
Abstract
Purpose
Poor oral health appears to be a risk factor for pancreatic cancer, possibly implicating the oral microbiota. In this pilot study, we evaluated the characteristics of the oral microbiota in patients with pancreatic ductal adenocarcinoma (PDAC), intraductal papillary mucinous neoplasms (IPMN), and healthy controls.
Methods
Forty newly diagnosed PDAC patients, 39 IPMN patients, and 58 controls, excluding current smokers and users of antibiotics, provided saliva samples. Common oral bacterial species were comprehensively surveyed by sequencing of the 16S rRNA microbial genes. We obtained measures of diversity and the mean relative proportions of individual taxa. We explored the degree to which these measures differed according to respondent characteristics based on individual interviews.
Results
PDAC cases did not differ in diversity measures from either controls or IPMN cases. PDAC cases had higher mean relative proportions of Firmicutes and related taxa, while controls had higher mean relative proportions of Proteobacteria and related taxa. Results were generally similar when comparing PDAC to IPMN cases. Among IPMNs and controls combined, younger individuals had higher levels of several taxa within the Proteobacteria. The only other variable consistently related to mean relative proportions was mouthwash use, with taxa within Firmicutes more common among users.
Conclusions
While there were no differences in diversity of the oral microbiota among these groups, there were differences in the mean relative proportions of some taxa. Characteristics of the oral microbiota are not associated with most measures of oral health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is a deadly disease that is expected to affect >53,000 people in the US in 2017; it has the lowest 5-year relative survival of any cancer, 8.5% [1, 2]. One likely reason for this poor outcome is that 92% of cases are diagnosed at a late stage when cure is not possible. Established risk factors for pancreatic cancer include older age, male gender [2], cigarette smoking [3, 4], long-term diabetes [5, 6], and high body mass index (BMI) [7, 8], while respiratory allergies have been consistently linked to lower risk [9,10,11].
A small number of prospective studies [12,13,14,15] have shown significantly increased risk of pancreatic cancer in individuals with poor oral health, measured by tooth loss, the presence of periodontal disease, or antibodies to Porphyromonas gingivalis ATCC 53978. One aspect of oral health that might be related to risk is the composition and characteristics of the oral microbiota.
Intraductal papillary mucinous neoplasms (IPMNs) are precursor lesions that may harbor or lead to pancreatic cancer [16]. While they are detectable on radiographic studies, it is challenging to determine their potential for malignancy without surgical intervention. Understanding the characteristics of individuals with these precursor lesions, including their oral health and oral microbiota characteristics, could potentially help delineate which patients need further intervention.
In this pilot study, we compared the oral microbiota in patients with newly diagnosed, untreated, PDAC, and healthy controls, hypothesizing that the oral microbiota would differ between cases and controls. We also included a group of patients with IPMNs, in order to investigate whether their oral microbiota were similar to those of the cases. Our questionnaire covered questions on oral health, in addition to questions on established risk factors, allowing us to explore whether self-reported oral health differed among the groups and whether established risk factors or oral health factors were related to characteristics of the oral microbiota.
Materials and methods
Study participants
In a hospital-based study, we enrolled 40 cases with PDAC, 39 patients with IPMNs, and 58 visitor controls between October 2013 and March 2015. Eligible participants were of age 21 or over, had not smoked tobacco products in the past year, had not taken antibiotics in the past 30 days, had not been treated for any cancer (other than non-melanoma skin cancer) in the past 2 years, and spoke English. Cases had newly diagnosed and confirmed PDAC and had not begun therapy. Controls were individuals accompanying patients to clinics at Memorial Sloan Kettering Cancer Center (MSKCC), other than clinics where patients with PDAC or IPMN were seen. Since there is no defined population from which patients with PDAC at MSKCC come, this method enabled us to enroll individuals who are likely to be similar in background characteristics to the patients with PDAC. Patients with IPMNs were being followed at MSKCC. Thirty-two had surgery for their IPMN; those who did not have surgery had IPMNs detected by endoscopic ultrasound and elevated cyst-fluid CEA levels (≥200 ng/dl).
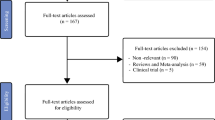
We approached 281 patients with newly diagnosed PDAC. A large majority of those approached were ineligible (80%); this was mainly because they had been previously treated for pancreatic cancer (49% of the total), reflecting the common use of neo-adjuvant chemotherapy during this time period. Other frequent reasons for being ineligible were recent use of antibiotics (9%), smoking (8%), and not speaking English (7%). Seventeen percent of the cases declined to take part, most before screening for eligibility. For controls, 182 individuals who were visitors accompanying patients at MSK clinics were approached; 33% declined (most before screening for eligibility) and 30% were ineligible. Reasons for being ineligible were similar to those in the cases, excluding cancer therapy. We approached 75 patients with IPMNs; 31 were ineligible and 4 declined (one was later excluded). The study was reviewed by the Institutional Review Board at MSKCC and all participants provided written informed consent.
Collection of data and specimens
This study was carried out in the context of our ongoing MSKCC Pancreatic Tumor Registry, which includes an extensive epidemiologic questionnaire focused on risk factors for pancreatic cancer. For this pilot study, we also obtained information on exposures related to oral health: number of teeth missing; ever diagnosed with periodontal disease; number of dental visits in the past 10 years for checkup or cleaning; use of mouthwash at least once a week in the past 5 years. Other variables included use of antibiotics in the past 3 years and alcohol consumption in the past 5 years. Saliva was collected using OMNIgene·DISCOVER (OM-501, DNA Genotek Inc, Ottawa, ON, Canada). Specimens were delivered the same day they were collected to the Molecular Epidemiology Laboratory where they were processed in accordance with the OMNIgene·DISCOVER protocol and stored at −20 °C. Six PDAC cases provided a saliva sample but did not complete the questionnaire, mainly because of severe illness or death. A blood sample or second saliva sample was also collected for future use of germline DNA in accordance with the Pancreatic Tumor Registry protocol.
16S rRNA gene amplification, sequencing, and characterization
Bacterial DNA was extracted from frozen aliquots of approximately 100 mg and microbial cells were lysed by the method of beadbeating, followed by phenol:chloroform:isoamyl alcohol extraction. DNA was precipitated with ethanol and resuspended in 50 µl of TE buffer with 100 µl/ml RNase. The QIAamp DNA Mini Kit (Qiagen, Hilden, Germany) was used for DNA purification, and the Invitrogen Qubit fluorescence assay (Life Technologies, Carlsbad CA) for quantifying DNA. For amplification of samples, duplicate 50-µl PCR reactions were performed with primers designed to amplify the V4-V5 regions using universal primers 563F (5′-nnnnnnnn-NNNNNNNNNNNN-AYTGGGYDTAAAGNG-3′) and 926R (5′- nnnnnnnn-NNNNNNNNNNNN-CCGTCAATTYHTTTRAGT-3′). The primers were preceded by a unique 12-base barcode to identify samples [17]. Quality control measures included use of extraction blanks and PCR blanks to ensure that they do not contain amplicons prior to sequencing. All but one sample (from a patient with IPMN) were successfully amplified. Replicate PCR products were pooled and amplicons were purified using the Qiaquick PCR Purification Kit (Qiagen). Illumina barcodes and adaptors were ligated on using the Ilumina TruSeq Sample Preparation protocol. The completed library was sequenced on the Illumina MiSeq platform following the manufacturer’s recommended procedures with a paired-end 250 × 250 bp kit. Sequence data were compiled and processed using MOTHUR [18]. Paired-end read files were converted to standard FASTQ format before being merged. Poor quality sequences were excluded from the analysis. Sequences were aligned to the 16S rRNA gene, using as template the SILVA reference alignment [19], and the Needleman–Wunsch algorithm [20] with the default scoring options. Potentially chimeric sequences were removed using the UChime algorithm [21]. After filtering, 2000 sequences were randomly selected from the filtered reads for each individual for analysis. To minimize the effect of pyrosequencing errors in overestimating microbial diversity [22], rare abundance sequences that differ in 1 or 2 nucleotides from a high abundant sequence were merged to the high abundant sequence using the pre.cluster option in MOTHUR. Sequences were grouped into operational taxonomic units (OTUs) using the furthest neighbor algorithm. Sequences with distance-based similarity of 97% or greater were assigned to the same OTU. Each sequence was classified using a modified in-house database containing sequences from GreenGenes 99 and retrieved 16S sequences from Genbank through the Bayesian classifier algorithm described by Wang and colleagues with the bootstrap cutoff of 60% [23]. The relative abundance of the microbiota is represented by the percentages of the classified taxa sequences out of the total sequences present in the sample.
Data analysis
We compared the PDAC cases and controls with respect to demographics, established risk factors, and variables related to oral health. Similar comparisons were made between PDAC cases and those with IPMNs. Because of differences in the gender and age distribution of the groups, we used logistic regression to calculate odds ratios and 95% confidence intervals (CI) for these variables adjusted for gender and age (<60, 60–69, ≥70). Several measures were used to evaluate potential differences in the oral microbiota between groups. The non-parametric (NP) Shannon Index and Inverse Simpson statistic were used to evaluate the richness (number of species) of microbial communities and the evenness of their distribution in each individual (alpha diversity, or the diversity within each sample [24]). We also compared the groups with respect to species richness (the number of OTUs). Higher scores indicate more diversity. We calculated means and standard deviations on these measures for each of the three groups. We also used LEfSe (linear discriminant analysis effect size) analysis [25] to evaluate global differences between groups in the overall distribution of taxa, using the non-parametric Kruskal–Wallis statistic. For those taxa for which there were statistically significant overall differences, a second step tested each pairwise comparison to determine which pairs differed, using the Wilcoxon rank sum test. The results were then used to construct a linear discriminant analysis (LDA) model that ranked the individual taxa according to the effect size with which they differentiate between groups. We also compared the mean relative proportions of individual taxa between cases and controls, and between cases with PDAC and those with IPMNs, using t-tests, considering those taxa for which the mean relative proportion among all respondents was ≥ 1% and excluding those that were unclassified; this resulted in a total of 68 taxa (Supplemental Table). As another way of comparing the groups, we used qualitative (unweighted) UniFrac [26] to obtain distance measures that reflect differences in phylogenetic lineages among groups. Each pair of participants was compared with respect to the unique fraction of phylogenetic branches that they shared [27]. Based on these data, principal component analysis was used to determine how individuals clustered, based on their similarity.
Since the IPMNs represent a range of severity, we explored associations in two subgroups: one group (n = 12) consisted of those who had carcinoma in situ or high dysplasia; the other (n = 20) had moderate or low dysplasia found at the time of surgery. This analysis excluded the 7 who did not have surgery for their IPMN. Fisher’s exact test was used to evaluate differences between these groups in demographics and risk factors.
Because few reports are available on factors that might be related to the characteristics of the oral microbiota, we investigated whether participant characteristics, risk factors for PDAC, and oral health measures were related to differences in the diversity or composition of the oral microbiota, focusing on the seventeen taxa that were found to be different between PDAC cases and controls. The variables included respondent characteristics (age, gender); risk factors for PDAC (body mass index (BMI), diabetes, smoking history (past/never), allergies); oral health factors (number of missing teeth, history of gum disease, number of dental visits for checkups in the past 10 years, use of mouthwash at least once a week); and prior use of antibiotics and use of alcohol. Because of our small sample size, and because there were few differences between IPMNs and controls, we combined these two groups for this analysis. Among the variables studied, only age and use of mouthwash were consistently related to the mean relative proportions of specific taxa; therefore we used regression models to obtain p values adjusted for age (<70 and ≥70) and mouthwash use (yes/no) for analysis of individual taxa.
Results
Sequencing of 16S
The mean (range) of sequencing reads for all participants combined was 32,915 (7,593–117,123) before filtering and 32,574 (7,560–115,445) after filtering. The means for the three groups of respondents were PDAC: unfiltered 31,256, filtered 30,964; controls: unfiltered 33,427, filtered 33,060; IPMN: unfiltered 33,911, filtered 33,556. The number of taxa identified at each level was 17 phyla; 37 classes; 68 orders; 111 families; 191 genera; and 400 species.
PDAC cases and controls
Characteristics of study participants
Cases were more likely to be men and age ≥70. Among established risk factors, cases were more likely to be obese, to have smoked in the past, and to have long-standing diabetes, and were less likely to have allergies. Differences reflected established risk factors but were not statistically significant. For measures related to oral health, PDAC patients reported fewer dental visits in the past 10 years compared to controls and, while most respondents reported consuming alcohol in the past 5 years, PDAC patients were more likely to be non-drinkers (Table 1).
Measures of the oral microbiota
As shown in Table 2, PDAC cases and controls were very similar in measures of alpha diversity. Table 3 shows results for 17 taxa (out of the 68 studied, listed in Supplemental Table) found to have at least nominally significant differences (p < 0.05) in mean relative proportion between PDAC cases and controls. Adjusted p values are shown for t tests of differences in means; differences found by linear discriminant analysis (LDA) are also indicated. Compared to controls, PDAC cases were found to have higher levels of Firmicutes and related taxa (Bacilli, Lactobacillales, Streptococcaceae, Streptococcus, Streptococcus thermophilus); however, only the difference at the phylum level remained statistically significant after correction for multiple comparisons (0.05/17 = 0.003). Controls were found to have higher levels of Proteobacteria and related taxa (Gammaproteobacteria, Pasteurellales, Pasteurellaceae, Haemophilus, Haemophilus parainfluenzae; and Betaproteobacteria, Neisseriales, Neisseriaceae, Neisseria, Neisseria flavescens). These differences were statistically significant after correction for multiple comparisons. Adjustment for age and mouthwash use did not influence results (unadjusted data not shown). Similar results were found using LDA. Principal component analysis based on UniFrac measures did not indicate any clear clustering of cases separately from controls and explained very little of the variance (<4% for the first principal component).
PDAC and IPMN cases
Characteristics of study participants
Patients with IPMNs were older than those with PDAC, with 59% aged ≥70. PDAC and IPMN patients were similar with respect to obesity, past smoking, and allergies, while PDAC cases were more likely to report diabetes. For measures related to oral health, PDAC patients had significantly more missing teeth, reported fewer dental visits in the past 10 years, and were somewhat less likely to use mouthwash. Patients with PDAC reported significantly less use of antibiotics than IPMN cases. PDAC patients were more likely to be non-drinkers (Table 1). The IPMN patients with more severe dysplasia (n = 12), compared to those with less dysplasia (n = 20), were more likely to be former smokers (75 vs. 30%, p = 0.03), to have used antibiotics in the past 3 years (67 vs. 5%, p = 0.05), and to have had fewer than 20 dental visits in the past 10 years (58 vs. 25%, p = 0.08).
Measures of the oral microbiota
The PDAC and IPMN groups were very similar in measures of alpha diversity (Table 2). In Table 3, comparing individual taxa between PDAC cases and IPMNs, we observed that for Firmicutes and related taxa, the mean relative proportions among the IPMNs were lower than that among the PDAC cases, and generally similar to that in the controls. These adjusted differences between PDAC and IPMNs were nominally significant (p < 0.05), but few were significant after correction for multiple comparisons. For other taxa, the mean relative proportion among IPMNs was generally between that for the cases and the controls. Adjustment for age and mouthwash use did not influence results (unadjusted data not shown). LDA confirmed some of these differences, and also identified some others. There were no differences between the 12 patients whose IPMNs showed more dysplasia and those with mild or moderate dysplasia (data not shown). Principal component analysis based on UniFrac measures did not indicate the presence of clusters and explained <4% of the variance.
Respondent characteristics related to oral microbiota
For controls and IPMNs combined, alpha diversity, measured by NP Shannon, Inverse Simpson, and richness (number of OTUs), was generally not related to respondent characteristics, established risk factors, or measures of oral health. The only exceptions were that individuals who consumed alcohol had somewhat lower diversity on the NP Shannon index (5.1 vs. 5.4, p = 0.03) and lower richness (590.7 vs. 663.9, p = 0.03). For the 17 individual taxa with significant differences between cases and controls, we found that age had a consistent influence, with Proteobacteria and related taxa having higher mean relative proportions in respondents <70 years of age. Regular use of mouthwash in the past 5 years also influenced the mean relative proportions of the taxa studied: users had higher levels of Firmicutes and related taxa, while non-users had higher levels of Proteobacteria and related taxa (Table 4). Women and former smokers had higher levels of Haemophilus and H. parainfluenzae, and those with fewer teeth missing also had higher levels of H. parainfluenzae. Individuals with diabetes had higher levels of Betaproteobacteria, Neisseriales, Neisseriaceae, and Neisseria. Those who consumed alcohol had lower mean relative proportion of Firmicutes and higher levels of N. flavescens. There were no statistically significant differences in mean relative proportion of the taxa studied according to BMI, allergies, history of gum disease, number of dental visits for checkups in the past 10 years, or prior use of antibiotics (Table 4).
Discussion
In this pilot study, we found no differences between patients with PDAC and healthy controls, or between patients with PDAC and those with IPMNs, on measures of alpha diversity of the oral microbiota. We observed some differences in the mean relative proportions of specific taxa, with PDAC cases having higher levels of Firmicutes and related taxa, and controls having higher levels of Proteobacteria and related taxa. Differences between patients with PDAC and IPMNs generally mirrored those between PDAC cases and controls, although fewer comparisons were statistically significant. This reflects both the generally smaller differences between PDAC cases and IPMN cases as well as the smaller sample size for IPMNs than for controls.
Three smaller studies of PDAC have investigated associations with oral microbiota using a case–control design. Our results were in agreement with those of Jacobs et al. [28] with respect to finding higher levels of Firmicutes, and lower levels of Proteobacteria, in cases than in controls. This, study, as well as ours, reported lower levels of Neisseria in cases and were similar in finding no differences in diversity measures. Farrell et al. [29] reported lower proportions of both N. elongata and S. mitis in cases compared to controls. Our results for N. elongata were in the same direction as those reported by Farrell et al. [29] but our results for S. mitis were not; the mean relative proportions were very low for these species. We did not replicate the findings reported by Lin et al. [30].
A larger study with a prospective design [31] reported higher levels of P. gingivalis and A. actinomycetemcomitans in cases; these were candidate species known to be oral pathogens. Other results showed that taxa within Fusobacteria and Bacteroidetes phyla were associated with decreased or increased risk of PDAC, respectively. We did not find similar results in our study. Other prospective studies have also highlighted a role for P. gingivalis. In one study [13], higher levels of serum IgG to P. gingivalis were associated with death from orodigestive cancer in individuals with normal dental exams, although pancreatic cancer was not reported separately. In another study [14], high levels of antibodies to P. gingivalis ATTC 53978 increased risk of PDAC two-fold while respondents with overall higher levels of antibodies had 45% lower risk. Our study did not find P. gingivalis in any samples, and the associated phylum, class, order, family, and genus were not found to be different in cases and controls. The other case–control studies also did not report on P. gingivalis. It is possible that P. gingivalis was present in our study participants but that the primers used may not have amplified these bacteria. Changes in the oral microbiota related to the presence of disease may also have influenced these results.
The epidemiologic findings linking oral health to increased risk of PDAC are based on a small number of prospective studies using various measures of oral health. In a study of male smokers, those who had lost all their teeth were at 63% increased risk of pancreatic cancer compared to those missing 10 or fewer teeth [12]. In contrast, the number of missing teeth was not related to risk of death from pancreatic cancer in a cohort of elderly Japanese [32]. Among male health professionals, self-reported periodontal disease significantly increased risk of pancreatic cancer, particularly in those who also reported tooth loss [15]. Using data from the National Health and Examination Study, in which periodontitis was ascertained by clinical exam, Ahn and colleagues [13] found at least doubled risk of death from any orodigestive cancer (including pancreatic cancer) and from pancreatic cancer in those with periodontitis; there were only 18 deaths from pancreatic cancer in this young cohort. While these studies present mostly consistent evidence of associations with pancreatic cancer, it is not clear which particular aspects of oral health are important for risk.
In our exploratory analysis of associations between respondent characteristics (risk factors and measures of oral health) and measures of diversity and mean relative proportions of individual taxa, we found few differences overall. There were some differences according to alcohol use, age, and use of mouthwash, indicating that these factors should be considered in planning future studies of the oral microbiota. We are not aware of other publications that have reported on how these factors influence the oral microbiota. In our study, we sought to avoid the influence of smoking (within one year) and antibiotic use (within 30 days) by exclusion criteria. A number of studies have reported that smokers and non-smokers differ in the oral microbiota [33,34,35] and other aspects of oral health [36, 37]. Differences between smokers and non-smokers have also been noted in studies of the microbiota at other sites [38, 39].
The primary limitation of this pilot study is the small sample size. We limited eligibility for PDAC cases to those without prior treatment for pancreatic cancer, to avoid any possible effects of systemic treatment on the oral microbiota; we are not aware of data on the influence of chemotherapy on oral microbiota. Although all cases with PDAC were diagnosed within 3 months of enrollment, they may have been atypical of patients at our institution because they were too ill for consideration for treatment. Studies of the oral microbiota before and after treatment would help determine whether case–control studies are feasible for this investigation, or whether prospective studies are needed. Another potential limitation is that the oral samples were taken at only one time. Overall, based on this pilot study, the oral microbiota does not seem to be strongly related to risk of PDAC or IPMNs; however, differences in mean relative proportions of individual taxa should be evaluated in larger studies. Larger studies are also needed to address more thoroughly the question of confounding of associations between case–control status by respondent characteristics.
References
ACS (2017) Cancer Facts & Figures 2015. American Cancer Society, Altanta
Howlader N, Noone A, Krapcho M, Garshell J, Neyman N, Altekruse S, Kosary C, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis D, Chen H, Feuer E, Cronin K, (eds) (2014) SEER Cancer Statistics Review, 1975–2012. National Cancer Institute Bethesda, MD, http://seercancergov/csr/1975_2012/, based on November 2014 SEER data submission, posted to the SEER web site, April 2015
Bosetti C, Lucenteforte E, Silverman DT, Petersen G, Bracci PM, Ji BT, Negri E, Li D, Risch HA, Olson SH, Gallinger S, Miller AB, Bueno-de-Mesquita HB, Talamini R, Polesel J, Ghadirian P, Baghurst PA, Zatonski W, Fontham E, Bamlet WR, Holly EA, Bertuccio P, Gao YT, Hassan M, Yu H, Kurtz RC, Cotterchio M, Su J, Maisonneuve P, Duell EJ, Boffetta P, La Vecchia C (2011) Cigarette smoking and pancreatic cancer: an analysis from the International Pancreatic Cancer Case–Control Consortium (Panc4). Ann Oncol. doi:10.1093/annonc/mdr541
Maisonneuve P, Lowenfels AB (2015) Risk factors for pancreatic cancer: a summary review of meta-analytical studies. Int J Epidemiol 44(1):186–198. doi:10.1093/ije/dyu240
Elena JW, Steplowski E, Yu K, Hartge P, Tobias GS, Brotzman MJ, Chanock SJ, Stolzenberg-Solomon RZ, Arslan AA, Bueno-de-Mesquita HB, Helzlsouer K, Jacobs EJ, LaCroix A, Petersen G, Zheng W, Albanes D, Allen NE, Amundadottir L, Bao Y, Boeing H, Boutron-Ruault MC, Buring JE, Gaziano JM, Giovannucci EL, Duell EJ, Hallmans G, Howard BV, Hunter DJ, Hutchinson A, Jacobs KB, Kooperberg C, Kraft P, Mendelsohn JB, Michaud DS, Palli D, Phillips LS, Overvad K, Patel AV, Sansbury L, Shu XO, Simon MS, Slimani N, Trichopoulos D, Visvanathan K, Virtamo J, Wolpin BM, Zeleniuch-Jacquotte A, Fuchs CS, Hoover RN, Gross M (2013) Diabetes and risk of pancreatic cancer: a pooled analysis from the pancreatic cancer cohort consortium. Cancer Causes Control 24(1):13–25. doi:10.1007/s10552-012-0078-8
Bosetti C, Rosato V, Li D, Silverman D, Petersen GM, Bracci PM, Neale RE, Muscat J, Anderson K, Gallinger S, Olson SH, Miller AB, Bas Bueno-de-Mesquita H, Scelo G, Janout V, Holcatova I, Lagiou P, Serraino D, Lucenteforte E, Fabianova E, Ghadirian P, Baghurst PA, Zatonski W, Foretova L, Fontham E, Bamlet WR, Holly EA, Negri E, Hassan M, Prizment A, Cotterchio M, Cleary S, Kurtz RC, Maisonneuve P, Trichopoulos D, Polesel J, Duell EJ, Boffetta P, La Vecchia C (2014) Diabetes, antidiabetic medications, and pancreatic cancer risk: an analysis from the International Pancreatic Cancer Case–Control Consortium. Ann Oncol 25(10):2065–2072. doi:10.1093/annonc/mdu276
Stolzenberg-Solomon RZ, Schairer C, Moore S, Hollenbeck A, Silverman DT (2013) Lifetime adiposity and risk of pancreatic cancer in the NIH-AARP Diet and Health Study cohort. Am J Clin Nutr 98(4):1057–1065. doi:10.3945/ajcn.113.058123
Arslan AA, Helzlsouer KJ, Kooperberg C, Shu XO, Steplowski E, Bueno-de-Mesquita HB, Fuchs CS, Gross MD, Jacobs EJ, Lacroix AZ, Petersen GM, Stolzenberg-Solomon RZ, Zheng W, Albanes D, Amundadottir L, Bamlet WR, Barricarte A, Bingham SA, Boeing H, Boutron-Ruault MC, Buring JE, Chanock SJ, Clipp S, Gaziano JM, Giovannucci EL, Hankinson SE, Hartge P, Hoover RN, Hunter DJ, Hutchinson A, Jacobs KB, Kraft P, Lynch SM, Manjer J, Manson JE, McTiernan A, McWilliams RR, Mendelsohn JB, Michaud DS, Palli D, Rohan TE, Slimani N, Thomas G, Tjonneland A, Tobias GS, Trichopoulos D, Virtamo J, Wolpin BM, Yu K, Zeleniuch-Jacquotte A, Patel AV (2010) Anthropometric measures, body mass index, and pancreatic cancer: a pooled analysis from the Pancreatic Cancer Cohort Consortium (PanScan). Arch Intern Med 170(9):791–802. doi:10.1001/archinternmed.2010.63
Olson SH, Hsu M, Satagopan JM, Maisonneuve P, Silverman DT, Lucenteforte E, Anderson KE, Borgida A, Bracci PM, Bueno-de-Mesquita HB, Cotterchio M, Dai Q, Duell EJ, Fontham EH, Gallinger S, Holly EA, Ji BT, Kurtz RC, La Vecchia C, Lowenfels AB, Luckett B, Ludwig E, Petersen GM, Polesel J, Seminara D, Strayer L, Talamini R (2013) Allergies and risk of pancreatic cancer: a pooled analysis from the pancreatic cancer case–control consortium. Am J Epidemiol 178(5):691–700. doi:10.1093/aje/kwt052
Cotterchio M, Lowcock E, Hudson TJ, Greenwood C, Gallinger S (2014) Association between allergies and risk of pancreatic cancer. Cancer Epidemiol Biomark Prev. doi:10.1158/1055-9965.EPI-13-0965
Gomez-Rubio P, Zock JP, Rava M, Marquez M, Sharp L, Hidalgo M, Carrato A, Ilzarbe L, Michalski C, Molero X, Farre A, Perea J, Greenhalf W, O’Rorke M, Tardon A, Gress T, Barbera V, Crnogorac-Jurcevic T, Dominguez-Munoz E, Munoz-Bellvis L, Alvarez-Urturi C, Balcells J, Barneo L, Costello E, Guillen-Ponce C, Kleeff J, Kong B, Lawlor R, Lohr M, Mora J, Murray L, O’Driscoll D, Pelaez P, Poves I, Scarpa A, Real FX, Malats N (2015) Reduced risk of pancreatic cancer associated with asthma and nasal allergies. Gut. doi:10.1136/gutjnl-2015-310442
Stolzenberg-Solomon RZ, Dodd KW, Blaser MJ, Virtamo J, Taylor PR, Albanes D (2003) Tooth loss, pancreatic cancer, and Helicobacter pylori. Am J Clin Nutr 78(1):176–181
Ahn J, Segers S, Hayes RB (2012) Periodontal disease, Porphyromonas gingivalis serum antibody levels and orodigestive cancer mortality. Carcinogenesis 33(5):1055–1058. doi:10.1093/carcin/bgs112
Michaud DS, Izard J, Wilhelm-Benartzi CS, You DH, Grote VA, Tjonneland A, Dahm CC, Overvad K, Jenab M, Fedirko V, Boutron-Ruault MC, Clavel-Chapelon F, Racine A, Kaaks R, Boeing H, Foerster J, Trichopoulou A, Lagiou P, Trichopoulos D, Sacerdote C, Sieri S, Palli D, Tumino R, Panico S, Siersema PD, Peeters PH, Lund E, Barricarte A, Huerta JM, Molina-Montes E, Dorronsoro M, Quiros JR, Duell EJ, Ye W, Sund M, Lindkvist B, Johansen D, Khaw KT, Wareham N, Travis RC, Vineis P, Bueno-de-Mesquita HB, Riboli E (2013) Plasma antibodies to oral bacteria and risk of pancreatic cancer in a large European prospective cohort study. Gut 62(12):1764–1770. doi:10.1136/gutjnl-2012-303006
Michaud DS, Joshipura K, Giovannucci E, Fuchs CS (2007) A prospective study of periodontal disease and pancreatic cancer in US male health professionals. J Natl Cancer Inst 99(2):171–175. doi:10.1093/jnci/djk021
Chandwani R, Allen PJ (2016) Cystic neoplasms of the pancreas. Annu Rev Med 67:45–57. doi:10.1146/annurev-med-051914-022011
Caporaso JG, Lauber CL, Walters WA, Berg-Lyons D, Huntley J, Fierer N, Owens SM, Betley J, Fraser L, Bauer M, Gormley N, Gilbert JA, Smith G, Knight R (2012) Ultra-high-throughput microbial community analysis on the Illumina HiSeq and MiSeq platforms. ISME J 6(8):1621–1624. doi:10.1038/ismej.2012.8
Schloss PD, Westcott SL, Ryabin T, Hall JR, Hartmann M, Hollister EB, Lesniewski RA, Oakley BB, Parks DH, Robinson CJ, Sahl JW, Stres B, Thallinger GG, Van Horn DJ, Weber CF (2009) Introducing mothur: open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl Environ Microbiol 75(23):7537–7541. doi:10.1128/aem.01541-09
Pruesse E, Quast C, Knittel K, Fuchs BM, Ludwig W, Peplies J, Glockner FO (2007) SILVA: a comprehensive online resource for quality checked and aligned ribosomal RNA sequence data compatible with ARB. Nucl acids Res 35(21):7188–7196. doi:10.1093/nar/gkm864
Needleman SB, Wunsch CD (1970) A general method applicable to the search for similarities in the amino acid sequence of two proteins. J Mol Biol 48(3):443–453
Edgar RC, Haas BJ, Clemente JC, Quince C, Knight R (2011) UCHIME improves sensitivity and speed of chimera detection. Bioinformatics (Oxford, England) 27(16):2194–2200. doi:10.1093/bioinformatics/btr381
Huse SM, Welch DM, Morrison HG, Sogin ML (2010) Ironing out the wrinkles in the rare biosphere through improved OTU clustering. Environ Microbiol 12(7):1889–1898. doi:10.1111/j.1462-2920.2010.02193.x
Wang Q, Garrity GM, Tiedje JM, Cole JR (2007) Naive Bayesian classifier for rapid assignment of rRNA sequences into the new bacterial taxonomy. Appl Environ Microbiol 73(16):5261–5267. doi:10.1128/aem.00062-07
Human Microbiome Project Consortium (2012) Structure, function and diversity of the healthy human microbiome. Nature 486(7402):207–214. doi:10.1038/nature11234
Segata N, Izard J, Waldron L, Gevers D, Miropolsky L, Garrett WS, Huttenhower C (2011) Metagenomic biomarker discovery and explanation. Genome Biol 12(6):R60. doi:10.1186/gb-2011-12-6-r60
Lozupone C, Knight R (2005) UniFrac: a new phylogenetic method for comparing microbial communities. Appl Environ Microbiol 71(12):8228–8235. doi:10.1128/aem.71.12.8228-8235.2005
Martin AP (2002) Phylogenetic approaches for describing and comparing the diversity of microbial communities. Appl Environ Microbiol 68(8):3673–3682
Jacobs EJ, Gapstur SM, Purdue MP, Abnet CC, Stolzenberg-Solomon R, Miller G, Ravel J, Hayes RB, Ahn J, Torres PJ, Fletcher EM, Gibbons SM, Bouvet M, Doran KS, Kelley ST (2015) Characterization of the salivary microbiome in patients with pancreatic cancer. Gut 3:e1373. doi:10.1136/gutjnl-2016-31258010.7717/peerj.1373
Farrell JJ, Zhang L, Zhou H, Chia D, Elashoff D, Akin D, Paster BJ, Joshipura K, Wong DT (2012) Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer. Gut 61(4):582–588. doi:10.1136/gutjnl-2011-300784
Lin IH, Wu J, Cohen SM, Chen C, Bryk D, Marr M, Melis M, Newman E, Pachter HL, Alekseyenko AV, Hayes RB, Ahn J (2013) Pilot study of oral microbiome and risk of pancreatic cancer. Cancer Res. doi:10.1158/1538-7445.AM2013-101
Fan X, Alekseyenko AV, Wu J, Peters BA, Jacobs EJ, Gapstur SM, Purdue MP, Abnet CC, Stolzenberg-Solomon R, Miller G, Ravel J, Hayes RB, Ahn J (2016) Human oral microbiome and prospective risk for pancreatic cancer: a population-based nested case–control study. Gut. doi:10.1136/gutjnl-2016-312580
Ansai T, Takata Y, Yoshida A, Soh I, Awano S, Hamasaki T, Sogame A, Shimada N (2013) Association between tooth loss and orodigestive cancer mortality in an 80-year-old community-dwelling Japanese population: a 12-year prospective study. BMC Public Health 13:814. doi:10.1186/1471-2458-13-814
Ge X, Rodriguez R, Trinh M, Gunsolley J, Xu P (2013) Oral microbiome of deep and shallow dental pockets in chronic periodontitis. PLoS ONE 8(6):e65520. doi:10.1371/journal.pone.0065520
Thomas AM, Gleber-Netto FO, Fernandes GR, Amorim M, Barbosa LF, Francisco AL, de Andrade AG, Setubal JC, Kowalski LP, Nunes DN, Dias-Neto E (2014) Alcohol and tobacco consumption affects bacterial richness in oral cavity mucosa biofilms. BMC Microbiol 14:250. doi:10.1186/s12866-014-0250-2
Morris A, Beck JM, Schloss PD, Campbell TB, Crothers K, Curtis JL, Flores SC, Fontenot AP, Ghedin E, Huang L, Jablonski K, Kleerup E, Lynch SV, Sodergren E, Twigg H, Young VB, Bassis CM, Venkataraman A, Schmidt TM, Weinstock GM (2013) Comparison of the respiratory microbiome in healthy nonsmokers and smokers. Am J Respir Crit Care Med 187(10):1067–1075. doi:10.1164/rccm.201210-1913OC
Michaud DS, Izard J, Rubin Z, Johansson I, Weiderpass E, Tjonneland A, Olsen A, Overvad K, Boutron-Ruault MC, Clavel-Chapelon F, Dossus L, Kaaks R, Katzke VA, Boeing H, Foerster J, Trichopoulou A, Naska A, Ziara G, Vineis P, Grioni S, Palli D, Tumino R, Mattiello A, Peeters PH, Siersema PD, Barricarte A, Huerta JM, Molina-Montes E, Dorronsoro M, Quiros JR, Duell EJ, Ohlsson B, Jeppsson B, Johansson A, Lif P, Khaw KT, Wareham N, Travis RC, Key TJ, Freisling H, Duarte-Salles T, Stepien M, Riboli E, Bueno-de-Mesquita HB (2013) Lifestyle, dietary factors, and antibody levels to oral bacteria in cancer-free participants of a European cohort study. Cancer Causes Control 24(11):1901–1909. doi:10.1007/s10552-013-0265-2
Freudenheim JL, Genco RJ, LaMonte MJ, Millen AE, Hovey KM, Mai X, Nwizu N, Andrews CA, Wactawski-Wende J (2016) Periodontal disease and breast cancer: prospective cohort study of postmenopausal women. Cancer Epidemiol Biomark Prev 25(1):43–50. doi:10.1158/1055-9965.epi-15-0750
Charlson ES, Chen J, Custers-Allen R, Bittinger K, Li H, Sinha R, Hwang J, Bushman FD, Collman RG (2010) Disordered microbial communities in the upper respiratory tract of cigarette smokers. PLoS ONE 5(12):e15216. doi:10.1371/journal.pone.0015216
Vogtmann E, Flores R, Yu G, Freedman ND, Shi J, Gail MH, Dye BA, Wang GQ, Klepac-Ceraj V, Paster BJ, Wei WQ, Guo HQ, Dawsey SM, Qiao YL, Abnet CC (2015) Association between tobacco use and the upper gastrointestinal microbiome among Chinese men. Cancer Causes Control 26(4):581–588. doi:10.1007/s10552-015-0535-2
Acknowledgments
This study was supported by a Grant from the Lucille Castori Center for Microbes, Inflammation and Cancer (R. Kurtz) and P30CA008748 (C. Thompson).
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Olson, S.H., Satagopan, J., Xu, Y. et al. The oral microbiota in patients with pancreatic cancer, patients with IPMNs, and controls: a pilot study. Cancer Causes Control 28, 959–969 (2017). https://doi.org/10.1007/s10552-017-0933-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-017-0933-8