
Abstract
Purpose
Air pollution is an established lung carcinogen, and there is increasing evidence that air pollution also negatively affects the brain. We have previously reported an association between air pollution and risk of brain tumors in a cohort study based on only 95 cases. We set out to replicate that finding in a large nationwide case–control study.
Methods
We identified all 4,183 adult brain tumor cases in Denmark in the years 2000–2009 and 8,018 risk set sampled population controls matched on gender and year of birth. We extracted residential address histories and estimated mean residential nitrogen oxides (NO x ) concentrations since 1971 with a validated dispersion model. Categorical and linear odds ratios (OR) and confidence intervals (CI) were calculated with conditional logistic regression models.
Results
The highest risk estimates for any brain cancer were observed among subjects with the highest average exposure levels (80–99 µg/m3: OR 1.27, 95 % CI 0.82–1.96; ≥100 µg/m3: 1.40, 95 % CI 0.87–2.26 as compared to <20 µg/m3 NO x ), but there was no increased OR at NO x levels below 80 µg/m3 and when modeled linearly there was no significant association with risk of brain cancer (OR 1.11, 95 % CI 0.84–1.46 per 100 µg/m3 NO x ). In sub-analysis the OR associated with exposures ≥100 µg/m3 was 2.30 (95 % CI 1.15–4.59) for non-glioma and 0.89 (95 % CI 0.44–1.77) for glioma.
Conclusions
This study did not support the relatively strong linear association between air pollution and risk of brain tumors which was found in our previous study. The suggestion of an increased brain tumor risk at high exposures merits further attention as does the differing results according to tumor morphology.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
The etiology of brain tumors is largely unknown and even though a long range of hypothesized risk factors have been investigated, the only established risk factors are ionizing radiation and rare hereditary conditions [1].
Ambient air pollution is a ubiquitous and complex mixture of substances. It has since many years been known that air pollution poses a health hazard, but only recently air pollution [2] and diesel exhaust [3], a major component of traffic-related air pollution, have been classified as carcinogenic by IARC. The major body of epidemiological evidence for these classifications relate to lung cancer. For other tumor locations, few studies are available. There is growing evidence that exposure to air pollution affects the brain e.g., by causing neuroinflammation and inducing oxidative stress and studies have reported associations with a range of health effects including impaired cognition [4–7] and stroke [6, 8, 9]. Particulate matter (PM) appears to be the component of air pollution most closely related to negative central nervous system (CNS) effects [10]. The relevant route(s) by which the pollution affects the brain are unresolved but there is evidence that ultrafine particles (PM < 100 nm in diameter), may exert indirect effects on the brain via induced systemic inflammation, or enter the brain directly by crossing the blood–brain barrier or by migration along the olfactory neurons [10, 11].
Although the few existing epidemiological studies on air pollution and brain tumor risk have produced some positive results they remain inconclusive [12–14]. The studies have limitations, such as area level exposure proxies assessed at a single point in time and mortality data or county level incidence rates rather than individual level incidence data.
We previously reported an association between air pollution and risk of brain cancer (incidence rate ratios 2.28; 95 % CI 1.25–4.19 per 100 µg/m3 NO x ) in the Diet Cancer and Health (DCH) cohort of 54,304 Danes recruited during 1993–1997 and followed-up for cancer through 2006 [15]. The study had high quality modeled residential NO x concentrations since 1971 for all participants, but was limited by small number of cases. In the present study, we investigate the association of air pollution and risk for brain tumors in all adult brain tumor cases in Denmark over the period 2000–2009.
Materials and methods
We conducted a register based case–control study among the entire population of Denmark (5.4 million inhabitants). All Danish citizens have since 1968 been assigned a personal identification number (PIN) by the central population register (CPR) allowing every resident to be tracked in and across all Danish health and administrative registers [16, 17].
Case ascertainment
Cases were identified from the Danish Cancer Registry which has virtually complete records of all cancer cases in Denmark since 1943 [18, 19]. Cases were all Danes (aged 18–85 years) registered with a benign or malignant tumor of the brain proper (i.e., not including spinal cord, meninges or cranial nerves) (ICD10: C71, D330–D332, D430–D432), in the years 2000–2009. We included only first, primary tumors, thus excluding any with preceding tumors (except non-melanoma skin cancers) as well as all metastases. To increase the likelihood of included cases having sufficient address history for exposure assessment, it was required that cases had been born in Denmark and had a known address in Denmark (excluding Greenland and the Faroe islands) at time of diagnosis.
Control sampling
For each case two random controls, matched on gender and year of birth, were selected from the CPR. Controls which were dead, emigrated or diagnosed with cancer before the diagnosis date of their matched case were excluded and, substitute controls, matched on gender and year of birth, were sampled from surplus controls from the present study as well as from random population controls sampled for other ongoing studies. All controls in the final sample were required to be born in Denmark and to be alive, cancer free (except non-melanoma skin cancer), and living at a known address in Denmark (except Greenland and Faroe islands) at time of diagnosis of their matched case.
Exposure assessment
We used the PIN to trace complete address histories for the study participants from 1971 until end of 2009 or death. All addresses in Denmark were geocoded and subsequently outdoor NO x concentrations were estimated from the Danish AirGIS modeling system which provides estimates of traffic-related air pollution at 2 m height at the front door of all addresses in Denmark since 1971. Time-weighted mean NO x levels were calculated over all known addresses with exposure data since birth or 1971, until date of diagnosis of matched case. We also did a sensitivity analysis disregarding exposure in the last 10 years prior to diagnosis. In a further analysis, we used only exposure during the last 10 years prior to diagnosis. In all analyses subjects with exposure data for less than 80 % of the relevant exposure window were excluded. The exposure model is described in more detail elsewhere [20] (see also http://envs.au.dk/videnudveksling/luft/model/airgis/). In short the model is based on detailed time varying data on three contributors: (1) local air pollution from street traffic, calculated from input data on traffic (intensity and type), emission factors for the car fleet, street and building geometry, and meteorology; (2) urban background, calculated from data on urban vehicle emission density, city dimensions, and building heights; and (3) regional background, estimated from trends at rural monitoring stations and from national vehicle emissions. The model has demonstrated good correlation between modeled and measured NO2 concentrations [21–23]. The model cannot provide reliable estimates for historical particular matter concentrations, as the required background concentrations and historical emission data are not available. NO x has, however, been shown to correlate well with total particle number concentration in Danish streets with r = 0.9 for particle size 10–700 nm and r = 0.7 for particle size <10 µm [24, 25]. We have therefore, as in previous publications [15, 26], used NO x as proxy for traffic-related air pollution including particulate matter.
Statistical methods
Using conditional logistical regression, we calculated odds ratios (ORs) and 95 % confidence intervals for brain cancer among Danish adults according to time-weighted mean NO x exposure levels (<20, 20 to <40, 40 to <60, 60 to <80, 80 to <100 and 100+ µg/m3) with the lowest exposure category as reference. As including a second degree polynomial of NO x in a linear model, offered no significantly (likelihood ratio testing) improved fit over a linear model we found no deviation from a linear association with mean NO x exposure overall (p = 0.09); hence, we also analyzed NO x linearly.
Apart from the implicit adjustment for the matching variables: gender and year of birth, we also adjusted for years living in highly urbanized municipalities (the Greater Copenhagen area, Aarhus and Odense) as a linear variable with an indicator for never living in these municipalities. We performed separate analysis of malignant (ICD10: C71) and non-malignant (ICD10: D33.0–D33.2, D43.0–D43.2) tumors and of glioma (ICD-O-3 topography codes C71.0–71.9 and morphology codes 9380/3–9481/3) and non-glioma tumors (All other morphologies. In our data, 81 % of these cases had no morphology information Table 1). Post hoc, we stratified analysis by having ever lived more than 1 year in the highly urbanized municipalities and we also did analysis restricting the study to cases 50–77 of age at diagnosis. To gain power in the stratified analysis, we broke the matching and used unconditional logistic regression with adjustment for the matching variables: gender and date of birth. Data were analyzed using SAS 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
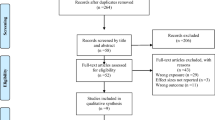
We identified 5,702 persons diagnosed with a tumor of the brain in the years 2000–2009. We excluded 829 coded as possible metastasis and 13 with preceding records in the DCR, 237 diagnosed at age 85 or older, 267 not recorded as born in Denmark, 15 with insufficient address data at diagnosis, 137 cases with less than 80 % known address history and finally 21 cases without a control. The final study population consisted of 4,183 cases (348 with only one control) and 8,018 controls.
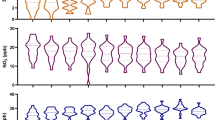
The final study population comprised 57 % men (Table 2) and was diagnosed equally across the period 2000–2009 with the majority (73 %) diagnosed at 50 years of age or older. We had access to exposure data since 1971, providing lifelong coverage for 9 % of cases and 8 % of controls. For those born before 1971 we had 34–38 years of exposure history for 46 % of cases and at least 29 years of exposure history for the remaining subjects. The average NO x concentrations over all available years were very similar for cases and controls with a median NO x concentration of 17 µg/m3 in both groups, the highest average exposure observed was slightly higher in the case group (261 µg/m3) than among the controls (250 µg/m3). In total, 44 % of cases and controls had lived one or more years in the highly urbanized municipalities. Years of living in a highly urbanized municipality was correlated with average lifetime NO x concentrations with a Pearson correlation coefficient of 0.38 (p < 0.0001) (data not shown).
When modeled linearly there was no significant association between NO x and risk of brain cancer (Table 3). There was, however, suggestion of an increased risk in subjects with the highest exposure levels 80–99 µg/m3 (1.27, 95 % CI 0.82–1.96) and ≥100 µg/m3 (1.40, 95 % CI 0.87–2.26). Disregarding exposure in the last 10 years prior to diagnosis or reversely only including exposure during the last 10 years provided more unstable results than the overall analysis (Table 3), but no clear difference in the results.
When looking at tumor types (Table 4), the number of high exposed cases were small and risk estimates were more unstable but the general picture was similar to the overall analysis, with no linear association but the highest risk estimates in the higher exposure categories. For glioma the highest risk estimate (1.34, 95 % CI 0.75–2.38) was seen among subjects with an exposure level of 80–99 µg/m3, whereas no increase was observed in the higher exposure category. The opposite was seen for non-glioma tumors where the ORs were a little above the null for exposure levels from 40 µg/m3 reaching 2.30 (95 % CI 1.15–4.59) in those exposed to more than 100 µg/m3. For non-glioma tumors, there was a significant linear association with an odds ratio of 1.53 (95 % CI 1.02–2.29) in association with a 100 µg/m3 increase in NO x . The association seemed mainly to be restricted to the highest exposure category (100+ µg/m3 NO x ).
For malignant tumors the observed ORs in the two higher exposure categories were 1.68 (95 % CI 1.05–2.70) and 1.22 (95 % CI 0.71–2.10). For the non-malignant tumors no clear picture emerged, although the highest estimate (2.40, 95 % CI 0.85–6.79) was seen for people with the highest exposure (>100 µg/m3); numbers were, however, small and confidence intervals wide.
As the results conflicted with our previously reported association between NO x and risk of brain tumors in the DCH-cohort [15], we conducted a number of post hoc analyses to closer emulate that study: Restricting our analysis to cases aged 50–77 years at diagnosis did not yield materially different results (data not shown). When stratifying analyses by ever having lived more than 1 year in one of the major urban municipalities of Denmark, we found a risk estimate of 1.27 (95 % CI 0.97–1.66) per 100 µg/m3 NO x when as in the previous study, not adjusting for years of urban living (Table 5). Adjustment brought the OR to 1.24 (95 % CI 0.94–1.64). Also, the categorical estimates among the highly exposed participants tended to be higher than in the overall analysis (Table 5). For persons living less than a year in a major urban municipality, there was no evidence of increased risks; only few persons in this group experienced high exposure precluding meaningful interpretation. The p value for the interaction between exposure level and urban living was 0.15.
Discussion
In a nationwide study of over 4,000 brain tumor cases and matched controls, all with lifelong or at least 29 years of information on residential NO x exposure, we found no overall association with risk of brain tumors. There was, however, a tendency for elevated risk among subjects with average lifetime NO x exposures above 80 µg/m3. Such exposure levels were almost exclusively observed in subjects who lived for more than a year in a major urban area and restricting analysis to urban inhabitants accentuated risk estimates.
A Taiwanese case–control study of children and younger adults (age <30) used proportion of municipality residents occupied in non-petrochemical industry as a proxy for industrial air pollution and found a positive association with mortality from brain cancer [14]. An ecological study in Indiana, USA, reported a positive association at county level between industrial release of volatile organic compounds and incidence of brain tumors [12]. In contrast, in a large convenience sampled cohort of adults aged 30+ in the USA and Puerto Rico with exposure based on routine measurement data for the county of residence at enrollment, there was no association between either NO2 or PM2.5 levels and brain cancer mortality in adults [13]. Differences in age ranges and exposure metric and the lack of individual incidence data and individual exposure data taking into account peoples migration histories hampers comparison with our results. Our previous study [15], based on the predominantly urban DCH-cohort spurred the present study: using the same exposure assessment method, the risk for cancer of the CNS was found to increase 2.28-fold (95 % CI, 1.25–4.19) per 100 µg/m3 increase in NO x . This result is in contrast to that of the present study, which is rather compatible with a lack of association between air pollution and risk of brain tumors. The result of the DCH-cohort study may, thus, be a chance finding given the exploratory nature and small number of brain cancer cases included (n = 95). We did, however, observe the highest risk estimates in association with the highest exposure levels and in the post hoc analysis most similar to the previous study we found an OR of 1.27 (95 % CI 0.97–1.66) per 100 µg/m3 NO x among the sub-population living one or more years in a major urban municipality. The OR of 1.27 is just within the confidence interval of the DCH-study. Thus, an association between air pollution and risk for brain cancer might only be detectable in urban areas with higher levels and a wider range of exposures to air pollution. Our results could, however, also well be down to chance as they never reached significance and were based on relatively small numbers. Also, neither our present nor our previous study [15] detected significant deviation from a linear relationship between NO x and brain tumors. Such deviation would, however, be difficult to detect statistically given the low proportion of highly exposed subjects.
We found no clear evidence of different associations between exposure and outcome depending on the exposure time-window applied; the results based on the restricted exposure time-windows seemed more unstable. With 10 year latency, the highest estimate was seen at the second highest exposure level, whereas when looking only at the 10 years preceding diagnosis the highest estimate was in the highest exposure category with no increase in the 80–99 µg/m3 group.
There was some evidence of an association of NO x and risk of non-glioma tumors. These results were, however, small and confidence intervals were wide; it may be a chance finding. To our knowledge, there are no previous studies on air pollution in relation to non-glioma tumors of the brain. We were unable to further investigate this finding due to insufficient morphology (84 %) or topology (73 %) information.
A major strength of our study is the virtually complete Danish health and population registers which allowed identification of all primary brain tumors and matched population controls. Furthermore, we established complete address and exposure histories since 1971 for the vast majority of subjects, using a successfully validated, state-of-the-art, air pollution modeling system.
Our study is limited by the lack of data on exposure during work or commuting and the reliance on modeled residential NO x levels even though ultrafine particles are probably more relevant for neurological effects [10]. Our model has, however, demonstrated good correlation with measured concentrations of ultrafine particles [24, 25] and has demonstrated its relevance in many previous studies [15, 20, 26–28].
By design we were restricted to information about potential confounders routinely registered in Denmark. There are, however, very few established risk factors for brain tumors.
Another limitation was the small number of highly exposed cases which impeded analysis of specific tumor types and locations.
Overall, this population wide study did not corroborate our previous finding of a strong linear association between air pollution and risk of brain tumors. The suggestion of an increased brain tumor risk among persons with high exposure merits further attention preferably in a design with more high exposed cases with detailed information on tumor type and location.
References
Bondy ML, Scheurer ME, Malmer B et al (2008) Brain tumor epidemiology: consensus from the Brain Tumor Epidemiology Consortium. Cancer 113:1953–1968
Loomis D, Grosse Y, Lauby-Secretan B et al (2013) The carcinogenicity of outdoor air pollution. Lancet Oncol 14:1262–1263
Benbrahim-Tallaa L, Baan RA, Grosse Y et al (2012) Carcinogenicity of diesel-engine and gasoline-engine exhausts and some nitroarenes. Lancet Oncol 13:663–664
Ranft U, Schikowski T, Sugiri D, Krutmann J, Kramer U (2009) Long-term exposure to traffic-related particulate matter impairs cognitive function in the elderly. Environ Res 109:1004–1011
Gatto NM, Henderson VW, Hodis HN et al (2014) Components of air pollution and cognitive function in middle-aged and older adults in Los Angeles. Neurotoxicology 40:1–7
Corea F, Silvestrelli G, Baccarelli A et al (2012) Airborne pollutants and lacunar stroke: a case cross-over analysis on stroke unit admissions. Neurol Int 4:e11
Power MC, Weisskopf MG, Alexeeff SE, Coull BA, Spiro A III, Schwartz J (2011) Traffic-related air pollution and cognitive function in a cohort of older men. Environ Health Perspect 119:682–687
Andersen ZJ, Olsen TS, Andersen KK, Loft S, Ketzel M, Raaschou-Nielsen O (2010) Association between short-term exposure to ultrafine particles and hospital admissions for stroke in Copenhagen, Denmark. Eur Heart J 31:2034–2040
Andersen ZJ, Kristiansen LC, Andersen KK et al (2012) Stroke and long-term exposure to outdoor air pollution from nitrogen dioxide: a cohort study. Stroke 43:320–325
Block ML, Calderon-Garciduenas L (2009) Air pollution: mechanisms of neuroinflammation and CNS disease. Trends Neurosci 32:506–516
Genc S, Zadeoglulari Z, Fuss SH, Genc K (2012) The adverse effects of air pollution on the nervous system. J Toxicol 2012:782462
Boeglin ML, Wessels D, Henshel D (2006) An investigation of the relationship between air emissions of volatile organic compounds and the incidence of cancer in Indiana counties. Environ Res 100:242–254
McKean-Cowdin R, Calle EE, Peters JM et al (2009) Ambient air pollution and brain cancer mortality. Cancer Causes Control 20:1645–1651
Liu CC, Chen CC, Wu TN, Yang CY (2008) Association of brain cancer with residential exposure to petrochemical air pollution in Taiwan. J Toxicol Environ Health A 71:310–314
Raaschou-Nielsen O, Andersen ZJ, Hvidberg M et al (2011) Air pollution from traffic and cancer incidence: a Danish cohort study. Environ Health 10:67
Thygesen LC, Daasnes C, Thaulow I, Bronnum-Hansen H (2011) Introduction to Danish (nationwide) registers on health and social issues: structure, access, legislation, and archiving. Scand J Public Health 39:12–16
Pedersen CB (2011) The Danish civil registration system. Scand J Public Health 39:22–25
Gjerstorff ML (2011) The Danish cancer registry. Scand J Public Health 39:42–45
Storm HH, Michelsen EV, Clemmensen IH, Pihl J (1997) The Danish Cancer Registry—history, content, quality and use. Dan Med Bull 44:535–539
Raaschou-Nielsen O, Sorensen M, Ketzel M et al (2013) Long-term exposure to traffic-related air pollution and diabetes-associated mortality: a cohort study. Diabetologia 56:36–46
Berkowicz R, Ketzel M, Jensen SS, Hvidberg M, Raaschou-Nielsen O (2008) Evaluation and application of OSPM for traffic pollution assessment for a large number of street locations. Environ Model Softw 23:296–303
Raaschou-Nielsen O, Hertel O, Vignati E et al (2000) An air pollution model for use in epidemiological studies: evaluation with measured levels of nitrogen dioxide and benzene. J Expo Anal Environ Epidemiol 10:4–14
Ketzel M, Berkowicz R, Hvidberg M, Jensen SS, Raaschou-Nielsen O (2011) Evaluation of AirGIS: a GIS-based air pollution and human exposure modelling system. Int J Environ Pollut 47:226–238
Ketzel M, Wahlin P, Berkowicz R, Palmgren F (2003) Particle and trace gas emission factors under urban driving conditions in Copenhagen based on street and roof level observations. Atmos Environ 37:2735–2749
Hertel O, Jensen S, Andersen H et al (2001) Human exposure to traffic pollution. Experience from Danish studies. Pure Appl Chem 73:137–145
Sorensen M, Hoffmann B, Hvidberg M et al (2012) Long-term exposure to traffic-related air pollution associated with blood pressure and self-reported hypertension in a Danish cohort. Environ Health Perspect 120:418–424
Andersen ZJ, de Nazelle A, Mendez MA et al (2015) A study of the combined effects of physical activity and air pollution on mortality in elderly urban residents: the Danish diet, cancer, and health cohort. Environ Health Perspect 123:557–563
Andersen ZJ, Bonnelykke K, Hvidberg M et al (2012) Long-term exposure to air pollution and asthma hospitalisations in older adults: a cohort study. Thorax 67:6–11
Acknowledgments
We wish to express particular thanks to Nick Martinussen for his tireless efforts with the data management.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Poulsen, A.H., Sørensen, M., Andersen, Z.J. et al. Air pollution from traffic and risk for brain tumors: a nationwide study in Denmark. Cancer Causes Control 27, 473–480 (2016). https://doi.org/10.1007/s10552-016-0721-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-016-0721-x