
Abstract
There are over 1.4 million adolescents living with HIV in sub-Saharan Africa, the majority of whom acquired the virus through perinatal transmission (PHIV). HIV stigma is particularly high among adolescents living with HIV and is associated with several outcomes that worsen health and increase the risk of onward HIV transmission. We tested associations between internalized HIV stigma and four of these outcomes over a one-year period among a sample of adolescent boys living with PHIV in Soweto, South Africa. Participants (N = 241) answered questions about internalized HIV stigma at baseline. They completed weekly mobile surveys over the following year to answer questions about their experiences with depression, binge drinking, medication adherence, and violence victimization. Using generalized linear mixed models, we found that baseline internalized HIV stigma was associated with increased odds of depression (OR 1.74), alcohol misuse (OR 2.09), and violence victimization (OR 1.44) and decreased odds of medication adherence (OR 0.60) over the course of a year. These outcomes negatively impact the health and wellbeing of adolescents living with PHIV and increase their risk of transmitting HIV to their partners in the future. Our findings provide novel, longitudinal evidence for the deleterious effects of HIV stigma. To improve health outcomes for adolescents with PHIV, it will be crucial to develop effective HIV stigma reduction interventions that address specific developmental, gendered, and cultural experiences.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
There are over 1.6 million adolescents currently living with HIV, 1.4 million of whom live in sub-Saharan Africa [1]. Most adolescents living with HIV acquired the virus through perinatal transmission (PHIV) [2]. Adolescents living with PHIV face a multitude of challenges. While many of those on antiretroviral therapy (ART) struggle with adherence, those who are not on ART experience significantly higher morbidity and mortality than their HIV-negative peers due to HIV/AIDS-related conditions [3]. Many adolescents with PHIV have lost one or both parents to HIV/AIDS-related conditions, resulting in economic insecurity, housing instability, and significant decline in psychological well-being [4]. In addition to these challenges, adolescents with PHIV are exposed to discriminatory and stigmatizing beliefs about HIV that weaken their social relationships, self-esteem, and ability to manage their HIV [5].
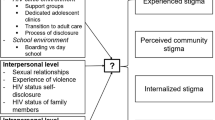
HIV stigma has been identified as a pervasive challenge to the health and wellbeing of people living with HIV [5, 6]. Internalized stigma occurs when a person with HIV is exposed to negative beliefs about HIV and incorporates those beliefs into their self-concept [7]. People with internalized stigma may report feeling guilt, shame, and worthlessness due to being HIV-positive [8]. Internalized HIV stigma is common: in a survey study of over 10,000 South Africans living with HIV, approximately 43% of respondents reported some internalized HIV stigma, with the highest levels among young adults 15–24 [9]. Adolescents may experience increased internalized HIV stigma because they are still developing an understanding of what their HIV diagnosis means, because they are particularly sensitive to the ways in which HIV treatment (e.g., clinic appointments, taking medications) differentiates them from their peers, and because they experience additional social stigma from having a parent who also has HIV [9,10,11]. Moreover, internalized HIV stigma directly and indirectly affects physical and psychological health, including several outcomes that shape the wellbeing of PHIV adolescents [12, 13].
In samples of adolescents and adults in sub-Saharan Africa, internalized HIV stigma has been associated with higher levels of depression, and with risky behaviors like inconsistent condom use mediated through depression [14, 15]. Similar studies have established links between internalized HIV stigma and alcohol misuse in adults and between internalized HIV stigma and medication adherence among adolescents [10, 16, 17]. These behaviors are critical in part because they increase the risk of onward HIV transmission.
There may also be a link between internalized HIV stigma and violence victimization, including bullying from peers and intimate partner violence, though the direction of these associations is unclear [18, 19]. Adolescents with PHIV may experience violence after disclosing their HIV status, exacerbating internalized stigma. Alternatively, high internalized stigma may weaken self-esteem and social support, leading an adolescent with PHIV to expect and accept abusive treatment and leaving them vulnerable to further violence. Violence victimization is associated with unsuppressed viral load, depression, and increased risk of sexually transmitted infections [20,21,22]. Therefore, confirming this association between stigma and victimization has important implications for PHIV treatment outcomes.
Much of the existing research on HIV stigma has been conducted among adults living with HIV. Adolescence is a developmental period characterized by risk taking (e.g., binge drinking [23]), the emergence of mental health disorders (e.g., depression [24]) and experiences of victimization (e.g., intimate partner violence, bullying, and domestic abuse [25]). Much of the internalized HIV stigma work has been cross-sectional [26] and has not focused on adolescents. Longitudinal studies can provide evidence for temporal ordering and causal relationships between these constructs. Clarifying longitudinal associations can inform interventions to reduce HIV stigma and its sequalae, thereby improving the wellbeing of adolescents with PHIV and preventing secondary transmission. The present study seeks to test if internalized HIV stigma is associated with four important outcomes (depression, alcohol misuse, medication adherence, violence victimization) over a one-year period among a sample of adolescent boys living with PHIV in South Africa.
Methods
Study Setting
This study took place in Soweto, South Africa. Soweto, a township of Johannesburg, was originally developed under apartheid to segregate Black Africans and later became a site of protest and resistance against the apartheid government. Approximately 13% of the 5.3 million people living in Johannesburg are living with HIV [27]. Globally, South Africa has the largest number of people living with HIV and the largest number of adolescents and young adults living with HIV [1, 28].
Participant Recruitment and Data Collection
Data collection occurred between November 2020 and June 2023. Participants were eligible if they were between 15 and 19 years old and identified as male, living in Soweto, in a current dating or sexual relationship, and with a history of HIV before age ten, indicating a likely perinatally-acquired infection. Study recruiters approached eligible patients at public HIV care clinics. Those interested visited the Perinatal HIV Research Unit, affiliated with the University of the Witwatersrand, for screening. Adolescents completed informed consent or assent procedures; caregivers also provided informed consent for those under age 18. Once enrolled, participants completed a baseline survey in the clinic and returned home with a smartphone to complete weekly mobile surveys. They received a prompt to complete the mobile survey each week for one year. Participants were able to communicate with the study team through WhatsApp or a 24-hour hotline. In addition, responses associated with potential psychological risks (e.g., suicidality) triggered an email to the team. In such cases, a counselor reached out to assess the participant and, if needed, provide referrals for additional care. IRB approval was obtained by the University of the Witwatersrand in South Africa and by Stony Brook University in the United States.
Measures
Stigma
HIV stigma was measured at baseline with an adapted version of the Internalized AIDS-Related Stigma Scale [8]. This scale was developed and validated using data from participants in South Africa, Swaziland, and the United States and has been validated in samples from other low- and middle- income countries including Tanzania, Uganda, and India [29,30,31]. Participants rated their agreement with six statements (e.g., “I am ashamed that I am HIV positive”) from the scale. Upon the suggestion of the clinic staff, who work directly with the participants, we added a seventh item to capture feelings of anger at being HIV positive. The number of endorsed statements were summed to create a total score (0–7; Cronbach’s alpha = 0.7).
Outcome Variables
All outcome variables were assessed at each weekly survey and coded dichotomously. To capture depression, we used a single item from the Screening Tool for Psychological Distress (STOP-D [32]). This scale has been validated in Canadian and Brazilian contexts [33, 34]. Participants were asked: “In the past 24 hours, how much have you been bothered by feeling sad, down, or uninterested in life?” Participants who indicated that they were “moderately” or “severely” bothered were categorized as experiencing possible depression.
To measure binge drinking, participants were asked: “In the past 24 hours, how many alcoholic drinks did you have?” Participants who reported consuming four or more alcoholic drinks in the previous 24 h were categorized as engaging in binge drinking.
To measure medication adherence, participants were asked: “In the past 24 hours, how did you do taking your HIV medicines?” Participants who reported taking all of their pills were categorized as adherent.
To measure violence victimization, participants were asked three questions assessing their experiences with physical (e.g., being choked), sexual (e.g., experiencing forced sex), and emotional (e.g., being threatened) victimization over the past week. Participants who endorsed at least one form of violence victimization were identified as experiencing violence.
Analyses
Descriptive statistics are presented to describe the sociodemographic characteristics of the study sample and to characterize the study variables. The outcome measures were assessed at each survey with a dichotomous (yes/no) question. Descriptive statistics for these outcomes are averaged across surveys nested within participants, so that the mean reflects the proportion of surveys in which the outcome is present.
To account for the nested structure of the survey data, we use logistic mixed effects models, which allow for fixed and random effects within each model [35]. Baseline HIV stigma (z-score transformed) was entered as a predictor into four separate multivariate models – one for each hypothesized outcome. All models control for participant age (continuous) and survey week (continuous). To reduce error and maximize generalizability, all models also include a random intercept at the participant level and a random slope for HIV stigma [36].
Results
The analytic sample for this study consists of the 241 adolescent boys with PHIV who completed the baseline survey and at least one of the weekly follow-up surveys. The majority (91%) of participants were Black African and the mean age was 16.5 years old. On average, participants completed 28.5 of the 52 weekly follow-up surveys (total observations (O) = 6,870). Participants’ average score on the adapted internalized HIV stigma measure was 3.68 (SD = 1.78; for the standard six-item scale, M = 3.16, SD = 1.51). There were no significant differences in baseline HIV stigma by survey completion rate (i.e., participants who completed less than half of the 52 weekly surveys compared to participants who completed more than half). Table 1 contains full sociodemographic information for the sample.
Many participants reported depression (N = 134), binge alcohol drinking (N = 104), medication nonadherence (N = 137), and violence victimization (N = 166) in at least one of their weekly surveys. However, these participants did not report these events frequently. Calculating intraindividual means (i.e., averaging across surveys within participants and then across participants), found low levels of depression (M = 0.11, O = 6,840), alcohol misuse (M = 0.06, O = 6,846), and violence victimization (M = 0.13, O = 6,723) and moderate levels of medication adherence (M = 0.83, O = 6,624). Participant-level descriptive statistics for the outcome variables are presented in Table 2. The intraclass correlation (ICC) calculates the ratio of between-person variance to total variance in each outcome. The ICCs in Table 2 indicate remaining unexplained variance; for instance, 49% of the total variance in depression is at the between-person level, so the remaining 51% is a combination of within-person variance and error. The ICCs suggest that our outcomes did vary within participants over time, confirming their appropriateness for mixed effects models.
Table 3 contains the adjusted odds ratios and 95% confidence intervals for the effect of HIV stigma on each outcome of interest. As hypothesized, internalized HIV stigma significantly increased the odds of experiencing depression over the course of the study (OR 1.74 per 1 SD unit increase in HIV stigma at baseline; 95% CI: 1.29, 2.36). Similarly, internalized HIV stigma significantly increased the odds of reporting alcohol misuse over the course of the study (OR 2.09, 95% CI: 1.48, 2.96). Internalized HIV stigma significantly decreased the odds of medication adherence over time (OR 0.60, 95% CI: 0.39, 0.92). Finally, internalized HIV stigma significantly increased the odds of reporting violence victimization over time (OR 1.44, 95% CI: 1.15, 1.81).
Discussion
In this study of adolescent boys with PHIV, we found that internalized HIV stigma was associated with several important health outcomes. In line with previous HIV stigma work, we confirmed that internalized HIV stigma decreased medication adherence and increased depression and binge drinking. This study adds new, longitudinal evidence for the temporal order of these events. We also identified a novel association between internalized HIV stigma and violence victimization. These findings highlight stigma as a critical contributor to health and have important implications for future research and intervention.
First, we found moderate levels of internalized HIV stigma in this sample (M = 3.68 for the seven-item adapted measure; M = 3.16 for the standard six-item measure). Compared to other research using the same measure, the scores in this sample are higher than those collected among adults in South Africa (M = 3.0) [8], Uganda (M = 2.06), and Tanzania (M = 2.35) [29] and among adolescents in Uganda (M = 2.58) [37]. Our findings are in line with previous studies, which have found moderate to high levels of internalized HIV stigma among South African adolescents with HIV [6, 9]. Moreover, 98% of our sample endorsed at least one of the seven HIV stigma items, confirming again that internalized stigma is a common experience among adolescents with PHIV.
Second, we found that internalized HIV stigma significantly predicted mental health and heath behaviors over time. Our findings align with prior work and underscore the need to prioritize HIV stigma research and intervention among the vulnerable group of adolescents born with HIV [5, 6]. Specifically, in this sample, internalized HIV stigma increased the odds of depression over time. A recent review of the literature on HIV stigma and depression concluded that these constructs were related to each other, but that a lack of longitudinal designs prevented understanding the direction or mechanism of the association [14]. This study – using repeat, longitudinal measures – adds new evidence in support of a causal association between HIV stigma and depression. Beyond the emotional and cognitive burden, depression reduces treatment adherence and may even increase viral load independently of adherence [38, 39]. Adolescents with PHIV would likely benefit (mentally and physically) from increased depression screening and comprehensive mental health care that includes stigma as an important component of mental health.
Internalized stigma also affected two important health behaviors: binge drinking and medication adherence. Stigma can shape behavioral outcomes through maladaptive and avoidant coping. Specifically, the stress and discomfort of internalized stigma may lead to self-medication with alcohol [16]. Similarly, people living with HIV may avoid taking their medication if other people are around to witness it, which may be particularly challenging for adolescents who are busy with school and extracurricular activities [40]. This study confirms again the association between stigma and these health behaviors. Moreover, higher levels of baseline stigma were associated with higher odds of maladaptive behavior over a one-year period, suggesting that internalized stigma has a lasting impact. It is possible that participants had stable levels of internalized stigma, or that internalized stigma sparked negative coping behaviors that quickly became habitual. Future research should test how soon a reduction in stigma results in an associated reduction of maladaptive behavior. Given the importance of these health behaviors for HIV maintenance and secondary transmission (e.g., risky sex [41]), HIV care clinics should provide patients with information about the role of coping and suggestions for specific coping behaviors.
This study also found that internalized HIV stigma predicted later violence victimization. Previous research has identified cross-sectional associations between stigma and victimization and has tested victimization as a predictor of stigma [18, 19]. Our findings suggest that stigma may affect later victimization, indicating a bidirectional relationship between the two constructs. HIV stigma may increase vulnerability to violence, particularly among adolescents, by reducing their self-esteem and social support, leading them to expect maltreatment and isolating them from close others who could intervene in the abuse [42, 43]. This is especially critical for adolescents with PHIV, as having a parent experience HIV/AIDS-related illness and death is already associated with increased social stigma and abuse [44]. Violence against adolescent boys is typically underreported due to threats and coercion from perpetrators, a lack of social support, and shame surrounding victimization [45]. This potentially creates a negative cycle in which internalized stigma increases vulnerability to violence victimization, while victimization increases feelings of shame and isolation that exacerbate stigma. Future research should seek to better conceptualize the link between stigma and victimization and identify interventions to break the feedback loop between them. This could include more frequent screenings for mental health problems and victimization, embedding social workers in clinical settings, and reducing bias at the community level against people living with HIV and victims of violence.
Community-level norms and attitudes are important to consider in contextualizing these findings and identifying appropriate interventions. Compared to other areas in sub-Saharan Africa, alcohol use is particularly high among men in Soweto [46]. Most adolescents in Soweto have already tried alcohol, and witnessing and experiencing violence is significantly associated with alcohol use [47]. Relatedly, two-thirds of adolescents in Soweto have witnessed violence in their community [47, 48]. Exposure to violence early in life may normalize violent behavior, making it more difficult to recognize as a problem, and may increase vulnerability to victimization later in life [49]. Further, boys and men in South Africa report feeling that the typical resources for victims of violence, including the police and clinicians, are biased against male victims [50, 51]. This bias is present even in South African policies on violence, which typically do not include men when defining who is vulnerable to violence [52]. These experiences likely intersect with experiences of discrimination against people living with HIV, which are also common [53, 54]. Therefore, interventions are necessary at the community and national level. This includes providing comprehensive education about HIV in educational and clinical settings, developing support groups for adolescents struggling with alcohol use [55], and creating and advertising resources specifically for boys and men experiencing violence. Educational content transmitted through television and social media may also work to change adolescent knowledge and attitudes, and researchers should consider incorporating modern forms of media in their intervention work [56].
There are few existing interventions designed to address internalized HIV stigma. Even fewer have been developed and tested among adolescents [57]. Interventions to combat internalized HIV stigma are necessary in clinical, educational, and community settings. Research among adults with HIV in high-income countries has found that effective interventions are typically multi-session programs grounded in behavior change theory and guided by trained counselors, with educational content about HIV and support for strengthening coping behaviors [58,59,60,61]. Future intervention work should build on these findings while incorporating the unique needs and experiences of adolescents and South African cultural contexts. Beyond targeted programming, clinicians should also consider screening for internalized HIV stigma and providing brief psychoeducation to patients with high stigma levels. Clinicians and social workers could also consider recruiting patients with high internalized stigma into support groups where they can discuss their experiences with each other, which can reduce stigma over time [62]. Because internalized HIV stigma stems from exposure to negative attitudes toward people with HIV, broader social awareness campaigns that correct myths and stereotypes about people with HIV may also indirectly decrease internalized stigma [63].
One strength of the current study is the longitudinal design, which allows us to make inferences about HIV stigma as a predictor of health outcomes over time. Although some of these associations are well established in cross-sectional survey studies, they are rarely tested longitudinally. Identifying HIV stigma as an antecedent of behavioral health outcomes creates opportunities for new interventions to improve the wellbeing of PHIV adolescents. Additionally, this study focused on an important, but underserved, population. Adolescents living with HIV report higher levels of internalized stigma than adults with HIV [9]. They are also at a critical point developmentally – they are beginning to engage in sexual relationships, experimenting with substance use, and beginning to manage their HIV independently [5, 64]. Identifying ways to reduce stigma in this population has crucial implications for improving the health of individuals with PHIV and decreasing the risk of secondary transmission. A limitation of the current study is that the study population was recruited from HIV clinics, therefore these findings may not reflect the experiences of adolescents with PHIV who are not clinically engaged. As stigma may deter adolescents from seeking care, it is possible that stigma is much higher in the general population of adolescents with PHIV. Similarly, these findings may not generalize to adolescents living with non-perinatally acquired HIV, whose behavior and sociodemographic characteristics may differ from adolescents with PHIV [65, 66].
Our findings identify internalized HIV stigma as a deleterious influence on behavioral health and wellbeing over time among adolescents with PHIV. As the prevalence of HIV among South African adolescents continues to increase, so does the need for targeted interventions that improve treatment adherence and strengthen wellbeing in this population [67, 68]. Specifically addressing internalized HIV stigma in educational and clinical contexts has the potential to improve the long-term outcomes for this generation of individuals with PHIV and reduce further transmission.
References
UNICEF, Adolescent HIV. prevention. 2023; https://data.unicef.org/topic/hivaids/adolescents-young-people/.
UNAIDS. A Progress Report: All in to End the Adolescent AIDS Epidemic. 2016. Geneva, Switzerland 2016.
Lowenthal ED, Bakeera-Kitaka S, Marukutira T, Chapman J, Goldrath K, Ferrand RA. Perinatally acquired HIV infection in adolescents from Sub-saharan Africa: a review of emerging challenges. Lancet Infect Dis Jul. 2014;14(7):627–39.
Nabunya P, Ssewamala FM. The effects of parental loss on the psychosocial wellbeing of AIDS-orphaned children living in AIDS-impacted communities: does gender matter? Child Youth Serv Rev Aug. 2014;1:43:131–7.
Woollett N. Adolescents living with HIV: emerging issues in public health in South Africa. In: Liamputtong P, editor. Children and Young People Living with HIV/AIDS: a cross-cultural perspective. Springer; 2016. pp. 65–88.
Pantelic M, Boyes M, Cluver L, Meinck F. HIV, violence, blame and shame: pathways of risk to internalized HIV stigma among South African adolescents living with HIV. J Int AIDS Soc Aug. 2017;21(1):21771.
Lee R, Kochman A, Sikkema KJ. Internalized stigma among people living with HIV-AIDS. AIDS Behav. 2002;6(4):309–19.
Kalichman SC, Simbayi LC, Cloete A, Mthembu PP, Mkhonta RN, Ginindza T. Measuring AIDS stigmas in people living with HIV/AIDS: the internalized AIDS-Related Stigma Scale. AIDS Care Jan. 2009;21(1):87–93.
SANAC. The people living with HIV stigma index: South Africa 2014. Pretoria: South African National AIDS Council; 2015.
Madiba S, Josiah U. Perceived stigma and fear of unintended disclosure are barriers in medication adherence in adolescents with perinatal HIV in Botswana: A qualitative study. BioMed Research International. 2019;2019.
Earnshaw VA, Bogart LM, Courtney I, et al. Exploring treatment needs and expectations for people living with HIV in South Africa: a qualitative study. AIDS Behav Aug. 2018;22(8):2543–52.
Earnshaw VA, Bogart LM, Laurenceau JP, et al. Internalized HIV stigma, ART initiation and HIV-1 RNA suppression in South Africa: exploring avoidant coping as a longitudinal mediator. J Int AIDS Soc Oct. 2018;21(10):e25198.
Lyimo RA, Stutterheim SE, Hospers HJ, de Glee T, van der Ven A, de Bruin M. Stigma, disclosure, coping, and medication adherence among people living with HIV/AIDS in Northern Tanzania. AIDS Patient Care STDs. 2014;28(2):98–105.
MacLean JR, Wetherall K. The association between HIV-stigma and depressive symptoms among people living with HIV/AIDS: a systematic review of studies conducted in South Africa. J Affect Disord. 2021;287:125–37.
Nduna M, Jewkes RK, Dunkle KL, Shai NP, Colman I. Associations between depressive symptoms, sexual behaviour and relationship characteristics: a prospective cohort study of young women and men in the Eastern Cape, South Africa. J Int AIDS Soc Nov. 2010;15:13:44.
Wardell JD, Shuper PA, Rourke SB, Hendershot CS. Stigma, coping, and alcohol use severity among people living with HIV: a prospective analysis of bidirectional and mediated associations. Ann Behav Med Aug. 2018;16(9):762–72.
Masa R, Zimba M, Tamta M, Zimba G, Zulu G. The association of perceived, internalized, and enacted HIV stigma with medication adherence, barriers to adherence, and mental health among young people living with HIV in Zambia. Stig Health. 2022;7(4):443–53.
Boyes ME, Pantelic M, Casale M, Toska E, Newnham E, Cluver LD. Prospective associations between bullying victimisation, internalised stigma, and mental health in South African adolescents living with HIV. J Affect Disord. 2020;276:418–23.
Matseke G, Rodriguez VJ, Peltzer K, Jones D. Intimate partner violence among HIV positive pregnant women in South Africa. J Psychol Afr. 2016;26(3):259–66.
Merrill KG, Campbell JC, Decker MR, et al. Past-year violence victimization is associated with viral load failure among HIV-positive adolescents and young adults. AIDS Behav. 2021;25(5):1373–83.
Boyes ME, Cluver LD. Relationships between familial HIV/AIDS and symptoms of anxiety and depression: the mediating effect of bullying victimization in a prospective sample of South African children and adolescents. J Youth Adolesc. 2015;44(4):847–59.
O’Leary A, Jemmott JB III, Jemmott LS, et al. Associations between psychosocial factors and incidence of sexually transmitted disease among South African adolescents. Sex Transm Dis. 2015;42(3):135–9.
Ma C, Bovet P, Yang L, Zhao M, Liang Y, Xi B. Alcohol use among young adolescents in low-income and middle-income countries: a population-based study. Lancet Child Adolesc Health. 2018;2(6):415–29.
Solmi M, Radua J, Olivola M, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27(1):281–95.
Le MT, Holton S, Romero L, Fisher J. Polyvictimization among children and adolescents in low-and lower-middle-income countries: a systematic review and meta-analysis. Trauma Violence Abuse. 2018;19(3):323–42.
Earnshaw VA, Kidman RC, Violari A. Stigma, depression, and substance use problems among perinatally HIV-infected youth in South Africa. AIDS Behav Dec. 2018;22(12):3892–6.
Johannesburg Co. City of Johannesburg profile on the HIV epidemic: Trends to accelerate progress of HIV response 2020.
Zuma K, Simbayi L, Zungu N et al. The HIV Epidemic in South Africa: key findings from 2017 national population-based survey. Int J Environ Res Public Health 2022;19(13).
Geibel S, Gottert A, Friedland BA, et al. Internalized stigma among people living with HIV: assessing the internalized AIDS-Related Stigma Scale in four countries. AIDS. Volume 34. LWW; 2020. pp. S33–41.
Chan BT, Pradeep A, Chandrasekaran E, et al. Reliability, validity, and factor structure of the internalized AIDS-Related Stigma Scale in southern India. J Int Assoc Provid AIDS Care. 2019;18:2325958219831025.
Tsai AC, Weiser SD, Steward WT, et al. Evidence for the reliability and validity of the internalized AIDS-related Stigma Scale in rural Uganda. AIDS Behav. 2013;17:427–33.
Young Q-R, Ignaszewski A, Fofonoff D, Kaan A. Brief screen to identify 5 of the most common forms of psychosocial distress in cardiac patients: validation of the Screening Tool for Psychological Distress. J Cardiovasc Nurs. 2007;22(6):525–34.
Young Q-R, Nguyen M, Roth S, Broadberry A, Mackay MH. Single-item measures for depression and anxiety: validation of the Screening Tool for Psychological Distress in an inpatient cardiology setting. Eur J Cardiovasc Nurs. 2015;14(6):544–51.
Gontijo IBR, Souza JR, Barbosa DF, Rassi S. Validation of the Brazilian version of the Screening Tool for Psychosocial Distress (STOP-D) for cardiac patients. Int J Cardiovasc Sci. 2019;32:438–46.
Diez-Roux AV. Multilevel analysis in public health research. Annu Rev Public Health. 2000;21(1):171–92.
Barr DJ, Levy R, Scheepers C, Tily HJ. Random effects structure for confirmatory hypothesis testing: keep it maximal. J Mem Lang. 2013;68(3):255–78.
Ashaba S, Cooper-Vince C, Maling S, Rukundo GZ, Akena D, Tsai AC. Internalized HIV stigma, bullying, major depressive disorder, and high-risk suicidality among HIV-positive adolescents in rural Uganda. Glob Ment Health. 2018;5:e22.
Gonzalez JS, Batchelder AW, Psaros C, Safren SA. Depression and HIV/AIDS treatment nonadherence: a review and meta-analysis. J Acquir Immune Defic Syndr. 2011;58(2).
Meffert S, Neylan T, McCulloch C, et al. East African HIV care: Depression and HIV outcomes. Glob Ment Health. 2019;6:e9.
Kalichman SC, Mathews C, Banas E, Kalichman MO. Treatment adherence in HIV stigmatized environments in South Africa: stigma avoidance and medication management. Int J STD AIDS. 2019;30(4):362–70.
Gerbi GB, Habtemariam T, Tameru B, Nganwa D, Robnett V. The correlation between alcohol consumption and risky sexual behaviours among people living with HIV/AIDS. J Subst Use. 2009;14(2):90–100.
Small LA, Huynh AK, Parchment TM. The association between self-esteem, stigma, and mental health among South African youth living with HIV: the need for integrated HIV care services. AIDS Care. 2022;34(1):86–94.
Takada S, Weiser SD, Kumbakumba E, et al. The dynamic relationship between social support and HIV-related stigma in rural Uganda. Ann Behav Med. 2014;48(1):26–37.
Cluver L, Orkin M, Boyes ME, Sherr L, Makasi D, Nikelo J. Pathways from parental AIDS to child psychological, educational and sexual risk: developing an empirically-based interactive theoretical model. Soc Sci Med. 2013;87:185–93.
Blackburn K, Grubb LK, Vargas G. Sexual violence experiences among adolescent and young adult males: a review to empower healthcare providers. Curr Opin Pediatr. 2022;34(4):297–305.
Boua PR, Soo CC, Debpuur C, et al. Prevalence and socio-demographic correlates of tobacco and alcohol use in four sub-saharan African countries: a cross-sectional study of middle-aged adults. BMC Public Health. 2021;21(1):1126.
Otwombe KN, Dietrich J, Sikkema KJ, et al. Exposure to and experiences of violence among adolescents in lower socio-economic groups in Johannesburg, South Africa. BMC Public Health. 2015;15(1):1–11.
Magidson JF, Dietrich J, Otwombe KN, Sikkema KJ, Katz IT, Gray GE. Psychosocial correlates of alcohol and other substance use among low-income adolescents in peri-urban Johannesburg, South Africa: a focus on gender differences. J Health Psychol. 2017;22(11):1415–25.
Spriggs AL, Halpern CT, Martin SL. Continuity of adolescent and early adult partner violence victimisation: Association with witnessing violent crime in adolescence. J Epidemiol Community Health. 2009;63(9):741–8.
Kgatle MO, Mafa P. Absent voices: help-seeking behaviour among South African male victims of intimate partner violence. Technium Soc Sci J. 2021;24:717.
Majola KB, Mkhize SM, Udoh JA. Gender-based violence: sociocultural barriers to men speaking up and seeking help in South Africa. Afr J Gend Soc Dev. 2023;12(1):27.
Van Niekerk A, Tonsing S, Seedat M, Jacobs R, Ratele K, McClure R. The invisibility of men in South African violence prevention policy: National prioritization, male vulnerability, and framing prevention. Global Health Action. 2015;8(1):27649.
Maughan-Brown BG. Attitudes towards people with HIV/AIDS: Stigma and its determinants amongst young adults in Cape Town, South Africa. S Afr Rev Sociol. 2006;37(2):165–88.
Ndinda C, Chimbwete C, Mcgrath N, Pool R, Group M. Community attitudes towards individuals living with HIV in rural KwaZulu-Natal, South Africa. AIDS Care. 2007;19(1):92–101.
Morojele NK, Ramsoomar L. Addressing adolescent alcohol use in South Africa. S Afr Med J. 2016;106(6):551–3.
Shamu S, Khupakonke S, Farirai T, et al. Knowledge, attitudes and practices of young adults towards HIV prevention: an analysis of baseline data from a community-based HIV prevention intervention study in two high HIV burden districts, South Africa. BMC Public Health. 2020;20:1–10.
Andersson GZ, Reinius M, Eriksson LE, et al. Stigma reduction interventions in people living with HIV to improve health-related quality of life. Lancet HIV. 2020;7(2):e129–40.
Harper GW, Lemos D, Hosek SG, Interventions AMTNHA. Stigma reduction in adolescents and young adults newly diagnosed with HIV: findings from the Project ACCEPT intervention. AIDS Patient Care STDs. 2014;28(10):543–54.
Yigit I, Modi RA, Weiser SD et al. Effects of an intervention on internalized HIV-related stigma for individuals newly entering HIV care. AIDS. Vol 34: LWW; 2020:S73-S82.
Tshabalala J, Visser M. Developing a cognitive behavioural therapy model to assist women to deal with HIV and stigma. S Afr J Psychol. 2011;41(1):17–28.
Rao D, Desmond M, Andrasik M, et al. Feasibility, acceptability, and preliminary efficacy of the unity workshop: an internalized stigma reduction intervention for African American women living with HIV. AIDS Patient Care STDs. 2012;26(10):614–20.
Bauermeister J, Muessig K, LeGrand S, et al. HIV and sexuality stigma reduction through engagement in online forums: results from the HealthMPowerment intervention. AIDS Behav. 2019;23:742–52.
Watt MH, Minja L, Knettel BA, et al. Pilot outcomes of Maisha: an HIV stigma reduction intervention developed for antenatal care in Tanzania. AIDS Behav. 2021;25:1171–84.
Folayan MO, Odetoyinbo M, Brown B, Harrison A. Addressing the socio-development needs of adolescents living with HIV/AIDS in Nigeria: a call for action: perspectives paper. Afr J Reprod Health. 2014;18(1):93–101.
Tsondai PR, Davies MA, Singtoroj T, et al. Improving methods to classify perinatal versus nonperinatal HIV acquisition in young adolescents 10–14 years of age. Pediatr Infect Dis J. 2021;40(5):453–6.
Weijsenfeld AM, Smit C, Wit FW et al. Long-term virological treatment outcomes in adolescents and young adults with perinatally and non-perinatally acquired human immunodeficiency virus. Paper presented at: Open Forum Infectious Diseases. 2022.
Mabaso M, Maseko G, Sewpaul R, et al. Trends and correlates of HIV prevalence among adolescents in South Africa: evidence from the 2008, 2012 and 2017 South African National HIV prevalence, incidence and behaviour surveys. AIDS Res Ther. 2021;18(1):97.
Inbarani N, Sinovuyo T, Ronel S, et al. Past and current status of adolescents living with HIV in South Africa, 2005–2017. BMC Res Notes. 2022;15(1):132.
Acknowledgements
The authors would like to thank the members of the study staff at PHRU, including Candice Ramsammy and Phumla Madi. We would also like to thank all participants for their time and effort in this study.
Funding
Research reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number R01MH119878. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
Conceptualization: EI, AV and RK; Methodology: AV and RK; Data analysis: EI; Writing - original draft preparation: EI; Writing - review and editing: BND, AV, and RK; Funding acquisition: AV and RK.
Corresponding author
Ethics declarations
Ethics Approval
was obtained from the ethics committee of the University of the Witwatersrand in South Africa and by Stony Brook University in the United States. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Conflicts of Interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Inman, E.M., Nkala-Dlamini, B., Violari, A. et al. HIV Stigma, Health, and Violence: A Longitudinal Study among Adolescent Boys with HIV in Soweto, South Africa. AIDS Behav (2024). https://doi.org/10.1007/s10461-024-04407-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s10461-024-04407-x