
Abstract
Our study aimed to investigate whether changes in brain function measured with functional magnetic resonance imaging (fMRI) can be detected among individuals with depressive disorders and suicidal ideation. The association between depression severity and brain images is also discussed. Our study recruited 111 participants in three groups: 35 depressive patients with suicidal ideation (SI), 32 depressive patients without suicidal ideation (NS), and 44 healthy controls (HCs). All participants were scanned using 3T MRI to obtain resting-state functional images, and functional connectivity (FC), amplitude of low-frequency fluctuation (ALFF), regional homogeneity (ReHo), and graph theoretical analysis (GTA) were performed. We found functional activity differences, such as the hippocampus and thalamus, in the SI group compared with the NS group. We also concluded lower activity in the thalamus and cuneus regions were related to suicidal ideation. We also found several functional connectivity of the brain areas, such as hippocampus, cuneus, and frontal regions, in the SI group correlated with Hamilton Depression Rating Scale (HAM-D) and Hospital Anxiety and Depression Scale (HADS). A graph theoretical analysis (GTA) and network-based statistical (NBS) analysis revealed different topological organization and slightly better local segregation of the brain network in healthy participants compared with those in depressive patients with suicidal ideation. We suggest that brain functional connectivity may be affected in depressive patients with suicidal ideation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Suicide is an important and serious public health problem worldwide, and its effects are observed throughout all regions, countries, and cultures. In 2012, approximately 800,000 people died from self-inflicted injuries (World-Health-Organization 2014). Suicide is conceptualized as a process or a continuum of ideations/behaviors developing from mild to severe forms of suicidality (Sveticic and De Leo 2012). An international survey in 17 developed and developing countries showed a 9.2% prevalence of lifetime suicidal ideation (Nock et al. 2008). One study in Asia revealed comparable conditional probabilities among ideators to develop a suicide plan (29%) or make a suicide attempt (32%) (Lee et al. 2007). Studies find that within12 months, approximately one third of suicide ideators will go on to attempt suicide (Nock et al. 2013). Around 60% of transitions from suicidal ideation to a first attempt occurring within a year of ideation onset (Nock et al. 2008). Approximately two-thirds (66%) of people who have seriously considered suicide report having a prior psychiatric disorder, most often major depressive disorder (Nock et al. 2009).
Suicide risk evaluation still relies on clinicians’ experiences, and many healthcare practitioners are not familiar with suicide risk assessment. However, patient denial of suicidal ideation can easily become the justification for reduced vigilance, even in persons with a history of suicidal ideation or behavior (Sveticic and De Leo 2012). Consequently, very high rates of suicide among postdischarge patients highlight the limitations of current suicide risk assessments (Isometsa et al. 2014). Monitoring suicidal ideation behavior should not solely be based on self-report (Sveticic and De Leo 2012). Therefore, it is important to create new and objective methods to evaluate the risk of suicide.
Some resting functional MRI studies have been reported in this field. One recent study revealed that female MDD patients with suicidal ideation showed a significant difference in resting-state functional connectivity (rsFC) between the amygdala and precuneus/cuneus compared with those without suicidal ideation and HC group (Wei et al. 2018). Compared with MDD without SI, the SI group showed decreased brain dynamics in the dorsal anterior cingulate cortex, the left orbital frontal cortex, the left inferior temporal gyrus, and the left hippocampus (Li et al. 2019). Suicide ideation links to decreased intrinsic functional connectivity between the rostral anterior cingulate cortex (ACC), the orbitomedial prefrontal cortex and the right middle temporal pole (Du et al. 2017). Low frequency blood oxygenation level-dependent (BOLD) signal in dorsal, ventral posterior cingulate cortex PCC, dorsal ACC was reduced in the ideators (Chase et al. 2017). Another study showed that lower coherence in the left executive control networks were associated with greater lifetime severity of suicidal ideation among adolescent MDD patients (Ordaz et al. 2018). Several functional and structural network-based statistical (NBS) and graph theoretical analyses were performed to assess differences in the inter-regional connectivity (Myung et al. 2016; Li et al. 2018; Weng et al. 2019). The inconsistent findings may due to the different focus study population like adolescent (Ordaz et al. 2018), female (Wei et al. 2018), heterogeneous diagnosed group (Chase et al. 2017) and some of them showed low sample size (Du et al. 2017; Wei et al. 2018). More related studies with higher sample size, homogenous diagnosis and appropriate control are therefore warranted.
The present study aimed to investigate whether MRI-measured functional changes can be detected among individuals with depressive disorders and suicidal ideation, including functional connectivity (FC), amplitude of low-frequency fluctuation (ALFF), regional homogeneity (ReHo), and graph theoretical analysis (GTA). The association between depression severity and brain images is also discussed.
Materials and Methods
Participants
In our study, we recruited three groups of 111 participants: 35 depressive patients with suicidal ideation (SI) (age 21–60 years, mean = 41.11 years, SD 11.78 years), 32 depressive patients without suicidal thoughts (NS) (age 21–60 years, mean = 47.88 years, SD 8.99 years), and 44 healthy controls (HCs) (age 20–58 years, mean = 41.98 years, SD 9.27 years). All participants were at least 20 years of age and right-handed. The confirmation of depressive disorders, suicidal ideation was primarily based on psychiatrists’ diagnosis and the Mini-International Neuropsychiatric Interview (MINI) carried out by the trained research nurse. The assessment of suicide by MINI has been validated before (Roaldset et al. 2012). The final confirmation was carried out by the principle investigator (V.C.H) according to all available information. The participants were recruited via outpatient clinic of department of psychiatry at Chiayi Chang Gung Hospital and recruitment advertisements. Exclusion criteria for all participants were any eye diseases (e.g., cataract and glaucoma), history of suicidal attempt, another primary severe mental disorder (e.g., schizophrenia or bipolar disorder), alcohol/illicit substance use disorder during the past year, any neurological illnesses, and metallic implants or other contraindications for MRI. The study was approved by the Institutional Review Board of Chang Gung Memorial Hospital, Chiayi, Taiwan. (Nos. 104-0838B, 104-9337B, 201602027B0). All participants joined in the study after providing informed consent, and all research was performed in accordance with relevant guidelines and regulations.
The Hamilton Depression Rating Scale (HAM-D) and Hospital Anxiety and Depression Scale (HADS) were used to assess possible anxiety and depression symptoms and carried out by the trained research nurse.
MRI Data Acquisition
All participants were scanned using a 3T MRI (Verio, SIEMENS, Erlangen, Germany) system with a standard 8-channel head coil. A gradient-echo echo planar image (EPI) sequence to obtain resting-state functional images. The phase-encode direction was along anterior-posterior axis. During resting-state MR image acquisition, all participants were instructed not to focus their thoughts on anything in particular and to keep their eyes closed. For all participants, the following sequence was used: repetition time (TR)/echo time (TE) = 2000/30 ms, field of view (FOV) = 220 mm × 220 mm, matrix size = 64 × 64, in-plane resolution (pixel size) = 3.4 × 3.4 mm2, thickness = 4 mm, number of repetitions = 300, scan time for functional imaging = 10 min, and 31 axial slices aligned along AC-PC lines without gap to cover the whole cerebrum. The research nurse confirmed the persistence of suicide ideation on the date of MRI examination.
Functional Image Preprocessing
We used statistical parametric mapping 8 (SPM8, Wellcome Department of Cognitive Neurology, London, UK) software to conduct preprocessing of functional images. After slice-timing correction, we calculated the center of each image and realigned the data to the first volume for motion correction. After motion correction, data were normalized to standard Montreal Neurological Institute (MNI) space with affine transformation, and the data were resampled to isotropic 3-mm voxels. The data were then spatially smoothed using a 6-mm full-width at half-maximum (FWHM) Gaussian kernel for a better signal-to-noise ratio gain. Then, using the six head motion parameters as covariates, we performed nuisance regression. Then, the whole brain, WM, and CSF masks were used to remove the physiological noise. Linear detrending and band-pass temporal filtering were performed on the time series of each voxel to minimize the effects of low-frequency drifts and physiological signals by the Resting-State Data Analysis tool kit v1.8 (REST v1.8, Center for Cognition and Brain Disorders, Hangzhou Normal University, Zhejiang, China). We used the frequency range from 0.01 to 0.12 Hz to observe the complex functional networks and mitigate the influence of low-frequency drift and high-frequency physiological noise (Baria et al. 2011).
Functional Connectivity (FC) and Seed‐Based Correlation Analysis (SCA)
As spontaneous, coherent, and low-frequency fluctuations of the BOLD signal were used for the resting-state analysis, the BOLD time series for each participant was extracted and band-pass filtered (0.01–0.12 Hz). Correlating the averaged BOLD signal of the user-defined region of interest to the BOLD signal of every other single voxel for each participant formed correlation maps at the voxel level. The SCA analysis locates the seed on the selected spherical ROI coordinates and observes the activation of the contralateral brain region when the brain region is activated, that is, the functional connectivity between the brain regions on both sides. We selected brain regions associated with depression, including the amygdala, hippocampus, thalamus, visual cortex, motor cortex, posterior cingulate cortex (PCC), anterior cingulate cortex (ACC), and precuneus. To enforce a Gaussian distribution of the correlation data, Pearson’s r was then transformed into z scores using Fisher’s r to z transformation.
Amplitude of Low‐Frequency Fluctuations (ALFFs)
Amplitude low-frequency fluctuations is used to report the absolute intensity of spontaneous brain activity. The ALFF during the resting-state is considered to be physiologically meaningful and to reflect spontaneous neural activity (Zang et al. 2007; Zou et al. 2008). The ALFFs were calculated in the frequency range of 0.01 to 0.12 Hz. The procedure for calculating ALFFs is briefly described as follows: for a given voxel, the time series is first converted to the frequency domain using a fast Fourier transformation. The square root of the power spectrum is computed, averaged, and normalized across a predefined frequency interval, which is termed the ALFF at the given voxel (Yue et al. 2015). The mean fractional ALFF (mfALFF) can be regarded as a normalized mean ALFF and is calculated using the total energy over the detectable frequency range. The mfALFF can provide a more specific measure of low-frequency oscillatory phenomena than the mALFF (Zou et al. 2008). In voxel-based analysis (VBA), we assessed the differences in mfALFFs between the SI, NS and healthy control groups using false discovery rate (FDR)-corrected two-sample t-tests. In the study, depression (depression score that does not include suicidality), anxiety indices, age, gender and years of education were used as the covariates to eliminate the effect caused by differences between each group. We also probed the relationship between the SI participants’ mfALFF and Hamilton depression rating scale (HAM-D)/ Hospital Anxiety and Depression Scale (HADS) scores using multiple regressions with FDR correction. In the study, age, gender and years of education were used as the covariates. We used a T1-weighted MNI template to create the underlying map to view the results.
Regional Homogeneity (ReHo)
Regional homogeneity is based on the concept that BOLD signal fluctuations in a specific region reflect near neuronal activity arising at the same frequency and that this temporal synchrony is confined to groups of neurons that perform related functions (Zang et al. 2004). To analyze the ReHo, linear detrending and band-pass filtering (0.01–0.12 Hz) were performed on the time series of each voxel by REST v1.8. The resting state cortical activity in the SI, the NS and the healthy control groups was evaluated with the ReHo approach. Each individual ReHo map was generated by calculating Kendall’s coefficient of concordance (KCC), which computes the ReHo of the BOLD time series data in each voxel and its 26 nearest adjacent voxels (Zang et al. 2004). Then, a mask was used to remove nonbrain tissues and noise on the ReHo maps, and the individual ReHo maps were divided by their own mean KCC within the mask for standardization purposes to compute the mean ReHo (mReHo). We conducted a whole-brain voxel-wise comparison using FDR-corrected two-sample t-tests to evaluate group differences in mReHo between the SI, the NS and the healthy control groups. In the study, depression (depression score that does not include suicidality), anxiety indices, age, gender and years of education were used as the covariates to eliminate the effect caused by differences between each group. We also assessed the relationship between the SI participants’ mReHo and the HAM-D/ HADS scores using multiple regressions with FDR correction. Age, gender and years of education were used as the covariates. To view the results, we used a T1-weighted MNI template to create the underlying map.
Graph Theoretical Analysis (GTA)
Using the functional connectivity toolbox (CONN, The Gabrieli Lab, McGovern Institute for Brain Research, MIT, Cambridge, MA, USA), the whole brain was divided into 90 regions of interest (ROIs) (45 per hemisphere) with an automated anatomical labeling (AAL) template, each of which was considered a node (Behzadi et al. 2007; Whitfield-Gabrieli and Nieto-Castanon 2012). The edge represented the brain’s functional connectivity between two nodes. The degree of a node was the number of edges connecting it to the rest of the network, which allowed characterization of the edge distributions of all nodes in the network (Bullmore and Bassett 2011).
The resting-state functional image was registered to the T1-weighted image and then to the MNI space. The transformation matrix from the resting space to MNI space was calculated by the transformation matrices created in the two aforementioned register processing steps and was stored for later use. We spatially normalized the resting-state functional images to the AAL template in MNI native space, and the connectivity matrix was obtained after functional connectivity analysis. The functional connectivity matrix was acquired from the functional connectivity toolbox (CONN). Finally, we perform a graph theoretical analysis by using the connectivity matrix.
Analyses of network properties were performed using the Graph Analysis Toolbox (GAT, Stanford University School of Medicine, Stanford, CA, USA) (Hosseini et al. 2012). The GAT was used to extract the functional connectivity between each of the 90 ROIs from the 90 × 90 connectivity matrix for each individual. A histogram was used to represent the degree distribution of the 90 nodes in both groups. Next, the networks of the two groups were created at different correlation thresholds, ranging from 0.2 to 0.5 in 0.01 increments. After examining all the networks, the minimum network density at which no individual network was fragmented was identified as 0.2 (Hosseini et al. 2012). Graph theoretical analysis was then conducted to investigate the systematic alteration of the whole-brain functional topological organization, including the clustering coefficient (C), normalized clustering coefficient (γ), characteristic path length (L), normalized characteristic path length (λ), local efficiency, global efficiency, transitivity, assortativity and small-worldness index (σ). To test for the statistical significance of the between-group differences in network topology and regional network measures, we manually extracted the area under the curve between 0.2 and 0.5 of the density to calculate the p value of the two-sample t-test.
Network‐Based Statistical (NBS) Analysis
We used network-based statistical (NBS, Melbourne Neuropsychiatry Centre, The University of Melbourne and Melbourne Health, Australia) analysis to identify the significance of any connected subnetworks evident in the set of altered connections found in healthy controls and depressive patients with and without suicidal ideation. NBS analysis attempts to identify any potentially connected structures formed by an appropriately chosen set of suprathreshold links. The topological extent of any such structure is then used to determine its significance. The test statistical (i.e., primary threshold) computed for each pairwise association is used to construct a set of suprathreshold links (Zalesky et al. 2010). The null distribution of the number of edges was empirically obtained using nonparametric permutation (5,000 permutations) to assess the significance of each of the connected edges.
Results
Participants
Table 1 shows demographic characteristics. There were significant differences in age, gender, and years of education among the three groups. Therefore, age, gender, and years of education were used as covariates for subsequent analyses.
FC and SCA
In the FC analysis between the SI and the NS groups, we found higher FC in the right hippocampus (Fig. 1a) and the left hippocampus (Fig. 1b) in the SI group compared with the NS group. In the FC analysis between the NS and the HC groups, we found lower FC of the right thalamus (Fig. 1c), the left thalamus (Fig. 1d), the right motor cortex (Fig. 1e), and the left motor cortex (Fig. 1f) in the NS group compared with the HC group (all corrected p < 0.05).

Higher FC of the a right hippocampus and b left hippocampus was found in the SI group compared with the NS group. Lower FC of the c right thalamus, d left thalamus, e right motor cortex, and f left motor cortex was found in the NS group compared with the HC group
VBA of mfALFF and mReHo
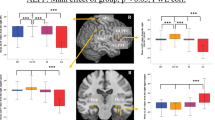
In the VBA of mfALFF between the SI and the NS groups (Fig. 2a, NS > SI), we found lower mfALFF activation of the left cuneus in the SI group compared with the NS group (Fig. 2b) and higher mfALFF activation of the right middle temporal pole gyrus (Fig. 2c) in the SI group compared with the NS group. In the VBA of mReHo between the SI and the NS groups (Fig. 2d, NS > SI), we found lower regional homogeneity of the right cuneus in the SI group compared with the NS group (Fig. 2e). We also found higher regional homogeneity of the left middle temporal gyrus (MTG) (Fig. 2f) in the SI group compared with the NS group (all corrected p < 0.05).

a Two-sample t-test results of mfALFF between the SI and the NS groups (NS > SI, color bar represents t-score). b Lower mfALFF of the left cuneus and c higher mfALFF of the right middle temporal pole gyrus were found in the SI group compared with the NS group. d Two-sample t-test results of mReHo between the SI and the NS groups (NS > SI; color bar represents t-score). e Lower mReHo of the right cuneus and f higher mReHo of the left middle temporal gyrus (MTG) were found in the SI group compared with the NS group
Association Between HAM-D, Anxiety Scores, and Depression Scores and mfALFF/mReHo
In the SI participants’ multiple regression analysis (Fig. 3) of the correlation between HAM-D and mfALFF, a positive correlation in the left cuneus gyrus (Fig. 3a) was found, and a negative correlation in the right hippocampus, superior temporal pole gyrus, and parahippocampal gyrus (Fig. 3b) was found. A positive correlation between HAM-D and mReHo in the right cuneus gyrus (Fig. 3c) was found. A positive correlation between anxiety score and mReHo in the left postcentral gyrus (Fig. 3d) was found. A positive correlation between anxiety score and mReHo in the left inferior and middle frontal gyrus (Fig. 3e) was found, and a negative correlation in the right lingual gyrus (Fig. 3f) was found. A positive correlation between depression score and mfALFF in the right postcentral gyrus (Fig. 3g) and left cuneus gyrus (Fig. 3h) was found. A positive correlation between depression score and mReHo in the right cuneus gyrus (Fig. 3i) was found (all corrected p < 0.05).

The correlation with suicidal ideation. a Positive correlation between HAM-D and mfALFF in the left cuneus gyrus. b Negative correlation between HAM-D and mfALFF in the right hippocampus, superior temporal pole gyrus, and parahippocampal gyrus. c Positive correlation between HAM-D and mReHo in the right cuneus gyrus. d Positive correlation between anxiety score and mReHo in the left postcentral gyrus. e Positive correlation between anxiety score and mReHo in the left inferior and middle temporal gyrus. f Negative correlation between anxiety score and mReHo in right lingual gyrus. g Positive correlation between depression score and mfALFF in the right postcentral gyrus. h Positive correlation between depression score and mfALFF in the left cuneus gyrus. i Positive correlation between depression score and mReHo in the right cuneus gyrus
GTA
In the GTA of the three groups, we found a significant tendency (NS > SI > HC) in the global efficiency (Fig. 4a, corrected p < 0.05). However, no significant tendency was found in assortativity (Fig. 4b), transitivity (Fig. 4c), and small-worldness index (σ) (Fig. 4d). Although all participants maintained a small-worldness functional brain network according to the σ calculation, the network was more like a random network in the SI group.

The topological parameters, including a global efficiency, b assortativity, c transitivity, and d small-worldness (σ) among the three groups, i.e., the SI, NS and HC groups.
NBS Analysis
For the NBS analysis, we compared the edges of the brain networks between the NS and SI groups. One subnetwork showed more edges in the NS group compared with the SI group (Fig. 5, p < 0.05), including connections from the orbital frontal gyrus to the right precentral gyrus, bilateral posterior cingulate cortex, left parahippocampal gyrus, right inferior frontal operculum gyrus, and left precuneus gyrus; from the left rectus to the right precentral gyrus, left postcentral gyrus, left superior parietal gyrus, and left inferior parietal gyrus; from the right middle occipital gyrus to the left parahippocampal gyrus and left superior parietal gyrus. We also compared the edges of the brain networks between the NS and HC groups, however no significant result were found.

The NBS analysis results. A disrupted subnetwork was found in the SI group compared with the NS group (NS > SI)
Discussion
Our results demonstrated that widespread and disrupted network changes in brain functional networks and their interconnectivity was associated in depressive patients with suicidal ideation. Our results suggest that the neural basis underlying the psychopathology in depressive patients with suicidal ideation involves multiple brain functional networks and their interaction, which is consistent with one recent review (Schmaal et al. 2020).
Our results showed an increase in functional connectivity between both sides of the hippocampus in the SI group. The activation of the bilateral hippocampus in the SI group was greater than that in the NS group. The finding was consistent with that from an fMRI study revealing recall of suicide action was associated with increased activity in the hippocampus (Reisch et al. 2010). In a previous DTI study, the white matter fibers in the hippocampus of the SI group had larger RDs than those in the NS and HC groups, and the FA value was smaller than those of the NS and HC groups (Taylor 2015). This result indicated a reduced integrity of white matter fibers in the SI group. Taken together, these findings of the low integrity of white matter of hippocampus may represent the weak and vulnerable state of brain to suicide ideation while hyperactivity of hippocampus may represent the compensation response to suicide ideation. Further studies combing structural and function MRI to explore this concept are warranted.
In our FC analysis between the NS and the HC groups, we found lower FC of the bilateral thalamus in the NS group compared with the HC group. In a previous DTI study, the RD values of the anterior thalamic radiation of the SI group were greater than those of the NS and HC groups, and the FA value was smaller than those of the NS and HC groups, representing the reduced integrity of white matter fibers in the SI group (Taylor 2015). Our results showed decreased functional connectivity between the thalamus in the SI and NS groups, which was consistent with the DTI study. In a previous study using NBS analysis, it was found that the number of connections between the brain regions of the NS group was larger than that of the SI group, including the left superior frontal gyrus and the bilateral thalamus (Kim et al. 2017), and the decrease in brain activity may indirectly lead to a reduction in the number of connections between networks. Thalamus has been involved in executive functions (such as planning, cognitive control, working memory, and decision-making) (Ouhaz et al. 2018) and executive function deficits is associated with suicidality (Bredemeier and Miller 2015).
In the voxel-based analysis results between the SI and NS groups, we found that the mfALFF of the left cuneus in the SI group was smaller than that in the NS group, and the right middle temporal pole gyrus was larger than that in the NS group. We also found that the mReHo of the right cuneus in the SI group was smaller than that in the NS group, and the left middle temporal gyrus was larger than that in the NS group. A previous study noted that the functional connectivity between the amygdala and precuneus/cuneus on both sides in the SI group was greater than those of the NS group and the HC group (Wei et al. 2018), and our results showed that the cuneus of the SI group had decreased activity. This may result in an increase in the functional connectivity between the amygdala and precuneus/cuneus to maintain functional integrity. A recent study found that the intrinsic functional connectivity of the right middle temporal pole gyrus was positively correlated with the severity of suicidal ideation, indicating that the stronger the degree of suicidal ideation is, the higher the intrinsic functional connectivity of the right middle temporal pole gyrus is (Du et al. 2017).
The affective network includes the amygdala, orbitofrontal cortex, temporal cortex, pallidum, and insular cortex. Crucially, the affective network has been associated with processing and regulation of emotions. Emerging neuroimaging findings suggest an involvement of the affective network in the pathophysiology of depression (Li et al. 2018). The insula is a component of the salience network and through connections with the amygdala and cingulate cortex may potentiate the neural response to negative stimuli. The pulvinar nucleus of the thalamus is also involved in this network, and observations of disruption in the internal capsule and thalamic radiations further support this network may be disrupted in individuals with suicidal ideation (Hamilton 2012). The default mode network (DMN) mainly encompasses the precuneus, posterior cingulate cortex, medial prefrontal cortex, and the inferior parietal cortex. This network is known as a task-negative network as regions within this network generally demonstrate deactivation during performance of cognitive tasks. Enhanced DMN connectivity is marked in depression (Li et al. 2018). Our data and previous study provided important clues about neural circuits involvement in suicidal ideation. In a previous study, the activation of the DMN was negatively correlated with the severity of suicidal ideation (Ordaz et al. 2018), which means that when suicidal ideation is more serious, the activation of the DMN brain region is reduced. It has been suggested that this network may be important in the excessive negative and blunted positive internal states that can stimulate suicide ideation (Schmaal et al. 2020).
In a multiple regression analysis, the association between the mfALFF and mReHo images of suicidal ideation depressive patients and depression-related scales, including the HAM-D and the anxiety score and depression score of HADS was performed. An imaged brain area positively associated with the scale indicates a higher representative scale score and higher activity of the brain area (SI > HC); an imaged brain area negatively associated with the scale indicates a lower the score of the representative scale and higher activity of the brain area (HC > SI). First, regarding the correlation between mfALFF and HAM-D, we found that the left cuneus of SI was positively correlated with HAM-D, and the right hippocampus, right superior temporal pole gyrus and right parahippocampal gyrus were negatively correlated with HAM-D. Regarding the correlation between mReHo and HAM-D, we found that the right cuneus of SI was positively correlated with HAM-D. A previous study noted that the functional connectivity between the amygdala and precuneus/cuneus on both sides of the SI group were greater than those in the NS and HC groups (Wei et al. 2018), and the result was similar to our results. More depressed patients have higher activity of cuneus. A previous study mentioned that the activation of DMN was negatively correlated with the severity of suicidal ideation (Ordaz et al. 2018), indicating that a stronger degree of suicidal ideation was associated with lower activation of the brain region of the DMN, medial prefrontal cortex, posterior cingulate cortex and hippocampus, consistent with our results.
Regarding the correlation between mReHo and anxiety score, we found that the left postcentral gyrus, left inferior temporal gyrus and left middle temporal gyrus in the SI group were positively correlated with the anxiety score, and the right lingual gyrus was negatively correlated with the anxiety score. This means that higher patient anxiety was associated with higher regional homogeneity around the brain regions of the left postcentral gyrus, left inferior temporal gyrus and left middle temporal gyrus. Lower patient anxiety was associated with lower regional homogeneity of the brain around the right lingual gyrus. In the correlation between the mfALFF and depression score, we found that right postcentral gyrus and left cuneus in SI were positively correlated with the depression score. In the correlation between mReHo and depression score, we found that the right cuneus gyrus in SI was positively correlated with the depression score. This means that when the patient has a higher degree of depression, the activity of the brain area is also higher. A previous study mentioned the functional connectivity between the amygdala and precuneus/cuneus on both sides of the SI group was greater than those in the NS and HC groups (Wei et al. 2018), which was similar to our experimental results.
In the graph theory analysis, we found that the global efficiency of HC was significant less than that of the NS group. Although the other topological parameters were not significant, there was still a trend. We found larger global efficiency and lower assortativity, transitivity in the SI group compared with HC group. The small-worldness is used to describe the state of the brain network connection with a value between 0and1. Although our results showed all participants maintained a small-worldness functional brain network according to the σ calculation, the network was more like a random network in the SI group.
Regarding the NBS analysis results, we found that the number of connections between brain regions in the NS group was larger than that of the SI group. In a previous study using NBS analysis (Myung et al. 2016), it was found that the number of connections between brain regions of the NS group was larger than that of the SI group, similar to our results, and similar brain regions were found, including the left middle orbitofrontal gyrus, right middle occipital gyrus and left superior parietal gyrus.
It is noteworthy to mention the limitation for the unmeasured characteristics of healthy control like obesity, gambling, internet addiction, ADHD etc. These characteristics links to reward deficiency syndrome (RDS) and a hypodopaminergic trait (Blum et al. 2000). It has been suggested that DA-related genetic variants including catechol-O-methyltransferase (COMT), DA D2 receptor (DRD2), and DA transporter gene (DAT) are related to depression while reward network mediates the relationship between the dopamine genetic profile and depression (Gong et al. 2017). The small sample sizes and unbalanced age and sex of case and control subjects create limitations on the study findings. While the sizes of groups are small thus reducing power and overall stability of findings, we added FDR adjustment and co-varying age and sex in the analysis for meeting the current standard. Further studies are warranted to include larger sample size of age- and sex-matching depressive patients with suicidal ideation to explore the association between different level of severity of suicidal ideation and brain image, such as level of suicide intent or lethality of suicide methods. The confirmation suicidal ideation was primarily based on psychiatrists’ diagnosis and the Mini-International Neuropsychiatric Interview (MINI) carried out by the trained research nurse. Although the information still came from patients, since the assessment was based on the volunteer participants’ understanding for the research goal to create the objective tool to detect suicide ideation rather than real world practice, the participants were less likely to deny the suicide ideation.
Conclusions
We found functional activity differences, such as the hippocampus and thalamus, in the SI group compared with the NS group. We also concluded lower activity in the thalamus and cuneus regions were related to suicidal ideation. We also found several connectivity of the brain areas, such as hippocampus, cuneus, and frontal regions, in the SI group correlated with severity of anxiety and depression. GTA and NBS analysis revealed different topological organization and slightly better local segregation of the brain network in healthy participants compared with those in depressive patients with suicidal ideation. We concluded that the brain function of depressive disorders with suicidal ideation was different than that in depressive disorders without suicidal ideation and in healthy participants. The findings from present study can serve as the basis for further algorithm studies by machine learning method to stratify the risk population.
References
Baria AT, Baliki MN, Parrish T, Apkarian AV (2011) Anatomical and functional assemblies of brain BOLD oscillations. J Neurosci 31(21):7910–7919
Behzadi Y, Restom K, Liau J, Liu TT (2007) A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage 37(1):90–101
Blum K, Braverman ER, Holder JM, Lubar JF, Monastra VJ, Miller D, Lubar JO, Chen TJ, Comings DE (2000) Reward deficiency syndrome: a biogenetic model for the diagnosis and treatment of impulsive, addictive, and compulsive behaviors. J Psychoact Drugs 32(Suppl 1):1–112
Bredemeier K, Miller IW (2015) Executive function and suicidality: a systematic qualitative review. Clin Psychol Rev 40:170–183
Bullmore ET, Bassett DS (2011) Brain graphs: graphical models of the human brain connectome. Annu Rev Clin Psychol 7:113–140
Chase HW, Segreti AM, Keller TA, Cherkassky VL, Just MA, Pan LA, Brent DA (2017) Alterations of functional connectivity and intrinsic activity within the cingulate cortex of suicidal ideators. J Affect Disord 212:78–85
Du L, Zeng J, Liu H, Tang D, Meng H, Li Y, Fu Y (2017) Fronto-limbic disconnection in depressed patients with suicidal ideation: a resting-state functional connectivity study. J Affect Disord 215:213–217
Gong L, He C, Yin Y, Wang H, Ye Q, Bai F, Yuan Y, Zhang H, Lv L, Zhang H, Zhang Z, Xie C (2017) Mediating role of the reward network in the relationship between the dopamine multilocus genetic profile and depression. Front Mol Neurosci 10:292
Hamilton E (2012) Functional neuroimaging of major depressive disorder a meta-analysis and new integration of base line activation and neural response data. Am J Psychiatry 169(7):693–703
Hosseini SM, Hoeft F, Kesler SR (2012) GAT: a graph-theoretical analysis toolbox for analyzing between-group differences in large-scale structural and functional brain networks. PLoS ONE 7(7):e40709
Isometsa E, Sund R, Pirkola S (2014) Post-discharge suicides of inpatients with bipolar disorder in Finland. Bipolar Disord 16(8):867–874
Kim K, Kim SW, Myung W, Han CE, Fava M, Mischoulon D, Papakostas GI, Seo SW, Cho H, Seong JK, Jeon HJ (2017) Reduced orbitofrontal-thalamic functional connectivity related to suicidal ideation in patients with major depressive disorder. Sci Rep 7(1):15772
Lee S, Tsang A, Zhang MY, Huang YQ, He YL, Liu ZR, Shen YC, Kessler RC (2007) Lifetime prevalence and inter-cohort variation in DSM-IV disorders in metropolitan China. Psychol Med 37(1):61–71
Li BJ, Friston K, Mody M, Wang HN, Lu HB, Hu DW (2018) A brain network model for depression: from symptom understanding to disease intervention. CNS Neurosci Ther 24(11):1004–1019
Li J, Duan X, Cui Q, Chen H, Liao W (2019) More than just statics: temporal dynamics of intrinsic brain activity predicts the suicidal ideation in depressed patients. Psychol Med 49(5):852–860
Myung W, Han CE, Fava M, Mischoulon D, Papakostas GI, Heo JY, Kim KW, Kim ST, Kim DJ, Kim DK, Seo SW, Seong JK, Jeon HJ (2016) Reduced frontal-subcortical white matter connectivity in association with suicidal ideation in major depressive disorder. Transl Psychiatry 6(6):e835
Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, Beautrais A, Bruffaerts R, Chiu WT, de Girolamo G, Gluzman S, de Graaf R, Gureje O, Haro JM, Huang Y, Karam E, Kessler RC, Lepine JP, Levinson D, Medina-Mora ME, Ono Y, Posada-Villa J, Williams D (2008) Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry 192(2):98–105
Nock MK, Hwang I, Sampson N, Kessler RC, Angermeyer M, Beautrais A, Borges G, Bromet E, Bruffaerts R, de Girolamo G, de Graaf R, Florescu S, Gureje O, Haro JM, Hu C, Huang Y, Karam EG, Kawakami N, Kovess V, Levinson D, Posada-Villa J, Sagar R, Tomov T, Viana MC, Williams DR (2009) Cross-national analysis of the associations among mental disorders and suicidal behavior: findings from the WHO World Mental Health Surveys. PLoS Med 6(8):e1000123
Nock MK, Green JG, Hwang I, McLaughlin KA, Sampson NA, Zaslavsky AM, Kessler RC (2013) Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry 70(3):300–310
Ordaz SJ, Goyer MS, Ho TC, Singh MK, Gotlib IH (2018) Network basis of suicidal ideation in depressed adolescents. J Affect Disord 226:92–99
Ouhaz Z, Fleming H, Mitchell AS (2018) Cognitive functions and neurodevelopmental disorders involving the prefrontal cortex and mediodorsal thalamus. Front Neurosci 12:33
Reisch T, Seifritz E, Esposito F, Wiest R, Valach L, Michel K (2010) An fMRI study on mental pain and suicidal behavior. J Affect Disord 126(1–2):321–325
Roaldset JO, Linaker OM, Bjørkly S (2012) Predictive validity of the MINI suicidal scale for self-harm in acute psychiatry: a prospective study of the first year after discharge. Arch Suicide Res 16(4):287–302
Schmaal L, van Harmelen AL, Chatzi V, Lippard ETC, Toenders YJ, Averill LA, Mazure CM, Blumberg HP (2020) Imaging suicidal thoughts and behaviors: a comprehensive review of 2 decades of neuroimaging studies. Mol Psychiatry 25(2):408–427
Sveticic J, De Leo D (2012) The hypothesis of a continuum in suicidality: a discussion on its validity and practical implications. Ment Illn 4(2):e15
Taylor WD, Boyd B, McQuoid DR, Kudra K, Saleh A, MacFall JR (2015) Widespread white matter but focal gray matter alterations in depressed individuals with thoughts of death. Prog Neuropsychopharmacol Biol Psychiatry 62:22
Wei S, Chang M, Zhang R, Jiang X, Wang F, Tang Y (2018) Amygdala functional connectivity in female patients with major depressive disorder with and without suicidal ideation. Ann Gen Psychiatry 17:37
Weng JC, Chou YS, Tsai YH, Lee CT, Hsieh MH, Chen VC (2019) Connectome analysis of brain functional network alterations in depressive patients with suicidal attempt. J Clin Med 8(11):1966
Whitfield-Gabrieli S, Nieto-Castanon A (2012) Conn: a functional connectivity toolbox for correlated and anticorrelated brain networks. Brain Connect 2(3):125–141
World-Health-Organization (2014) Preventing suicide: a global imperative. World-Health-Organization, Geneva
Yue Y, Jia X, Hou Z, Zang Y, Yuan Y (2015) Frequency-dependent amplitude alterations of resting-state spontaneous fluctuations in late-onset depression. Biomed Res Int 2015:505479
Zalesky A, Fornito A, Bullmore ET (2010) Network-based statistic: identifying differences in brain networks. Neuroimage 53(4):1197–1207
Zang Y, Jiang T, Lu Y, He Y, Tian L (2004) Regional homogeneity approach to fMRI data analysis. Neuroimage 22(1):394–400
Zang YF, He Y, Zhu CZ, Cao QJ, Sui MQ, Liang M, Tian LX, Jiang TZ, Wang YF (2007) Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev 29(2):83–91
Zou QH, Zhu CZ, Yang Y, Zuo XN, Long XY, Cao QJ, Wang YF, Zang YF (2008) An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. J Neurosci Methods 172(1):137–141
Acknowledgements
This study was supported by the research programs MOST105-2314-B-182-028, MOST106-2314-B-182-040-MY3, and MOST109-2314-B-182-047-MY3, which were sponsored by the Ministry of Science and Technology, Taipei, Taiwan. The funders had no role in the conduct of the study nor the collection, analysis, and interpretation of data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Additional information
Handling Editor: Armida Mucci.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chen, V.CH., Chou, YS., Tsai, YH. et al. Resting‐State Functional Connectivity and Brain Network Abnormalities in Depressive Patients with Suicidal Ideation. Brain Topogr 34, 234–244 (2021). https://doi.org/10.1007/s10548-020-00817-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10548-020-00817-x