
Abstract
Mesenchymal stem cells (MSCs), a class of adult stem cells, are considered a promising source for bone regeneration. Although combining MSCs with biomaterial scaffolds offers an interesting clinical strategy for bone tissue engineering, the presence of the scaffolds could induce an undesirable effect on cell–cell interactions. Moreover, before the application of scaffold materials in bone tissue reconstruction, cells must be manipulated with proteolytic enzymes, such as trypsin or dispase that degrade extracellular matrix (ECM) molecules and cell surface proteins, which can result in the cell damage and loss of cellular activity. Therefore, the development of alternative strategies for bone regeneration is required to solve these problems. Recently, a novel tissue engineering technology named ‘cell sheet’ has been efficaciously utilized in the regeneration of bone, corneal, cardiac, tracheal and periodontal ligament-like tissues. The cell sheet is a layer of cells, which contains intact ECM and cell surface proteins such as growth factor receptors, ion channels and cell-to-cell junction proteins. MSC sheets can be easily fabricated by layering the recovered cell sheets without any scaffolds or complicated manipulation. This review summarizes the current state of the literature regarding the use of MSCs to produce cell sheets and assesses their applicability in bone tissue regeneration and repair.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tissue engineering approaches for bone regeneration by seeding cells into a scaffold have recently produced promising clinical results (Gao et al. 2009). As a consequence, the use of scaffolds in combination with osteogenic cells has become the gold standard in bone tissue engineering strategies (Pirraco et al. 2011). However, the usual method of tissue engineering involving the injection of isolated cell suspensions or the seeding of cells into biodegradable scaffolds may present some complications such as the cell loss, small quantities of seeded cells and inflammatory reactions with degradation of the scaffolds (Chen et al. 2016). In addition, this method has failed to produce the required results due to cell necrosis at the bulk of the scaffold related to nutrients diffusion and deficient oxygen (Pirraco et al. 2011). To overcome these limitations, the scaffold-free approach may be a suitable alternative to scaffold-based tissue engineering (Ma et al. 2010; Yorukoglu et al. 2017). In 2004, Nishida et al. established an innovative technique called ‘cell sheet’, in which cells were harvested together with endogenous extracellular matrix (ECM) and intact cell–cell contacts (Nishida et al. 2004). Cell sheet technology offers useful advantages with respect to cell suspension seeding strategy for bone tissue engineering. Most importantly, cell sheet and deposited ECM can be attached to host tissues with minimal loss of cells (Gao et al. 2009). To be specific, these cell sheets were formed from hyperconfluent cells until they produce extensive cell-to-cell interactions and synthesize a great quantity of ECM (Yorukoglu et al. 2017). In the last few years, cell sheets of mesenchymal stem cells (MSCs) have been widely utilized for the regeneration of many tissues and organs including bone, meniscus, cartilage, tendons, tooth, periodontal tissue and skin (see Table 1 for references). Moreover, MSC sheets have been also used for the regeneration of cornea (Gomes et al. 2010), cardiac tissue (Miyahara et al. 2006; Wang et al. 2007; Zhang et al. 2010; Huang et al. 2013; Haraguchi et al. 2014; Tano et al. 2014; Chang et al. 2015; Kawamura et al. 2015; Tanaka et al. 2016), nasal epithelium (Kavuzlu et al. 2017), blood vessels (Zhao et al. 2012), wound healing (McLaughlin and Marra 2013), digestive fistula (Rahmi et al. 2016), oral ulcers (Lee et al. 2017) and spinal cord defects (See et al. 2011; Okuda et al. 2017) (Table 1).
Cell sheets are thin films of about 80–150 μm thickness that can be generated in 2 weeks of In vitro culture using MSCs, as observed for example, using human PDL stem cells (PDLSCs) and human jaw bone mesenchymal stem cells (JBMSC) (Chen et al. 2007; Wang et al. 2016b).
Importantly, cell sheets contain a large amount of ECM proteins and cell-to-cell junctions, and therefore can be transplanted directly to tissue without the use of additional scaffolds (Iwata et al. 2015). This methodology preserves cell–cell interactions and the structure of ECM due to the fact that enzymatic digestion of the cells is not needed before application (Gao et al. 2009; Nakamura et al. 2010). The cell sheet consists in different layers of cells (usually 4–5) with approximately 80–150 μm thickness embedded in its self-secreted-ECM (Xie et al. 2015), in which cells maintain intact cell surface proteins such as cell–cell junctions, adhesion molecules, growth factor receptors and ion channels. The best characteristic of cell sheets is that the intact ECM at the bottom of the sheet permits direct adhesion of the sheet to the target organ. Therefore, the transplantation of the cell sheet does not require suturing, because it is obtained by the adhesion of the ECM at the bottom of the sheet to the target organ (Oka et al. 2018). More importantly, it is demonstrated that cell sheets transplanted remain at the transplant site for an extended period of time, with a higher graft survival rate with respect to that obtained with cell transplantation using isolated cell injections (Sekine et al. 2011; Oka et al. 2018). Therefore, due to the fact that ECM is present on the basal surface of the cell sheets, they can be easily transplanted directly to tissue beds or even overlapped, generating three-dimensional tissue-like structures (Chen et al. 2015).
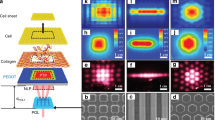
Cell sheets can be generated by culturing MSCs at high confluence on dishes coated with a thermo-responsive polymer (Kwon et al. 2000; Long et al. 2014; Shang et al. 2017). At 37 °C, the dish surface is slightly hydrophobic and therefore cells can adhere to the dish and proliferate. When the temperature is lowered to 20 °C, the hydrophobic surface of the dishes reversibly changes to hydrophilic, determining the gradual detachment of a sheet of cells from the culture surface (Fig. 1) (Kwon et al. 2000; Long et al. 2014; Shang et al. 2017). These temperature-responsive culture surfaces possess several advantages with respect to the enzymatic harvesting of cells from culture dishes because the ECM components, cell-to-cell connections and adhesive proteins were conserved by this method. As a consequence, cell sheets could offer unique features that retain the microenvironment of the cells by avoiding enzymatic treatment and retaining cell–cell junctions and their deposited ECM (Nakamura et al. 2010).

Schematic representation of cell sheets formation
Importantly, it has been shown that the formation of MSC sheets can be also obtained by using other methods such as pH change-, magnetism-, electricity- and light-induced methods (Jiang et al. 2017; Yorukoglu et al. 2017). For example, Guillaume-Gentil et al. have shown that electro-chemically-induced pH lowering at the bio-interface is able to instigate cell sheet detachment by using poly(allylamine hydrochloride) and anionic poly(styrene sulfonate) polyelectrolytes (PAH/PSS) multilayer thin films as substrates for MSCs culture (Guillaume-Gentil et al. 2011). The advantages of this method are that recovered MSC sheets remain viable and maintain their differentiation capacity, whereas a disadvantage is that it requires cell cultures compatible with PAH/PSS substrates (Guillaume-Gentil et al. 2011). In the magnetic force-based tissue engineering technology, cells are incubated with magnetic nanoparticle-containing liposomes and a magnet is placed on the reverse side. In this condition, cells form multilayered cell sheets after 24-h of incubation (Ishii et al. 2014).
Another technique for engineering cellular tissues called electrochemical method has been proposed by Inaba et al. in 2009 (Inaba et al. 2009). In this method, cells are cultured on a self-assembled monolayer of alkanethiol. Then, the self-assembled monolayer can be reductively desorbed from the gold substrate by the application of a negative electrical potential, resulting in the detachment of cell sheets from the gold surface (Inaba et al. 2009). Furthermore, it was developed a light-induced cell sheet technology in which cell sheets can be detached from a TiO2 nanodot-coated quartz substrate after UV365 illumination (Jiang et al. 2017). It is important to underline that the above described methods for cell sheet harvesting have taken advantage of surface property variations to induce cell detachment.
MSC sheets could be considered a promising tool for the regeneration of damaged tissues due to the fact that they do not require the use of non-self-materials such as biodegradable scaffolds, which can induce an inflammatory reaction in the host (Tsumanuma et al. 2011). Current treatment options to repair large bone defects caused by injuries, infections and degenerative diseases are mainly based on the usage of autologous or allogeneic bone grafts (Wen et al. 2017; Yorukoglu et al. 2017). Although these methods are commonly used, autologous bone grafts are limited by the availability of graft material and morbidity at the donor site such as pain or infections, whereas allogenic bone grafts are limited by disease transmission and potential immunological responses. Another current method for bone repair is the use of artificial bone, but it possesses several limitations such as weak synostosis, poor biodegradability and low mechanical strength (Wen et al. 2017). In this context, MSC sheet-based tissue engineering seems to be the appropriate strategy that can overcome the shortcomings of the previous methods. The aim of this review is to describe the cell sheets of MSCs and assess their applicability in bone tissue regeneration and repair (Table 2).
Use of MSC sheets for bone regeneration and repair
The use of MSC sheets for the regeneration of osteogenic tissue was firstly described by Ouyang et al. in 2006 (Ouyang et al. 2006a). In their pioneering study, these authors analysed the effects of MSC sheets assembled onto demineralized bone grafts by using the wrapping method on the repair of large-bone and tendon defects. The results showed that when MSC sheets were assembled with large allografts, there was a formation of a periosteum tissue-like structure, which was important for the repair of bone defects (Ouyang et al. 2006a). Importantly, this study shed light on the fact that MSC sheets can be easily fabricated by layering the recovered cell sheets without any scaffolds or complicated manipulation and can be used as a novel strategy for clinical regeneration of large skeletal defects. Therefore, wrapping MSC sheets on devitalized allograft segments have been used as a tissue-engineered periosteum prior to transplantation. In this context, by comparing early-passaged young (P3) MSC sheets and later-passaged aged (P10) MSC sheets into a femoral allograft mouse model, it has been shown that young cultured MSC sheets can significantly increase the bone callus formation around allografts (Shang et al. 2017).
To evaluate if MSC sheets can be used for bone reconstruction, Chen et al. generated tube-like constructs composed of MSC sheets and polylactic–co-glycolic acid (PLGA) meshes and implanted them into nude rats (Chen et al. 2007). Their results showed that there was the formation of dense mineralized tissue in the subcutaneous sites of these rats. Importantly, three other studies have shown that it is possible to obtain viable bone constructs using MSC sheets obtained by similar wrapping methods (Zou et al. 2009; Long et al. 2014; Uchihara et al. 2015). In the first study, Zou and colleagues reported that when MSC sheets were wrapped onto an allograft and implanted in mice there was a formation of cortical bone (Zou et al. 2009). In the second study, Long et al. showed that allografts wrapped with MSC sheets were able to enhance graft-host osteointegration as well as bone callus formation (Long et al. 2014), whereas in the third study, Uchihara et al. co-transplanted cell sheets derived from bone marrow stromal cells (BMSCs) with irradiated bone in the rat femur and demonstrated that MSC sheets can be used to facilitate osteogenesis of irradiated bones (Uchihara et al. 2015). Importantly, it has been shown that it is possible to obtain bone grafts in predetermined shapes and similar structure to the native bone using mineralised osteogenic BMSC sheets in combination with tubular coral scaffolds (Chen et al. 2007). Therefore, these findings also support the concept that the combination of MSC sheets with scaffolds is an encouraging technology for the regeneration of large bone grafts.
The strategy of using a combination of coral particles and MSC sheets for bone tissue engineering has also been successfully demonstrated by Geng et al. (Geng et al. 2013). Several other scaffolds have been combined with MSC sheets for bone regeneration, such as those composed of poly(sebacoyl diglyceride) (PSeD) (Xie et al. 2015) and poly-ε-caprolactone (PLC)/β-tricalcium phosphate (β-TCP) (Kim et al. 2016). PSeD scaffolds combined with human ethmoid sinus mucosa membrane (hESMSCs) and PLC/β-TCP scaffolds were able to stimulate the formation of new bone in critical-sized calvarial defects of rats (Xie et al. 2015; Kim et al. 2016).
Interestingly, to enhance osteogenesis of MSC sheets, they have also been combined with scaffolds containing biological agents (Table 2). In this context, bone morphogenetic protein-2-loaded calcium sulfate (Qi et al. 2012), chitosan/hyaluronic acid nanoparticles plus microRNA-21 (Wang et al. 2016a), nanoscale hydroxy-apatite combined with autologous platelet‐rich fibrin (Wang et al. 2017) and polyethylenimine–alginate nanocomposites plus human BMP-2 (Jin et al. 2014) were successfully used to induce bone regeneration when combined with MSC sheets. Similar results were obtained by combining MSC sheets with biological agents and without scaffolds such as gelatin (Kim et al. 2017) and stromal cell-derived factor-1 (SDF-1) (Chen et al. 2016) (Table 2). For example, it has been shown that the supplementation of gelatin in osteogenic medium (GCSs) induces higher osteogenic differentiation abilities than conventional osteogenic cell sheets (OSCs) (Kim et al. 2017), whereas the addition of SDF-1 to MSC sheets was able to induce new bone formation in fractures and also bone union (Chen et al. 2016).
Although the use of MSC sheets in combination with bone grafts or scaffolds/biological agents have shown promising results, three other studies have shown that MSC sheets can be used also without any graft or scaffolds (Akahane et al. 2008, 2010a; Nakamura et al. 2010). Akahane et al. in 2008 were the first authors that investigated the graft-free use of MSC sheets to obtain bone tissue (Akahane et al. 2008). They generated rat MSC sheets using osteogenic supplements and rolled them to obtain tube-like structures that were subsequently transplanted into subcutaneous sites of rats. There was a formation of ectopic calcification 6 weeks after sheet transplantation, indicating that osteogenic MSC sheets can be used as osteogenic implants for bone tissue reconstruction (Akahane et al. 2008). Later, the same authors injected MSC sheets derived from BMSCs through a needle into subcutaneous sites and dead bone of rats (Akahane et al. 2010a). Their results confirmed that MSC sheets can be also transplanted via a needle without the use of graft or scaffolds to reconstruct hard tissue in osteonecrosis and non-union treatment. Currently, the possibility to use scaffold-free MSC sheets represents an intriguing strategy with several advantages over scaffold-based strategies, such as the absence of inflammatory reactions after transplantation to the host. These findings were confirmed by two different studies by Nakamura et al. and Ma et al, in which the use of MSC sheets without exogenous scaffolds showed that a femoral fracture was completely cured in a rat non-union model (Nakamura et al. 2010) and that BMSC sheets can accelerate the development of functional 3D bone tissues (Ma et al. 2010).
Limitations of cell-sheet technology
While there have been significant advances in the production of MSC sheets for bone regeneration, more than one parameter has been used such as the composition of the culture medium, the In vitro culture period and the use of cell sheets with or without scaffolds/grafts (Yorukoglu et al. 2017). Therefore, several questions are required to be solved before this technology goes into clinical practice. Moreover, the immunogenicity and the survival of MSC sheets after implantation should be investigated (Ouyang et al. 2006b). For this purpose, the autologous cell source should be used to avoid immunological rejection. Importantly, additional studies are still needed to understand the choice of scaffold material and ideal culture conditions (Chen et al. 2007), and to determine any clinical applications of MSC sheet technology (Akahane et al. 2010b).
One limitation of the cell sheet technology is the possible risk of using ex vivo expanded MSCs. In fact, the growth of MSCs requires culture medium supplemented with fetal bovine serum (FBS), which can increase the risk of contamination and induce unfavourable cellular modifications. To replace the FBS and to reduce the possible re‐implantation problems of cultivated MSC sheets, some investigators have used platelet-rich fibrin (PRF) as a possible substitute (Wang et al. 2017). Another important problem of the cell sheet technology is the limited blood supply that is necessary for bone regeneration (Yorukoglu et al. 2017). In fact, large and thick tissue grafts, such as those generated by the cell sheet technology, could induce the generation of necrotic cores due to limited passive diffusion of molecules such as nutrients and oxygen. In order to resolve this problem, several researchers are trying to produce 3D vascularized tissues using cell sheet technology (65).
Importantly, today, cell sheet manufacture is manual and requires a highly skilled operator to produce the sheets. Therefore, a number of questions have to be answered before this technique goes to clinical practice. First of all, a method of quality control for cell sheets is needed. For example, prior to the scheduled day of transplantation, the prepared autologous cell sheets should be subjected to various quality tests such as cell number, the percentage of cell viability, cell purity and thicknesses of cell sheets. Moreover, also unknown variation in the surfaces of materials could have a significant impact on safety, efficacy and consistency of a product (Kirby et al. 2018). Importantly, it is also essential to underline that in clinical applications, cell sheets should be also negative for Mycoplasma pneumoniae, endotoxin, bacteria, fungi and viruses (Yamamoto et al. 2017). Therefore, more extensive research and clinical trials are needed to define a method of quality control for cell sheets in clinical applications.
Conclusions and future perspectives
In the first studies, several biomaterials were combined with MSC sheets for the regeneration of the osteogenic tissues such as polylactic-co-glycolic acid (PLGA) meshes (2), coral particles (Geng et al. 2013), β-tricalcium phosphate (Akahane et al. 2010b; Kim et al. 2016), hydroxyapatite particles (Wang et al. 2016a), surface-modified titanium and zirconia (Zhou et al. 2010), coumarin-like derivative osthole (Gao et al. 2013) and a complex of polyethylenimine-alginate nanocomposites (Jin et al. 2014). Moreover, biological agents such as Notch activation by Jagged1 (Tian et al. 2017), vitamin C (Guo et al. 2015), stromal cell-derived factor-1 (Chen et al. 2016), platelet-rich fibrin (Wang et al. 2017) and simvastatin (Qi et al. 2013) were utilized in combination with MSC sheets to improve their osteogenesis. However, due to the fact that cell sheet engineering can improve the concentration of MSCs at the site of delivery without the use of external scaffolds, several studies have shown that is possible to use MSC sheets without any graft or scaffolds in bone regeneration and repair (Akahane et al. 2008, 2010b; Nakamura et al. 2010). Therefore, tissue-derived MSC sheets can be used either in scaffold/graft-free applications or in combination with various grafts or scaffolds to shorten the treatment period of bone regeneration. The principal drawback of the cell sheet technology is the potential induction of necrosis within the cell sheets caused by the absence of vascularization. Therefore, the current literature on this field encourages the production of 3D vascularized tissues by cell sheet engineering (Sakaguchi et al. 2015). Even if the major part of the studies used MSCs from human or animal bone marrow (BMSCs) to generate sheets for bone regeneration (Ouyang et al. 2006b; Chen et al. 2007; Gao et al. 2009; Zou et al. 2009; Akahane et al. 2010a, b; Nakamura et al. 2010), human ethmoid sinus mucosa membrane (hESMSCs) (Xie et al. 2015) and adipose-derived MSCs (Ad-MSCs) (Kim et al. 2016, 2017) have also been successfully used for this purpose.
To summarize, this review focused on a novel concept, which is the use of cell sheet technology to enhance the transplant efficiency and the bone regeneration ability of MSCs. Cell sheets not only offer an optimal microenvironment to enhance osteogenic differentiation potential of MSCs but also could be used as a promising approach for bone tissue regeneration and repair.
References
Akahane M, Nakamura A, Ohgushi H et al (2008) Osteogenic matrix sheet-cell transplantation using osteoblastic cell sheet resulted in bone formation without scaffold at an ectopic site. J Tissue Eng Regen Med 2:196–201
Akahane M, Shigematsu H, Tadokoro M et al (2010a) Scaffold-free cell sheet injection results in bone formation. J Tissue Eng Regen Med 4:404–411
Akahane M, Ueha T, Shimizu T et al (2010b) Cell sheet injection as a technique of osteogenic supply. Int J Stem Cells 3:138–143
Chang D, Shimizu T, Haraguchi Y et al (2015) Time course of cell sheet adhesion to porcine heart tissue after transplantation. PLoS ONE 10:e0137494
Chen F, Zhou Y, Barnabas ST et al (2007) Engineering tubular bone constructs. J Biomech 40:S73–S79
Chen G, Qi Y, Niu L et al (2015) Application of the cell sheet technique in tissue engineering. Biomed Rep 3:749–757
Chen G, Fang T, Qi Y et al (2016) Combined use of mesenchymal stromal cell sheet transplantation and local injection of SDF-1 for bone repair in a rat nonunion model. Cell Transplant 25:1801–1817
Chen L, Xing Q, Zhai Q et al (2017) Pre-vascularization enhances therapeutic effects of human mesenchymal stem cell sheets in full thickness skin wound repair. Theranostics 7:117–131
Cui Y, Yao M, Liu Y et al (2016) Effects of cartilage-derived morphogenetic protein 1 (CDMP1) transgenic mesenchymal stem cell sheets in repairing rabbit cartilage defects. Genet Mol Res. https://doi.org/10.4238/gmr.15028058
Gao Z, Chen F, Zhang J et al (2009) Vitalisation of tubular coral scaffolds with cell sheets for regeneration of long bones: a preliminary study in nude mice. Br J Oral Maxillofac Surg 47:116–122
Gao L-N, An Y, Lei M et al (2013) The effect of the coumarin-like derivative osthole on the osteogenic properties of human periodontal ligament and jaw bone marrow mesenchymal stem cell sheets. Biomaterials 34:9937–9951
Gao H, Li B, Zhao L, Jin Y (2015) Influence of nanotopography on periodontal ligament stem cell functions and cell sheet based periodontal regeneration. Int J Nanomed 10:4009
Geng W, Ma D, Yan X et al (2013) Engineering tubular bone using mesenchymal stem cell sheets and coral particles. Biochem Biophys Res Commun 433:595–601
Gomes JÁP, Monteiro BG, Melo GB et al (2010) Corneal reconstruction with tissue-engineered cell sheets composed of human immature dental pulp stem cells. Invest Ophthalmol Vis Sci 51:1408–1414
Guillaume-Gentil O, Semenov OV, Zisch AH et al (2011) pH-controlled recovery of placenta-derived mesenchymal stem cell sheets. Biomaterials 32:4376–4384
Guo P, Zeng J, Zhou N (2015) A novel experimental study on the fabrication and biological characteristics of canine bone marrow mesenchymal stem cells sheet using vitamin C. Scanning 37:42–48
Haraguchi Y, Shimizu T, Matsuura K et al (2014) Cell sheet technology for cardiac tissue engineering. Cardiac tissue engineering. Springer, New York, pp 139–155
Huang C-C, Tsai H-W, Lee W-Y et al (2013) A translational approach in using cell sheet fragments of autologous bone marrow-derived mesenchymal stem cells for cellular cardiomyoplasty in a porcine model. Biomaterials 34:4582–4591
Inaba R, Khademhosseini A, Suzuki H, Fukuda J (2009) Electrochemical desorption of self-assembled monolayers for engineering cellular tissues. Biomaterials 30:3573–3579
Ishii M, Shibata R, Shimizu Y et al (2014) Multilayered adipose-derived regenerative cell sheets created by a novel magnetite tissue engineering method for myocardial infarction. Int J Cardiol 175:545–553
Iwata T, Washio K, Yoshida T et al (2015) Cell sheet engineering and its application for periodontal regeneration. J Tissue Eng Regen Med 9:343–356
Jiang Z, Xi Y, Lai K et al (2017) Laminin-521 promotes rat bone marrow mesenchymal stem cell sheet formation on light-induced cell sheet technology. Biomed Res Int. https://doi.org/10.1155/2017/9474573
Jin H, Zhang K, Qiao C et al (2014) Efficiently engineered cell sheet using a complex of polyethylenimine–alginate nanocomposites plus bone morphogenetic protein 2 gene to promote new bone formation. Int J Nanomed 9:2179
Kavuzlu A, Tatar EÇ, Karagöz T et al (2017) The effects of the stem cell on ciliary regeneration of injured rabbit sinonasal epithelium. Eur Arch Otorhinolaryngol 274:3057–3064
Kawamura M, Miyagawa S, Fukushima S et al (2015) Xenotransplantation of bone marrow-derived human mesenchymal stem cell sheets attenuates left ventricular remodeling in a porcine ischemic cardiomyopathy model. Tissue Eng Part A 21:2272–2280
Kim Y, Lee SH, Kang B et al (2016) Comparison of osteogenesis between adipose-derived mesenchymal stem cells and their sheets on poly–caprolactone/-tricalcium phosphate composite scaffolds in canine bone defects. Stem Cells Int. https://doi.org/10.1155/2016/8414715
Kim AY, Kim Y, Lee SH et al (2017) Effect of gelatin on osteogenic cell sheet formation using canine adipose-derived mesenchymal stem cells. Cell Transplant 26:115–123
Kirby GT, Michelmore A, Smith LE et al (2018) Cell sheets in cell therapies. Cytotherapy 20:169–180
Kwon OH, Kikuchi A, Yamato M et al (2000) Rapid cell sheet detachment from poly (N-isopropylacrylamide)-grafted porous cell culture membranes. J Biomed Mater Res 50:82–89
Lee DY, Kim H, Shim IK et al (2017) Treatment of chemically induced oral ulcer using adipose-derived mesenchymal stem cell sheet. J Oral Pathol Med 46:520–527
Long T, Zhu Z, Awad HA et al (2014) The effect of mesenchymal stem cell sheets on structural allograft healing of critical sized femoral defects in mice. Biomaterials 35:2752–2759
Ma D, Ren L, Liu Y et al (2010) Engineering scaffold-free bone tissue using bone marrow stromal cell sheets. J Orthop Res 28:697–702
McLaughlin MM, Marra KG (2013) The use of adipose-derived stem cells as sheets for wound healing. Organogenesis 9:79–81
Miyahara Y, Nagaya N, Kataoka M et al (2006) Monolayered mesenchymal stem cells repair scarred myocardium after myocardial infarction. Nat Med 12:459
Nakamura A, Akahane M, Shigematsu H et al (2010) Cell sheet transplantation of cultured mesenchymal stem cells enhances bone formation in a rat nonunion model. Bone 46:418–424
Nishida K, Yamato M, Hayashida Y et al (2004) Corneal reconstruction with tissue-engineered cell sheets composed of autologous oral mucosal epithelium. N Engl J Med 351:1187–1196
Oka M, Miyabe Y, Sugiura N et al (2018) Cell sheet engineering and kidney diseases. Contrib Nephrol 195:74–80
Okuda A, Horii-Hayashi N, Sasagawa T et al (2017) Bone marrow stromal cell sheets may promote axonal regeneration and functional recovery with suppression of glial scar formation after spinal cord transection injury in rats. J Neurosurg Spine 26:388–395
Ouyang HW, Cao T, Zou XH et al (2006) Mesenchymal stem cell sheets revitalize nonviable dense grafts: implications for repair of large-bone and tendon defects. Transplantation 82:170–174
Pirraco RP, Obokaokata H, Iwata T et al (2011) Development of osteogenic cell sheets for bone tissue engineering applications. Tissue Eng Part A 17:1507–1515
Qi Y, Wang Y, Yan W et al (2012) Combined mesenchymal stem cell sheets and rhBMP-2-releasing calcium sulfate–rhBMP-2 scaffolds for segmental bone tissue engineering. Cell Transplant 21:693–705
Qi Y, Zhao T, Yan W et al (2013) Mesenchymal stem cell sheet transplantation combined with locally released simvastatin enhances bone formation in a rat tibia osteotomy model. Cytotherapy 15:44–56
Qi Y, Du Y, Li W et al (2014) Cartilage repair using mesenchymal stem cell (MSC) sheet and MSCs-loaded bilayer PLGA scaffold in a rabbit model. Knee Surg Sports Traumatol Arthrosc 22:1424–1433
Qi Y, Chen G, Feng G (2016) Osteoarthritis prevention and meniscus regeneration induced by transplantation of mesenchymal stem cell sheet in a rat meniscal defect model. Exp Ther Med 12:95–100
Rahmi G, Pidial L, Silva AK et al (2016) Designing 3D mesenchymal stem cell sheets merging magnetic and fluorescent features: when cell sheet technology meets image-guided cell therapy. Theranostics 6:739
Sakaguchi K, Shimizu T, Okano T (2015) Construction of three-dimensional vascularized cardiac tissue with cell sheet engineering. J Controll Release 205:83–88
See EY-S, Toh SL, Goh JC-H (2011) Effects of radial compression on a novel simulated intervertebral disc–like assembly using bone marrow–derived mesenchymal stem cell cell-sheets for annulus fibrosus regeneration. Spine 36:1744–1751
Sekine H, Shimizu T, Dobashi I et al (2011) Cardiac cell sheet transplantation improves damaged heart function via superior cell survival in comparison with dissociated cell injection. Tissue Eng Part A 17:2973–2980
Shang X, Shu B, Wang Y et al (2017) Human mesenchymal stromal cell sheet enhances allograft repair in a mouse model. Sci Rep 7:7982
Tanaka Y, Shirasawa B, Takeuchi Y et al (2016) Autologous preconditioned mesenchymal stem cell sheets improve left ventricular function in a rabbit old myocardial infarction model. Am J Transl Res 8:2222
Tano N, Narita T, Kaneko M et al (2014) Epicardial placement of mesenchymal stromal cell-sheets for the treatment of ischemic cardiomyopathy; in vivo proof-of-concept study. Mol Ther 22:1864–1871
Tian Y, Xu Y, Xue T et al (2017) Notch activation enhances mesenchymal stem cell sheet osteogenic potential by inhibition of cellular senescence. Cell Death Dis 8:e2595
Tsumanuma Y, Iwata T, Washio K et al (2011) Comparison of different tissue-derived stem cell sheets for periodontal regeneration in a canine 1-wall defect model. Biomaterials 32:5819–5825
Uchihara Y, Akahane M, Shimizu T et al (2015) Osteogenic matrix cell sheets facilitate osteogenesis in irradiated rat bone. Biomed Res Int. https://doi.org/10.1155/2015/629168
Ueyama Y, Yagyuu T, Maeda M et al (2016) Maxillofacial bone regeneration with osteogenic matrix cell sheets: an experimental study in rats. Arch Oral Biol 72:138–145
Wang C-C, Chen C-H, Lin W-W et al (2007) Direct intramyocardial injection of mesenchymal stem cell sheet fragments improves cardiac functions after infarction. Cardiovasc Res 77:515–524
Wang Z, Wu G, Wei M et al (2016a) Improving the osteogenesis of human bone marrow mesenchymal stem cell sheets by microRNA-21-loaded chitosan/hyaluronic acid nanoparticles via reverse transfection. Int J Nanomed 11:2091
Wang Z-S, Feng Z-H, Wu G-F et al (2016b) The use of platelet-rich fibrin combined with periodontal ligament and jaw bone mesenchymal stem cell sheets for periodontal tissue engineering. Sci Rep 6:28126
Wang X, Li G, Guo J et al (2017) Hybrid composites of mesenchymal stem cell sheets, hydroxyapatite, and platelet-rich fibrin granules for bone regeneration in a rabbit calvarial critical size defect model. Exp Ther Med 13:1891–1899
Wei F, Song T, Ding G et al (2013) Functional tooth restoration by allogeneic mesenchymal stem cell-based bio-root regeneration in swine. Stem Cells Dev 22:1752–1762
Wen Y, Yang H, Liu Y et al (2017) Evaluation of BMMSCs-EPCs sheets for repairing alveolar bone defects in ovariectomized rats. Sci Rep 7:16568
Xie Q, Wang Z, Huang Y et al (2015) Characterization of human ethmoid sinus mucosa derived mesenchymal stem cells (hESMSCs) and the application of hESMSCs cell sheets in bone regeneration. Biomaterials 66:67–82
Yamamoto K, Yamato M, Morino T et al (2017) Middle ear mucosal regeneration by tissue-engineered cell sheet transplantation. NPJ Regen Med 2:6
Yorukoglu AC, Kiter A, Akkaya S et al (2017) A concise review on the use of mesenchymal stem cells in cell sheet-based tissue engineering with special emphasis on bone tissue regeneration. Stem Cells Int 2017:2374161
Zhang D, Huang W, Dai B et al (2010) Genetically manipulated progenitor cell sheet with diprotin A improves myocardial function and repair of infarcted hearts. Am J Physiol-Heart Circ Physiol 299:H1339–H1347
Zhao J, Liu L, Wei J et al (2012) A novel strategy to engineer small-diameter vascular grafts from marrow-derived mesenchymal stem cells. Artif Organs 36:93–101
Zhou W, Han C, Song Y et al (2010) The performance of bone marrow mesenchymal stem cell–implant complexes prepared by cell sheet engineering techniques. Biomaterials 31:3212–3221
Zou XH, Cai HX, Yin Z et al (2009) A novel strategy incorporated the power of mesenchymal stem cells to allografts for segmental bone tissue engineering. Cell Transplant 18:433–441
Acknowledgements
This study was supported by Natural Science Foundation of Zhejiang Province (LY18H060013), Foundation of Zhejiang Province medical health (2016KYB299, 2018KY820), Medical and Health Research Project of Zhejiang Province (2017KY662, 2018KY825), Science and technology project of Shaoxing (2017CX007, 2017B70031).
Author information
Authors and Affiliations
Contributions
All the authors have contributed to this paper.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chen, M., Xu, Y., Zhang, T. et al. Mesenchymal stem cell sheets: a new cell-based strategy for bone repair and regeneration. Biotechnol Lett 41, 305–318 (2019). https://doi.org/10.1007/s10529-019-02649-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10529-019-02649-7