compared to the ESC guidelines, which give the physician more options in the selection of the appropriate diagnostic tool.
This explains why a surprisingly lower incidence of obstructive CAD was found in the group with suspected ischemia in the stress test as compared to those with inconclusive stress test results. Despite to higher frequency of atypical angina and the lower pretest probability among the less comorbid patient cohort, this result was nevertheless expected by the physicians. Invasive coronary angiography could be avoided more often in patients with suspected ischemia in the stress test group than for patients who tested for no ischemia in stress test. Therefore, CCTA provides valuable results and is a reliable non-invasive option for ruling-out obstructive CAD irrespective of the stress test result.
Limitations
There was no definition of criteria which classified the stress test as positive or negative. The proportion of patients for whom Duke criteria indicate a high-risk patient is unknown. The judgment of the attending physicians carrying out the CT scan to question the results of the stress test remains a matter of speculation. The proportion of stress tests incorrectly classified as “conclusive” cannot be known. Lastly, it is unclear whether the stress tests were carried out by the referring physicians or the expert center .
Conclusions
In a large study of patients investigated in experienced clinical settings, the decision to perform invasive coronary CTA to test for suspected stable CAD relied on previous stress test results. The stress ECG was the preferred stress test of the registry with known limited accuracy in detection of ischemia as well as with regard to a proper interpretation. Therefore, CCTA provides valuable results in daily routine and is helpful in avoiding invasive coronary angiography in patients for whom stress test seemed to be false positive or for whom high cardiovascular mortality risk from ischemia is not present.
References
Cho I, Chang HJ, Ó Hartaigh B, Shin S, Sung JM, Lin FY, Achenbach S, Heo R, Berman DS, Budoff MJ, Callister TQ, Al-Mallah MH, Cademartiri F, Chinnaiyan K, Chow BJ, Dunning AM, DeLago A, Villines TC, Hadamitzky M, Hausleiter J, Leipsic J, Shaw LJ, Kaufmann PA, Cury RC, Feuchtner G, Kim YJ, Maffei E, Raff G, Pontone G, Andreini D, Min JK (2005) Incremental prognostic utility of coronary CT angiography for asymptomatic patients based upon extent and severity of coronary artery calcium: results from the COronary CT Angiography EvaluatioN For Clinical Outcomes InteRnational Multicenter (CONFIRM) study. Eur Heart J 36:501–508
Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O’Gara P, Rubin GD, American College of Cardiology Foundation Appropriate Use Criteria Task Force; Society of Cardiovascular Computed Tomography; American College of Radiology; American Heart Association, American Society of Echocardiography; American Society of Nuclear Cardiology; North American Society for Cardiovascular Imaging; Society for Cardiovascular Angiography and Interventions; Society for Cardiovascular Magnetic Resonance, Kramer CM, Berman D, Brown A, Chaudhry FA, Cury RC, Desai MY, Einstein AJ, Gomes AS, Harrington R, Hoffmann U, Khare R, Lesser J, McGann C, Rosenberg A, Schwartz R, Shelton M, Smetana GW, Smith SC Jr (2010) ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 56:1864–1894
Wolk MJ, Bailey SR, Doherty JU, Douglas PS, Hendel RC, Kramer CM, Min JK, Patel MR, Rosenbaum L, Shaw LJ, Stainback RF, Allen JM, American College of Cardiology Foundation Appropriate Use Criteria Task Force (2014) ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Am Coll Cardiol 63:380–406
Maurer MH, Zimmermann E, Schlattmann P, Germershausen C, Hamm B, Dewey M (2012) Indications, imaging technique, and reading of cardiac computed tomography: survey of clinical practice. Eur Radiol 22:59–72
Schulman-Marcus J, Danad I, Truong QA (2015)) State-of-the-art updates on cardiac computed tomographic angiography for assessing coronary artery disease. Curr Treat Option Cardiovasc Med 17:398
Meijboom WB, Meijs MF, Schuijf JD, Cramer MJ, Mollet NR, van Mieghem CA, Nieman K, van Werkhoven JM, Pundziute G, Weustink AC, de Vos AM, Pugliese F, Rensing B, Jukema JW, Bax JJ, Prokop M, Doevendans PA, Hunink MG, Krestin GP, de Feyter PJ (2008) Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 52:2135–2144
Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, Paul N, Clouse ME, Shapiro EP, Hoe J, Lardo AC, Bush DE, de Roos A, Cox C, Brinker J, Lima JA (2008) Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med 359:2324–2336
Moss AJ, Williams MC, Newby DE, Nicol ED (2017) The updated NICE guidelines: cardiac CT as the first-line test for coronary artery disease. Curr Cardiovasc Imaging Rep 10:15
Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, Bugiardini R, Crea F, Cuisset T, Di Mario C, Ferreira JR, Gersh BJ, Gitt AK, Hulot JS, Marx N, Opie LH, Pfisterer M, Prescott E, Ruschitzka F, Sabaté M, Senior R, Taggart DP, van der Wall EE, Vrints CJ, ESC Committee for Practice Guidelines, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Document Reviewers, Knuuti J, Valgimigli M, Bueno H, Claeys MJ, Donner-Banzhoff N, Erol C, Frank H, Funck-Brentano C, Gaemperli O, Gonzalez-Juanatey JR, Hamilos M, Hasdai D, Husted S, James SK, Kervinen K, Kolh P, Kristensen SD, Lancellotti P, Maggioni AP, Piepoli MF, Pries AR, Romeo F, Rydén L, Simoons ML, Sirnes PA, Steg PG, Timmis A, Wijns W, Windecker S, Yildirir A, Zamorano JL (2013) 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 34:2949–3003
Steyerberg EW, Alkadhi H, Leschka S, Desbiolles L, Nieman K, Galema TW, Meijboom WB, Mollet NR, de Feyter PJ, Cademartiri F, Maffei E, Dewey M, Zimmermann E, Laule M, Pugliese F, Barbagallo R, Sinitsyn V, Bogaert J, Goetschalckx K, Schoepf UJ, Rowe GW, Schuijf JD, Bax JJ, de Graaf FR, Knuuti J, Kajander S, van Mieghem CA, Meijs MF, Cramer MJ, Gopalan D, Feuchtner G, Friedrich G, Krestin GP, Hunink MG, CAD Consortium (2011) A clinical prediction rule for the diagnosis of coronary artery disease: validation, updating, and extension. Eur Heart J 32:1316–1330
Achenbach S, Barkhausen J, Beer M, Beerbaum P, Dill T, Eichhorn J, Fratz S, Gutberlet M, Hoffmann M, Huber A, Hunold P, Klein C, Krombach G, Kreitner KF, Kühne T, Lotz J, Maintz D, Mahrholdt H, Merkle N, Messroghli D, Miller S, Paetsch I, Radke P, Steen H, Thiele H, Sarikouch S, Fischbach R (2012) Consensus recommendations of the German Radiology Society (DRG), the German Cardiac Society (DGK) and the German Society for Pediatric Cardiology (DGPK) on the use of cardiac imaging with computed tomography and magnetic resonance imaging. Rofo 184:345–368
Acknowledgements
We are indebted to all participants of the registry and the staff of the Stiftung Institut für Herzinfarktforschung of Ludwigshafen, Germany.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Stephan Achenbach has received research grants from Siemens Healthcare. Mohamed Marwan has received speaker honoraria from Siemens Healthcare. All patients at participating sites gave written informed consent for CT scan and inclusion in the registry. The registry was approved by the participating institution's IRBs.
Rights and permissions
About this article

Cite this article
Barth, S., Marwan, M., Hausleiter, J. et al. Coronary computed tomography angiography (CCTA) in patients with suspected stable coronary artery disease (CAD): diagnostic impact and clinical consequences in the German Cardiac CT Registry depending on stress test results. Int J Cardiovasc Imaging 35, 741–748 (2019). https://doi.org/10.1007/s10554-018-1504-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-018-1504-0