
Abstract
The aim of this study was to assess cardiac deformation patterns in myocarditis applying feature tracking imaging (FTI) to cardiovascular magnetic resonance (CMR) images. Thirty-six patients (31 males) with acute myocarditis and 36 age- and gender-matched healthy volunteers were studied. CMR examinations were performed in a 1.5 T MR-scanner including late gadolinium enhancement (LGE). FTI was applied to standard cine images of long and short axis views. Global peak circumferential, longitudinal and radial systolic strains as well as long axis strain (LAS) were measured. Patients showed significantly impaired global peak circumferential (−24.4 ± 4.2 % vs. −28.8 ± 3.8 %, p < 0.0001), longitudinal (−17.6 ± 4.4 % vs. −23.8 ± 3.1 %, p < 0.0001) and radial (26.1 ± 5.4 % vs. 37.9 ± 7.6 %, p < 0.0001) systolic strains. Even patients with a preserved ejection fraction (pEF, ≥55 %) had significantly reduced longitudinal (−20.0 ± 4.8 % vs. −23.8 ± 3.1 %, p < 0.01) and radial (27.7 ± 5.5 % vs. 37.9 ± 7.6 %, p < 0.0001) strains. The extent of LGE in patients did not correlate to their respective strains. Regarding the differentiation between patients and controls, the addition of global peak systolic strains to ejection fraction led to a significant improvement of the logistic regression model (χ2 48.7 vs. 71.5; p < 0.001) resulting in a high AUC of 0.98. Applying previously published reference values, 75 % or 31 % of patients with pEF showed at least one strain value or a LAS, which fell below the limit of 1 or respectively 2 standard deviations from the reference mean value. Cardiac strains measured by CMR–FTI are significantly impaired in patients with acute myocarditis even in those with pEF. Therefore, strain assessment may improve the diagnostic accuracy of CMR for myocarditis.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute myocarditis is associated significantly with morbidity and mortality. The long-term mortality rate in patients with viral myocarditis reaches 19 % and epidemiologic studies have shown that myocarditis may account for up to 12 % of sudden cardiac deaths in young individuals [1–3]. The diagnosis of myocarditis is challenging due to its unspecific clinical presentation and its wide variability of myocardial changes. Cardiovascular magnetic resonance (CMR) is the method of choice for the non-invasive assessment of cardiac morphology and function as well as tissue characterization [4]. Furthermore, it has shown to offer a prognostic value in patients with suspected or proven myocarditis [3, 5]. Besides the precise quantification of cardiac volumes and the detection of tissue alterations, CMR offers the possibility to evaluate cardiac deformation. The assessment of cardiac strains provides an incremental value for risk stratification in various cardiac diseases [6–8]. Recently, feature tracking imaging (FTI) has been applied to cine CMR images and reference values have been published [9, 10]. In previous studies, a robust correlation between strain values derived from CMR–FTI and MR tagging as well as echocardiography (EC) speckle tracking has been shown [11–15]. Furthermore, FTI-derived strain values featured an excellent intra- and inter-observer reproducibility as well as a good inter-study agreement [9, 10]. The aim of this study was to characterize cardiac strain alterations in patients with acute myocarditis in comparison to matched healthy controls applying FTI.
Methods
Patients and control group
We retrospectively included 36 patients (31 male, 5 female) in the final study population who were admitted with acute myocarditis and underwent a clinically indicated CMR examination. The patients presented with acute symptoms of myocarditis (e.g. chest pain or dyspnoea) in our chest pain unit or were referred to our tertiary cardiology centre by other hospitals or physicians. Blood samples were taken at the initial presentation as well as during hospital stay. C-reactive protein (CRP) as well as cardiac Troponin T (cTnT; fourth generation TnT assay, Elecsys 2010, Roche Diagnostics, Penzberg, Germany) until June 2009 and high-sensitivity cardiac Troponin T (hscTnT; Elecsys Troponin T hs Test, COBAS E411, Roche Diagnostics, Penzberg, Germany) after June 2009 were measured and peak levels during hospital stay were determined. The control group consisted of proven healthy volunteers from a well-characterized reference population who were matched with regard to age and gender. All healthy controls passed through an extensive selection process including medical history, physical examination, electrocardiogram (ECG), lab tests, oral glucose tolerance test and stress CMR. They were not allowed for any regular medication except for contraceptives, chronic thyroid hormone substitution or vitamins. The body mass index (BMI) as well as the body surface area (BSA) according to the Mosteller formula were calculated [16].
The study was in accordance with the declaration of Helsinki and approved by the local ethics committee. The reference population was part of several previous studies and publications [10, 17] (NCT01100710).
Image acquisition
CMR images were acquired in a 1.5 T whole body MR scanner (Achieva, Philips Medical Systems, Best, The Netherlands) in supine position applying a vector-ECG triggering. Short axis (SAX) from base to apex as well as two-, three- and four-chamber views of the left ventricle (LV) were obtained using a standard cine steady-state free precession (SSFP) sequence. Myocardial oedema was assessed applying a T2-weighted triple-inversion recovery black blood sequence. Late gadolinium enhancement (LGE) imaging was performed 10 min after the administration of 0.2 mmol Gd-DTPA/kg body weight (Magnograf, Bayer Healthcare, Leverkusen, Germany).
Image analysis
The cardiac morphology including LV enddiastolic (EDV) and endsystolic (ESV) volumes, stroke volume (SV) and ejection fraction (EF) was quantified by two experienced observers independently. Cardiac strain was assessed in short and long axis views of cine CMR images applying the FTI algorithm (2D CPA CMR Feature tracking software, TomTec Imaging Systems, Unterschleißheim, Germany) (Fig. 1). Global peak circumferential endocardial and global peak radial systolic strains were obtained in three SAX, which covered the apical, midventricular and basal LV segments. The global peak longitudinal endocardial systolic strain was averaged from the measurements of the two-, three- and four-chamber views. Furthermore, the long axis strain (LAS) was determined according to the previously published epi/mid approach [18]. LGE was assessed visually and quantified using a dedicated CMR analysis software (cmr42, Circle Cardiovascular Imaging, Calgary, Canada). The quantification of the affected myocardium was performed applying a threshold of 3 standard deviations (SD) above the mean of the remote myocardium as recommended in current literature [19]. In addition, thresholds of 2, 4, 5, 6, 8 and 10 SD above the mean of the remote myocardium were assessed.

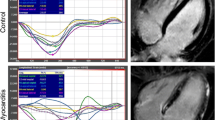
Feature tracking. Left Example of the tracking of short and long axis SSFP images. Right Example of the resulting strain curves. The mean curves are indicated by arrows
Statistics
Data was tested for normal distribution applying the D’Agostino Pearson test. Continuous data is presented as mean ± SD. Non-parametric data is presented as median (interquartile range). For the comparison of two groups the Student’s t test or the Welch test were used for parametric data, non-parametric data was assessed by the Mann–Whitney test. Parametric data of more than two groups was assessed with an ANOVA with a post-hoc Student–Newman–Keuls test. Correlation was evaluated using Pearson’s correlation coefficient or Spearman’s rho as applicable. Categorical data was assessed employing the Chi-square test. Receiver operating characteristics (ROC) were applied and the area under the curve (AUC) was calculated. A stepwise logistic regression model was used to assess the diagnostic significance of different parameters. For the comparison with recently published reference values for global peak circumferential, longitudinal and radial systolic strains as well as the LAS [10, 18], two lower limits were defined as 1 or 2 SD from the respective mean value. Statistical analyses were conducted using MedCalc Statistical Software version 15.8 (MedCalc Software, Ostend, Belgium). A statistical significance was assumed at p < 0.05.
Results
Clinical characteristics, cardiac function and deformation of myocarditis patients compared to healthy controls
An overview of the patients’ characteristics is given in Table 1. Pre-existing congestive heart failure was reported for none of the included patients. Furthermore, subjects did not show valvular stenosis or other than mild forms of valvular regurgitation. Arterial hypertension was reported in seven patients (19 %).
The compositions of the patient group and of the control group were similar with regard to age [40.5 (27.5–48.0) years vs. 41.0 (29.0–48.5) years, p = n.s.], gender (31 males and 5 females vs. 31 males and 5 females, p = n.s.), BMI [25.3 (22.0–28.3) kg/m2 vs. 24.8 (23.1–26.8) kg/m2, p = n.s.] and BSA (2.0 ± 0.2 m2 vs. 2.0 ± 0.2 m2, p = n.s.).
The CMR examinations of the patients were performed 2 (1–3) days after hospital admission. The EDV was similar between patients and healthy controls (171.8 ± 33.4 ml vs. 168.5 ± 41.0 ml, p = n.s.), whereas the ESV was significantly increased in patients (78.6 ± 20.9 ml vs. 55.9 ± 19.5 ml, p < 0.0001) resulting in a lower SV (93.2 ± 21.1 ml vs. 112.6 ± 23.5 ml, p < 0.001) and a reduced EF (54.4 ± 8.3 % vs. 67.5 ± 4.6 %, p < 0.0001). In patients, myocardial oedema was present in 25 of 33 cases (76 %) with assessable oedema CMR.
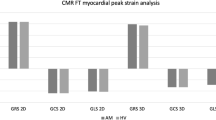
FTI analysis revealed significantly reduced global peak circumferential (−24.4 ± 4.2 % vs. −28.8 ± 3.8 %, p < 0.0001) and longitudinal (−17.6 ± 4.4 % vs. −23.8 ± 3.1 %, p < 0.0001) systolic strains in myocarditis patients resulting in less negative values (Fig. 2). Likewise, the global peak radial systolic strain was significantly lower in patients than in controls (26.1 ± 5.4 % vs. 37.9 ± 7.6 %, p < 0.0001). The global peak circumferential, longitudinal and radial systolic strains correlated well with EF (r = −0.75, r = −0.62, r = 0.60; all p < 0.0001). There was no significant correlation between the extent of LGE and the assessed systolic strains (all p = n.s.). The fraction of myocardium which was affected by LGE in myocarditis patients is given in Table 2. In addition, its distribution pattern is displayed in Fig. 3.

Comparison of cardiac strains between myocarditis patients and healthy controls. The global peak circumferential, longitudinal and radial systolic strains were significantly reduced in myocarditis patients compared to healthy volunteers. *p < 0.05

Distribution pattern of late gadolinium enhancement in myocarditis patients. Fraction of myocardial segments according to the 17-segment model of the American Heart Association which showed late gadolinium enhancement in the patient cohort. The proportion of affected segments is given in percentage
Subgroup analysis of myocarditis patients with preserved ejection fraction
We performed a subgroup analysis in myocarditis patients with a preserved LV EF (≥55 %, n = 16) compared to healthy subjects (n = 36). The composition of this subgroup showed no significant difference to the healthy controls with regard to age, gender, BMI and BSA (all p = n.s.). Although the EF was formally not impaired, the patients showed reduced global peak longitudinal (−20.0 ± 4.8 % vs. −23.8 ± 3.1 %, p < 0.01) and radial (27.7 ± 5.5 % vs. 37.9 ± 7.6 %, p < 0.0001) systolic strains. Yet, the global peak circumferential (−27.9 ± 2.9 % vs. −28.8 ± 3.8 %, p = n.s.) systolic strain was not significantly different (Fig. 4).

Comparison of cardiac strains between myocarditis patients without and with pEF and healthy controls. The difference between myocarditis patients with pEF and healthy controls yielded significance for the global peak longitudinal and radial systolic strains. All assessed strains differed significantly between myocarditis patients with impaired EF and healthy volunteers. Group 1: myocarditis patients with impaired EF (<55 %), Group 2: myocarditis patients with pEF (≥ 55 %), Group 3: healthy controls; *p < 0.05
The global peak circumferential (−21.6 ± 2.7 % vs. −27.9 ± 2.9 %, p < 0.0001) and longitudinal (−15.7 ± 2.8 % vs. −20.0 ± 4.8 %, p < 0.01) systolic strains showed a significant difference between myocarditis patients without and with preserved EF (pEF). The global peak radial systolic strain revealed a trend which, however, did not reach significance (24.9 ± 5.1 % vs. 27.7 ± 5.5 %, p = n.s.). Both groups showed no significant difference regarding age, gender, BMI and BSA (all p = n.s.).
Assessment of the diagnostic value of cardiac deformation in myocarditis patients
The ROC analysis showed good AUC values for the differentiation between myocarditis patients and healthy controls which allowed for the determination of threshold values and the calculation of their respective sensitivities and specificities (Fig. 5). Regarding the EF, the AUC was 0.92 yielding a sensitivity of 89 % and a specificity of 86 %. The AUC was 0.78 for the global peak circumferential systolic strain with a sensitivity of 58 % and specificity of 89 %. For the global peak longitudinal systolic strain the AUC was 0.86 reaching a sensitivity of 81 % and specificity of 86 %. The ROC analysis of the radial systolic strain featured an AUC of 0.90 with a sensitivity of 83 % and a specificity of 81 %. Regarding the myocarditis patients with pEF, the AUC of the global peak longitudinal systolic strain was 0.74 with a sensitivity of 63 % and specificity of 86 % (Fig. 6). The ROC analysis of the global peak radial systolic strain featured an AUC of 0.86 with a sensitivity of 100 % and a specificity of 58 %. However, the ROC analysis of the global peak circumferential systolic strain yielded no significance in the patients with pEF compared to healthy controls.

ROC curves of the cardiac strains for the differentiation between myocarditis patients and healthy controls. The area under the curve was 0.92 for EF (criterion ≤ 62 %), 0.78 for global peak circumferential (criterion > −24.9 %), 0.86 for global peak longitudinal (criterion > −20.9 %) and 0.90 for radial (criterion ≤ 31.3 %) systolic strains. The p values of all analyses were <0.0001

ROC curves of the cardiac strains for the differentiation between the subgroup of myocarditis patients with pEF and healthy controls. The AUC was 0.74 for global peak longitudinal (criterion > −20.9 %) and 0.86 for radial (criterion ≤ 35.6 %) systolic strains. The p values of all analyses were <0.01
In the logistic regression analysis, which included the global peak circumferential, longitudinal and radial systolic strains, EF, age and gender, all assessed strains as well as the EF contributed significantly to the model (χ2 71.5, 90.3 % of cases classified correctly, AUC 0.98, see Table 3). In addition to the EF, the cardiac strains improved the regression model significantly (Fig. 7).

Chi-square values of the logistic regression model for the differentiation between myocarditis patients and healthy controls. In addition to the EF the cardiac strains improved the regression model significantly. *p < 0.001
Implementation of current reference values for cardiac deformation
Previously published reference values were applied to distinguish between myocarditis patients and healthy controls (see Table 4). In the myocarditis cohort, the lower limit was exceeded in 39 % of the global peak circumferential systolic strain values, in 69 % of the global peak longitudinal systolic strain values and in 72 % of the global peak radial systolic strain values using a threshold of 1 SD from the reference mean value. In 83 % of the cases at least one of these strain values fell below the limit. The limit was exceeded in 19 % of the global peak circumferential systolic strain values, in 36 % of the global peak longitudinal systolic strain values and in 19 % of the global peak radial systolic strain values when a threshold of 2 SD from the reference mean value was applied. Hereby, 47 % of cases showed a least one value below the limit.
Applying the reference values to the 16 myocarditis patients with pEF, the lower limit was exceeded in 0 % of the global peak circumferential systolic strain values, in 44 % of the global peak longitudinal systolic strain values and in 56 % of the global peak radial systolic strain values using a threshold of 1 SD from the reference mean value. In 69 % of the cases at least one of these values fell below the limit. The limit was exceeded in 0 % of the global peak circumferential systolic strain values, in 19 % of the global peak longitudinal systolic strain values and in 19 % and of the global peak radial systolic strain values when a threshold of 2 SD from the reference mean value was applied. Hereby, 25 % of cases showed a least one value below the limit.
For a further examination of the myocarditis patients with pEF, the LAS was assessed employing recently published reference values [18]. In 63 % or 19 % of the cases the LAS fell below the limit when 1 or 2 SD from the previously published reference mean value were applied as threshold (−14.8 % or −12.5 % respectively).
Combining all assessed strain values, i.e. the global peak systolic strains and the LAS, in myocarditis patients with pEF, in 75 % or 31 % of the cases at least one of these values exceeded the limit when 1 or 2 SD from the mean were set as one-sided threshold, respectively.
Discussion
In this study, the cardiac deformation of myocarditis patients was assessed by FTI of cine CMR images and compared to healthy volunteers.
The major findings were: (1) In patients with myocarditis the cardiac deformation as measured by global peak endocardial systolic strain values is significantly impaired. (2) Even patients with a preserved EF show markedly reduced global peak longitudinal and radial systolic strain values. (3) Strain measurements allow to distinguish between patients and controls with good accuracy. (4) The application of recently published reference values may improve the identification of myocarditis patients in clinical routine.
The current CMR criteria (Lake Louise criteria) for the diagnosis of myocarditis use morphological features as early and late gadolinium enhancement as well as myocardial oedema [20]. The evaluation of cardiac function has only supportive character in this definition. However, EC studies indicated that myocarditis patients show impaired cardiac strains despite a pEF and that the assessment of cardiac deformation has the potential to improve the diagnosis in these patients [21, 22]. The assessment of cardiac strains in CMR examinations can be performed by FTI with little effort and without the need for additional scans or sequences as standard cine SSFP images are utilised. For this purpose, the FTI algorithm tracks the motion of cardiac features as tissue inhomogeneities in relation to each other throughout the cardiac cycle. As mentioned before, prior studies demonstrated an excellent intra- and inter-observer reproducibility as well as a good inter-study agreement [9, 10]. Furthermore, FTI-derived strain measurements showed an independency of field strengths of 1.5 and 3 T [23]. The application of deformation analyses on CMR studies offers the possibility to gain information on cardiac morphology, function and tissue in a single non-invasive examination. This may be beneficial for the assessment of patients with suspected or proven myocarditis in clinical routine as well as for research purposes.
The strain measurements performed in this study allowed for a good differentiation between myocarditis patients and healthy controls leading to high AUC values in the ROC analysis, which is in agreement with prior EC findings [24]. Sensitivity and specificity reached a considerable level so that the definition of cut-off values for the differentiation between healthy and diseased subjects seems feasible. However, previous studies on the cardiac deformation of healthy volunteers showed, that strain values are age- and gender-dependent and that the use of specific reference values is recommendable [9, 10, 11]. As the size of the population of the current study did not allow for the formation of subgroups with regard to age and gender, we applied previously published reference values [10, 18].
Applying a cut-off value, which was defined as 1 SD from the mean given in literature, 39 % of the patients showed a global peak circumferential, 69 % a global peak longitudinal and 72 % a global peak radial systolic strain value that was outside the normal range. If all strain values are evaluated, 83 % of all myocarditis patients revealed at least one abnormal result. However, as the strain values of the underlying reference population showed a normal distribution, about 15.9 % of the healthy subjects have per definition values, which are outside a one-sided reference interval applying 1 SD. A combination of different cut-off values increases the probability that at least one of them is outside the reference range. Therefore, we used a second reference interval, which was defined as one-sided with 2 SD from the reference mean value. In this case, only about 2.3 % of healthy subjects fall below the limit. Yet, in myocarditis patients, the limit was exceeded in 19 % of the global peak circumferential systolic strain values, in 36 % of the global peak longitudinal systolic strain values and in 19 % and of the global peak radial systolic strain values. A combined analysis of all these values led to 47 % of the cases showing at least one abnormal result.
When we focused on the myocarditis patients with pEF, the combination of values led to 69 % or 25 % of the cases, respectively, which exceeded the limit when 1 or 2 SD were applied to define the threshold. When the LAS was included 75 % or 31 % of patients with pEF showed a least one value, which fell below the limit of 1 or 2 SD.
Although, we defined a high threshold of ≥55 % for a pEF, the assessment of global peak systolic strains and LAS yielded positive results in these patients.
The logistic regression model, which comprised all assessed global peak systolic strains and the EF as significant parameters, showed an excellent fit with a correct classification in over 90 % of the cases. Therefore, the assessment of global peak systolic strains may have an incremental value to the established criteria for the detection of myocarditis. These results support findings from the trial of Hsiao et al., who assessed cardiac strain in myocarditis patients applying EC speckle tracking [24]. In this study on 45 myocarditis patients and 83 healthy controls, the cardiac deformation parameters were still significant predictors for myocarditis after the adjustment for gender, septal thickness, EF and SV index.
In contrast to a previous EC trial of diBella et al., our study showed significant differences regarding not only the longitudinal but also the radial and the circumferential strain between myocarditis patients and healthy subjects [21]. Besides, the study cohort of the EC trial was relatively small consisting of only 13 male myocarditis patients and 13 healthy controls. Our findings are supported by the results of other EC studies on patients with myo- or perimyocarditis, which showed a significant reduction of the longitudinal and circumferential strains whereas radial strains were not assessed [24, 25].
Besides its diagnostic value, the assessment of cardiac deformation may contribute to risk stratification. Escher et al. could show that patients with biopsy-proven persistent inflammation have a reduced longitudinal strain as measured by EC speckle tracking compared to those patients who showed a recovery [26]. Furthermore, the longitudinal strain correlated with lymphocytic infiltrates which are a predictor of poor outcome [27]. The EC study of Hsiao et al. showed, that a decline of the circumferential or longitudinal strain was associated to major clinical events during a median follow-up period of 14.7 months [24]. Regarding CMR, the presence of LGE is a strong predictor of long-term outcome [3]. Thus, the combination with FTI-derived strain may further enhance the prognostic value of CMR examinations in myocarditis patients.
Limitations
As in most of the prior trials, the number of myocarditis patients in our retrospective analysis was relatively small. We accounted for that by drawing a reference population who was matched regarding not only age and gender but also BMI and BSA. Even the subgroup of myocarditis patients with pEF showed no significant differences of the assessed basic anthropometric parameters to the healthy volunteers. Yet, the number of cases in the subgroups was relatively small handicapping the statistical analysis. Potentially, bigger groups might have led to more distinct statistical results.
The current CMR study has no follow-up data, so that the prognostic value of the FTI-derived cardiac strains could not be assessed. This might be an objective of future trials.
CMR offers the possibility of advanced tissue characterization by using mapping techniques, which showed promising results in previous trials [28, 29]. Yet, the assessment of these techniques was beyond the scope of this study. Further trials might address the incremental diagnostic benefit of a combination of cardiac strain analysis with tissue characterization in myocarditis patients.
Conclusions
The assessment of cardiac strains applying FTI on standard cine CMR images is feasible in patients with acute myocarditis. As patients in total as well as with preserved ejection fraction showed significantly reduced cardiac strains, FTI may contribute to the diagnosis of myocarditis without the need for additional scans. Further studies are needed to assess its incremental beneficial value for diagnosis and risk stratification especially in combination with mapping techniques.
References
Fabre A, Sheppard MN (2006) Sudden adult death syndrome and other non-ischaemic causes of sudden cardiac death. Heart 92(3):316–320. doi:10.1136/hrt.2004.045518
Doolan A, Langlois N, Semsarian C (2004) Causes of sudden cardiac death in young Australians. Med J Aust 180(3):110–112
Grun S, Schumm J, Greulich S, Wagner A, Schneider S, Bruder O, Kispert EM, Hill S, Ong P, Klingel K, Kandolf R, Sechtem U, Mahrholdt H (2012) Long-term follow-up of biopsy-proven viral myocarditis: predictors of mortality and incomplete recovery. J Am Coll Cardiol 59(18):1604–1615. doi:10.1016/j.jacc.2012.01.007
Pennell DJ (2010) Cardiovascular magnetic resonance. Circulation 121(5):692–705. doi:10.1161/CIRCULATIONAHA.108.811547
Schumm J, Greulich S, Wagner A, Grun S, Ong P, Bentz K, Klingel K, Kandolf R, Bruder O, Schneider S, Sechtem U, Mahrholdt H (2014) Cardiovascular magnetic resonance risk stratification in patients with clinically suspected myocarditis. J Cardiovasc Magn Reson 16:14. doi:10.1186/1532-429X-16-14
Cho GY, Marwick TH, Kim HS, Kim MK, Hong KS, Oh DJ (2009) Global 2-dimensional strain as a new prognosticator in patients with heart failure. J Am Coll Cardiol 54(7):618–624. doi:10.1016/j.jacc.2009.04.061
Buss SJ, Emami M, Mereles D, Korosoglou G, Kristen AV, Voss A, Schellberg D, Zugck C, Galuschky C, Giannitsis E, Hegenbart U, Ho AD, Katus HA, Schonland SO, Hardt SE (2012) Longitudinal left ventricular function for prediction of survival in systemic light-chain amyloidosis: incremental value compared with clinical and biochemical markers. J Am Coll Cardiol 60(12):1067–1076. doi:10.1016/j.jacc.2012.04.043
Korosoglou G, Gitsioudis G, Voss A, Lehrke S, Riedle N, Buss SJ, Zugck C, Giannitsis E, Osman NF, Katus HA (2011) Strain-encoded cardiac magnetic resonance during high-dose dobutamine stress testing for the estimation of cardiac outcomes: comparison to clinical parameters and conventional wall motion readings. J Am Coll Cardiol 58(11):1140–1149. doi:10.1016/j.jacc.2011.03.063
Taylor RJ, Moody WE, Umar F, Edwards NC, Taylor TJ, Stegemann B, Townend JN, Hor KN, Steeds RP, Mazur W, Leyva F (2015) Myocardial strain measurement with feature-tracking cardiovascular magnetic resonance: normal values. Eur Heart J. doi:10.1093/ehjci/jev006
Andre F, Steen H, Matheis P, Westkott M, Breuninger K, Sander Y, Kammerer R, Galuschky C, Giannitsis E, Korosoglou G, Katus HA, Buss SJ (2015) Age- and gender-related normal left ventricular deformation assessed by cardiovascular magnetic resonance feature tracking. J Cardiovasc Magn Reson 17(1):25. doi:10.1186/s12968-015-0123-3
Augustine D, Lewandowski AJ, Lazdam M, Rai A, Francis J, Myerson S, Noble A, Becher H, Neubauer S, Petersen SE, Leeson P (2013) Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: comparison with tagging and relevance of gender. J Cardiovasc Magn Reson 15:8. doi:10.1186/1532-429X-15-8
Hor KN, Gottliebson WM, Carson C, Wash E, Cnota J, Fleck R, Wansapura J, Klimeczek P, Al-Khalidi HR, Chung ES, Benson DW, Mazur W (2010) Comparison of magnetic resonance feature tracking for strain calculation with harmonic phase imaging analysis. Cardiovas Imaging 3(2):144–151. doi:10.1016/j.jcmg.2009.11.006
Onishi T, Saha SK, Ludwig DR, Onishi T, Marek JJ, Cavalcante JL, Schelbert EB, Schwartzman D, Gorcsan J 3rd (2013) Feature tracking measurement of dyssynchrony from cardiovascular magnetic resonance cine acquisitions: comparison with echocardiographic speckle tracking. J Cardiovasc Magn Reson 15:95. doi:10.1186/1532-429X-15-95
Williams LK, Urbano-Moral JA, Rowin EJ, Jamorski M, Bruchal-Garbicz B, Carasso S, Pandian NG, Maron MS, Rakowski H (2013) Velocity vector imaging in the measurement of left ventricular myocardial mechanics on cardiac magnetic resonance imaging: correlations with echocardiographically derived strain values. J Am Soc Echocardiogr 26(10):1153–1162. doi:10.1016/j.echo.2013.06.008
Moody WE, Taylor RJ, Edwards NC, Chue CD, Umar F, Taylor TJ, Ferro CJ, Young AA, Townend JN, Leyva F, Steeds RP (2015) Comparison of magnetic resonance feature tracking for systolic and diastolic strain and strain rate calculation with spatial modulation of magnetization imaging analysis. J Magn Reson Imaging 41(4):1000–1012. doi:10.1002/jmri.24623
Mosteller RD (1987) Simplified calculation of body-surface area. N Engl J Med 317(17):1098. doi:10.1056/NEJM198710223171717
Giannitsis E, Kurz K, Hallermayer K, Jarausch J, Jaffe AS, Katus HA (2009) Analytical validation of a high-sensitivity cardiac troponin T assay. Clin Chem 56(2):254–261. doi:10.1373/clinchem.2009.132654
Riffel JH, Andre F, Maertens M, Rost F, Keller MG, Giusca S, Seitz S, Kristen AV, Muller M, Giannitsis E, Korosoglou G, Katus HA, Buss SJ (2015) Fast assessment of long axis strain with standard cardiovascular magnetic resonance: a validation study of a novel parameter with reference values. J Cardiovasc Magn Reson 17(1):69. doi:10.1186/s12968-015-0171-8
Schulz-Menger J, Bluemke DA, Bremerich J, Flamm SD, Fogel MA, Friedrich MG, Kim RJ, von Knobelsdorff-Brenkenhoff F, Kramer CM, Pennell DJ, Plein S, Nagel E (2013) Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) board of trustees task force on standardized post processing. J Cardiovasc Magn Reson 15:35. doi:10.1186/1532-429X-15-35
Friedrich MG, Sechtem U, Schulz-Menger J, Holmvang G, Alakija P, Cooper LT, White JA, Abdel-Aty H, Gutberlet M, Prasad S, Aletras A, Laissy JP, Paterson I, Filipchuk NG, Kumar A, Pauschinger M, Liu P, International Consensus Group on Cardiovascular Magnetic Resonance in Myocarditis (2009) Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol 53(17):1475–1487. doi:10.1016/j.jacc.2009.02.007
Di Bella G, Gaeta M, Pingitore A, Oreto G, Zito C, Minutoli F, Anfuso C, Dattilo G, Lamari A, Coglitore S, Carerj S (2010) Myocardial deformation in acute myocarditis with normal left ventricular wall motion—a cardiac magnetic resonance and 2-dimensional strain echocardiographic study. Circulation 74(6):1205–1213
Khoo NS, Smallhorn JF, Atallah J, Kaneko S, Mackie AS, Paterson I (2012) Altered left ventricular tissue velocities, deformation and twist in children and young adults with acute myocarditis and normal ejection fraction. J Am Soc Echocardiogr 25(3):294–303. doi:10.1016/j.echo.2011.10.010
Schuster A, Morton G, Hussain ST, Jogiya R, Kutty S, Asrress KN, Makowski MR, Bigalke B, Perera D, Beerbaum P, Nagel E (2013) The intra-observer reproducibility of cardiovascular magnetic resonance myocardial feature tracking strain assessment is independent of field strength. Eur J Radiol 82(2):296–301. doi:10.1016/j.ejrad.2012.11.012
Hsiao JF, Koshino Y, Bonnichsen CR, Yu Y, Miller FA Jr, Pellikka PA, Cooper LT Jr, Villarraga HR (2013) Speckle tracking echocardiography in acute myocarditis. Int J Cardiovasc Imaging 29(2):275–284. doi:10.1007/s10554-012-0085-6
Leitman M, Bachner-Hinenzon N, Adam D, Fuchs T, Theodorovich N, Peleg E, Krakover R, Moravsky G, Uriel N, Vered Z (2011) Speckle tracking imaging in acute inflammatory pericardial diseases. Echocardiography 28(5):548–555. doi:10.1111/j.1540-8175.2010.01371.x
Escher F, Kasner M, Kuhl U, Heymer J, Wilkenshoff U, Tschope C, Schultheiss HP (2013) New echocardiographic findings correlate with intramyocardial inflammation in endomyocardial biopsies of patients with acute myocarditis and inflammatory cardiomyopathy. Mediat Inflamm 2013:875420. doi:10.1155/2013/875420
Kindermann I, Kindermann M, Kandolf R, Klingel K, Bultmann B, Muller T, Lindinger A, Bohm M (2008) Predictors of outcome in patients with suspected myocarditis. Circulation 118(6):639–648. doi:10.1161/CIRCULATIONAHA.108.769489
Radunski UK, Lund GK, Stehning C, Schnackenburg B, Bohnen S, Adam G, Blankenberg S, Muellerleile K (2014) CMR in patients with severe myocarditis: diagnostic value of quantitative tissue markers including extracellular volume imaging. Cardiovasc Imaging 7 (7):667–675. doi:10.1016/j.jcmg.2014.02.005
Hinojar R, Foote L, Arroyo Ucar E, Jackson T, Jabbour A, Yu CY, McCrohon J, Higgins DM, Carr-White G, Mayr M, Nagel E, Puntmann VO (2015) Native T1 in discrimination of acute and convalescent stages in patients with clinical diagnosis of myocarditis: a proposed diagnostic algorithm using CMR. Cardiovasc Imaging 8 (1):37–46. doi:10.1016/j.jcmg.2014.07.016
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Informed consent
All individual participants of the study gave informed consent to the clinically indicated examinations. For the retrospective analysis of the obtained data a waiver of all consents was granted from the institutional research committee.
Rights and permissions
About this article

Cite this article
André, F., Stock, F.T., Riffel, J. et al. Incremental value of cardiac deformation analysis in acute myocarditis: a cardiovascular magnetic resonance imaging study. Int J Cardiovasc Imaging 32, 1093–1101 (2016). https://doi.org/10.1007/s10554-016-0878-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-016-0878-0