
Abstract
Purpose
The association between smoking and the risk of skin cancers has been studied without reaching consistent findings. This study aims to assess this association through an updated meta-analysis of cohort studies.
Methods
We retrieved cohort studies that investigated the temporal association between smoking and the risk of basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and malignant melanoma (MM). Pooled relative risks (RRs) and confidence intervals (CIs) of the included articles were calculated for current, former, and heavy smoking compared with never smoking. Publication bias was detected using the Egger’s regression.
Results
A total of 15 studies, published between 1990 and 2018, were included. Current smoking was associated with a higher risk of SCC (pooled RR = 1.32, 95% CI 1.15, 1.52) but with a lower risk of BCC (pooled RR = 0.85, 95% CI 0.75, 0.96) and MM (pooled RR = 0.72, 95% CI 0.64, 0.82). No publication bias was detected, and no single study had a substantial impact on the pooled results. Similar results were detected for heavy smoking, while former smoking was not associated with the risk of skin cancer.
Conclusion
Current smoking and heavy smoking were associated with a higher risk of SCC but a decreased risk of BCC and MM, while former smoking was not associated with skin cancer risk.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Skin cancers, including basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and malignant melanoma (MM), are the most frequently diagnosed cancers in Caucasians and their incidence has been increasing over time [1, 2]. Despite showing various behavior, growth, and metastatic attitudes that could be lethal, early identification of skin cancers can improve the prognosis [3].
Several risk factors have been identified to be associated with the development of skin cancers such as skin color, sun exposure, and old age [4]. Although smoking is considered an established risk factor for many cancers [5], previous studies showed conflicting findings regarding its association with the risk of skin cancers. In a previous meta-analysis, Song et al. summarized the results on the association between ever smoking and skin cancer and reported a positive association with SCC (Odds Ratio (OR) = 1.08, 95% confidence interval (CI): 1.01, 1.15) and a weak association with BCC (OR = 1.02, 95% CI 1.00, 1.04). On the other hand, they found a lower risk of MM among male ever smokers in cohort studies (Relative Risk [RR] = 0.73; 95% CI 0.67, 0.80) and among ever smokers, regardless of sex, in case–control studies (OR = 0.70; 95% CI 0.61, 0.80). Yet, their meta-analysis covered a limited number of cohort studies (n = 4) and included case–control studies that encompass limitations such as selection bias and recall bias. They also did not examine the association of smoking intensity with the risk of skin cancer [6]. Since then, several large prospective cohort studies have been published. For example, in the UK Million Women Study, Piere and colleagues described heterogeneous relationships of SCC and BCC with smoking, i.e., increased risk of SCC but decreased risk of BCC [7]. Given the emerging and controversial evidence, we, therefore, aimed to systematically investigate the prospective association between smoking and risk of BCC, SCC, and MM by conducting an updated meta-analysis of cohort studies.
Methods
Literature search
The present meta-analysis was reported according to the checklist of MOOSE [8] and the checklist of PRISMA [9]. We searched MEDLINE (PubMed), Web of Science, and Cochrane Library for potential studies published in English before 28/2/2019 using the following search terms: (smoking) AND (melanoma OR nonmelanoma skin cancer OR squamous cell skin cancer OR basal cell carcinoma). No other restrictions were imposed. A manual search of the reference lists of obtained articles was performed for additional studies. We made no effort to identify unpublished studies.
Eligibility criteria
Studies were included for analysis if they met the following criteria: a cohort design was used, a temporal analysis between smoking and subsequent risk of skin cancer was examined, and risk estimates in the form of RRs with their 95% CIs for current/former versus never smokers were provided.
Study selection
The full manuscripts of all articles extracted by the primary search were reviewed by 2 authors independently. Then, the articles were subjected to our eligibility criteria to create a shortlist of studies to be included in this meta-analysis. Relevant information was extracted from the studies in the shortlist: last name of the first author, publication year, country, sample size, sex of subjects, type of skin cancer, adjusted RRs with corresponding 95% CIs. Quality of studies was determined by the Newcastle–Ottawa Scale (NOS) with scores 5 or 6 for average-quality studies and ≥ 7 for good-quality ones. When more than one article was analyzing the same dataset, the most recent article only was included.
Statistical analysis
The extracted RRs and their CIs were used as measures of association. I2was calculated to evaluate the statistical heterogeneity across studies [10] and the pooled RRs were computed using the fixed- or random-effects model [11]. Also, we conducted subgroup analysis according to study quality and length of the follow-up period. Further, we conducted a sensitivity analysis to identify the influence of each study on the pooled RRs by removing the included studies one by one and analyzing the remainders. Since the study by Karagas et al. [14] investigated secondary BCC and SCC in patients with prior skin cancer, we conducted further sensitivity analysis be removing this study and conducting the analysis on the remaining studies. Publication bias was assessed using Egger’s test [12]. We planned to examine the dose–response relationship between pack years of smoking and the risk of skin cancer; however, there were very limited numbers of studies with necessary data (only 1 study for BCC, 2 for SCC, and 3 for MM), making such an analysis unreliable. Instead, we conducted additional analyses to examine the association between heavy smoking and the risk of skin cancer. We also performed analyses for former smoking. All analyses were conducted using R-3.2.0 statistical package.
Results
Study selection
Primary literature search led to retrieving 1006 studies before we created a shortlist of 15 studies (Fig. 1) [6, 7, 13,14,15,16,17,18,19,20,21,22,23,24,25] in which the association between smoking and risk of BCC was detected in 6 studies, smoking and risk of SCC in 6 studies, and smoking with risk of MM in 8 studies. While smoking was assessed using questionnaires or interviews, histopathological reporting was needed to document subtypes of skin cancer of all included studies. The most adjusted covariates included age, sex, BMI, race/ethnicity, sun exposure (recreational and/or occupational), sunburn, and residence.

Flow chart of the study selection process
Smoking and subsequent risk of BCC
The 6 studies (7 cohorts) included in this analysis analyzed data published between 1990 and 2017 from the USA (3 studies), Australia (2 studies), and the UK (1 study) with a follow-up period ranging between 3 and 26 years (mean: 11.7 ± 8.3 years). Half of the studies were of good quality according to the NOS while the other half was of average quality (Table 1).
Only 2 studies showed a statistically significant inverse association between smoking and the risk of BCC (the HPFS study [6] and the UK Million Women Study [7]), while the associations in the remaining studies were insignificant. Combined, smoking was shown to be associated with a decreased risk of BCC (pooled RR = 0.85, 95% CI 0.75, 0.96, I2 = 92.8%, p for heterogeneity < 0.001) (Fig. 2). After removing the NHS study [6] from the analysis, heterogeneity decreased significantly (I2 = 20.9%, p for heterogeneity = 0.276). We did not recognize extreme studies that had substantial influences on the pooled RR, and no publication bias was detected (z = -0.965, p for publication bias = 0.335). Restricting the analysis to the good-quality studies and studies with follow-up period ≥ 10 years did not change the pooled risk or heterogeneity (pooled RR = 0.85, 95% CI 0.73, 0.99, I2 = 95.9%, p for heterogeneity < 0.001) and (pooled RR = 0.86, 95% CI 0.74, 1.00, I2 = 95.9%, p for heterogeneity < 0.001); respectively. Also, removing Karagas et al. study [14] showed no effect on the pooled risk or heterogeneity (pooled RR = 0.86, 95% CI 0.75, 0.98, I2 = 93.5%, p for heterogeneity < 0.001).

Forest plot of the selected cohort studies for the association between current smoking and the risk of basal cell carcinoma
In comparison to never smokers, heavy smokers were less likely to develop BCC (pooled RR = 0.85, 95% CI 0.73, 1.00, I2 = 90.6%). However, former smoking was not associated with the risk of BCC (pooled RR = 0.98, 95% CI 0.91, 1.06, I2 = 82.9%) (Table 2).
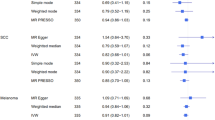
Smoking and subsequent risk of SCC
A total of 6 studies (7 cohorts) were included in this analysis: 2 conducted on subjects from the USA, 2 Australia, 1 the UK, and 1 Sweden. The studies were published during the period between 1992 and 2018 with a follow-up period ranging between 3 and 26 years (mean: 13.9 ± 7.9 years) and half of them were of good quality (Table 1). Pooled together, current smokers had a significantly increased risk of developing SCC compared to never smokers (pooled RR = 1.32, 95% CI 1.15, 1.52, I2 = 58.5%, p for heterogeneity = 0.025) (Fig. 3). Removing the study by Dusingize et al. (2017) [24] significantly reduced the heterogeneity (I2 = 32.6%, p for heterogeneity = 0.191). No individual studies were shown to have significant influences on the pooled RR. No publication bias was detected (z = 1.323, p for publication bias = 0.186). Restricting the analysis to the good-quality studies and studies with follow-up ≥ 10 years did not significantly change the risk (pooled RR = 1.37, 95% CI 1.16, 1.61, I2 = 66.0%, p for heterogeneity = 0.032) and (pooled RR = 1.23, 95% CI 1.16, 1.30, I2 = 0.0%, p for heterogeneity = 0.423); respectively. Removing Karagas et al. study [14] showed no effect on the pooled risk or heterogeneity (pooled RR = 1.28, 95% CI 1.12, 1.47, I2 = 54.8%, p for heterogeneity = 0.050).

Forest plot of the selected cohort studies for the association between current smoking and the risk of squamous cell carcinoma
Compared to never smokers, heavy smokers were more likely to develop SCC (pooled RR = 1.26, 95% CI 1.05, 1.52, I2 = 50.5%). However, former smoking was not associated with the risk of SCC (pooled RR = 1.02, 95% CI 0.95, 1.11, I2 = 37.8%) (Table 2).
Smoking and subsequent risk of MM
This analysis included 8 studies (10 cohorts) from the USA, Norway, Sweden, New Zealand, and Australia. The studies were published between 1997 and 2018 with a follow-up period ranging between 4 and 26 years (mean: 13.7 ± 6.7 years) and 3 studies were of good quality (Table 1).
The pooled risk estimate showed a diminished risk of MM among current smokers in comparison to never smokers (pooled RR = 0.72, 95% CI 0.64, 0.82, I2 = 63.7%, p for heterogeneity = 0.026) (Fig. 4). Removing the NHS study [6] decreased the heterogeneity significantly (I2 = 0.0%, p for heterogeneity = 0.501). No individual studies had significant impact on the overall RR and no publication bias was detected (z = -0.652, p for publication bias = 0.514). Restricting the analysis to the good-quality studies and studies with follow-up ≥ 10 years slightly affected the overall risk (pooled RR = 0.77, 95% CI 0.55, 1.07, I2 = 60.7%, p for heterogeneity = 0.054) and (pooled RR = 0.71, 95% CI 0.63, 0.80, I2 = 37%, p for heterogeneity = 0.123); respectively.

Forest plot of the selected cohort studies for the association between current smoking and the risk of malignant melanoma
Compared to never smokers, heavy smokers were less likely to develop MM (pooled RR = 0.72, 95% CI 0.56, 0.94, I2 = 55.2%). Former smoking was not associated with the risk of MM (pooled RR = 0.92, 95% CI 0.82, 1.02, I2 = 54.4%) (Table2).
Discussion
Results of this meta-analysis of prospective cohort studies indicated that current smoking was associated with an increased risk of SCC, but a decreased risk of BCC and MM. Similar results were detected in heavy smokers, while former smoking was not associated with the risk of skin cancer. We observed various degrees of heterogeneity between studies, but we were able to detect the possible source of heterogeneity by leaving out one study in each turn.
In agreement with our findings, previous case–control studies showed that smoking could moderately increase the risk of SCC [26] but slightly reduce the risk of BCC [27, 28] and MM [29, 30]. Smoking encompasses many carcinogenic compounds, attenuates immune responses, and decreases cutaneous blood flow, which may explain the increased risk of SCC among smokers [26]. Yet, several hypotheses, although inconclusive, have been suggested to explain the inverse association between smoking and the risk of BCC and MM. For example, smoking might decrease BCC risk by interacting with genes conferring susceptibility to BCC [31, 32]. It also hinders the growth of melanoma cells by downregulating gene expression of the Notch pathway that controls the differentiation and development of multiple cell types. Further, among heavy smokers, nicotine accumulates in tissues containing melanin and suppresses the inflammatory responses to UV radiation [33, 34]. Moreover, smoking has been shown to accelerate skin elastosis that protects from MM [35].
On the other hand, Dusingize et al. [24] justified the lower likelihood of BCC among current smokers compared to never smokers with the possibility of detection bias attributed to the tendency of never smokers to undergo regular skin checks. Thompson and colleagues [36] suggested various scenarios assuming a null and positive association between smoking and MM and concluded that the published literature could hide selection bias. Yet, neither detection bias nor selection bias could explain the positive association between smoking and SCC. Conversely, McBride et al. [20] denied the causative association between smoking and the risk of SCC and referred it to the incomplete adjustment for important covariates. Still, most of the included studies adjusted their results for the potential confounders such as age, skin color, sun exposure, and history of sunburns. Furthermore, restricted analysis to studies of good quality did not significantly affect the overall risk. Nevertheless, the risk of residual confounding could not be fully excluded given the observational nature of the study design.
Our study had several strengths such as the restriction of the analysis to cohort studies that imply a temporal association and have fewer limitations compared to case–control designs, the average to good quality of all included studies, diagnosis of skin cancer using histopathological reporting which minimizes reporting bias and misclassification bias, the enlarged sample size, computing the effect of heavy, current, and former smoking on skin cancer, and the adjustment of results in most studies to the most potential confounders. However, it should be noted that the subjective reporting of smoking and the possibility of residual confounding and measurement error are considerable limitations of this meta-analysis.
Conclusion
The present meta-analysis suggested that smoking was associated with an increased risk of SCC, but a decreased risk of BCC and MM. Future experimental studies to unveil the biological mechanisms of these associations and examine the effect of smoking cessation on skin cancer susceptibility are needed. The findings of this study must not be used as a prompt to start or continue smoking, or as arguments for any potential benefits of smoking.
References
Perera E, Gnaneswaran N, Staines C et al (2015) Incidence and prevalence of non-melanoma skin cancer in Australia: a systematic review. Aust J Dermatol 56:258–267
Whiteman DC, Green AC, Olsen CM (2016) The growing burden of invasive melanoma: projections of incidence rates and numbers of new cases in six susceptible populations through 2031. J Invest Dermatol 136:1161–1171
Apalla Z, Nashan D, Weller R et al (2017) Skin cancer: epidemiology, disease burden, pathophysiology, diagnosis, and therapeutic approaches. Dermatol Ther 7:5–19
Etzkorn JR, Parikh RP, Marzban SS et al (2013) Identifying risk factors using a skin cancer screening program. Cancer Control 20:248–254
Jacob L, Freyn M, Kalder M et al (2018) Impact of tobacco smoking on the risk of developing 25 different cancers in the UK: a retrospective study of 422,010 patients followed for up to 30 years. Oncotarget 9:17420–17429
Song F, Qureshi AA, Gao X et al (2012) Smoking and risk of skin cancer: a prospective analysis and a meta-analysis. Int J Epidemiol 41:1694–1705
Pirie K, Beral V, Heath AK et al (2018) Heterogeneous relationships of squamous and basal cell carcinomas of the skin with smoking: the UK Million Women Study and meta-analysis of prospective studies. Br J Cancer 119:114–120
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283:2008–2012
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ Clin Res Ed 339:b2535
Higgins JP, Thompson SG, Deeks JJ et al (2003) Measuring inconsistency in meta-analyses. BMJ Clin Res Ed 327:557–560
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Egger M, Davey Smith G, Schneider M et al (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ Clin Res Ed 315:629–634
Hunter DJ, Colditz GA, Stampfer MJ et al (1990) Risk factors for basal cell carcinoma in a prospective cohort of women. Ann Epidemiol 1:13–23
Karagas MR, Stukel TA, Greenberg ER et al (1992) Risk of subsequent basal cell carcinoma and squamous cell carcinoma of the skin among patients with prior skin cancer. Skin Cancer Prev Study Group JAMA 267:3305–3310
Veierod MB, Thelle DS, Laake P (1997) Diet and risk of cutaneous malignant melanoma: a prospective study of 50,757 Norwegian men and women. Int J Cancer 71:600–604
Freedman DM, Sigurdson A, Doody MM et al (2003) Risk of melanoma in relation to smoking, alcohol intake, and other factors in a large occupational cohort. Cancer Causes Control 4:847–857
Odenbro A, Bellocco R, Boffetta P et al (2005) Tobacco smoking, snuff dipping and the risk of cutaneous squamous cell carcinoma: a nationwide cohort study in Sweden. Br J Cancer 92:1326–1328
Odenbro A, Gillgren P, Bellocco R et al (2007) The risk for cutaneous malignant melanoma, melanoma in situ and intraocular malignant melanoma in relation to tobacco use and body mass index. Br J Dermatol 156:99–105
DeLancey JO, Hannan LM, Gapstur SM et al (2011) Cigarette smoking and the risk of incident and fatal melanoma in a large prospective cohort study. Cancer Causes Control 22:937–942
McBride P, Olsen CM, Green AC (2011) Tobacco smoking and cutaneous squamous cell carcinoma: a 16-year longitudinal population-based study. Cancer Epidemiol Biomark Prev 20:1778–1783
Blakely T, Barendregt JJ, Foster RH et al (2013) The association of active smoking with multiple cancers: national census-cancer registry cohorts with quantitative bias analysis. Cancer Causes Control 24:1243–1255
Hughes MC, Olsen CM, Williams GM et al (2014) A prospective study of cigarette smoking and basal cell carcinoma. Arch Dermatol Res 306:851–856
Henderson MT, Kubo JT, Desai M et al (2015) Smoking behavior and association of melanoma and nonmelanoma skin cancer in the Women's Health Initiative. J Am Acad Dermatol 72:190–191
Dusingize JC, Olsen CM, Pandeya NP et al (2017) Cigarette smoking and the risks of basal cell carcinoma and squamous cell carcinoma. J Invest Dermatol 137:1700–1708
Dusingize JC, Olsen CM, Pandeya N et al (2018) Smoking and cutaneous melanoma: findings from the QSkin Sun and Health Cohort Study. Cancer Epidemiol Biomark Prev 27:874–881
De Hertog SA, Wensveen CA, Bastiaens MT et al (2001) Relation between smoking and skin cancer. J Clin Oncol 19:231–238
D'Errico M, Calcagnile A, Iavarone I et al (1999) Factors that influence the DNA repair capacity of normal and skin cancer-affected individuals. Cancer Epidemiol Biomark Prev 8:553–559
Rees JR, Stukel TA, Perry AE et al (2007) Tea consumption and basal cell and squamous cell skin cancer: results of a case-control study. J Am Acad Dermatol 56:781–785
Kessides MC, Wheless L, Hoffman-Bolton J et al (2011) Cigarette smoking and malignant melanoma: a case-control study. J Am Acad Dermatol 64:84–90
Shors AR, Solomon C, McTiernan A et al (2001) Melanoma risk in relation to height, weight, and exercise (United States). Cancer Causes Control 12:599–606
Nan H, Xu M, Kraft P et al (2011) Genome-wide association study identifies novel alleles associated with risk of cutaneous basal cell carcinoma and squamous cell carcinoma. Hum Mol Genet 20:3718–3724
Stacey SN, Gudbjartsson DF, Sulem P et al (2008) Common variants on 1p36 and 1q42 are associated with cutaneous basal cell carcinoma but not with melanoma or pigmentation traits. Nat Genet 40:1313–1318
Sopori M (2002) Effects of cigarette smoke on the immune system. Nat Rev Immunol 2:372–377
Yerger VB, Malone RE (2006) Melanin and nicotine: a review of the literature. Nicotine Tob Res 8:487–498
Grant WB (2008) Skin aging from ultraviolet irradiance and smoking reduces risk of melanoma: epidemiological evidence. Anticancer Res 28:4003–4008
Thompson CA, Zhang ZF, Arah OA (2013) Competing risk bias to explain the inverse relationship between smoking and malignant melanoma. Eur J Epidemiol 28:557–567
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Arafa, A., Mostafa, A., Navarini, A.A. et al. The association between smoking and risk of skin cancer: a meta-analysis of cohort studies. Cancer Causes Control 31, 787–794 (2020). https://doi.org/10.1007/s10552-020-01319-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-020-01319-8