
Abstract
The average age-specific cumulative risk (penetrance) of breast cancer has been studied for BRCA1 and BRCA2 mutation carriers living in Western countries, but not for those living in East Asian countries where the population breast cancer incidence is lower. From 2007 to 2011, the Korean Hereditary Breast Cancer study identified 151 BRCA1 and 225 BRCA2 mutation-carrying families from family cancer clinics. We estimated the hazard ratio (HR) for female carriers relative to the population, and hence the penetrance, using a modified segregation analysis of cancer family histories conditioned on ascertainment. The breast cancer HR estimates [95 % confidence interval (CI)] for BRCA1 and BRCA2 mutation carriers were 18 (3–103) and 11 (5–27), respectively. The breast cancer penetrance estimates (95 % CI) to age 70 years were 49 % (11–98) and 35 % (16–65) for BRCA1 and BRCA2 mutation carriers, respectively. The breast cancer HR and penetrance estimates were similar for Korean and Western women (all P > 0.4). The point estimates of breast cancer penetrance were similar to age 50 years, though less for Korean carriers at older ages. Breast cancer risk for Korean and Western mutation carriers might reflect underlying population risks which in turn likely reflect differences in environmental and lifestyle factors. This raises the possibility of identifying modifiers of cancer risk for carriers with implications for prevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
BRCA1 and BRCA2 are tumor suppressor genes which play a role in DNA-damage repair, regulation of gene expression, and cell-cycle control [1]. Germline mutations in BRCA1 and BRCA2 are the most common known cause of hereditary breast and ovarian cancer [2], and screening for mutations in these genes is widely offered to women with a strong family history or early-onset breast cancer in countries with genetic counseling centers. Once a mutation carrier is identified, other family members are recommended to be tested for that particular mutation. Accurate estimate of the breast cancer risk for mutation carriers is critical to inform risk-reducing options [3].
The initial estimates of average cumulative breast cancer risk (penetrance) to age 70 years for female mutation carriers were 85 % for BRCA1 [4] and 84 % for BRCA2 [5]. Since these estimates were from studies of extreme multiple-case families with at least four family members with breast or ovarian cancer, these penetrance estimates might not be relevant for counseling mutation carriers without such a strong cancer family history [6, 7]. Consistent with this, studies of the relatives of population-based or hospital-based cases selected regardless of a family history have found lower estimates of penetrance to age 70 years, less than 60 % for breast cancer risk for BRCA1 mutation carriers and 30–56 % for BRCA2 mutation carriers [6, 8–12]. In addition, some studies have found evidence that risk varies by specific mutations [13, 14], other genetic modifiers [15–17], birth cohort [18, 19], and reproductive and lifestyle factors [20, 21].
But these studies have been conducted in Western populations, and breast cancer incidences are different in other populations. For women living in East Asia, the breast cancer incidences are lower and the age-specific incidences peak in younger age groups. Therefore, the published estimates might not be applicable for mutation carriers living in East Asian countries where, due to the combined size of their populations, a large proportion of the world’s BRCA1 and BRCA2 mutation carriers live. The aim of this study was to estimate the breast cancer penetrance for female carriers of germline mutations in BRCA1 and BRCA2 using a Korean nationwide study.
Materials and methods
Study participants
This study comprised families recruited into the Korean Hereditary Breast Cancer (KOHBRA) study during the period 2007–2011 from family cancer clinics. A proband is defined to be a person suspected of having hereditary breast cancer and who attended the family cancer clinic after referred by breast cancer surgeons based on their personal and family cancer histories. Details of the study design are described in full elsewhere [22]. The KOHBRA study is a prospective, nationwide, multicenter cohort study whose aims include determining the penetrance of breast cancer for BRCA1 and BRCA2 mutation carriers identified from mutation testing of eligible families. Mutation screening for BRCA1 and BRCA2 was performed for female probands with breast cancer aged 20 years or older, referred to the family cancer clinic, and who had (1) a family history of breast or ovarian cancer in any relatives; or (2) no family history of breast or ovarian cancer but was either 40 years or younger at diagnosis, had bilateral breast cancer, or was diagnosed with another primary malignancy. Male probands with breast cancer were also screened, irrespective of their cancer family history. If a screened person was found to have a mutation (see below for definition) in BRCA1 or BRCA2, they were asked to contact their female and male relatives aged 20 years or older to see if they too could be approached to participate in the KOHBRA study.
Mutation screening and definition
Screening for mutations in BRCA1 and BRCA2 was performed by four laboratories certified annually by the Korean Institute of Genetic Testing Evaluation. Each laboratory used various techniques, including fluorescence-based conformation-sensitive gel electrophoresis, denaturing high-performance liquid chromatography, or direct sequencing. This study was approved by the Institutional Review Board (IRB #B-0707-047-005) of each participating center, and all participants provided their written informed consent. A variant was considered a mutation if it was a protein-truncating mutation, or a missense mutation which has a confirmed association with disease [22].
Data collection
All participants were asked to complete a structured questionnaire and offered genetic counseling, during which a pedigree covering at least three generations was constructed. For each participant, information on year of birth, year of death, types of cancer, age at cancer diagnosis, genetic mutation status (carrier, non-carrier, not tested), and year of genetic counseling and mutation testing of both participants and family members was collected. If a participant could not give information on year of birth or year of death of a family member, we asked current age for living family members and age at death for deceased relatives. For living family members, participants had missing ages if they did not give information on either year of birth or current age. The missing information was imputed from the known birth year and/or current age of the siblings or spouse using average age differences between siblings or spouses in the general Korean population, or estimated from average age differences between generations within the general Korean population. Missing information on age at death for deceased individuals was imputed from individual age at cancer diagnosis if they had a cancer and otherwise treated as missing. Missing information was imputed for 14 % of living family members with missing information on age and 29 % of deceased family members with missing information on age at death. We excluded those with missing ages as the ages were considered to be unreliable.
Statistical analysis
Breast cancer penetrance for female mutation carriers was based on mutation-carrying families and was estimated using modified segregation analyses implemented in the pedigree analysis software MENDEL v3.3.5 [23]. The details of the model have been described previously [18, 23–25].
Estimation and statistical inference were carried out using the method of maximum likelihood. To adjust for the fact that families with multiple affected individuals were ascertained, we conditioned the likelihood on the genotype of the proband and the phenotypes (cancer statuses and related ages) of all family members. Female family members were assumed to be at risk of developing breast or ovarian cancer from birth until the earliest of breast cancer diagnosis, ovarian cancer diagnosis, death, last known age, or age 80 years.
A major gene model with mutation frequency of 0.001 for both genes was assumed (though risk estimates are not sensitive to this assumption, data not shown). Given the rarity of carriers, the incidences for non-carriers were assumed to be equal to the Korean population incidences obtained from the Korean Central Cancer Registry for the year 2010 [26]. The hazard ratio (HR) at age t years, defined as the age-specific incidence λ(t) for carriers divided by the age-specific incidence λ 0(t) for non-carriers, was estimated as both a constant function of age and as a log-linear function of age.
The modified segregation analysis therefore incorporated a parametric survival analysis, where λ(t) = HR λ 0(t). The cumulative risk to age t years (CR(t)) was estimated from the HR estimates as one minus the exponential of minus the cumulative risk to age t years (where the cumulative risk is the integral of λ(s) from 0 to t). The 10-year risk at age t years was estimated as (CR(t + 10) − CR(t))/(1 − CR(t)). Confidence intervals for cumulative and 10-year risks were estimated using a parametric bootstrap in which the HR estimates were sampled from their distributions under asymptotic likelihood theory.
To test if our HR estimates depended on calendar year of birth, we multiplied the above HRs by a log-linear function of year of birth and tested if this function differed from 1.
Results
Table 1 shows that there were 151 BRCA1 and 225 BRCA2 mutation-carrying families. Data were available for in total 12,820 family members (5012 were family members from BRCA1 mutation carriers’ pedigree information and 7808 were family members from BRCA2 mutation carriers’ pedigree information). From mutation testing, there were 227 confirmed carrier family members and 205 confirmed non-carrier family members. The mean age at diagnosis for breast cancer cases was 41.9 [standard deviation (SD) = 10.8] years for the BRCA1 mutation-carrying families, earlier than for the BRCA2 mutation-carrying families [44.8 (SD = 11.4), P = 0.001]. For proven BRCA1 mutation carrier breast cancer cases, the mean age at diagnosis was earlier than for proven BRCA2 mutation carriers (37.8 vs. 42.1 years, P < 0.001). The maximum age at diagnosis of breast cancer was 75 years for BRCA1 mutation carriers and 80 years for BRCA2 mutation carriers, and for ovarian cancer the corresponding ages were 75 and 79 years. There were no differences in mean age at diagnosis for ovarian cancer cases between BRCA1 and BRCA2 mutation-carrying families (P = 0.4) or between proven BRCA1 and BRCA2 carriers (P = 0.7).
The estimated breast cancer HRs were 18 [95 % confidence interval (CI) 3–103] and 11 (95 % CI 5–27) for BRCA1 and BRCA2 mutation carriers, respectively, when the HRs were assumed to be constant with age. There was weak evidence that the BRCA1 breast cancer HR depends on age (P = 0.15); the estimated HR decreased by 8 % (95 % CI 0–17) per year either side of a baseline of 29 (95 % CI 6–134) at age 40 years. There was no evidence that the BRCA2 breast cancer HR depends on age (P = 0.4). Consequently, all cumulative and 10-year risks below are based on the HRs being constant with age.
Table 2 shows that the estimated breast cancer penetrances to age 70 years were 49 % (95 % CI 11–98) and 35 % (95 % CI 16–65) for BRCA1 and BRCA2 mutation carriers, respectively. The estimates to age 50 years were 27 % (95 % CI 5–84) for BRCA1 mutation carriers and 18 % (95 % CI 8–39) for BRCA2 mutation carriers.
Table 3 shows that the estimated 10-year risks of breast cancer for unaffected BRCA1 and BRCA2 carriers peaked at ages of 40 and 50 years then decreased for older ages.
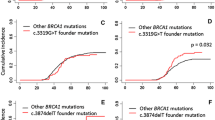
There was no evidence that the HRs depend on year of birth (all P > 0.5) or on mutation position (all P > 0.2, data not shown).
Discussion
To the best of our knowledge, this penetrance study is of the largest number of BRCA1 and BRCA2 mutation-carrying families living in Asia yet reported. We have derived the average cumulative cancer risks from the HRs estimated by modified segregation analysis and the age-specific breast cancer incidence in the general population in Korea. We have also provided 10-year risks of breast cancer for BRCA1 and BRCA2 mutation carriers who have not developed cancer before a given age, and this might be helpful in genetic counseling clinics to suggest surveillance strategies or prophylactic options. Previous studies have found that the risk assessment models developed in Western countries have poor performance for both prediction of breast cancer risk [27] and prediction of BRCA1 and BRCA2 mutation carrier status [28], suggesting a need for race- and country-specific models.
In Korea, the breast cancer incidence in the general population increases with age to peak in the mid-40s and is not dissimilar to the incidence in Western populations up to that age. But from the mid-40s onwards the incidence in Korea declines, in sharp contrast to Western populations where the incidence continues to increase for at least several decades [26, 27]. Therefore, if the breast cancer risk for carriers was independent of the country in which the carrier has lived and equal to that established for Western women, we should have found that the HRs for Korean women increase with age, especially after the mid-40s. We found no evidence for this.
The resulting point estimates of average cumulative breast cancer risks for Korean BRCA1 and BRCA2 mutation carriers were less than the corresponding estimates for Western women found by Antoniou et al. [18], in which the average cumulative risk of breast cancer to age 70 years was 65 % (95 % CI = 44–78) for BRCA1 mutation carriers and 45 % (95 % CI = 31–56) for BRCA2 mutation carriers. A recent meta-analysis of six family studies of population-based cases and four studies of families selected for family history found similar estimates: 57 % (95 % CI = 47–66) for BRCA1 and 49 % (95 % CI = 40–57) for BRCA2 mutation carriers [29]. However, given the wide CIs of the Korean estimates due to limited number of cases, comparison of our estimates with those of Western countries might be difficult statistically. In addition, we found few breast cancers in carrier families, let alone known carriers, diagnosed after the age of 50 years (six carrier breast cancer cases diagnosed after the age 50 years in 54 family members who were more than 50 years old and carriers of BRCA1 or BRCA2 mutations).
Our study has several weaknesses. First, we had to rely on the probands’ reported family history given during the genetic counseling and could not validate the cancer history of family members. Previous studies have shown that proband’s reporting is highly reliable, at least for breast cancers in first-degree relatives, in Western countries [30, 31]. Second, missing information on the ages of living family members or ages at diagnosis of deceased relatives with cancer was imputed in a conservative way. Although the misclassification of age could be random and unlikely to cause biased estimates, it would reduce the precision of estimates. Third, while we have taken the first steps to obtain valid unbiased estimates of risk that will be applicable to clinical mutation testing in families living in Korea and, perhaps more broadly, in other Asian families, our estimates are not precise due to limited number of carriers and mutation-tested family members.
Estimation of penetrance from the cancer histories of carrier families sampled because they have a cancer family history is non-trivial. One needs to condition the likelihood on why the carrier family came into the study [32], and for ‘clinic-based families’ conditioning only on the proband being affected will result in upwardly biased estimates [33, 34]. The likelihood approach we have taken here has been used extensively [6, 18, 24, 25], but is conservative in that it conditions on the entire family cancer history. It enables information on all family members to be used irrespective of their known mutation status, and clearly the more the information on which relatives carry mutations, the more information on risk. In practice it is often difficult, as we found, to obtain DNA samples from affected relatives in older generations.
In conclusion, the breast cancer risks for Korean and Western carriers might reflect the underlying population risks which in turn likely reflect environmental and lifestyle factors. This raises the possibility of identifying modifiers of risk through prospective studies of Asian and Western carriers. Finding the environmental and lifestyle factors that influence risk for mutation carriers is difficult using retrospective studies, but now that mutation testing has been carried out for two decades some prospective cohorts in Western populations are beginning to have power to address these issues, especially if the data are carefully pooled. It will be important to also establish similar cohorts of Asian women, and KOHBRA is working toward this aim.
References
Venkitaraman AR (2002) Cancer susceptibility and the functions of BRCA1 and BRCA2. Cell 108(2):171–182
Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J, Collins N, Gregory S, Gumbs C, Micklem G (1995) Identification of the breast cancer susceptibility gene BRCA2. Nature 378(6559):789–792. doi:10.1038/378789a0
Narod SA, Offit K (2005) Prevention and management of hereditary breast cancer. J Clin Oncol 23(8):1656–1663. doi:10.1200/jco.2005.10.035
Easton DF, Ford D, Bishop DT (1995) Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast cancer linkage consortium. Am J Hum Genet 56(1):265–271
Ford D, Easton DF, Stratton M, Narod S, Goldgar D, Devilee P, Bishop DT, Weber B, Lenoir G, Chang-Claude J, Sobol H, Teare MD, Struewing J, Arason A, Scherneck S, Peto J, Rebbeck TR, Tonin P, Neuhausen S, Barkardottir R, Eyfjord J, Lynch H, Ponder BA, Gayther SA, Zelada-Hedman M et al (1998) Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. The breast cancer linkage consortium. Am J Hum Genet 62(3):676–689
Hopper JL, Southey MC, Dite GS, Jolley DJ, Giles GG, McCredie MR, Easton DF, Venter DJ (1999) Population-based estimate of the average age-specific cumulative risk of breast cancer for a defined set of protein-truncating mutations in BRCA1 and BRCA2. Australian Breast Cancer Family Study. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive. Oncology 8(9):741–747
Levy-Lahad E, Friedman E (2007) Cancer risks among BRCA1 and BRCA2 mutation carriers. Br J Cancer 96(1):11–15. doi:10.1038/sj.bjc.6603535
Struewing JP, Hartge P, Wacholder S, Baker SM, Berlin M, McAdams M, Timmerman MM, Brody LC, Tucker MA (1997) The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med 336(20):1401–1408. doi:10.1056/nejm199705153362001
Warner E, Foulkes W, Goodwin P, Meschino W, Blondal J, Paterson C, Ozcelik H, Goss P, Allingham-Hawkins D, Hamel N, Di Prospero L, Contiga V, Serruya C, Klein M, Moslehi R, Honeyford J, Liede A, Glendon G, Brunet JS, Narod S (1999) Prevalence and penetrance of BRCA1 and BRCA2 gene mutations in unselected Ashkenazi Jewish women with breast cancer. J Natl Cancer Inst 91(14):1241–1247
Thorlacius S, Struewing JP, Hartge P, Olafsdottir GH, Sigvaldason H, Tryggvadottir L, Wacholder S, Tulinius H, Eyfjord JE (1998) Population-based study of risk of breast cancer in carriers of BRCA2 mutation. Lancet 352(9137):1337–1339
Anglian Breast Cancer Study Group (2000) Prevalence and penetrance of BRCA1 and BRCA2 mutations in a population-based series of breast cancer cases. Br J Cancer 83(10):1301–1308. doi:10.1054/bjoc.2000.1407
Satagopan JM, Offit K, Foulkes W, Robson ME, Wacholder S, Eng CM, Karp SE, Begg CB (2001) The lifetime risks of breast cancer in Ashkenazi Jewish carriers of BRCA1 and BRCA2 mutations. Cancer Epidemiol Biomark Prev 10(5):467–473
Thompson D, Easton D (2001) Variation in cancer risks, by mutation position, in BRCA2 mutation carriers. Am J Hum Genet 68(2):410–419. doi:10.1086/318181
Thompson D, Easton DF (2002) Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst 94(18):1358–1365
Ding YC, McGuffog L, Healey S, Friedman E, Laitman Y, Paluch-Shimon S, Kaufman B, Liljegren A, Lindblom A, Olsson H, Kristoffersson U, Stenmark-Askmalm M, Melin B, Domchek SM, Nathanson KL, Rebbeck TR, Jakubowska A, Lubinski J, Jaworska K, Durda K, Gronwald J, Huzarski T, Cybulski C, Byrski T, Osorio A, Cajal TR, Stavropoulou AV, Benitez J, Hamann U, Rookus M, Aalfs CM, de Lange JL, Meijers-Heijboer HE, Oosterwijk JC, van Asperen CJ, Gomez Garcia EB, Hoogerbrugge N, Jager A, van der Luijt RB, Easton DF, Peock S, Frost D, Ellis SD, Platte R, Fineberg E, Evans DG, Lalloo F, Izatt L, Eeles R, Adlard J, Davidson R, Eccles D, Cole T, Cook J, Brewer C, Tischkowitz M, Godwin AK, Pathak H, Stoppa-Lyonnet D, Sinilnikova OM, Mazoyer S, Barjhoux L, Leone M, Gauthier-Villars M, Caux-Moncoutier V, de Pauw A, Hardouin A, Berthet P, Dreyfus H, Ferrer SF, Collonge-Rame MA, Sokolowska J, Buys S, Daly M, Miron A, Terry MB, Chung W, John EM, Southey M, Goldgar D, Singer CF, Tea MK, Gschwantler-Kaulich D, Fink-Retter A, Hansen TV, Ejlertsen B, Johannsson OT, Offit K, Sarrel K, Gaudet MM, Vijai J, Robson M, Piedmonte MR, Andrews L, Cohn D, DeMars LR, DiSilvestro P, Rodriguez G, Toland AE, Montagna M, Agata S, Imyanitov E, Isaacs C, Janavicius R, Lazaro C, Blanco I, Ramus SJ, Sucheston L, Karlan BY, Gross J, Ganz PA, Beattie MS, Schmutzler RK, Wappenschmidt B, Meindl A, Arnold N, Niederacher D, Preisler-Adams S, Gadzicki D, Varon-Mateeva R, Deissler H, Gehrig A, Sutter C, Kast K, Nevanlinna H, Aittomaki K, Simard J, Spurdle AB, Beesley J, Chen X, Tomlinson GE, Weitzel J, Garber JE, Olopade OI, Rubinstein WS, Tung N, Blum JL, Narod SA, Brummel S, Gillen DL, Lindor N, Fredericksen Z, Pankratz VS, Couch FJ, Radice P, Peterlongo P, Greene MH, Loud JT, Mai PL, Andrulis IL, Glendon G, Ozcelik H, Gerdes AM, Thomassen M, Jensen UB, Skytte AB, Caligo MA, Lee A, Chenevix-Trench G, Antoniou AC, Neuhausen SL (2012) A nonsynonymous polymorphism in IRS1 modifies risk of developing breast and ovarian cancers in BRCA1 and ovarian cancer in BRCA2 mutation carriers. Cancer Epidemiol Biomark Prev 21(8):1362–1370. doi:10.1158/1055-9965.epi-12-0229
Antoniou AC, Kuchenbaecker KB, Soucy P, Beesley J, Chen X, McGuffog L, Lee A, Barrowdale D, Healey S, Sinilnikova OM, Caligo MA, Loman N, Harbst K, Lindblom A, Arver B, Rosenquist R, Karlsson P, Nathanson K, Domchek S, Rebbeck T, Jakubowska A, Lubinski J, Jaworska K, Durda K, Zlowowcka-Perlowska E, Osorio A, Duran M, Andres R, Benitez J, Hamann U, Hogervorst FB, van Os TA, Verhoef S, Meijers-Heijboer HE, Wijnen J, Gomez Garcia EB, Ligtenberg MJ, Kriege M, Collee JM, Ausems MG, Oosterwijk JC, Peock S, Frost D, Ellis SD, Platte R, Fineberg E, Evans DG, Lalloo F, Jacobs C, Eeles R, Adlard J, Davidson R, Cole T, Cook J, Paterson J, Douglas F, Brewer C, Hodgson S, Morrison PJ, Walker L, Rogers MT, Donaldson A, Dorkins H, Godwin AK, Bove B, Stoppa-Lyonnet D, Houdayer C, Buecher B, de Pauw A, Mazoyer S, Calender A, Leone M, Bressac-de Paillerets B, Caron O, Sobol H, Frenay M, Prieur F, Ferrer SU, Mortemousque I, Buys S, Daly M, Miron A, Terry MU, Hopper JL, John EM, Southey M, Goldgar D, Singer CF, Fink-Retter A, Tea MK, Kaulich DU, Hansen TV, Nielsen FC, Barkardottir RB, Gaudet M, Kirchhoff T, Joseph V, Dutra-Clarke A, Offit K, Piedmonte M, Kirk J, Cohn D, Hurteau J, Byron J, Fiorica J, Toland AE, Montagna M, Oliani C, Imyanitov E, Isaacs C, Tihomirova L, Blanco I, Lazaro C, Teule A, Valle JD, Gayther SA, Odunsi K, Gross J, Karlan BY, Olah E, Teo SH, Ganz PA, Beattie MS, Dorfling CM, van Rensburg EU, Diez O, Kwong A, Schmutzler RK, Wappenschmidt B, Engel C, Meindl A, Ditsch N, Arnold N, Heidemann S, Niederacher D, Preisler-Adams S, Gadzicki D, Varon-Mateeva R, Deissler H, Gehrig A, Sutter C, Kast K, Fiebig B, Schafer D, Caldes T, de la Hoya M, Nevanlinna H, Muranen TA, Lesperance B, Spurdle AB, Neuhausen SL, Ding YC, Wang X, Fredericksen Z, Pankratz VS, Lindor NM, Peterlongo P, Manoukian S, Peissel B, Zaffaroni D, Bonanni B, Bernard L, Dolcetti R, Papi L, Ottini L, Radice P, Greene MH, Loud JT, Andrulis IL, Ozcelik H, Mulligan AU, Glendon G, Thomassen M, Gerdes AM, Jensen UB, Skytte AB, Kruse TA, Chenevix-Trench G, Couch FJ, Simard J, Easton DF (2012) Common variants at 12p11, 12q24, 9p21, 9q31.2 and in ZNF365 are associated with breast cancer risk for BRCA1 and/or BRCA2 mutation carriers. Breast Cancer Res BCR 14(1):R33. doi:10.1186/bcr3121
Catucci I, Verderio P, Pizzamiglio S, Manoukian S, Peissel B, Zaffaroni D, Roversi G, Ripamonti CB, Pasini B, Barile M, Viel A, Giannini G, Papi L, Varesco L, Martayan A, Riboni M, Volorio S, Radice P, Peterlongo P (2011) The CASP8 rs3834129 polymorphism and breast cancer risk in BRCA1 mutation carriers. Breast Cancer Res Treat 125(3):855–860. doi:10.1007/s10549-010-1068-8
Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O, Borg A, Pasini B, Radice P, Manoukian S, Eccles DM, Tang N, Olah E, Anton-Culver H, Warner E, Lubinski J, Gronwald J, Gorski B, Tulinius H, Thorlacius S, Eerola H, Nevanlinna H, Syrjakoski K, Kallioniemi OP, Thompson D, Evans C, Peto J, Lalloo F, Evans DG, Easton DF (2003) Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet 72(5):1117–1130. doi:10.1086/375033
King MC, Marks JH, Mandell JB (2003) Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science 302(5645):643–646. doi:10.1126/science.1088759
Iodice S, Barile M, Rotmensz N, Feroce I, Bonanni B, Radice P, Bernard L, Maisonneuve P, Gandini S (2010) Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis. Eur J Cancer 46(12):2275–2284. doi:10.1016/j.ejca.2010.04.018
Milne RL, Osorio A, Ramon y Cajal T, Baiget M, Lasa A, Diaz-Rubio E, de la Hoya M, Caldes T, Teule A, Lazaro C, Blanco I, Balmana J, Sanchez-Olle G, Vega A, Blanco A, Chirivella I, Esteban Cardenosa E, Duran M, Velasco E, Martinez de Duenas E, Tejada MI, Miramar MD, Calvo MT, Guillen-Ponce C, Salazar R, San Roman C, Urioste M, Benitez J (2010) Parity and the risk of breast and ovarian cancer in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res Treat 119(1):221–232. doi:10.1007/s10549-009-0394-1
Han SA, Park SK, Ahn SH, Lee MH, Noh DY, Kim LS, Noh WC, Jung Y, Kim KS, Kim SW (2011) The Korean Hereditary Breast Cancer (KOHBRA) study: protocols and interim report. Clin Oncol 23(7):434–441. doi:10.1016/j.clon.2010.11.007
Lange K, Weeks D, Boehnke M (1988) Programs for pedigree analysis: MENDEL, FISHER, and dGENE. Genet Epidemiol 5(6):471–472. doi:10.1002/gepi.1370050611
Brohet RM, Velthuizen ME, Hogervorst FB, Meijers-Heijboer HE, Seynaeve C, Collee MJ, Verhoef S, Ausems MG, Hoogerbrugge N, van Asperen CJ, Gomez Garcia E, Menko F, Oosterwijk JC, Devilee P, van’t Veer LJ, van Leeuwen FE, Easton DF, Rookus MA, Antoniou AC (2014) Breast and ovarian cancer risks in a large series of clinically ascertained families with a high proportion of BRCA1 and BRCA2 Dutch founder mutations. J Med Genet 51(2):98–107. doi:10.1136/jmedgenet-2013-101974
Milne RL, Osorio A, Cajal TR, Vega A, Llort G, de la Hoya M, Diez O, Alonso MC, Lazaro C, Blanco I, Sanchez-de-Abajo A, Caldes T, Blanco A, Grana B, Duran M, Velasco E, Chirivella I, Cardenosa EE, Tejada MI, Beristain E, Miramar MD, Calvo MT, Martinez E, Guillen C, Salazar R, San Roman C, Antoniou AC, Urioste M, Benitez J (2008) The average cumulative risks of breast and ovarian cancer for carriers of mutations in BRCA1 and BRCA2 attending genetic counseling units in Spain. Clin Cancer Res 14(9):2861–2869. doi:10.1158/1078-0432.ccr-07-4436
The Korea Central Cancer Registry, National Cancer Center (2012) Annual report of cancer statistics in Korea in 2010, Ministry of Health and Welfare
Park B, Ma SH, Shin A, Chang MC, Choi JY, Kim S, Han W, Noh DY, Ahn SH, Kang D, Yoo KY, Park SK (2013) Korean risk assessment model for breast cancer risk prediction. PLoS One 8(10):e76736. doi:10.1371/journal.pone.0076736
Kang E, Park SK, Yang JJ, Park B, Lee MH, Lee JW, Suh YJ, Lee JE, Kim HA, Oh SJ, Kim SW (2012) Accuracy of BRCA1/2 mutation prediction models in Korean breast cancer patients. Breast Cancer Res Treat 134(3):1189–1197. doi:10.1007/s10549-012-2022-8
Chen S, Parmigiani G (2007) Meta-analysis of BRCA1 and BRCA2 penetrance. J Clin Oncol 25(11):1329–1333. doi:10.1200/jco.2006.09.1066
Theis B, Boyd N, Lockwood G, Tritchler D (1994) Accuracy of family cancer history in breast cancer patients. Eur J Cancer Prev 3(4):321–327
Ziogas A, Anton-Culver H (2003) Validation of family history data in cancer family registries. Am J Prev Med 24(2):190–198
Ewens WJ, Shute NC (1986) A resolution of the ascertainment sampling problem. I. Theory. Theor Popul Biol 30(3):388–412
Carayol J, Khlat M, Maccario J, Bonaiti-Pellie C (2002) Hereditary non-polyposis colorectal cancer: current risks of colorectal cancer largely over estimated. J Med Genet 39(5):335–339
Carayol J, Bonaiti-Pellie C (2004) Estimating penetrance from family data using a retrospective likelihood when ascertainment depends on genotype and age of onset. Genet Epidemiol 27(2):109–117. doi:10.1002/gepi.20007
Acknowledgments
This study was supported by a Grant from the National R&D Program for Cancer Control, Ministry of Health and Welfare, Republic of Korea (#1020350 and #1420190).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Park, B., Dowty, J.G., Ahn, C. et al. Breast cancer risk for Korean women with germline mutations in BRCA1 and BRCA2 . Breast Cancer Res Treat 152, 659–665 (2015). https://doi.org/10.1007/s10549-015-3495-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-015-3495-z