
Abstract
As in other parts of sub-Saharan Africa, youth in Kenya report low rates of condom use. Although several studies have explored reasons for the low condom use among Kenyan youth, not many have established linkages between lack of use and normative beliefs and attitudes around condoms. Using the Theory of Planned Behavior (TPB), this article examined whether beliefs and attitudes around condoms influenced intentions and actual condom use. Data for the study were restricted to 1453 sexually active youth during the last school break. Path analysis was used to examine the relationship between the TPB constructs and condom use among Kenyan youth. Results indicated a direct relationship between attitudes and condom use for male respondents and an indirect relationship between these two variables for females. Both males and females who expressed greater intentions to use condoms were significantly more likely to report they used condoms consistently. Also, male and female youth with higher perceived behavioral control were significantly more likely to have used condoms consistently. Males with friends who used condoms were significantly more likely to use condoms consistently. The findings suggest the importance of examining young people’s attitudes toward condoms—in particular, those deeply rooted in misconceptions that serve to discourage safer sexual behaviors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Globally, it is estimated that about 2.1 million young people between the ages of 10 and 19 live with HIV/AIDS; out of which 1.4 million (64%) reside in Eastern and Southern Africa (UNICEF, 2015). Recent evidence in Kenya indicates declines in HIV prevalence from 10.5% in 1995–1996 to 5% in 2013 (UNAIDS, 2014). Despite the declining prevalence, youth in Kenya and sub-Saharan Africa in general are heavily burdened with the virus (Idele et al., 2014). In Kenya, approximately 29% of all new HIV infections are among young people (National AIDS Control Council, 2015). Thus, some studies show that the current challenge in reducing the transmission of HIV resides among youth, especially as they are vulnerable to risky sexual behaviors (Njoroge, Olsson, Pertet, & Ahlberg, 2010).
In the prevention of HIV transmission among youth, condoms are often considered the first line of defense, yet several studies show low condom use among young people in sub-Saharan Africa (Beksinska, Smit, & Mantell, 2012; Chialepeh & Susuman 2015; Maticka-Tyndale & Tenkorang, 2010; Njoroge et al., 2010; Oppong, Osafo, & Doku, 2016). Evidence from Nyanza province in Kenya showed that only 26.8% of sexually active males and 29.2% of females in upper primary schools used condom in their last sexual activity (Maticka-Tyndale & Tenkorang, 2010). Several reasons are documented for lack of use among youth, including concerns about the safety of condoms and the cultural perception that associates condom use with promiscuity and infidelity (Adebiyi & Asuzu, 2009; Chimbiri, 2007; Fehr, Vidourek, & King 2015). In addition, the feeling of embarrassment in purchasing condoms, misperceptions about their effectiveness and the societal shroud that covers condom purchase have all contributed to low usage in many parts of sub-Saharan Africa (Kennedy et al., 2007). Other structural and systemic reasons often cited for lack of use among youth include challenges in accessing condoms in a timely manner (Adebiyi & Asuzu, 2009; Musinguzi et al., 2015; Njoroge et al., 2010; Sarkar, 2008), cost of purchasing condoms and the ambivalence that characterizes messages of condom use in schools and communities (Buhi, 2015; Maticka-Tyndale & Kyeremeh, 2010; Njoroge et al., 2010; Shrestha, Farnham, Whitham, & Sansom, 2016).
It is equally important to note that due to the patriarchal norms in most African societies, condom use is particularly gendered. In this regard, decisions about condom use in sexual encounters are often framed as the responsibility of men, while women are expected to submit without questioning men’s judgement (Delvaux & Nöstlinger, 2007). Thus, the patriarchal control of condom use has silenced and delegitimized the rights of many women in sub-Saharan Africa (SSA) in negotiating for protection during sexual intercourse (Exavery et al., 2012). This suggests that any program to encourage condom use among youth in SSA cannot achieve desirable results without including strategies that challenge attitudinal and cultural barriers.
While a plethora of literature exists on condom use in sub-Saharan Africa, there is less emphasis on how normative beliefs and attitudes influence intention and actual condom use among youth (Bogart et al., 2011; Heeren, Jemmott, Mandeya, & Taylor, 2009; Montano & Kasprzyk, 2015; Peltzer, 2000). Using data collected in 2006 from a large sample of secondary school students in Kenya, this study contributes to filling this scholarly gap and adds to the growing body of literature on condom use among youth in sub-Saharan Africa. The study seeks to broaden our understanding of how beliefs, attitudes and intentions influence condom use among secondary school students in Kenya using the Theory of Planned Behavior (TPB) (Ajzen & Fishbein, 1975).
Theoretical and Empirical Considerations
The TPB (Ajzen, 1985) posits that intention to perform a specific behavior is a strong predictor of actual behaviors. Thus, behavioral intention represents a person’s readiness to perform a given behavior. As the immediate antecedent to actual behavior, behavioral intention is affected by other proximate determinants, such as attitude toward the behavior, subjective norms, and perceived behavioral control. Attitude toward behavior is conceptualized as a body of beliefs that aids individuals in their assessment of the desirability of engaging in the predicted behavior. These beliefs can be positive or negative. Subjective norms point to the influence of social or peer networks in determining whether and how the behavior in question should be performed. Perceived behavioral control measures the extent to which individuals have control or feel confident about performing the specific behavior. Generally, the model assumes that positive and favorable attitudes toward condoms may combine with greater perceived control to influence intentions to use condoms and actual condom use.
The empirical literature demonstrates that attitudes and beliefs about condoms affect actual condom use both directly and indirectly through individuals’ intentions to use condoms. In this regard, youth are more likely to use condoms when they perceive some benefits and develop positive attitudes toward condoms (Maharaj & Cleland, 2005; Taylor et al., 2014). Similarly, young people are less likely to use condoms when they perceive barriers and develop negative attitudes toward them (Van Rossem & Meekers, 2011). Maharaj and Cleland noted, for instance, that for young people to use or intend to use condoms, they must believe in the efficacy and ability of the condom to protect against HIV and other sexually transmitted infections. On the other hand, youth may not use condoms when they believe and perceive condoms as unreliable, capable of reducing sexual pleasure and causing sterility, etc., (Katikiro & Njau, 2012; Lule & Gruer, 1991; Ochieng, Kakai, & Abok, 2011). Some other beliefs about condoms include the misconception that they contain HIV and have been intentionally designed with pores to infect Africans (Bogart et al. 2011; Maticka-Tyndale & Kyeremeh, 2010). It is important to note that myths and misconceptions that undermine HIV preventive behaviors are largely consistent with the cultural ethos and religious beliefs of the majority of people in sub-Saharan Africa (see Bogart et al., 2011; Leclerc-Madlala, 2002; Tenkorang, 2014; Tenkorang, Obeng-Gyimah, Maticka-Tyndale, & Adjei, 2011b).
Besides attitudes and beliefs, several other factors have been discussed in the literature as important correlates of condom use in sub-Saharan Africa. For example, previous work has shown that commitment to condom use in sexual relationships depended on the nature and type of the relationship. In Kenya, one study showed that 20% of adults who were sexually experienced reported consistent condom use with regular or long-term partners while 65% reported consistent condom use with casual partners (Waithaka & Bessinger, 2001). Similarly, Hendriksen, Pettifor, Lee, Coates, and Rees (2007) found that young adults who had been in committed relationships for more than 6 months or longer were less likely to use condoms for their most recent sexual activity compared to those in unstable relationships. Some studies have also documented the level of formal education as a strong predictor of condom use among adolescents in SSA (Hendriksen et al., 2007). Young people with higher levels of formal education were significantly more likely to use condoms than those without formal education (Maticka-Tyndale et al., 2005; Waithaka & Bessinger, 2001).
Other psychosocial factors, including risk perception and knowledge about HIV/AIDS are considered theoretically relevant in explaining condom use among youth. Individuals who perceive they are at increased risk and those with greater knowledge about HIV and AIDS are theorized as more likely to use condoms. However, the evidence establishing associations between these psychosocial variables and condom use remains largely inconclusive (Katikiro & Njau, 2012; Qiao, Li, & Stanton, 2013; Tenkorang, 2014; Volkmann et al., 2013). Using data collected from youth in Kenya and employing the TPB, this article examined associations between attitudes, subjective norms, perceived behavioral control, intentions to use condoms and actual condom use.
Method
Participants
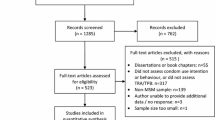
Data used for this study were collected between December 2005 to January 2006 from 14,173 Form 1 to 3 students (equivalent to Grades 9–11 in North America), aged 13–20 years, in 154 public secondary schools located in five of Kenya’s eight provinces (Central, Coast, Eastern, Nairobi and Rift Valley). Data were intended to provide a baseline/pre-program profile in preparation for delivery and evaluation of the Secondary School Action for Better Health (SSABH) HIV prevention program. The North Eastern province was avoided due to security reasons. Nyanza and the Western provinces were excluded to prevent potential confounding of results since they had earlier been flooded with HIV interventions. The schools that participated in this study were selected using stratified random sampling proportional to the number of public schools in each province. For the purposes of this study, the data were restricted to students who were sexually active during the last school break (N = 1453). Students completed surveys in English (the language of education), in gender-segregated groups under the supervision of research staff from Steadman Research Services Incorporated. Teachers were not present in classrooms during survey completion. Ethical clearance for this work was obtained from the University of Windsor’s Research Ethics Board.
Student questionnaires used for data collection were developed based on results obtained from formative elicitation research whose main objective was to first, provide some guidance to the development of an HIV prevention program for secondary schools and second, inform the development of a questionnaire that tapped respondents’ knowledge, attitudes, perceptions, and behaviors toward condom use, sexual behaviors, and HIV/AIDS (Maticka-Tyndale, 2010). The elicitation research consisted of 24 focus groups with students and 24 interviews with teachers from a sample of 12 schools. Focus group discussions and interviews addressed knowledge, beliefs, attitudes, preferences, and experiences with ABC (abstinence, be faithful to one partner, condom use); patterns of sexual activity; and attitudes, knowledge, and experience with HIV testing. During focus groups, students also reviewed and made comments on standardized questions used to assess knowledge of HIV transmission and prevention from the WHO/UNESCO Evaluation Tool Kit (WHO, 1999). Students made recommendations for additional and alternative questions they thought would test their knowledge of what was needed to keep them safe from HIV infection.
Measures
Condom Use During Last Sexual Break
The outcome measure used for analysis tapped the condom use experiences of secondary school youth in the last school break (this allowed students in all schools, even single-sex boarding schools to participate).Footnote 1 Specifically, students who reported sexual activity during the last school break were asked “How many times did you use a condom during the last school break?” Response categories included “never used condoms,” “used condoms sometimes,” and “always used condoms.”
Predictors of Condom Use During Last Sexual Break
The predictor variables captured aspects of the TPB as described earlier. Attitude toward condoms was measured with two proxy measures of attitude as conceptualized in the TPB. Questions asked whether respondents believed condoms had pores that allowed HIV to pass through them and also if condoms had chemicals that affected male infertility. Response categories for the research participants included “true = 0” and “false = 1.” These were considered proxy measures since they did not include a weighting of response by an evaluative component of these beliefs as portrayed in the measurement model of the TPB. The assumption was made in these measures that both passage of HIV through pores and male infertility were evaluated negatively. Perceived behavioral control was measured with four main variables that asked if the respondent could talk to their boyfriends/girlfriends about condom use (coded no = 0, yes = 1), could make sure they used condoms each time they had sex (coded no = 0; yes = 1), if a boy used a condom whether it meant he respected a girl (coded no = 0, yes = 1), and boys would agree to use condoms if it was the only way they could get sex (coded no = 0, yes = 1). Principal Component Analysis (PCA) was used, and the weighted factor scores (perceived behavioral control) underlying the factor structure extracted and used as a variable in the analysis. Social or subjective norms around condoms were measured with a question asking respondents if condoms were used in their group of friends (coded no = 0, yes = 1). Intention to use condoms, which is independent to actual condom use but dependent on attitude toward condoms, subjective norms, and perceived behavioral control, was measured with two variables that asked if study participants would insist on condom use even if their partners did not want to (coded no = 0, yes = 1); and if they would insist condoms be used every time they had sex even if they had not been tested for HIV (coded no = 0, yes = 1). Like attitudes, intention to use condoms was also a latent scalar measure derived from the above-mentioned indicators using PCA.
The study controlled for theoretically relevant psychosocial and demographic variables that could confound the simultaneous associations between predictor and outcome variables. Psychosocial variables included respondents’ perceived risks of contracting HIV measured as an ordinal variables (coded no risks = 0, low risk = 1, medium risk = 2, high risk = 3), whether respondents knew anyone infected with HIV in the school (coded no = 0, yes = 1) and whether they knew anyone who had died of AIDS (coded no = 0, yes = 1). Demographic variables included age of respondents measured in complete years; religious denomination (coded Christians = 0, Muslims = 1, no religion = 2, others = 3); region of residence (Central = 0, Coast = 1, Eastern = 2, Nairobi = 3, Rift Valley = 4). A dummy variable measuring whether the Ministry of Education’s HIV education program (Primary School Action for Better Health or PSABH) was present in the primary schools attended by the respondents. PSABH began to be delivered in primary schools in 2003 with the program rolled out across almost all schools in the country between 2002 and 2007. Gender-specific models were built to examine whether any differences existed among males and females regarding condom use.
Analytical Method
The theoretical framework adopted for this work identified key independent variables as directly and indirectly related to each other and to an outcome variable (condom use). For instance, while intention to use condoms predicts actual condom use, it is predicted by or dependent on perceived behavioral control, social norms about condoms, and attitude toward condom use. This complexity is best captured in a path-analytic model. Such a model estimates the simultaneous relationships between the specified dependent and independent variables. Path analysis estimates the direct, indirect, and total effects of the variables under consideration on the outcome of interest, in this case condom use at the last school break.
A direct effect implies an influence of one variable on the other unmediated by any other variable. An indirect effect, on the other hand, exists when the influence of a particular variable on another one is mediated by at least one intervening variable (Bollen, 1989).
Path coefficients are interpreted in the same way as regression coefficients. However, the use of the maximum likelihood estimation procedure allows us to interpret the coefficients by transforming them into probabilities or odds ratios. Thus, a positive coefficient (exponentiated) will mean youth were more likely to use condoms always than sometimes or never, while a negative coefficient indicated a lower likelihood of using condoms always than sometimes or never.
Results
Descriptive Information
Results in Table 1 show that, on average, respondents were about 17 years old and the majority identified as Christians. Respondents proportionately came from schools located in Rift Valley, Nairobi, Eastern, Central, Coastal, and the Central regions in that order. Since PSABH was still in the process of spreading out across the primary schools in the country, it is not surprising that less than half of these secondary school students had PSABH delivered in their primary schools. Regarding condom use, it was evident that the majority of respondents never used condoms during the last school break, with the percentage for nonuse higher among female youth. While both male and female youth had positive mean scores on behavioral control toward condom use, scores on intention to use condoms were negative, indicating they did not intend to use condoms. The majority of respondents endorsed the belief that condoms had pores that allowed HIV to pass through them. Similarly, the majority of respondents believed that condoms had chemicals that affect male infertility. A higher proportion of females believed in such myths compared to males. Consistent with previous studies, most youth perceived themselves at no risk of contracting HIV, although the majority knew people who had been infected or had died of AIDS.
Table 2 shows bivariate relationships between condom use and selected independent variables. For categorical variables, such relationships were assessed using cross-classification analysis. However, for continuous variables, one-way ANOVA was employed by comparing the scores for the three categories of the dependent variable. Results indicated significant relationships between perceived behavioral control, intention to use condoms, and actual condom use among male and female youth. It was evident that youth with higher scores on perceived behavioral control and intentions used condoms sometimes and always. Beliefs about condoms were significantly associated with condom use for males but not females. A higher proportion of males and females who endorsed negative beliefs about condoms never used condoms, albeit this was higher for girls. A substantial proportion of youth who believed their friends used condoms also used condoms consistently. Results indicated that risk perception was not significantly associated with condom use, but rather whether respondents knew others infected or deceased of HIV/AIDS. Demographic variables such as age and religious denomination were associated with condom use for males and not females. Specifically, male youth in the Eastern, Coastal, and Rift Valley provinces were significantly less likely to report they used condoms always, compared to those in the Central region of Kenya.
Multivariate Analysis
Tables 3 and 4 show the multivariate relationships between dependent and independent variables, and direct path coefficients are provided. Figures 1 and 2 depict the TPB with path coefficients for males and female, respectively. Results showed that attitudes toward condoms influenced intentions and actual condom use. Female youth who rejected the belief that condoms had chemicals that affect male infertility reported higher intentions to use condoms compared to those who endorsed such beliefs (Exp [.30] = 1.35). Also, male youth who rejected the belief that condoms had pores that allowed HIV to pass through had higher intentions of using condoms (Exp [.17] = 1.19).

Theory of Planned Behavior constructs predicting condom use at last school break for male youth

Theory of Planned Behavior constructs predicting condom use at last sexual break for female youth
Perceived behavioral control was associated with intention to use condoms and actual condom use for both male and female youth. Male and female youth with stronger behavioral control were, more likely to use condoms sometimes or always than never (Male = 22% and Female = 26%). Similarly, male and female youth with higher intentions to use condoms were more likely to use condoms always or sometimes than never (Male = 14% and Female = 15%). Males were more likely to use condoms if their friends did, but this was not significant for females. Compared to those in the Central province, male youth in schools located in the Coastal, Eastern, and Rift Valley provinces were all significantly less likely to use condoms always or sometimes than never. Knowing someone deceased of AIDS influenced intentions to use condom for female youth but not males.
Discussion
Kenya’s HIV situation has been described as stable in the last few years, especially as prevalence among young people has been declining. A report by the National AIDS Control Council (NACC) of Kenya estimated that in 2012 prevalence among female youth declined from 5.9 to 3.3%, while that for males remained between 1.1 and 1.5% over the period (NACC, 2015). It must be acknowledged that declines in prevalence may have been influenced, at least in part, by the delivery of HIV prevention programming in primary and secondary schools. Although progress made toward reducing HIV has been lauded, more work remains especially when new infections persist among young people, and the country is signatory to UNAIDS’ strategy of reaching zero prevalence between 2011 and 2015. Previous literature has demonstrated that youth have elevated risks of contracting HIV, mainly due to risky sexual behaviors (Prata, Vahidnia, & Fraser, 2006), and that providing gender-sensitive sexual health information could change attitudes and behaviors that render them vulnerable to contracting the deadly virus. Against this backdrop, condoms are considered an important line of defense, yet evidence across sub-Saharan Africa, including Kenya, demonstrates that youth use condoms inconsistently during sexual intercourse (Chimbiri, 2007; Njoroge et al., 2010). Using data collected in Kenya, and situated within the TPB, this study contributes to the existing body of literature that examines condom use among youth in Kenya.
Results indicate that for females, holding positive beliefs about condoms influenced actual condom use indirectly through intentions. Among males, the influence of intentions was directly onto actual condom use. The findings were largely consistent with the TPB that positive attitudes toward condom use (measured as a function of one’s belief in engaging in protective behavior) yield positive outcomes (Albarracin, Johnson, Fishbein, & Muerllerleile, 2001). This means it will be challenging and difficult for young people to develop positive attitudes toward condoms, especially under circumstances where they hold negative beliefs or endorse misconceptions about condoms. In the case of Kenyan male youth in this sample, endorsing such beliefs had direct impact on condom use. The findings corroborate studies elsewhere that demonstrated that the endorsement of myths about HIV transmission may undermine prevention efforts (Tenkorang & Maticka-Tyndale, 2013, 2014; Tenkorang, Maticka-Tyndale, & Rajulton, 2011a).
The TPB also postulates that attitudes toward condoms influence intentions to use condoms, which in turn affects actual condom use. Thus, intention to use condoms is considered proximal and directly associated with actual condom use. Our model showed a strong significant positive association between intentions to use condoms and condom use for both male and female respondents and was consistent with several other studies in sub-Saharan Africa and elsewhere that theorized intention as the cognitive representation of an individual’s readiness to act (Assefa & Haidar 2013; Couture, Caron, & Desrosiers, 2010).
Some gender differences were observed. For instance, descriptive results in Table 2 show that females who used condoms consistently had higher condom use intention scores than their male counterparts. This was different for actual condom use as higher proportions of males used condoms consistently than their female counterparts (see Table 1). Furthermore, while a direct relationship was shown between attitudes toward condoms and actual condom use for males, attitudes toward condoms affected actual condom use through intentions for females. Taken together, the results demonstrated that the theoretical pathways through which attitudes affected actual condom use may be gendered. Studies examining gender differences in attitudes, intentions and actual condom use are relatively scarce in the literature. Notwithstanding, Calsyn et al. (2013) documented gender differences in attitudinal barriers toward condom use. They found, for instance, that compared to females, males were significantly less likely to endorse motivational items related to “wanting” or “needing” to use condoms. These variations were attributed to differences in what males and females perceived as potential barriers to their sexual experiences. It was discovered that males often thought about condoms as reducing sexual pleasure, changing orgasm and reducing sexual intimacy compared to females, thus reducing their desire or intent to use condoms. We lacked these measures in our data to tease out these important relationships. However, our findings point to the need for more research on the gender dynamics on intentions and actual condom use experiences. Similarly, gender differences were observed in the influences of social norms around condoms and actual condom use. Unlike females, males were more likely to use condoms when they were in a network of friends who used condoms. This finding is consistent with the extant literature that reports that adolescents’ sexual behaviors could be influenced by their connections to the wider social environment and their peers (Fearson, Pettifor, & Hargreaves, 2015) and that such gender differences may be due to variations in the social and behavioral pressures to conform to gender norms and expectations within peer networks, which is greater for males than females (Peltzer, 2003; Taylor & Wong, 1996).
The majority of AIDS prevention models, including the TPB, have been criticized as individualistic. These models assume that the decision to engage in HIV preventive behaviors (condom use) is a rational decision taken by individuals. (Cochran & Mays, 1993), i.e., that individuals have control over behaviors that will keep them safe. Recognizing that this assumption is unrealistic, the TPB includes perceived behavioral control which captures the idea that other external realities may hamper an individual’s control over engaging in HIV preventive behaviors and that maintaining behavioral control is important. These theoretical suppositions were confirmed in our statistical models for both male and female respondents in Kenya, with perceived behavioral control influencing condom use both directly and indirectly through intentions. Thus, this research clearly showed the importance of perceived behavioral control for both males and females.
It was observed that male youth located in other provinces in Kenya had significantly lower odds of using condoms consistently compared to those from the Central province. This is consistent with results from the Kenya AIDS Indicator Survey conducted in 2007 that showed, for instance, that respondents from the Central province recorded the highest rates of condom use due mainly to increased sexual and reproductive health information in this province, compared to other provinces (National AIDS and STI Control Programme, 2007). While some studies in Kenya showed that psychosocial factors, including risk perception and knowledge of whether someone has died of AIDS are related to condom use (Maticka-Tyndale & Tenkorang, 2010; Van Rossem & Meekers, 2011), this study did not find such evidence.
The study has several policy implications. First, it is important to indicate that the TPB has important implications for community interventions that are modeled on social cognitive predictors. The TPB identified beliefs with an assumed evaluative component (as proxy for attitudes), social norms, perceived behavioral control and intention to use condoms as important to changing sexual behaviors and improving condom use among youth in Kenya. The findings suggest that it is important to examine young people’s attitudes toward condoms—in particular, those that are deeply rooted in myths and misconceptions and serve to discourage safer sexual behaviors among youth. However, the significance of social norms to condom use means that the true expectations about change do not only rest on individual attitudes and beliefs, but also the larger social networks within which individuals belong. Regional information about condom use from this study suggests that the Kenyan government might target youth in some regions in their fight against HIV/AIDS, especially those with lower condom use. Youth may be targeted with messages of condom use and other HIV preventive methods. In particular, we recommend that condoms be made free and accessible to young people in Kenya.
Limitations
There are several limitations to this study that should be kept in mind when interpreting our findings. For instance, data used were self-reported and may be subject to recall/memory and social desirability bias. Also, in the majority of sub-Saharan African countries, including Kenya, it is observed that cultural conceptions of masculinity and femininity affect response to survey questions; thus, males tend to overestimate their sexuality with females underestimating theirs (Poulin, 2010). Data were also collected about 10 years ago, so findings must be interpreted with extreme caution, especially given changes that have occurred in the Kenyan society to date. The cross-sectional nature of the data limits interpretation of the results to associations between independent and dependent variables. Although measures used tapped several aspects of the TPB, including other aspects of the constructs might have enhanced the reliability of latent variables used in the study. Also, youth in this study represented a privileged segment of Kenyan society. They were attending secondary school, unlike the majority of their peers.
Conclusion
These notwithstanding, it is relevant to indicate that this is one of the very few studies that used a large sample of secondary school students from Kenya to validate the TPB. Results showed that the TPB was relevant and may be useful to interventions that seek to prevent new infections among youth in Kenya and elsewhere in sub-Saharan Africa. This means, in spite of providing information about condoms, it will be equally necessary to equip youth with skills that build their self-efficacy toward condom use as this was significantly associated with intentions and actual condom use. Such interventions must appreciate the gendered and power dynamics that characterize condom use in Kenya, ensuring that females in particular can insist and have the ability to demand condoms in their sexual relationships.
Notes
The school year in Kenya is divided into 3 equal terms of 3 months each separated by 1 month school breaks. The last school break was 1 month (approximately 4 weeks).
References
Adebiyi, A. O., & Asuzu, M. C. (2009). Condom use amongst out of school youths in a Local Government Area in Nigeria. African Health Sciences, 9(2), 92–97.
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl & J. Beckman (Eds.), Action-control: From cognition to behavior (pp. 11–39). Heidelberg: Springer.
Ajzen, I. & Fishbein, M. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research. MA: Addison-Wesley.
Albarracín, D., Johnson, B. T., Fishbein, M., & Muellerleile, P. A. (2001). Theories of reasoned action and planned behavior as models of condom use: A meta-analysis. Psychological Bulletin, 127(1), 142–161.
Assefa, N., & Haidar, J. (2013). The utility of theory of planned behaviour in predicting consistent condom use intension of HIV patients on ART in North Shoa Zone health facilities, Ethiopia. Ethiopian Journal of Health Development, 27(1), 40–47.
Beksisnska, M. E., Smit, J. A., & Mantell, J. E. (2012). Progress to male and female condom use in South Africa. Sexual Health, 9(1), 51–58.
Bogart, L. M., Skinner, D., Weinhardt, L. S., Glasman, L., Sitzler, C., Toefy, Y., & Kalichman, S. C. (2011). HIV/AIDS misconceptions may be associated with condom use among black South Africans: An exploratory analysis. African Journal of AIDS Research, 10(2), 181–187.
Bollen, K. A. (1989). Structural equations with latent variables. New York: Wiley.
Buhi, E. R. (2015, November). Effects of an evidence-based positive youth development program on sexual behavior outcomes and intentions among adolescents living in non-metropolitan communities. Presented at the meeting of the American Public Health Association, Chicago, IL.
Calsyn, D. A., Peavy, K. M., Wells, E. A., Campbell, A. N. C., Hatch-Maillette, M. A., Greenfield, S. F., & Tross, S. (2013). Differences between men and women in condom use, attitudes, and skills in substance abuse treatment seekers. The American Journal on Addictions, 22(2), 150–157.
Chialepeh, W. N., & Susuman, A. S. (2015). Risk factors of inconsistent condom use among sexually active youths: Implications for human immunodeficiency virus and sexual risk behaviors in Malawi. Journal of Asian and African Studies. doi:10.1177/0021909615595992
Chimbiri, A. M. (2007). The condom is an ‘intruder’ in marriage: Evidence from rural Malawi. Social Science and Medicine, 64(5), 1102–1115.
Cochran, S. D., & Mays, V. M. (1993). Applying social psychological models to predicting HIV-related sexual risk behaviors among African Americans. Journal of Black Psychology, 19(2), 142–154.
Couture, M., Caron, C. D., & Desrosiers, J. (2010). Leisure activities following a lower limb amputation. Disability and Rehabilitation, 32, 57–64.
Delvaux, T., & Nöstlinger, C. (2007). Reproductive choice for women and men living with HIV: Contraception, abortion and fertility. Reproductive Health Matters, 15(29), 46–66.
Exavery, A., Kanté, A. M., Jackson, E., Noronha, J., Sikustahili, G., Tani, K., … Phillips, J. F. (2012). Role of condom negotiation on condom use among women of reproductive age in three districts in Tanzania. BMC Public Health, 12(1), 1097. doi:10.1186/1471-2458-12-1097
Fearson, E., Wiggins, R. D., Pettifor, A. E., & Hargreaves, J. R. (2015). Is the sexual behavior of young people in sub-Saharan Africa influenced by their peers? A systematic review. Social Science and Medicine, 146, 62–74.
Fehr, S. K., Vidourek, R. A., & King, K. A. (2015). Intra-and inter-personal barriers to condom use among college students: A review of the literature. Sexuality and Culture, 19(1), 103–121.
Heeren, G. A., Jemmott, J. B., III, Mandeya, A., & Tyler, J. C. (2009). Sub-Saharan African university students’ beliefs about condoms, condom-use intention, and subsequent condom use: A prospective study. AIDS and Behavior, 13(2), 268–276.
Hendriksen, E. S., Pettifor, A., Lee, S. J., Coates, T. J., & Rees, H. V. (2007). Predictors of condom use among young adults in South Africa: The reproductive health and HIV research unit national youth survey. American Journal of Public Health, 97(7), 1241–1248.
Idele, P., Gillespie, A., Porth, T., Suzuki, C., Mahy, M., Kasedde, S., & Luo, C. (2014). Epidemiology of HIV and AIDS among adolescents: Current status, inequities, and data gaps. Journal of Acquired Immune Deficiency Syndrome, 66, 144–153.
Katikiro, E., & Njau, B. (2012). Determinant of behavioural change for condom use among out of school youths in Tanzania. Global Journal of Medicine and Public Health, 1(5), 58–63.
Kennedy, S. B., Nolen, S., Applewhite, J., Pan, Z., Shamblen, S., & Vanderhoff, K. J. (2007). A quantitative study on the condom-use behaviors of eighteen-to twenty-four-year-old urban African American males. AIDS Patient Care and STDs, 21(5), 306–320.
Leclerc-Madlala, S. (2002). On the virgin cleansing myth: Gendered bodies, AIDS and ethnomedicine. African Journal of AIDS Research, 1(2), 87–95.
Lule, G. S., & Gruer, L. D. (1991). Sexual behaviour and use of condom among Ugandan students. AIDS Care, 3, 11–19.
Maharaj, P., & Cleland, J. (2005). Risk perception and condom use among married or cohabiting couples in KwaZulu-Natal, South Africa. International Family Planning Perspectives, 31(1), 24–29.
Maticka-Tyndale, E. (2010). Sustainability of gains made in a primary school HIV prevention programme in Kenya into the secondary school years. Journal of Adolescence, 33(4), 563–573.
Maticka-Tyndale, E., Gallant, M., Brouillard-Coyle, C., Holland, D., Metcalfe, K., Wildish, J., & Gichuru, M. (2005). The sexual scripts of Kenyan young people and HIV prevention. Culture, Health and Sexuality, 7(1), 27–41.
Maticka-Tyndale, E., & Kyeremeh, C. (2010). The trouble with condoms: Norms and meanings os sexuality and condom use among school-going youth in Kenya. International Journal of Sexual Health, 22(4), 234–247.
Maticka-Tyndale, E., & Tenkorang, E. Y. (2010). A multi-level model of condom use among male and female upper primary school students in Nyanza, Kenya. Social Science & Medicine, 71(3), 616–625.
Montano, D. E., & Kasprzyk, D. (2015). Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In K. Glanz, B. K. Rimer, & K. Viswanath (Eds.), Health behavior: Theory, research and practice (pp. 95–124). Hoboken, NJ: Wiley.
Musinguzi, G., Bastiaens, H., Matovu, J. K., Nuwaha, F., Mujisha, G., Kiguli, J., … Wanyenze, R. K. (2015). Barriers to condom use among high risk men who have sex with men in Uganda: A qualitative study. PLoS ONE, 10(7), e0132297. doi:10.1371/journal.pone.0132297
National AIDS Control Council. (2015). Kenya’s fast-track plan to end HIV and AIDS among adolescents and young people. Nairobi, Kenya: Author.
National AIDS and STI Control Programme. (2007). Kenya AIDS Indicator Survey Final Report. Nairobi, Kenya: Author.
Njoroge, K. M., Olsson, P., Pertet, A. M., & Ahlberg, B. M. (2010). Voices unheard: Youth and sexuality in the wake of HIV prevention in Kenya. Sexual & Reproductive Healthcare, 1(4), 143–148.
Ochieng, M. A., Kakai, R., & Abok, K. (2011). Knowledge, attitude and practice of condom use among secondary school students in Kisumu district, Nyanza province. Asian Journal of Medical Sciences, 3(1), 32–36.
Oppong, A. K., Osafo, J., & Doku, P. N. (2016). The role of condom use self-efficacy on intended and actual condom use among university students in Ghana. Journal of Community Health, 41(1), 97–104.
Peltzer, K. (2000). Factors affecting condom use among South African university students. East African Medical Journal, 77(1), 46–52.
Peltzer, K. (2003). Knowledge and practice of condom use among black and white South Africans. South African Family Practice Journal, 45(8), 17–20.
Poulin, M. (2010). Reporting on first sexual experience: The importance of interviewer-respondent interaction. Demographic Research, 22(11), 237–288.
Prata, N., Vahidnia, F., & Fraser, A. (2005). Gender and relationship differences in condom use among 15–24 year olds in Angola. International Family Planning Perspectives, 31, 192–199.
Qiao, S., Li, X., & Stanton, B. (2013). Social support and HIV-related risk behaviors: A systematic review of the global literature. AIDS and Behavior, 18(2), 419–441.
Sarkar, N. N. (2008). Barriers to condom use. European Journal of Contraception & Reproductive Health Care, 13(2), 114–122.
Shrestha, R. K., Farnham, P. G., Whitham, H. K., & Sansom, S. L. (2016). Challenges in estimating effectiveness of condom distribution campaigns to prevent HIV transmission. Journal of Acquired Immune Deficiency Syndromes, 73(2), e35–e38. doi:10.1097/QAI.0000000000001124
Taylor, E. D., & Wong, C. A. (1996). Gender differences in the impact of peer influences and peer orientation on African-American adolescents’ school value and academic achievement. Presented at the meeting of the Society for Research on Adolescence, Boston, MA. Retrieved from www.rcgd.isr.umich.edu/garp/articles/taylor96a.pdf
Taylor, M., Jinabhai, C., Dlamini, S., Sathiparsad, R., Eggers, M. S., & De Vries, H. (2014). Effects of a teenage pregnancy prevention program in KwaZulu-Natal, South Africa. Health Care for Women International, 35(7–9), 845–858.
Tenkorang, E. Y. (2014). Perceived vulnerability and HIV testing among youth in Cape Town, South Africa. Health Promotion International, 31, 270–279.
Tenkorang, E. Y., & Maticka-Tyndale, E. (2013). Individual- and school-level correlates of HIV testing among secondary school students in Kenya. Studies in Family Planning, 44(2), 169–187.
Tenkorang, E. Y., & Maticka-Tyndale, E. (2014). Assessing young people’s perceptions of HIV risks in Nyanza, Kenya: Are school and community level factors relevant? Social Science and Medicine, 116, 93–101.
Tenkorang, E. Y., Maticka-Tyndale, E., & Rajulton, F. (2011a). A multi-level analysis of risk perception, poverty and sexual risk-taking among young people in Cape Town, South Africa. Health & Place, 17(2), 525–535.
Tenkorang, E. Y., Obeng-Gyimah, S., Maticka-Tyndale, E., & Adjei, J. (2011b). Superstition, witchcraft and AIDS prevention in sub-Saharan Africa: The case of Ghana. Culture, Health & Sexuality, 13, 1001–1014.
UNAIDS. (2014). The Gap Report-Joint United Nations programme on HIV/AIDS (UNAIDS). Geneva: Author. Retrieved from http://www.stopaidsnow.org/sites/stopaidsnow.org/files/filemanager/UNAIDS_Gap_report_en.pdf
UNICEF. (2015). HIV prevalence in adolescents. Retrieved from http://data.unicef.org/hiv-aids/adolescents-young-people
Van Rossem, R., & Meekers, D. (2011). Perceived social approval and condom use with casual partners among youth in urban Cameroon. BMC Public Health, 11(1), 632.
Volkmann, T., Wagner, K. D., Strathdee, S. A., Semple, S. J., Ompad, D. C., Chavarin, C. V., & Patterson, T. L. (2013). Correlates of self-efficacy for condom use among male clients of female sex workers in Tijuana, Mexico. Archives of Sexual Behavior, 43(4), 719–727.
Waithaka, M. & Bessinger, R. (2001). Sexual behavior and condom use in the context of HIV prevention in Kenya. Population Services International, Kenya. Retrieved from http://pdf.usaid.gov/pdf_docs/PNADA257.pdf
World Health Organization. (1999). Prevention evaluation toolkit. Geneva: Author.
Funding
This study was funded by United States Agency for International Development (USAID).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
ABA declares that she has no conflict of interest. EYT declares that he has no conflict of interest. EMT declares that she has no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Research Ethics Board of the University of Windsor and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Appiah, A.B., Tenkorang, E.Y. & Maticka-Tyndale, E. Modeling Beliefs, Attitudes, and Intentions of Condom Use Among Secondary School Students in Kenya. Arch Sex Behav 46, 1949–1960 (2017). https://doi.org/10.1007/s10508-017-0966-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-017-0966-9