
Abstract
Purpose
Inter-individual differences in estrogen concentrations during treatment with aromatase inhibitors (AIs) may contribute to therapeutic response and toxicity. The aim of this study was to determine plasma concentrations of estradiol (E2), estrone (E1), and estrone sulfate (E1S) in a large cohort of AI-treated breast cancer patients.
Methods
In a randomized, multicenter trial of postmenopausal women with early-stage breast cancer starting treatment with letrozole (n = 241) or exemestane (n = 228), plasma estrogen concentrations at baseline and after 3 months were quantitated using a sensitive mass spectrometry-based assay. Concentrations and suppression below the lower limit of quantification (LLOQ) were compared between estrogens and between drugs.
Results
The ranges of baseline estrogen concentrations were <LLOQ–361 pg/mL for E2, <LLOQ–190 pg/mL for E1, and 8.3–4060 pg/mL for E1S. For E2, the frequency of suppression below the LLOQ was not statistically significantly different between AIs (exemestane: 89.0%, letrozole: 86.9%, p = 0.51). However, patients on letrozole were more likely to achieve suppression below the LLOQ of both E1 (exemestane: 80.1%, letrozole: 90.1%, p = 0.005) and E1S (exemestane: 17.4%, letrozole: 54.9%, p = 4.34e−15). After 3 months of AI therapy, the ranges of estrogen concentrations were <LLOQ–63.8 pg/mL, <LLOQ–36.7 pg/mL, and <LLOQ–1090 pg/mL for E2, E1, and E1S, respectively. During treatment, 16 patients had an increased concentration compared to the baseline concentration of at least one estrogen.
Conclusions
Letrozole had greater suppression of plasma E1 and E1S than exemestane, though the response was highly variable among patients. Additional research is required to examine the clinical relevance of differential estrogen suppression.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The aromatase inhibitors (AIs), such as anastrozole, exemestane, and letrozole, are recommended as first-line anti-estrogen therapy in postmenopausal women with hormone receptor (HR)-positive, early-stage breast cancer [1]. Anastrozole and letrozole, which are both azoles, are competitive inhibitors of aromatase. In contrast, the steroidal exemestane is an inactivator of aromatase. Clinical response to these drugs varies widely among patients. Adjuvant AI therapy significantly reduces breast cancer mortality compared to the selective estrogen receptor modulator tamoxifen, and therefore by extension compared to no endocrine therapy [2]. However, a substantial proportion of patients with HR-positive breast cancer will nonetheless develop recurrent disease despite receiving adjuvant AI therapy [2]. In addition, many patients develop adverse effects during AI therapy that may lead to treatment discontinuation [3].
Taken together, these data suggest heterogeneity in response to and toxicity from AI therapy. Currently, only standard factors such as pathologic stage are used to identify those patients at high risk of disease recurrence, and there are no validated biomarkers of increased risk of toxicity. We hypothesize that multiple mechanisms account for variable response to AIs including inter-patient differences in residual estrogen concentrations achieved during AI treatment [4]. The goal of many previous studies measuring AI-induced changes in blood estrogens and whole-body aromatization of androgens was to estimate and compare potency among AIs, with less attention to variability in their effects [4, 5]. Even so, many studies suggest heterogeneity in the pharmacologic effect of AIs [5–7]. However, it is unlikely that the heterogeneity observed in these early smaller trials, which were designed to conduct intensive monitoring and measurements, accurately reflects the effects of AIs on estrogen concentrations in the larger breast cancer population.
On average, third-generation AIs cause aromatase inhibition of at least 97.9% [8]. As a result, the ability to measure variability in residual estrogens during AI therapy requires analytical methods that are selective and sensitive [9–11]. Routine immunoassays for estradiol used in most clinical laboratories are not sufficiently sensitive to measure low concentrations of estradiol during AI therapy [12–14]. Furthermore, immune-based routine clinical assays cross-react with exemestane, the steroidal AI, which may result in the underestimation of the degree of estrogen suppression in patients receiving treatment with the medication [6]. In contrast, mass spectrometry-based methods are highly sensitive and more accurate for the measurement of low levels of estradiol [13, 15].
We conducted a prospective, randomized clinical trial of postmenopausal women with HR-positive breast cancer who were randomly assigned to letrozole or exemestane, and had serial plasma concentrations of E2, E1, and E1S measured using a selective and ultra-sensitive gas chromatography–tandem mass spectrometry (GC/MS/MS) assay. In these analyses, we examine the inter-patient heterogeneity in the reduction of circulating concentrations of estrogens during treatment with the two AI medications.
Methods
Patients
This analysis of plasma estrogens was conducted as one component of a prospective, open-label clinical trial, the Exemestane vs. Letrozole Pharmacogenomics (ELPh) study (ClinicalTrials.gov identifier: NCT00228956) conducted by the Consortium on Breast Cancer Pharmacogenomics (COBRA), a team of investigators from the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University, the University of Michigan Comprehensive Cancer Center, and the Indiana University Melvin and Bren Simon Cancer Center. The study design and inclusion and exclusion criteria have been previously described in detail [16, 17]. Briefly, eligible participants were postmenopausal women diagnosed with stage 0-III hormone receptor-positive breast cancer initiating AI therapy either as upfront adjuvant therapy or following tamoxifen therapy. Patients were screened and recruited at the study sites from August 2005 through July 2009. Recommended surgery, chemotherapy, and radiation for breast cancer were completed prior to study enrollment. The study was approved by the institutional review board at each study site and reviewed biannually by an independent data and safety monitoring committee. Written informed consent was obtained from each patient prior to undergoing protocol-directed procedures.
Study design
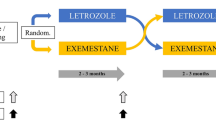
Eligible patients were stratified based on prior chemotherapy, prior tamoxifen therapy, and prior bisphosphonate use and then randomized to receive 25 mg exemestane or 2.5 mg letrozole orally once per day for 2 years. Venous blood samples were drawn in heparinized green top tubes prior to starting the study drug (baseline) and after 3 months of AI therapy. Patients who discontinued AI therapy before the 3-month time point, which occurred primarily because of drug toxicity, had plasma estrogens measured at baseline only [3]. Plasma was isolated after centrifugation at 1600×g for 10 min at 4 °C. Patients were requested to take the AI approximately 2 h before the estimated time of blood draw.
Analysis of exemestane and letrozole plasma concentrations
A liquid chromatography–tandem mass spectrometry (LC/MS/MS) method was developed to quantify steady-state plasma exemestane concentrations, whereas steady-state plasma letrozole concentrations were quantified using high-performance liquid chromatography with fluorescence detection, as previously described by Desta et al. [18] (described in Online Resource 1).
Analysis of estrogens in plasma
Plasma E2, E1, and E1S concentrations were measured by inVentiv Health (Princeton, NJ) using an established gas chromatography–tandem mass spectrometry (GC/MS/MS) assay [15]. Briefly, the analytes and deuterated internal standards were extracted from 0.4 mL of human plasma using Bond Elut Certify® solid–phase cartridges. Compounds were eluted from the cartridges with ethyl acetate and then underwent three separate derivatizations: reaction with pentafluorobenzoyl chloride, reaction with O–(2,3,4,5,6–pentafluorobenzyl)-hydroxylamine hydrochloride, and reaction with N-methyl-N-(trimethylsilyl) trifluoroacetamide. The derivatized analytes and standards were separated by gas chromatography and detected by tandem mass spectrometry using negative-ion chemical ionization. Calibration curves were obtained by performing weighted linear regression (weighted 1/x2) on the calibration standards. Lower and upper limits of quantification for each estrogen were dependent on the calibration curve for the corresponding analytical run. As a result, two lower limits of quantification (LLOQs) were observed for E2 and E1, which reflect slight variability in the assay between analytical runs. LLOQs for E2 were 0.625 or 1.25 pg/mL, LLOQs for E1 were 1.56 or 3.12 pg/mL, and the LLOQ for E1S was 3.13 pg/mL. Upper limits of quantification (ULOQs) for E2, E1, and E1S were 80, 200, and 800 pg/mL, respectively.
Characteristics of plasma estrogen measurements
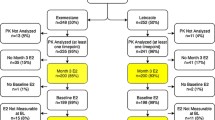
Not all patients had samples available at both baseline and after 3 months (Fig. 1). Reasons for missing data included patient withdrawal, insufficient sample volume, inability to draw blood, or un-assayed samples. Two patients with month-3 estrogen samples were excluded from the analysis because insufficient plasma was available for baseline measurements.

Patient flow diagram. Reasons for patient plasma samples not being assayed included the following: a No sample (N = 2); not enough sample (N = 1); sample not assayed (N = 6). b Unable to draw blood (N = 1); not enough sample (N = 8); sample not assayed (N = 12). c Unable to draw blood (N = 2); not enough sample (N = 4); sample not assayed (N = 11). d Not enough sample (N = 3); sample not assayed (N = 5)
Based on an initial review of the plasma estrogen concentrations, the following exclusion criteria were applied prior to data analysis. Nine patients had baseline plasma concentrations of one or more estrogens above the respective assay ULOQ. Due to uncertainty in the true concentrations in these samples, these specific measurements were excluded from data analysis. None of the estrogen concentrations were above the ULOQ after 3 months of AI therapy. In addition, the concentration of estrogens in some plasma samples could not be reliably determined and these specific measurements were also excluded from analysis (baseline: n = 3, month-3: n = 8). Excluding one estrogen metabolite from analysis did not influence the inclusion of other successfully measured estrogens in a given plasma sample (Online Resource 2).
Change in one or more estrogens could not be assessed in fifteen patients because both the baseline and month-3 concentrations were at or below the LLOQ. These pairs of estrogen measurements were excluded from the analysis of change due to the inability to detect a drug effect; however, the baseline and month-3 concentrations were included in the analysis at the respective time points. In total, concentration change from baseline to month-3 was not calculated for 18 pairs of estrogen measurements from 15 individual patients: E2 only (N = 10), E1 only (N = 2), E2 and E1 (N = 2), and E2 and E1S (N = 1). Ten of these fifteen patients were randomized to receive exemestane and five to receive letrozole.
Statistical analysis
The primary objective of the ELPh trial was to examine the correlation between changes in breast density and genetic variants in CYP19A1 [17]. In the pre-planned subanalysis reported in this manuscript, we describe the inter-patient heterogeneity in plasma estrogens before and during AI therapy. Preliminary descriptive analysis suggested that plasma estrogen concentrations were well described by a lognormal distribution, and therefore measurements were log10-transformed for data presentation and correlation analysis. Unless otherwise specified, summary statistics are given in the original scale as their median values [first quartile (Q1), third quartile (Q3)], where Q1 and Q3 are the median values of the bottom and top half of ranked values, respectively. Variability in plasma concentrations is described as standard deviation (SD) for log10-transformed concentrations and percent coefficient of variation (CV %) in the original scale, where CV % is calculated from log10-transformed concentrations (\({\text{CV}}\% = 100 \times \sqrt {e^{{\left( {{\text{SD}} \times \ln 10} \right)^{2} }} - 1}\)). Estrogen concentrations below the respective assay LLOQs were fixed at the LLOQ to approximate the actual sample concentration for percent-change and fold-change calculations. The frequency of suppression below the assay LLOQ at baseline and month-3 was compared between drugs using Chi square tests or Fisher’s exact test when appropriate. The drug effect on estrogen suppression below the assay LLOQs was determined using McNemar’s test. Estrogen concentrations and change from baseline were compared between patients randomized to exemestane or letrozole using the Wilcoxon rank-sum test and the drug-induced change within patients was analyzed by Wilcoxon signed-rank test. Pearson’s correlation coefficients (r) and p values were determined for pairwise correlation between concentrations of plasma estrogens at baseline. Statistical analysis and plotting were performed using R (version 2.15.2, Vienna, Austria). Due to limits of the statistical package’s numerical precision, p values smaller than 2.2e−16 are reported as “<2.2e−16.”
Results
Characteristics of patients and plasma estrogen measurements
Baseline demographics and clinical characteristics of patients enrolled in this study have been described in detail previously [3]. Briefly, the median age was 59 years, 88.2% of patients were white, and the mean BMI was 29.9 kg/m2. Baseline plasma estrogen concentrations were measured in 241 of 252 patients randomized to letrozole (96%) and 228 of 248 patients randomized to exemestane (92%) (Fig. 1). Following 3 months of AI therapy, plasma estrogens were measured from 204 patients receiving letrozole (85%) and 201 patients (88%) receiving exemestane. Reasons for missing data are described in the “Methods” section.
Estradiol, estrone, and estrone sulfate concentrations in plasma prior to and during exemestane or letrozole therapy
Estrogen concentrations at baseline
To qualitatively describe the effect of AI treatment on plasma estrogens, we classified patients based on whether baseline and month-3 estrogen concentrations were greater or less than the respective assay LLOQs. At baseline, 2.8, 0.9, and 0.2% of patients had E2, E1, and E1S concentrations below the assay LLOQ, respectively (Table 1). However, although all participants were considered postmenopausal at entry based on clinical assessment, baseline concentrations of quantifiable estrogens were highly variable, ranging from the LLOQ–361.00 pg/mL (CVE2(%) = 176) for E2, from the LLOQ–190.00 pg/mL (CVE1(%) = 106) for E1, and from the LLOQ–4060.00 pg/mL (CVE1S(%) = 181) for E1S (Fig. 2, Table 2).

Distribution of plasma estrogen concentrations at baseline and during exemestane or letrozole therapy. The frequency distribution of log-transformed concentrations of estradiol (a), estrone (b), and estrone sulfate (c) are represented as red bars at baseline (BL), while month-3 (M3) concentrations are represented as blue bars. Bin widths are 1/30th of the log-transformed concentration of each estrogen. Boxplots plotted above each histogram provide additional distributional detail of log-transformed concentrations at baseline (red) and M3 (blue). Boxplots depict five-number summaries as horizontal lines representing (from left to right) 75th percentile + (1.5 × interquartile range) (end of upper whisker), 75th percentile, median, 25th percentile, and 25th percentile—(1.5 × interquartile range) (end of lower whisker)
Estrogen concentrations during AI therapy
Month-3 concentrations of E2, E1, and E1S fell below assay LLOQ in 87.9, 85.1, and 36.3% of patients, respectively (Table 1). The frequency of E2 suppression below LLOQ was not statistically significantly different between AIs (exemestane: 89.0%, letrozole: 86.9%, p = 0.51); however, significant differences were observed for both E1 and E1S. E1 concentrations were reduced below the assay LLOQ in 90.1% of patients taking letrozole, compared to 80.1% of patients taking exemestane (p = 0.005). Similarly, although 54.9% of patients taking letrozole had month-3 E1S concentrations below the assay LLOQ, this reduction was only observed in 17.4% of patients taking exemestane (p = 4.34e−15).
Comparing analyte levels during treatment with the two drugs by fixing concentrations below the assay LLOQ at the LLOQ yielded similar findings to the analysis of the proportion of patients with estrogen levels below the LLOQ during AI therapy. Mean log10 plasma E2 concentrations during therapy were not different between the two drugs (p = 0.60, Fig. 2, Table 2). In contrast, mean log10 concentrations of both E1 and E1S at month-3 were significantly higher in patients receiving exemestane versus letrozole (E1: exemestane 0.29 (SD 0.24), letrozole 0.24 (SD 0.18), p = 0.007; E1S: exemestane 1.07 (SD 0.43), letrozole 0.78 (SD 0.49), p < 0.0001). Despite a significant reduction of plasma concentrations in response to AI therapy, estrogen concentrations remaining above the respective assay LLOQs during therapy exhibited large inter-patient variability (Fig. 2).
Inter-individual variability in drug-induced change in plasma estrogens during letrozole and exemestane therapy
The majority of patients had reduced plasma estrogen concentrations after 3 months of AI treatment compared to baseline (Fig. 2). However, the effect of AI treatment on plasma estrogens calculated as intra-individual change from baseline concentrations showed a large variability in response to both AIs (Fig. 3). In the group of 185 patients receiving exemestane with paired baseline and month-3 E2 measurements, 167 (90.2%) achieved 90% reduction from baseline or had a month-3 value below the LLOQ. For E1 and E1S, the number of exemestane-treated patients achieving that degree of suppression was 153 (82.7%) and 144 (77.8%), respectively. Similarly, of the 158 letrozole-treated patients with paired baseline and month-3 samples, the number of patients who achieved a 90% reduction from baseline or had a month-3 value below the LLOQ was 138 (87.3%) for E2, 145 (91.8%) for E1, and 142 (89.9%) for E1S.

Intra-individual change in plasma estrogen concentrations during exemestane or letrozole therapy. Lines join log-transformed plasma concentrations of estradiol (a), estrone (b), or estrone sulfate (c) prior to and following 3 months of exemestane or letrozole therapy. Each line represents a subject. Month-3 estrogen concentrations determined to be below the respective assay LLOQ were fixed at the assay LLOQ
Some of the observed variability in month-3 concentrations and percent change from baseline could be attributed to patients with increased concentrations of one or more estrogen metabolites from baseline. Of the patients with E2 (n = 384), E1 (n = 398), or E1S (n = 402) measured at baseline and month-3, we observed increased concentrations of one or more estrogens in 16 patients. Estrogen concentrations, drug concentrations, and clinical characteristics of these patients are presented in Online Resource 3. Five of the 16 patients had increased concentrations of at least two estrogens, and three of these five patients had increased concentrations of all 3 estrogens. The remaining 11 patients had increased concentration of only one estrogen, with the corresponding decreases in the other measured estrogens. Nine of these 11 patients had increased E2 concentrations from baseline. Interestingly, exemestane or letrozole was detected in the plasma of all 16 patients who exhibited increases in 1 or more estrogens, confirming that the patients were adhering to their therapy.
Relationships among plasma E2, E1, and E1S concentrations prior to AI therapy
Prior to treatment initiation, we observed statistically significant, strongly positive pairwise correlations between plasma concentrations of all estrogen pairs. The Pearson’s correlation coefficient for the correlation between E2 and E1 concentrations was r = 0.74 (p < 2.2e−16), for E1 and E1S concentrations it was r = 0.69 (p < 2.2e−16), and for E2 and E1S concentrations it was r = 0.63 (p < 2.2e−16) (Online Resource 4).
Discussion
In this prospective, randomized study examining the pharmacokinetic and pharmacodynamic effects of two third-generation AIs in postmenopausal women with HR-positive breast cancer, we compared the relative suppression of plasma estrogens between the nonsteroidal AI letrozole and the steroidal AI exemestane, with specific attention to inter-patient variability in the pharmacodynamic effects. Baseline estrogen concentrations were highly variable among patients and were consistent with those previously reported for postmenopausal women when measured with highly sensitive assays [19–21]. During treatment with the AIs, there was significant inter-patient heterogeneity in the degree of estrogen suppression, which may have potential clinical relevance.
Our observations are consistent with a previous study demonstrating variability in conjugated plasma estrogen changes in breast cancer patients receiving a different nonsteroidal AI, anastrozole. In that study, plasma estrogens were analyzed using the same highly sensitive methodology employed in our analysis [19, 22]. Taken together, these studies demonstrate that circulating conjugated estrogens persist in a substantial number of patients receiving AI therapy, while the concentrations of unconjugated estrogens above the assays’ LLOQ are uncommon in AI-treated patients.
Data from our study are in agreement with previous work, suggesting that letrozole is a more potent suppresser of estrogen production than exemestane and anastrozole [5, 6, 23, 24]. Notably, these differences in average potency have not translated into differences in clinical outcomes in large randomized trials comparing AIs [25]. However, it is possible that the continued presence of detectable systemic levels of conjugated estrogens could have clinical significance for the minority of patients with incomplete suppression of estrogens and lead to AI resistance. Although circulating E2 is suppressed below the LLOQ in the vast majority of patients, inter-conversion of E1 and E2 or desulfation of E1S through the action of tissue-specific sulfatases may significantly increase the tissue content of unconjugated estrogens in the breast and therefore influence local estrogen-dependent processes [26–29]. The association between concentrations of estrogens during AI therapy and disease outcomes has not been directly examined in the previously conducted large prospective trials. In addition, despite the use of a highly sensitive assay, we were unable to quantify plasma concentrations of the unconjugated estrogens, E2 and E1, for the majority of patients during AI treatment. A more complete characterization of the effects of the absolute degree of estrogen suppression on disease and toxicity outcome relationships may require an assay to measure unconjugated estrogens with an LLOQ several fold lower than the assay used in this study.
There are a number of factors that could mediate the variability in plasma estrogen concentrations during AI exposure identified in our study, including germline genetic variation in genes mediating estrogen biosynthesis and metabolism, adiposity, noncompliance with therapy, and variable drug exposure [22, 30–32]. However, not all studies have demonstrated positive associations with these factors, potentially due to differences in the genetic variants analyzed or differences in estrogen measurement methods [33, 34]. The 16 patients in our study who had an increase in one or more estrogens after 3 months of therapy compared to baseline had detectable drug concentrations, although they did not have suppression of all circulating estrogens. It is possible that a subset of patients had experienced the recovery of ovarian production of estrogen, thereby accounting for lack of suppression of estrogen [14, 35]. However, this is a plausible reason in only a minority of the patients considering that 11 of the 16 patients were above age 50 and at least two of the younger patients had undergone bilateral oophorectomy. Alternative explanations include rebound or incomplete suppression of plasma estrogens resulting from intermittent usage of therapy, or pharmacologic mechanisms, such as incomplete aromatase inhibition.
In summary, in these data derived from a large prospective randomized trial of postmenopausal women starting AI therapy, we demonstrated considerable variability in circulating estrogen concentrations. For each of the estrogens, more than 80% of patients had suppression to at least 90% of the baseline level or to below the level of quantification, although a minority of patients failed to achieve that goal. Failure to adequately suppress estrogen production is a potential mechanism of resistance for AI therapy. However, because of methodologic issues related to the measurement of estrogens, investigation of this mechanism remains challenging. Studies that examine the associations between the effect of AI therapy on circulating estrogens and the effects of AI therapy on disease outcomes and secondary effects are essential for tailoring therapy for individual patients in order to optimize the benefits and risks of endocrine therapy.
References
Burstein HJ, Prestrud AA, Seidenfeld J, Anderson H, Buchholz TA, Davidson NE, Gelmon KE, Giordano SH, Hudis CA, Malin J et al (2010) American Society of Clinical Oncology clinical practice guideline: update on adjuvant endocrine therapy for women with hormone receptor-positive breast cancer. J Clin Oncol 28:3784–3796. doi:10.1200/JCO.2009.26.3756
Early Breast Cancer Trialists’ Collaborative Group, Dowsett M, Forbes JF, Bradley R, Ingle J, Aihara T, Bliss J, Boccardo F, Coates A, Coombes RC et al (2015) Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials. Lancet 386:1341–1352. doi:10.1016/S0140-6736(15)61074-1
Henry NL, Azzouz F, Desta Z, Li L, Nguyen AT, Lemler S, Hayden J, Tarpinian K, Yakim E, Flockhart DA et al (2012) Predictors of aromatase inhibitor discontinuation due to treatment-emergent symptoms in early-stage breast cancer. J Clin Oncol 30:936–942
Felson DT, Cummings SR (2005) Aromatase inhibitors and the syndrome of arthralgias with estrogen deprivation. Arthritis Rheum 52:2594–2598
Geisler J, Haynes B, Anker G, Dowsett M, Lonning PE (2002) Influence of letrozole and anastrozole on total body aromatization and plasma estrogen levels in postmenopausal breast cancer patients evaluated in a randomized, cross-over study. J Clin Oncol 20:751–757
Geisler J, King N, Anker G, Ornati G, Di Salle E, Lonning PE, Dowsett M (1998) In vivo inhibition of aromatization by exemestane, a novel irreversible aromatase inhibitor, in postmenopausal breast cancer patients. Clin Cancer Res 4:2089–2093
Geisler J, King N, Dowsett M, Ottestad L, Lundgren S, Walton P, Kormeset PO, Lonning PE (1996) Influence of anastrozole (Arimidex), a selective, non-steroidal aromatase inhibitor, on in vivo aromatisation and plasma oestrogen levels in postmenopausal women with breast cancer. Br J Cancer 74:1286–1291
Folkerd EJ, Lonning PE, Dowsett M (2014) Interpreting plasma estrogen levels in breast cancer: caution needed. J Clin Oncol 14:1396–1400 [pii] JCO.2013.53.9411
Geisler J, Lonning PE (2005) Endocrine effects of aromatase inhibitors and inactivators in vivo: review of data and method limitations. J Steroid Biochem Mol Biol 95:75–81. doi:10.1016/j.jsbmb.2005.04.015
Stanczyk FZ, Lee JS, Santen RJ (2007) Standardization of steroid hormone assays: why, how, and when? Cancer Epidemiol Biomark Prev 16:1713–1719
Rosner W, Hankinson SE, Sluss PM, Vesper HW, Wierman ME (2013) Challenges to the measurement of estradiol: an Endocrine Society position statement. J Clin Endocrinol Metab 98:1376–1387. doi:10.1210/jc.2012-3780
Stanczyk FZ, Clarke NJ (2014) Measurement of estradiol–challenges ahead. J Clin Endocrinol Metab 99:56–58. doi:10.1210/jc.2013-2905
Jaque J, Macdonald H, Brueggmann D, Patel SK, Azen C, Clarke N, Stanczyk FZ (2013) Deficiencies in immunoassay methods used to monitor serum Estradiol levels during aromatase inhibitor treatment in postmenopausal breast cancer patients. Springerplus 2:5. doi:10.1186/2193-1801-2-5
Henry NL, Xia R, Banerjee M, Gersch C, McConnell D, Giacherio D, Schott AF, Pearlman M, Stearns V, Partridge AH et al (2013) Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol 24:2011–2016
Santen RJ, Demers L, Ohorodnik S, Settlage J, Langecker P, Blanchett D, Goss PE, Wang S (2007) Superiority of gas chromatography/tandem mass spectrometry assay (GC/MS/MS) for estradiol for monitoring of aromatase inhibitor therapy. Steroids 72:666–671
Henry NL, Giles JT, Ang D, Mohan M, Dadabhoy D, Robarge J, Hayden J, Lemler S, Shahverdi K, Powers P et al (2008) Prospective characterization of musculoskeletal symptoms in early stage breast cancer patients treated with aromatase inhibitors. Breast Cancer Res Treat 111:365–372
Henry NL, Chan HP, Dantzer J, Goswami CP, Li L, Skaar TC, Rae JM, Desta Z, Khouri N, Pinsky R et al (2013) Aromatase inhibitor-induced modulation of breast density: clinical and genetic effects. Br J Cancer 109:2331–2339. doi:10.1038/bjc.2013.587
Desta Z, Kreutz Y, Nguyen AT, Li L, Skaar T, Kamdem LK, Henry NL, Hayes DF, Storniolo AM, Stearns V et al (2011) Plasma letrozole concentrations in postmenopausal women with breast cancer are associated with CYP2A6 genetic variants, body mass index, and age. Clin Pharmacol Ther 90:693–700. doi:10.1038/clpt.2011.174
Ingle JN, Buzdar AU, Schaid DJ, Goetz MP, Batzler A, Robson ME, Northfelt DW, Olson JE, Perez EA, Desta Z et al (2010) Variation in anastrozole metabolism and pharmacodynamics in women with early breast cancer. Cancer Res 70:3278–3286 [pii] 0008-5472.CAN-09-3024
Lee JS, Ettinger B, Stanczyk FZ, Vittinghoff E, Hanes V, Cauley JA, Chandler W, Settlage J, Beattie MS, Folkerd E et al (2006) Comparison of methods to measure low serum estradiol levels in postmenopausal women. J Clin Endocrinol Metab 91:3791–3797
Warren R, Skinner J, Sala E, Denton E, Dowsett M, Folkerd E, Healey CS, Dunning A, Doody D, Ponder B et al (2006) Associations among mammographic density, circulating sex hormones, and polymorphisms in sex hormone metabolism genes in postmenopausal women. Cancer Epidemiol Biomark Prev 15:1502–1508 [pii] 15/8/1502
Ingle JN, Kalari KR, Buzdar AU, Robson ME, Goetz MP, Desta Z, Barman P, Dudenkov TT, Northfelt DW, Perez EA et al (2015) Estrogens and their precursors in postmenopausal women with early breast cancer receiving anastrozole. Steroids 99:32–38. doi:10.1016/j.steroids.2014.08.007
Dixon JM, Renshaw L, Young O, Murray J, Macaskill EJ, McHugh M, Folkerd E, Cameron DA, A’Hern RP, Dowsett M (2008) Letrozole suppresses plasma estradiol and estrone sulphate more completely than anastrozole in postmenopausal women with breast cancer. J Clin Oncol 26:1671–1676
Geisler J, Helle H, Ekse D, Duong NK, Evans DB, Nordbo Y, Aas T, Lonning PE (2008) Letrozole is superior to anastrozole in suppressing breast cancer tissue and plasma estrogen levels. Clin Cancer Res 14:6330–6335. doi:10.1158/1078-0432.CCR-07-5221
Goss PE, Ingle JN, Pritchard KI, Ellis MJ, Sledge GW, Budd GT, Rabaglio M, Ansari RH, Johnson DB, Tozer R et al (2013) Exemestane versus anastrozole in postmenopausal women with early breast cancer: NCIC CTG MA.27–a randomized controlled phase III trial. J Clin Oncol 31:1398–1404 [pii] JCO.2012.44.7805
Santner SJ, Feil PD, Santen RJ (1984) In situ estrogen production via the estrone sulfatase pathway in breast tumors: relative importance versus the aromatase pathway. J Clin Endocrinol Metab 59:29–33. doi:10.1210/jcem-59-1-29
Santner SJ, Leszczynski D, Wright C, Manni A, Feil PD, Santen RJ (1986) Estrone sulfate: a potential source of estradiol in human breast cancer tissues. Breast Cancer Res Treat 7:35–44
Lonning PE, Helle H, Duong NK, Ekse D, Aas T, Geisler J (2009) Tissue estradiol is selectively elevated in receptor positive breast cancers while tumour estrone is reduced independent of receptor status. J Steroid Biochem Mol Biol 117:31–41. doi:10.1016/j.jsbmb.2009.06.005
James MR, Skaar TC, Lee RY, MacPherson A, Zwiebel JA, Ahluwalia BS, Ampy F, Clarke R (2001) Constitutive expression of the steroid sulfatase gene supports the growth of MCF-7 human breast cancer cells in vitro and in vivo. Endocrinology 142:1497–1505. doi:10.1210/endo.142.4.8091
Wang L, Ellsworth KA, Moon I, Pelleymounter LL, Eckloff BW, Martin YN, Fridley BL, Jenkins GD, Batzler A, Suman VJ et al (2010) Functional genetic polymorphisms in the aromatase gene CYP19 vary the response of breast cancer patients to neoadjuvant therapy with aromatase inhibitors. Cancer Res 70:319–328. doi:10.1158/0008-5472.CAN-09-3224
Folkerd EJ, Dixon JM, Renshaw L, A’Hern RP, Dowsett M (2012) Suppression of plasma estrogen levels by letrozole and anastrozole is related to body mass index in patients with breast cancer. J Clin Oncol 30:2977–2980. doi:10.1200/JCO.2012.42.0273
Lonning PE, Haynes BP, Dowsett M (2014) Relationship of body mass index with aromatisation and plasma and tissue oestrogen levels in postmenopausal breast cancer patients treated with aromatase inhibitors. Eur J Cancer 50:1055–1064. doi:10.1016/j.ejca.2014.01.007
Lunardi G, Piccioli P, Bruzzi P, Notaro R, Lastraioli S, Serra M, Marroni P, Bighin C, Mansutti M, Puglisi F et al (2013) Plasma estrone sulfate concentrations and genetic variation at the CYP19A1 locus in postmenopausal women with early breast cancer treated with letrozole. Breast Cancer Res Treat 137:167–174. doi:10.1007/s10549-012-2306-z
Sini V, Lunardi G, Cirillo M, Turazza M, Bighin C, Giraudi S, Levaggi A, Piccioli P, Bisagni G, Gnoni R et al (2014) Body mass index and circulating oestrone sulphate in women treated with adjuvant letrozole. Br J Cancer 110:1133–1138. doi:10.1038/bjc.2014.2
Smith IE, Dowsett M, Yap YS, Walsh G, Lonning PE, Santen RJ, Hayes D (2006) Adjuvant aromatase inhibitors for early breast cancer after chemotherapy-induced amenorrhoea: caution and suggested guidelines. J Clin Oncol 24:2444–2447. doi:10.1200/JCO.2005.05.3694
Acknowledgements
This study was supported in part by the National Institutes of Health [Grant Numbers U-01GM61373 (DAF), 5T32-GM08425 (DAF, JDR), M01-RR000042 (UM), M01-RR00750 (IU), and M01-RR00052 (JHU)], the Department of Defense [Grant Number W81XWH-10-1-0349 (JDR)], Pfizer (DFH), Novartis Pharma AG (DFH), and the Fashion Footwear Association of New York/QVC Presents Shoes on Sale™ (DFH). Study medication was provided by Pfizer, Inc. and Novartis Pharma AG. We would like to thank the participating patients with breast cancer and the research nurse coordinators at each of the clinical trial sites. Finally, we express our gratitude to and respect for DAF, who provided tremendous expertise and leadership for this project prior to his untimely death.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
NLH received research funding from AstraZeneca, Eli Lilly, BioMarin Pharmaceuticals, Celldex Pharmaceuticals, and Sanofi Aventis. VS received research funding from Abbvie, Celgene, Medimmune, Merck, Novartis, Pfizer, and Puma. DFH worked as a consultant for Lilly Oncology, and received research funding from Merrimack, Lilly, Janssen R&D, Puma Biotechnology, Pfizer, and Astra Zeneca. DFH also has personal financial interest in Oncimmune and Inbiomotion and received royalties from Janssen R&D. DAF received research funding from Pfizer and Novartis and sat on the Scientific Board for Quest Diagnostics. The rest of the authors have no conflicts of interest to declare (JDR, ZD, ATN, LL, DLH, JMR, AMS, TCS).
Additional information
Todd C. Skaar, N. Lynn Henry: co-senior authors.
Rights and permissions
About this article

Cite this article
Robarge, J.D., Desta, Z., Nguyen, A.T. et al. Effects of exemestane and letrozole therapy on plasma concentrations of estrogens in a randomized trial of postmenopausal women with breast cancer. Breast Cancer Res Treat 161, 453–461 (2017). https://doi.org/10.1007/s10549-016-4077-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-016-4077-4