
Abstract
The purpose of this study was to explore the feasibility of subtraction coronary computed tomography angiography (CCTA) by second-generation 320-detector row CT in patients with severe coronary artery calcification using invasive coronary angiography (ICA) as the gold standard. This study was approved by the institutional board, and all subjects provided written consent. Twenty patients with calcium scores of >400 underwent conventional CCTA and subtraction CCTA followed by ICA. A total of 82 segments were evaluated for image quality using a 4-point scale and the presence of significant (>50 %) luminal stenosis by two independent readers. The average image quality was 2.3 ± 0.8 with conventional CCTA and 3.2 ± 0.6 with subtraction CCTA (P < 0.001). The percentage of segments with non-diagnostic image quality was 43.9 % on conventional CCTA versus 8.5 % on subtraction CCTA (P = 0.004). The segment-based diagnostic accuracy for detecting significant stenosis according to ICA revealed an area under the receiver operating characteristics curve of 0.824 (95 % confidence interval [CI], 0.750–0.899) for conventional CCTA and 0.936 (95 % CI 0.889–0.936) for subtraction CCTA (P = 0.001). The sensitivity, specificity, positive predictive value, and negative predictive value for conventional CCTA were 88.2, 62.5, 62.5, and 88.2 %, respectively, and for subtraction CCTA they were 94.1, 85.4, 82.1, and 95.3 %, respectively. As compared to conventional, subtraction CCTA using a second-generation 320-detector row CT showed improvement in diagnostic accuracy at segment base analysis in patients with severe calcifications.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
One of the major problems in coronary computed tomography angiography (CCTA) is the presence of severe calcification in the coronary arteries, which may interfere with assessment of the lumen. Severe calcification frequently reduces diagnostic accuracy and may even make it impossible to evaluate some arteries for the presence of stenosis [1–4].
On the other hand, we reported subtraction CCTA for such calcifications using first-generation 320-detector row CT. In subtraction CCTA, calcifications in the coronary arteries were eliminated by subtracting precontrast CT image data from contrast-enhanced CCTA image data [5–7].
Recently, a second-generation 320-detector row CT has been introduced. The gantry rotation time for a new second-generation scanner is faster than that of the first-generation scanner (275 vs. 350 ms), which may contribute to the improvement of temporal resolution.
The objective of this study was to assess the feasibility of subtraction CCTA by the second-generation 320-detector row scanner in patients with high calcium scores. We evaluated the ability of subtraction CCTA to improve calcified segment interpretation compared to conventional CCTA, using invasive coronary angiography (ICA) as the gold standard.
Materials and methods
Patient population
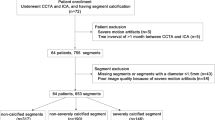
Twenty patients with suspected or known coronary artery disease and a coronary calcium score >400 (Agatston score) were prospectively enrolled from August 2012 in this study. All patients were clinically referred for CCTA and followed by ICA. Exclusion criteria were known allergy to iodinated contrast media, estimated glomerular filtration rate of <45 ml/min/1.73 m2, arrhythmia, previous cardiac surgery, coronary intervention within the past 6 months, evidence of acute coronary syndrome, heart failure of New York Heart Association functional class III or IV, aortic stenosis, intolerance to beta-blockers, body mass index >40 kg/m2, and inability to perform a 20–40 s breath-hold.
This study was approved by the institutional review board, and all patients gave written informed consent.
Invasive coronary angiography (ICA)
Clinically-indicated ICA was performed using the standard technique within 60 days after CCTA using the standard technique. The procedure was performed with a 4-F catheter. Quantitative coronary analysis (QCA) was performed by an observer with more than 15 years of experience using a software program (XA version 7.1, Medis Medical Imaging System, Leiden, The Netherlands). QCA was performed in coronary segments that exceeded 20 % luminal stenosis on visual assessment. Significant stenosis was defined as >50 % luminal reduction of the maximum stenosis.
Coronary CT angiography (CCTA)
Patients underwent axial imaging with a second-generation, 320 × 0.5-mm detector row CT scanner (Aquilion ONE ViSION Edition; Toshiba Medical Systems, Otawara, Japan) with a gantry rotation time of 275 ms. Images were reconstructed with a 512 × 512 matrix, 0.5-mm-thickness by using kernel FC44, iterative reconstruction (Adaptive Iterative Dose Reduction 3D, AIDR 3D, Toshiba Medical Systems) standard.
Patients with a heart rate greater than 75 bpm received intravenous beta-blockers (Landiolol Hydrochloride) at a rate of 0.125 mg/kg (maximum, 12.5 mg).
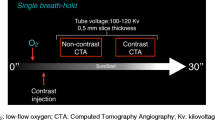
The imaging technique for CCTA has been reported previously [7]. In brief, the coronary calcium scoring scan was performed, and coronary calcium was calculated immediately on the console using the Agatston method [8]. Patients with a coronary calcium score >400 underwent subtraction CCTA. The subtraction CCTA protocol consisted of two CCTA scans, one precontrast and one contrast-enhanced scan, at identical settings. The contrast-enhanced scan was obtained immediately after the precontrast scan in a single breath-hold of 20–40 s.
The contrast-enhance scan was performed with iodinated contrast (iohexol 350, Daiichi Sankyo Company, Tokyo, Japan) injected intravenously at a rate of 0.07 × body weight (BW) ml/s in 10 s, followed by a 30 ml saline chaser bolus. To determine the scan start time, a test bolus technique of 0.07 × BW × 3 ml, followed by a saline chaser bolus of BW × 0.25 ml, was used. The coverage of both the precontrast and postcontrast scan was up to 16 cm. The tube voltage was 120 kV, and the target noise for the tube current was set at 28 Hounsfield units. All patients were imaged with prospective ECG-gating. The acquisition phase window (padding) was 65–80 %.
The effective radiation dose was estimated based on the dose-length product (DLP, mGy × cm) using the formula effective radiation dose = DLP × k, where k = 0.014 mSv × mGy−1 × cm−1.
Subtraction method
The subtraction technique was also reported previously [7]. Subtraction was performed using a dedicated algorithm “volumetric CT digital subtraction angiography” [9]. The subtraction images were obtained by subtracting the precontrast images from the contrast-enhanced images. In the first step, a global non-rigid registration was performed. In the next step, a local rigid registration for the targeted coronary segment was followed. As a result, the obtained subtraction images were only images of the targeted segments with calcification.
Image evaluation
The acquired conventional CCTA images and subtraction CCTA images were transferred to a workstation (Zio M900; Ziosoft, Tokyo, Japan) to generate a curved planar reformation (CPR) image and cross-sectional images. With regard to subtraction CCTA, these images were obtained only for the target artery or the segment with severe calcification. Severe calcification was defined as more than one quadrant calcification on a cross-sectional image of conventional CCTA.
First, the conventional CCTA images were evaluated for image quality and the presence of significant stenosis, defined as >50 % luminal narrowing. Two experienced observers with more than 10 years of experience performed the evaluation. They were blinded to the results of ICA but aware of the clinical history of the patients. Discrepancies were settled by consensus.
Axial slices, CPR images, and cross-sectional images were used for evaluation. Cross-sectional images were used for caliper measurements. The coronary arteries were divided into 17 segments according to the American Heart Association classification. Only segments with severe calcification were evaluated. Consequently, the same segments were evaluated on subtraction CCTA.
Image quality was evaluated using a 4-point scale method [10] on conventional CCTA images. Each segment was graded as (1) uninterpretable; evaluation not possible, (2) poor; severe artifacts limiting adequate evaluation of the segment (low reader confidence), (3) moderate; some artifact present, but interpretation possible (moderate reader confidence), or (4) good; good image quality without artifact (high reader confidence). Scores of 1 or 2 were considered to reflect non-diagnostic quality. The presence of significant stenosis (>50 % stenosis) was also determined.
The same observers performed an analysis of the subtraction CCTA images. In this process, both subtraction CCTA images and conventional CCTA images were used to allow the subtraction CCTA images to be verified with the original contrast enhanced images. Image quality and the presence of significant stenosis were assessed as described above.
Data and statistical analysis
We evaluated the data on a segment level. Segments with a coronary stent were excluded. The average image quality scores between conventional CCTA and subtraction CCTA were compared using a paired t test. The diagnostic image quality versus non-diagnostic image quality frequencies were compared using a McNemar’s test. Interobserver agreement was assessed based on the proportion of agreement and the value of the kappa coefficient.
Heart rate between the precontrast scan and contrast-enhanced scan was compared using a paired t test
The conventional CCTA and subtraction CCTA diagnostic accuracies (sensitivity, specificity, positive predictive value, negative predictive value) for detecting significant stenosis (>50 %) were assessed. ICA graded with QCA was used as the gold standard. To assess diagnostic accuracy, the area under the curve (AUC) of the receiver operating characteristic (ROC) was calculated for both conventional CCTA and subtraction CCTA. The ROC analysis was performed using R version 3.0.1 (The R Foundation for Statistical Computing) and pROC version 1.7.3 [11]. The Venkatraman method was used for comparison of the two ROC curves. The statistical analysis, except ROC analyses, was performed using PASW Statistics 21 (SPSS, Inc) for Microsoft Windows.
All statistical analyses were done with a 95 % CI.
Results
All 20 patients underwent both subtraction CCTA and ICA successfully. Patient characteristics of these 20 patients are specified in Table 1. The average coronary calcium score was 938 ± 640. Six patients (30 %) received intravenous beta blockers for heart rate control. Heart rate during the precontrast scan was 58.1 ± 5.8 beats/min (range, 50–69 beats/min). Heart rate during the contrast-enhanced scan was 57.7 ± 6.2 beats/min (range, 46–69 beats/min). There was no significant difference in heart rate between the precontrast scan and contrast-enhanced scan (P = 0.856). The number of selected detector rows was 280 rows in 3 cases, 256 rows in 4 cases, 240 rows in 10 cases, 200 rows in 1 case, and 120 rows in two cases. The average tube current was 260.5 ± 13.3 mA (range, 120–350 mA). The estimated effective radiation dose of subtraction CCTA (summation of precontrast and contrast-enhanced scan) was 3.20 ± 1.80 mSv (range, 1.16–8.80 mSv). A total of 82 calcified segments were evaluated. ICA revealed significant stenosis in 13 patients (65 %). Significant stenosis was observed in 34 of 82 (41 %) evaluated calcified segments. The median interval between CCTA and ICA was 31.3 ± 12.6 days (range, 3–49 days).
Conventional CCTA
The average image quality of conventional CCTA in all segments was 2.3 ± 0.8 (Table 2). The inter-observer kappa score for image quality score was 0.917. The AUC for conventional CCTA was 0.824 (95 % CI 0.750–0.899) for diagnosis of a segment with stenosis of >50 % as assessed by QCA (Fig. 1). Segmental sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were 88.2, 62.5, 62.5, 88.2, and 73.2 %, respectively (Table 3).

Area under the receiver operating curve characteristics of conventional CCTA and subtraction CCTA versus invasive coronary angiography
Subtraction CCTA
The average image quality of subtraction CCTA in all segments was 3.2 ± 0.6 (Table 2), which is significantly higher than conventional CCTA (P < 0.001). Image quality was reduced by mis-registration artifact in all affected segments. The inter-observer kappa score for image quality score was 0.870. The AUC for the diagnosis of a segment with stenosis of >50 % as assessed by QCA (Fig. 1) was 0.936 (95 % CI 0.889–0.983), which was significantly higher than for conventional CCTA (P = 0.001). Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were 94.1, 85.4, 82.1, 95.3 and 89.0 %, respectively (Table 3). Moreover, the percentage of segments with non-diagnostic image quality significantly decreased from 43.9 % (36 segments) to 8.5 % (7 segments) with subtraction CCTA (P = 0.004) (Table 2). Case examples are provided in Figs. 2 and 3.

An 81-year-old man with severe coronary artery calcification (calcium score = 675). a Conventional CCTA. Curved planar reformation image of the right coronary artery. A nodular calcification makes it difficult to assess the lumen (arrowhead). b Subtraction CCTA. Curved planar reformation image at the same position as in a. The calcification is eliminated, and severe stenosis is depicted (arrowhead). c Invasive coronary angiography. The severe stenosis is demonstrated in the right coronary artery (arrowhead)

A 77-year-old man with severe coronary artery calcification (calcium score = 1612). a Conventional CCTA. Curved planar reformation image of the left circumflex artery. Severe calcifications make it difficult to assess the lumen (arrowhead). b Subtraction CCTA. Curved planar reformation image at the same position as in a. The severe calcifications are eliminated, and no significant stenosis is depicted (arrowhead). c Conventional CCTA. A cross-sectional image of the left circumflex artery at the site of severe calcification. The semicircular calcification makes it difficult to assess the lumen (arrowhead). d Subtraction CCTA. A cross-sectional image at the same position as in c. The calcification is eliminated, making it possible to assess the lumen (arrowhead). e Invasive coronary angiography (superselective injection to the left circumflex artery due to the short left main trunk). No significant stenosis is demonstrated in the left circumflex artery (arrowhead)
Discussion
Subtraction CCTA using a second-generation 320-detector row CT provided improved diagnostic accuracy over conventional CCTA in patients with severe coronary artery calcification. This study represents the initial subtraction CCTA experience using a new second-generation 320-detector row CT system.
One of the major challenges in CCTA is the presence of severe calcification, which reduces diagnostic accuracy and may make it impossible to assess luminal stenosis. A multicenter study evaluating the diagnostic performance of coronary artery stenosis using a 64-detector CT revealed that calcium scores > 400 reduced specificity significantly [1]. A guideline shows that patients with a calcium score under 400 or equal to 400 are adequate for the decision to perform CCTA [12]. This is the reason why we enrolled patients with a calcium score >400 in this study.
Theoretically, calcifications may be eliminated by subtracting precontrast CT image data from contrast-enhanced CT angiography data. The subtraction requires images to be acquired at the same location and temporal phase before and after contrast administration. In 320-detector row CT, image data up to 16 cm in the z-axis direction can be acquired in a single rotation, permitting the entire heart to be scanned during a single heartbeat without moving the table. We considered that these unique features of the 320-detector row CT might be suitable to perform coronary artery subtraction. We reported the preliminary results of subtraction CCTA in patients with severe calcification using a first-generation 320-detector row CT [7]. In this study, subtraction CCTA was shown to be feasible, although not yet ready for clinical use.
Recently, a new second-generation 320-detector row CT scanner has been introduced. The gantry rotation time is reduced from 350 to 275 ms, resulting in improved temporal resolution. Accordingly, motion related artifact may be reduced. Chen et al. [13] showed that significantly better image quality was achieved by the second-generation system compared with the first-generation unit. For coronary artery subtraction, accurate registration between the two datasets is essential. Motion artifact should be avoided as much as possible as it may result in potential misregistration and image degradation. Therefore, we hypothesized that the higher temporal resolution can contribute to improved diagnostic performance of subtraction CCTA.
In the present study, the AUC of subtraction CCTA (0.936) was higher than that of conventional CCTA (0.824) (P = 0.001). These findings demonstrate that subtraction CCTA is effective in the diagnosis of significant stenosis in segments with severe calcifications.
The specificity and positive predictive value of conventional CCTA was low due to the high number of false positive segments. Severe calcifications obscure the patency of the lumen in conventional CCTA resulting in overestimation of the degree of stenosis. On the other hand, subtraction CCTA allowed the assessment of the lumen in such lesions by removing severe calcifications. The number of false positive segments in subtraction CCTA was reduced from 18 segments to 7 segments. As a result, the specificity and positive predictive value by subtraction CCTA was improved over 20 %. In subtraction CCTA using first-generation 320-detector row CT, an improvement in specificity and positive predictive value of approximately 10 and 5 %, respectively, was seen [7]. This is the major difference between subtraction CCTA using second-generation and first-generation 320-detector row CT. The image quality score of subtraction CCTA by second-generation 320-detector row CT (3.2 ± 0.6) showed no remarkable change compared with that of the first-generation scanner (3.1 ± 0.6). The percentage of segments with diagnostic image quality of subtraction CCTA by second-generation 320-detector row CT (87.3 %) also showed no remarkable difference as compared with the first-generation 320-detector scanner (91.5 %).
These results suggest that the second-generation 320-detector row CT allows for the correct diagnosis of significant stenosis even more often than first-generation scanners in successfully subtracted segments. Accurate caliber measurements in subtraction CCTA require images without misregistration artifacts. Most likely, misregistration artifacts that may not render a segment uninterpretable but do reduce image quality to less than excellent (such as image quality score 3) occur less frequently with second-generation 320-detector row CT than with first-generation scanners.
It is important to minimize the radiation dose in subtraction CCTA, because it requires two radiation exposures. We used the iterative reconstruction method as previously reported using the first-generation scanner [7]. We also employed the technique of optimizing the image range in the z-axis direction. In 320-detector row CT, the scan range in the z-axis direction can be reduced according to the size of the patient’s heart in order to minimize the radiation dose. It is possible to select 280 rows (14 cm), 256 rows (12.8 cm), 240 rows (12 cm), 200 rows (10 cm), 160 rows (8 cm,) or 120 rows (6 cm). Compared with scanning using the full 320 rows, the radiation dose is reduced to 12.5, 20, 25, 37.5, 50, and 62.5 %, respectively. We employed this technique in all cases, and 240 rows were most frequently (50 %) selected in this study. As a result, the mean estimated effective radiation dose of subtraction CCTA, the sum of the precontrast and contrast-enhancement scan, was 3.20 mSv (range, 1.16–8.80 mSv). These values are lower than the previously described experience with first-generation 320-detector row CT (5.21 mSv; range, 3.05–10.13 mSv). Setting a tube voltage of 100 kV is also considered to be an effective method for reducing radiation dose in 320-detector row CT [13, 14]. However, this method may also be effective in subtraction CCTA, but we had no experience with this at the time of data acquisition.
This study has some limitations. The first major limitation of this study is that only a small number of patients were studied. While the current study shows the feasibility of subtraction CCTA in segment-based analysis, no patient-based or vessel-based analysis can be made. Second, image quality and diagnostic accuracy in this study were not directly compared with results from the first-generation 320-detector row CT in the same patients. However, it is very difficult to do two sequential examinations using first-generation and second-generation scanners in a clinical setting. Third, the mean coronary calcium score in this study was only 938. Therefore, further study is needed to explore the feasibility of subtraction CCTA in patients with very high calcium scores. Finally, the subtraction algorithm still needs optimization to reduce misregistration artifact. There were fewer false positive lesions in subtraction CCTA than in conventional CCTA, but overestimation still occurred. Misregistration artifacts frequently caused “pseudo” luminal narrowing in these cases.
In conclusion, as compared to conventional CCTA, subtraction CCTA using a second-generation 320-detector row CT showed improvement in diagnostic accuracy at segment-based analysis in patients with severe calcifications.
References
Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, Scherer M, Bellinger R, Martin A, Benton R, Delago A, Min JK (2008) Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (assessment by coronary computed tomographic angiography of individuals undergoing invasive coronary angiography) trial. J Am Coll Cardiol 52(21):1724–1732
Vavere AL, Arbab-Zadeh A, Rochitte CE, Dewey M, Niinuma H, Gottlieb I, Clouse ME, Bush DE, Hoe JW, de Roos A, Cox C, Lima JA, Miller JM (2011) Coronary artery stenoses: accuracy of 64-detector row CT angiography in segments with mild, moderate, or severe calcification–a subanalysis of the CORE-64 trial. Radiology 261(1):100–108
Abdulla J, Pedersen KS, Budoff M, Kofoed KF (2012) Influence of coronary calcification on the diagnostic accuracy of 64-slice computed tomography coronary angiography: a systematic review and meta-analysis. Int J Cardiovasc Imaging 28(4):943–953
Arbab-Zadeh A, Miller JM, Rochitte CE, Dewey M, Niinuma H, Gottlieb I, Paul N, Clouse ME, Shapiro EP, Hoe J, Lardo AC, Bush DE, de Roos A, Cox C, Brinker J, Lima JA (2012) Diagnostic accuracy of computed tomography coronary angiography according to pre-test probability of coronary artery disease and severity of coronary arterial calcification. The CORE-64 (coronary artery evaluation using 64-row multidetector computed tomography angiography) International Multicenter Study. J Am Coll Cardiol 59(4):379–387
Yoshioka K, Miyata Y (1983) Changes in the distribution of the extrajunctional acetylcholine sensitivity along muscle fibers during development and following cordotomy in the rat. Neuroscience 9(2):437–443
Yoshioka K, Tanaka R, Muranaka K (2012) Subtraction coronary CT angiography for calcified lesions. Cardiol Clin 30(1):93–102
Tanaka R, Yoshioka K, Muranaka K, Chiba T, Ueda T, Sasaki T, Fusazaki T, Ehara S (2013) Improved evaluation of calcified segments on coronary CT angiography: a feasibility study of coronary calcium subtraction. Int J Cardiovasc Imaging 29(Suppl 2):75–81
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R (1990) Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15(4):827–832
Razeto M, Matthews J, Masood S, Steel J, Arakita K (2013) Accurate registration of coronary arteries for volumetric CT digital subtraction angiography. roc SPIE 8768, international conference on graphic and image processing (ICGIP 2012), pp 876834–876836
Meijboom WB, Meijs MF, Schuijf JD, Cramer MJ, Mollet NR, van Mieghem CA, Nieman K, van Werkhoven JM, Pundziute G, Weustink AC, de Vos AM, Pugliese F, Rensing B, Jukema JW, Bax JJ, Prokop M, Doevendans PA, Hunink MG, Krestin GP, de Feyter PJ (2008) Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 52(25):2135–2144
Robin X, Turck N, Hainard A, Tiberti N, Lisacek F, Sanchez JC, Muller M (2011) pROC: an open-source package for R and S + to analyze and compare ROC curves. BMC Bioinform 12:77
Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O’Gara P, Rubin GD, American College of Cardiology Foundation Appropriate Use Criteria Task F, Society of Cardiovascular Computed T, American College of R, American Heart A, American Society of E, American Society of Nuclear C, North American Society for Cardiovascular I, Society for Cardiovascular A, Interventions, Society for Cardiovascular Magnetic R, Kramer CM, Berman D, Brown A, Chaudhry FA, Cury RC, Desai MY, Einstein AJ, Gomes AS, Harrington R, Hoffmann U, Khare R, Lesser J, McGann C, Rosenberg A, Schwartz R, Shelton M, Smetana GW, Smith SC Jr (2010) ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 56(22):1864–1894
Chen MY, Shanbhag SM, Arai AE (2013) Submillisievert median radiation dose for coronary angiography with a second-generation 320-detector row CT scanner in 107 consecutive patients. Radiology 267(1):76–85
Zhang C, Zhang Z, Yan Z, Xu L, Yu W, Wang R (2011) 320-Row CT coronary angiography: effect of 100-kV tube voltages on image quality, contrast volume, and radiation dose. Int J Cardiovasc Imaging 27(7):1059–1068
Acknowledgments
Dr. Joanne Schuijf and Mrs. Yukie Osawa from Toshiba Medical Systems gave support and suggestions in writing and technical subjects, especially for the dedicated subtraction algorithms. This work was supported by the Japan Society for the Promotion of Science (JSPS KAKENHI, Grant Number 26461803).
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yoshioka, K., Tanaka, R., Muranaka, K. et al. Subtraction coronary CT angiography using second-generation 320-detector row CT. Int J Cardiovasc Imaging 31 (Suppl 1), 51–58 (2015). https://doi.org/10.1007/s10554-015-0630-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-015-0630-1