
Abstract
Substance use disorder (SUD), a common comorbidity among people with HIV (PWH), adversely affects HIV clinical outcomes and HIV-related comorbidities. However, less is known about the incidence of different chronic conditions, changes in overall comorbidity burden, and health care utilization by SUD status and patterns among PWH in Florida, an area disproportionately affected by the HIV epidemic. We used electronic health records (EHR) from a large southeastern US consortium, the OneFlorida + clinical research data network. We identified a cohort of PWH with 3 + years of EHRs after the first visit with HIV diagnosis. International Classification of Diseases (ICD) codes were used to identify SUD and comorbidity conditions listed in the Charlson comorbidity index (CCI). A total of 42,271 PWH were included (mean age 44.5, 52% Black, 45% female). The prevalence SUD among PWH was 45.1%. Having a SUD diagnosis among PWH was associated with a higher incidence for most of the conditions listed on the CCI and faster increase in CCI score overtime (rate ratio = 1.45, 95%CI 1.42, 1.49). SUD in PWH was associated with a higher mean number of any care visits (21.7 vs. 14.8) and more frequent emergency department (ED, 3.5 vs. 2.0) and inpatient (8.5 vs. 24.5) visits compared to those without SUD. SUD among PWH was associated with a higher comorbidity burden and more frequent ED and inpatient visits than PWH without a diagnosis of SUD. The high SUD prevalence and comorbidity burden call for improved SUD screening, treatment, and integrated care among PWH.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Substance use and substance use disorders (SUD) are common among persons with HIV (PWH) [1,2,3]. It has been estimated that 45–70% of PWH smoke tobacco, substantively higher than the proportion (∼ 16%) among the general population [3, 4]. An analysis of data from the Center for AIDS Research Network of Integrated Clinical Systems (CNICS), a multi-site electronic health record (EHR)-based clinical cohort of PWH in the United States (US), revealed that almost half of PWH have been diagnosed with at least one substance use disorder [5]. Cannabis, alcohol, and stimulant use are the top three most common substance use disorders, and previous studies have shown that approximately 20% of PWH have polysubstance use disorder (i.e., having more than one SUD) [5]. Substance use has been associated with a wide range of comorbidities [6,7,8,9] and increased risk of hospitalization and Emergency Department (ED) visits [10].
Advances in HIV antiretroviral therapy (ART) have transformed HIV infection into a manageable chronic condition and helped achieve longer life expectancies for PWH [11]. With increased life expectancy, an increased prevalence of aging-related comorbidities has been observed among PWH [12, 13]. Yang et al. used electronic health record (EHR) data to compare the comorbidity burden before and after HIV diagnosis [14]. Among all included predictors, tobacco use had the strongest association with increased comorbidity; alcohol, cocaine, and cannabis use were also top predictors. Aging, HIV, SUD, multimorbidity, and higher treatment burden could have synergistic interactions with one another making individuals more susceptible to adverse clinical outcomes [15,16,17].
Care visit frequencies have been associated with overall comorbidity burdens and could supplement the comorbidity index to represent patterns in healthcare resource utilization [18, 19]. Frequent hospitalization and ED visits have been associated with complex health needs, high treatment burdens, and high healthcare costs [20,21,22]. Past studies have compared comorbidity risk, emergency department visit, and hospitalization frequency by substance use or use disorder status in both clinical [23, 24] and community settings [25, 26]. However, there are a lack of studies conducting these comparisons in PWH, especially for individuals with multimorbidity, defined as ≥ 2 concurrent chronic conditions [27] and for PWH living in Florida, an epicenter of the HIV epidemic in the US. Examining the comorbidity burden and healthcare utilization patterns using real-world clinical data can provide actionable insights to developing and implementing high-impact care delivery and management strategies that bridge the substance use treatment gaps for PWH in Florida, and ultimately accelerate progress along the HIV care continuum in a region disproportionately affected by the HIV epidemic.
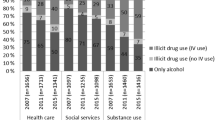
Additionally, people with SUD are heterogeneous with different SUD types and combinations [25, 28, 29]. The use of different psychoactive substances is associated with varied mechanisms of action, levels of social marginalization or stigma, legal consequences, and risk of polysubstance use [28,29,30,31] which may, directly and indirectly, impact the comorbidity risk and healthcare utilization. A latent class analysis of a community sample in Florida has identified three main substance use patterns: tobacco use only, alcohol, marijuana, or tobacco use, and any use of stimulants, opioids, and other illicit substances [25]. Other research among PWH provides supporting evidence for this SUD pattern classification [3, 32, 33]. However, less is known regarding the comorbidity and care visit variations across people with different SUD patterns.
To address the public health needs and literature gap listed above, the presented work (1) estimates the prevalence of diagnosed SUD, polySUDs, and SUD patterns among PWH in Florida using statewide, integrated EHR and claims data, and (2) employees a longitudinal study design to test our hypothesis that having a SUD diagnosis is associated with an overall higher comorbidity burden, more inpatient visits, and more ED visits than in PWH without a SUD diagnosis. Additionally, we assess differences in the progression of chronic comorbidity accumulation and healthcare utilization characteristics by SUD patterns.
Methods
Data Source
We used EHR and administrative claims data from the OneFlorida + Clinical Data Research Network (OneFL) which includes EHR data from ten health systems across Florida linked to statewide claims from Medicaid and Medicare. OneFL comprises longitudinal health data from 17.2 million unique patients who received care in Florida between January 2012 to March 2021 [34]. It has been estimated that OneFL partners serve 40–50% of Florida’s population, and the sociodemographic characteristics of the OneFL sample resemble the total Florida population [34]. The study was approved by the University of Florida Institutional Review Board (IRB202002581).
Identification of the HIV Cohort
Within OneFL, we previously developed and validated a computable phenotype algorithm to identify PWH [35]. The algorithm screens patient’s medical records and identifies PWH if they had at least one HIV diagnostic code plus at least one of the following: (1) had at least one positive HIV laboratory test, including HIV RNA and antigen/antibody test, (2) had been prescribed ART, or (3) had three or more visits with corresponding HIV diagnostic codes. The algorithm achieved 98.9% sensitivity and 97.6% specificity. It has been estimated that 114,541 PWH in Florida in 2020 and 84% of them linked to care [36]. Our algorithm identified 71,363 PWH from OneFL (updated to early 2021), corresponding to ∼ 70% of the number of PWH linked to care in Florida.
Study Design
A retrospective longitudinal cohort study design was used (Fig. 1). The index date was defined as the first HIV-related encounter: the first visit with an HIV diagnosis code, first positive HIV laboratory test, or first HIV ART prescription, whichever occurred first. The main exposure of interest was having a SUD diagnosis and the outcomes of interest were comorbidities summarized by the Charlson comorbidity index (CCI) and healthcare utilization (number of care visits per year). Health records documented during the first three-year post-index date (T1 period) were used to identify exposure and confounding factors. Health records documented more than three years after the index visit and up to the most recent visit documented in the EHR (T2 period) were used to identify the outcomes. The three-year cutoff was selected after examining the distribution length of medical records available post-index data and to ensure a long enough window to capture SUD diagnosis.

Flowchart of sample timeline and variables assessment period
The study sample was a subset of individuals who had at least three years of post-index date health records among the identified cohort of PWH. Therefore, all patients included had 1 + visit during the T1 and T2 periods, respectively. The length of T1 period is three years for all patients; the length of T2 period ranged from one to six years. T0 was defined as the period between the first clinical encounter in the EHR and the index visit. Patients whose first visit was an HIV-related encounter did not have a T0 period.
Measurements
Substance use Disorder
SUD diagnoses were identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) [37] and ICD-10-CM [38]. The ICD codes were selected based on computable phenotypes used in past research [39] and specified as tobacco use disorder (ICD-9 305.1; ICD-10 F17), alcohol use disorder (305.0, 303, 305.9; F10, 291), cannabis use disorder (305.2, 304.3; F12), cocaine use disorder (305.6, 304.2; F14), amphetamine and other stimulant use disorder (305.7, 304.4; F15), opioid use disorder (305.5, 304.0, 304.7; F11), sedative use disorder (305.4, 305.8, 304.1; F13), and hallucinogen use disorder (305.3, 304.5; F16), following the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [40]. The prevalence of each individual SUD was measured by having at least one of the above-mentioned ICDs recorded [24, 41, 42] during the first three-year post index visit (T1 period), regardless of any pre-index date diagnosis (T0 period).
Comorbidity Assessment
The Charlson comorbidity index (CCI) is the most widely used comorbidity index [43, 44]. It contains 16 chronic conditions, and each condition is assigned a weight according to its potential influence on mortality [43]. In our analyses. each individual condition included in the CCI was identified using the coding algorithm proposed by Deyo et al. for ICD-9-CM [45] and Quan et al. for ICD-10-CM [46]. To capture the post-exposure incidence of each individual comorbidity condition, the outcome was defined as having (1) a diagnosis code that occurred at least once in the medical record during the T2 period, and (2) no prior diagnosis during the T0 and T1 periods (Fig. 1).
Additionally, a comorbidity score was calculated using the original CCI weights [47], excluding HIV/AIDS since our sample are PWH. Cumulative CCI scores were calculated at the index visit, three years after the index visit, and at the most recent visit documented in the EHR. The cumulative score was calculated based on conditions that had at least one diagnosis code recorded ever before. For example, when calculating cumulative CCI scores at year 3, all EHR documented before the index visit (T0) and within the first three years after the index visit (T1 period) were examined and a condition was coded as present if a diagnosis occurred at least once during that time frame. These cumulative CCI scores supplemented the incidence of each individual comorbidity to better represent the prevalence of comorbidity and multimorbidity burdens. Having a cumulative CCI score between 1 and 2 indicates a mild comorbidity, 3–4 indicates moderate comorbidity, and ≥ 5 indicates severe comorbidity [47].
Health Care Utilization
The number of any care visits, including inpatient, outpatient, and ED visits, was estimated for each calendar year during the T2 period. Multiple care visits on the same day were counted only once. The average number of care visits, ED visits, and inpatient visits per year was calculated for each participant.
Covariates
Patient demographics, including age, sex, race and ethnicity were measured at enrollment. Age at index visit was calculated. Anxiety and depression were also included in the analysis as covariates since they are both common among people with SUD [48] and associated with higher comorbidity burden [49].
Analysis
We performed descriptive statistics to characterize the study sample, examine the prevalence of SUD among PWH within the first three years post index visit, and compare the incidence for each comorbidity condition, cumulative CCI score, and health care utilization by any SUD status. Based on cumulative CCI scores at different time points, increases in the score from the index visit to three years after the index visit and most recent visit were calculated. First, SUD was dichotomized into with or without SUD. Second, based on the most common polysubstance use disorder patterns observed, SUD pattern was classified into three mutually exclusive groups: (1) tobacco use disorder only, (2) any alcohol and/or cannabis use disorder with no other SUD except tobacco use disorder (alcohol/cannabis/tobacco use disorder only), and (3) any stimulant, opioid, sedative or hallucinogen use disorder with or without other SUD. Finally, comparisons were made across the three SUD patterns in the increase of cumulative CCI score over time and health care utilization indicators among people with any SUD.
Multivariable regression analysis was used with age, sex, race, ethnicity, anxiety, and depression controlled. Logistic regression was used for each comorbidity incidence; odds ratios (ORs) and corresponding 95% confidence interval (CI) were reported. Negative binomial regression was used for changes in CCI score over time and health care utilization (number of any care, ED, or inpatient visits per year); rate ratio (exp(β)) and corresponding 95% CI were reported. All analyses were conducted in SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Sample Characteristics and Substance use Disorder Prevalence
A total of 42,271 people with a confirmed HIV diagnosis and at least 3 years of post-index visit EHRs were identified from OneFL. The mean (SD) age at the index visit was 44.5 (12.9) years; 45.1% were female, 52.0% Black African American, and 15.8% Hispanic (Table 1). The top three most common comorbidity incidences were chronic pulmonary disease (12%), mild liver disease (11%), and renal disease (10%).
As shown in Tables 2 and 44.5% of PWH had at least one SUD. The most common substance-specific use disorders were tobacco use disorder (37.7%), followed by alcohol (14.9%), cocaine (10.4%), and cannabis (9.4%) use disorders. Almost half (45%) of people with any SUD had two or more substance-specific use disorders. Supplement Fig. 1 describes SUD patterns. Among people with any SUD, 43.7% had tobacco use disorder only, 23.6% had alcohol or cannabis, or tobacco use disorder only, 32.7% had any stimulant, opioid, sedative, or hallucinogen use disorder. Within the “alcohol, cannabis or tobacco use disorder only” pattern, the most common SUD combination was alcohol and tobacco use disorder. Within the “any stimulant, opioid, sedative, or hallucinogen use disorder” pattern, the vast majority had 1 + SUDs, and mostly with cocaine or opioid use disorder.
Comparison between People with and Without any SUD
Having a SUD diagnosis among PWH was consistently associated with higher comorbidity for all conditions included in CCI (Table 3). After controlling for covariates (age, sex, race, ethnicity, depression, and anxiety) in regression models the largest comorbidity incidence differences between people with and without SUD among PWH were observed for moderate/severe liver disease (OR = 2.05, 95%CI 1.74, 2.41) and myocardial infarction (OR = 1.78, 95%CI 1.63, 1.96); whereas diabetes (OR = 1.07, 95%CI 0.99, 1.16 for diabetes with complication; OR = 1.11, 95%CI 1.03,1.19 for diabetes without complication) had the smallest/non-statistically significant comorbidity incidence differences.
Changes in cumulative CCI scores from index visit to three-year after and the most recent visit available were estimated and compared by SUD status (Table 3). The mean cumulative CCI scores at the index visit were 0.3 (Standard deviation/SD: 0.9) and 0.4 (SD: 1.3) for people with and without SUD, respectively. The mean score increased to 1.7 (SD: 2.3) and 2.6 (SD: 2.9) three-years post index visit and to 2.9 (SD: 3.2) and 4.2 (SD: 3.8) at the most recent visit for people with and without SUD, respectively.
In multivariable regression, compared to people without SUD, people with SUD were associated with a 45% increase in cumulative CCI score from the index visit to three-year after index visits (RR = 1.45, 95%CI 1.42, 1.49) and a 39% increase from the index visit to most recent visit (RR = 1.39, 95%CI 1.36, 1.42).
Relative to PWH but no SUD, people with SUD had a higher mean number of any care visits (7.8 vs. 11.0), ED visits (0.7 vs. 1.4), and inpatient visits (1.5 vs. 3.3) per year (Table 3). In multivariable regression, having a SUD diagnosis had the strongest association with more frequent inpatient visits (RR = 1.86, 95%CI 1.80, 1.93) across the three healthcare utilization indicators (Table 3).
Comparison Across Different SUD Patterns
Among PWH and across the SUD patterns, having any stimulant, opioid, sedative, or hallucinogen disorder was associated with the greatest increase in comorbidity burden over time, followed by people with alcohol, cannabis, or tobacco use disorder only. This same pattern was also observed for the three healthcare utilization indicators (Table 4).
Discussion
This study describes the prevalence of diagnosed SUD among patients with HIV in Florida and compares comorbidity burden and health care utilization across substance use patterns. The prevalence of overall and specific (alcohol, cocaine, and opioid) SUD in our sample was comparable to the prevalence observed among HIV care enrollees from the CNICS, a multistate EHR network-based HIV cohort in the US [5]. However, compared to their study, we found a lower prevalence of marijuana use disorder and other stimulant use disorders. The CNICS [5] used self-reported data from AUDIT-C [50] and ASSIST [51] to measure substance use disorder, while our analysis used ICD diagnostic codes from EHRs. This discrepancy in the SUD measurements may contribute to the differences in identified SUD prevalence. Geographic heterogeneity in SUD prevalence may also play a role, as wide variations in SUDs across study sites have been observed in Hartzler et al.’s [51] analyses. The CNICS sample used in their study did not include PWH in Florida (the University of Miami site for CNICS was added in 2021). The top four prevalent SUDs (namely tobacco, alcohol, marijuana, and cocaine) found in our sample were supported by other studies among PWH in Florida with substance use measures [2, 52].
PWH with SUD had higher care visits than PWH without SUD. Most of those visits were mainly inpatient or ED visits, which may indicate that higher healthcare utilization for people with SUD does not necessarily portend better health outcomes, and might reflect complex health needs with fragmented care, high treatment burdens, and high healthcare costs. This care utilization pattern indicates that the patient’s healthcare needs are being addressed during acute episodes or emergencies rather than through proactive, coordinated, and continuous outpatient care. Our analysis indicates people with any stimulant/opioid/sedative/hallucinogen use disorder showed the highest risk for comorbidity and inpatient and ED visits across all SUD patterns. This finding is supported by past research that co-occurring stimulant and opioid use disorders contribute to adverse health outcomes, including higher morbidity and mortality [58, 59].
The incidence for each individual comorbidity listed in CCI and changes in cumulative CCI score suggests that having SUD is associated with an increased disease burden among PWH. Several mechanisms may explain this elevated disease burden. Firstly, there might be a direct causal link between SUD and increased comorbidity burden among PWH. Previous studies showed the causal role of alcohol use on liver disease [53, 54], cocaine use increases myocardial oxygen demand and accelerates atherosclerosis and therefore increases the risk for heart disease [55,56,57]. Our analyses found moderate/severe liver disease and myocardial infarction as major disease burdens among PWH with SUD compared to those without SUD. Moreover, HIV is an independent risk factor for increased morbidity, and PWH are at higher risk for comorbidities compared to the general population [60, 61]. PWH have approximately a 2-fold increased risk for cardiovascular disease, a 1.5-fold increased risk for malignancy, and are more likely to die from non-HIV/AIDS-related chronic medical conditions [62,63,64]. Substance use could have a drug-drug interaction effect with ART, leading to an increased risk for comorbidities. For example, alcohol has been found to interact with certain ART regimens and increase liver disease risk [65].
Our findings suggest PWH with SUD experience faster development in multimorbidity over time. The ending the HIV epidemic efforts are being undermined by the high burden of substance use and its associated morbidity; thus, additional efforts must be made towards addressing substance use and the gaps in substance use care (i.e., screening, education, and treatment) among PWH. Previous studies have shown persistent gaps in substance use care and services for PWH [66, 67], and our findings support a call to action to reduce these gaps and increase access to substance use services. Moreover, as findings from our study revealed that PWH and SUD have higher rates of healthcare visits, integrating substance use screening and treatment into these existing visits may be a missed opportunity [68]. This may include the use of evidence-based on-demand pharmacological interventions, such as medication-assisted treatment [69, 70], and targeted behavioral therapies [71], in both ED and outpatient settings to effectively reach and provide comprehensive care for PWH.
This study has some limitations. The use of having at least three years of EHR as an inclusion criterion allows a clear temporal relationship between exposure and outcome clear, however, it may also lead to selection bias and slight overestimation of comorbidity and healthcare utilization. Our sample represents PWH who were continuously enrolled in care and PWH who only engaged in care briefly may not be well represented in our sample. Additionally, a large proportion of PWH was identified from claims data and does not have laboratory results. Therefore, we are unable to include viral load and CD4 count in our analyses, which have been found in past studies to be associated with SUD and comorbidity burdens [72]. Furthermore, SUD was identified using ICD codes; these codes cannot accurately differentiate the severity and duration of SUDs which might also influence the comorbidity burden and healthcare utilization. Moreover, in our multivariable regression model, we controlled demographic and psychiatric conditions as confounders. However, there might still be residual confounders in the identified associations. Caution should be made when interpreting the OR/RR as causal effects. Additionally, social determinants of health, such as socio-economic status and occupational security, as well as societal factors like insurance coverage, could also impact health care utilization pattern among PWH. Future research studies could consider using conceptual frameworks and Directed Acyclic Graphs (DAGs) to further examine the causal relationship behind the observed associations and identify actionable factors to reduce the healthcare burden. Future studies could also examine whether providing SUD treatment could reduce the risk of other comorbidities among PWH and whether specific treatments work better than others. Lastly, it is important to better understand how having these comorbidities complicate patient care management and how patients prioritize treatments for these different health conditions. This could better inform interventions to improve patient-centered care for PWH.
Conclusion
Our analyses revealed a high prevalence of SUDs among PWH, of which 44.5% of the cohort had at least one SUD. Nearly half of PWH with SUD exhibited two or more SUDs, with tobacco, alcohol, and cocaine being the most common substances involved. Our results support our hypothesis, as we found that PWH with SUDs experienced a higher burden of chronic comorbidities, a faster accumulation of comorbid conditions, and more frequent inpatient and ED visits. Additionally, we found that more healthcare utilization does not necessarily result in better healthcare outcome. Our results indicate people with any stimulant or opioid use disorder had the highest healthcare utilization, but also the fastest comorbidity accumulation. The higher healthcare utilization observed among those with any SUD mainly consists of more frequent ED and inpatient visits. This calls for prioritizing integrated and patient-centered care models that comprehensively address the complex healthcare needs of PWH and SUD, promoting timely screening, coordinated support, and improved treatment outcomes.
References
Gamarel KE, Brown L, Kahler CW, Fernandez MI, Bruce D, Nichols S, et al. Prevalence and correlates of substance use among youth living with HIV in clinical settings. Drug Alcohol Depend. 2016;169:11–8.
Mannes ZL, Bryant VE, Burrell LE, Lu H, Ferguson EG, Zhou Z, et al. The prevalence and patterns of substance use by birth cohort among HIV-positive adults in Florida. Aging Ment Health. 2019;23(4):515–23.
Miles DRB, Bilal U, Hutton HE, Lau B, Lesko CR, Fojo A, et al. Tobacco Smoking, Substance Use, and Mental Health symptoms in people with HIV in an urban HIV Clinic. J Health Care Poor Underserved. 2019;30(3):1083–102.
Mdodo R, Frazier EL, Dube SR, Mattson CL, Sutton MY, Brooks JT, et al. Cigarette smoking prevalence among adults with HIV compared with the general adult population in the United States: cross-sectional surveys. Ann Intern Med. 2015;162(5):335–44.
Hartzler B, Dombrowski JC, Crane HM, Eron JJ, Geng EH, Christopher Mathews W, et al. Prevalence and predictors of Substance Use disorders among HIV Care enrollees in the United States. AIDS Behav. 2017;21(4):1138–48.
Davis L, Uezato A, Newell JM, Frazier E. Major depression and comorbid substance use disorders. Curr Opin Psychiatry. 2008;21(1):14–8.
Luther AWM, Reaume SV, Qadeer RA, Thompson K, Ferro MA. Substance use disorders among youth with chronic physical illness. Addict Behav. 2020;110:106517.
Alqahtani MM, Alanazi AM, Pavela G, Dransfield MT, Wells JM, Lein DH, et al. Binge Drinking Moderates the Association between Chronic Lung Disease and E-Cigarette Use. Respir Care. 2021;66(6):936–42.
Bahorik A, Bobrow K, Hoang T, Yaffe K. Increased risk of dementia in older female US veterans with alcohol use disorder. Addiction. 2021;116(8):2049–55.
Baillargeon J, Polychronopoulou E, Kuo YF, Raji MA. The impact of Substance Use Disorder on COVID-19 outcomes. Psychiatr Serv. 2021;72(5):578–81.
Antiretroviral Therapy Cohort Collaboration. Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Lancet. 2008;372(9635):293–9.
Pelchen-Matthews A, Ryom L, Borges Á, Edwards S, Duvivier C, Stephan C, et al. Aging and the evolution of comorbidities among HIV-positive individuals in a European cohort. AIDS. 2018;32(16):2405–16.
Pourcher V, Gourmelen J, Bureau I, Bouee S. Comorbidities in people living with HIV: an epidemiologic and economic analysis using a claims database in France. PLoS ONE. 2020;15(12):e0243529.
Yang X, Zhang J, Chen S, Weissman S, Olatosi B, Li X. Utilizing electronic health record data to understand comorbidity burden among people living with HIV: a machine learning approach. AIDS. 2021;35(Suppl 1):S39–51.
Womack JA, Justice AC. The OATH syndemic: opioids and other substances, aging, alcohol, tobacco, and HIV. Curr Opin HIV AIDS. 2020;15(4):218–25.
Tsuyuki K, Pitpitan EV, Levi-Minzi MA, Urada LA, Kurtz SP, Stockman JK, et al. Substance Use disorders, Violence, Mental Health, and HIV: differentiating a Syndemic factor by gender and sexuality. AIDS Behav. 2017;21(8):2270–82.
McMahon JM, Braksmajer A, Zhang C, Leblanc N, Chen M, Aidala A, et al. Syndemic factors associated with adherence to antiretroviral therapy among HIV-positive adult heterosexual men. AIDS Res Ther. 2019;16(1):32.
Shukla DM, Faber EB, Sick B. Defining and characterizing frequent attenders: systematic literature review and recommendations. J Patient Cent Res Rev. 2020;7(3):255–64.
Gaulin M, Simard M, Candas B, Lesage A, Sirois C. Combined impacts of multimorbidity and mental disorders on frequent emergency department visits: a retrospective cohort study in Quebec, Canada. CMAJ. 2019;191(26):E724–32.
Giannouchos TV, Washburn DJ, Kum HC, Sage WM, Ohsfeldt RL. Predictors of Multiple Emergency Department Utilization among Frequent Emergency Department Users in 3 states. Med Care. 2020;58(2):137–45.
Ondler C, Hegde GG, Carlson JN. Resource utilization and health care charges associated with the most frequent ED users. Am J Emerg Med. 2014;32(10):1215–9.
Huang M, van der Borght C, Leithaus M, Flamaing J, Goderis G. Patients’ perceptions of frequent hospital admissions: a qualitative interview study with older people above 65 years of age. BMC Geriatr. 2020;20(1):332.
Wu LT, Zhu H, Ghitza UE. Multicomorbidity of chronic diseases and substance use disorders and their association with hospitalization: results from electronic health records data. Drug Alcohol Depend. 2018;192:316–23.
Winhusen T, Theobald J, Kaelber DC, Lewis D. Medical complications associated with substance use disorders in patients with type 2 diabetes and hypertension: electronic health record findings. Addiction. 2019;114(8):1462–70.
Liu Y, Elliott AL, Serdarevic M, Leeman RF, Cottler LB. A latent class analysis of the past-30-day substance use patterns among lifetime cocaine users: findings from a community sample in North Central Florida. Addict Behav Rep. 2019;9:100170.
Hunt GE, Large MM, Cleary M, Lai HMX, Saunders JB. Prevalence of comorbid substance use in schizophrenia spectrum disorders in community and clinical settings, 1990–2017: systematic review and meta-analysis. Drug Alcohol Depend. 2018;191:234–58.
Fortin M, Stewart M, Poitras ME, Almirall J, Maddocks H. A systematic review of prevalence studies on multimorbidity: toward a more uniform methodology. Ann Fam Med. 2012;10(2):142–51.
Armoon B, Grenier G, Cao Z, Huỳnh C, Fleury MJ. Frequencies of emergency department use and hospitalization comparing patients with different types of substance or polysubstance-related disorders. Subst Abuse Treat Prev Policy. 2021;16(1):89.
Cleland CM, Gwadz M, Collins LM, Wilton L, Sherpa D, Dorsen C, et al. African American/Black and latino adults with detectable HIV viral load evidence substantial risk for Polysubstance Substance Use and co-occurring problems: a latent class analysis. AIDS Behav. 2021;25(8):2501–16.
Carliner H, Brown QL, Sarvet AL, Hasin DS. Cannabis use, attitudes, and legal status in the U.S.: a review. Prev Med. 2017;104:13–23.
DeBeck K, Cheng T, Montaner JS, Beyrer C, Elliott R, Sherman S, et al. HIV and the criminalisation of drug use among people who inject drugs: a systematic review. Lancet HIV. 2017;4(8):e357–74.
Lipira L, Rao D, Nevin PE, Kemp CG, Cohn SE, Turan JM, et al. Patterns of alcohol use and associated characteristics and HIV-related outcomes among a sample of African-American women living with HIV. Drug Alcohol Depend. 2020;206:107753.
Green TC, Kershaw T, Lin H, Heimer R, Goulet JL, Kraemer KL, et al. Patterns of drug use and abuse among aging adults with and without HIV: a latent class analysis of a US veteran cohort. Drug Alcohol Depend. 2010;110(3):208–20.
Hogan WR, Shenkman EA, Robinson T, Carasquillo O, Robinson PS, Essner RZ, et al. The OneFlorida Data Trust: a centralized, translational research data infrastructure of statewide scope. J Am Med Inf Assoc. 2022;29(4):686–93.
Liu Y, Siddiqi K, Cook r, Bian J, Squires P, Shenkman E et al. Optimizing identification of people living with HIV from electronic medical records (EHR): computable phenotype development and validation. Methods of Information in Medicine2021.
AIDSVu. Local Data: Florida 2021 [Available from: https://aidsvu.org/local-data/united-states/south/florida/.
Centers for Disease Control and Prevention. ICD - ICD-9-CM -. International Classification of Diseases, Ninth Revision, Clinical Modification 2021 [updated 2021-11-03T02:48:41Z. Available from: https://www.cdc.gov/nchs/icd/icd9cm.htm.
Centers for Disease Control and Prevention. ICD- 10 - CM International Classification of Diseases. Tenth Revision, Clinical Modification (ICD-10-CM) 2022 [updated 2022-04-06T06:07:13Z. Available from: https://www.cdc.gov/nchs/icd/icd-10-cm.htm.
Palumbo SA, Adamson KM, Krishnamurthy S, Manoharan S, Beiler D, Seiwell A, et al. Assessment of probable opioid use disorder using Electronic Health Record Documentation. JAMA Netw Open. 2020;3(9):e2015909.
DSM 5 Diagnostic Codes Related to Substance Use Disorders. http://www.acbhcs.org/providers/qa/docs/training/DSM-IV_DSM-5_SUD_DX.pdf 2022.
Rowe CL, Santos GM, Kornbluh W, Bhardwaj S, Faul M, Coffin PO. Using ICD-10-CM codes to detect illicit substance use: a comparison with retrospective self-report. Drug Alcohol Depend. 2021;221:108537.
Williams EC, Fletcher OV, Frost MC, Harris AHS, Washington DL, Hoggatt KJ. Surveys Across Sociodemographic Groups in the Veterans Health Administration. JAMA Netw Open. 2022;5(6):e2219651. Comparison of Substance Use Disorder Diagnosis Rates From Electronic Health Record Data With Substance Use Disorder Prevalence Rates Reported in.
Charlson M, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
de Groot V, Beckerman H, Lankhorst GJ, Bouter LM. How to measure comorbidity. A critical review of available methods. J Clin Epidemiol. 2003;56(3):221–9.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–9.
Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9.
Bannay A, Chaignot C, Blotière PO, Basson M, Weill A, Ricordeau P, et al. The best use of the Charlson Comorbidity Index with Electronic Health Care Database to Predict Mortality. Med Care. 2016;54(2):188–94.
Jones CM, McCance-Katz EF. Co-occurring substance use and mental disorders among adults with opioid use disorder. Drug Alcohol Depend. 2019;197:78–82.
Šprah L, Dernovšek MZ, Wahlbeck K, Haaramo P. Psychiatric readmissions and their association with physical comorbidity: a systematic literature review. BMC Psychiatry. 2017;17(1):2.
Dawson DA, Smith SM, Saha TD, Rubinsky AD, Grant BF. Comparative performance of the AUDIT-C in screening for DSM-IV and DSM-5 alcohol use disorders. Drug Alcohol Depend. 2012;126(3):384–8.
Humeniuk R, Ali R, Babor TF, Farrell M, Formigoni ML, Jittiwutikarn J, et al. Validation of the Alcohol, Smoking and Substance involvement screening test (ASSIST). Addiction. 2008;103(6):1039–47.
Diaz-Martinez J, Tamargo JA, Delgado-Enciso I, Liu Q, Acuña L, Laverde E, et al. Resilience, anxiety, stress, and substance use patterns during COVID-19 pandemic in the Miami Adult studies on HIV (MASH) Cohort. AIDS Behav. 2021;25(11):3658–68.
Rocco A, Compare D, Angrisani D, Sanduzzi Zamparelli M, Nardone G. Alcoholic disease: liver and beyond. World J Gastroenterol. 2014;20(40):14652–9.
Shamanna SB, Naik RR, Hamide A. Causes of liver disease and its outcome in HIV-infected individuals. Indian J Gastroenterol. 2016;35(4):310–4.
Schwartz B, Rezkalla S, Kloner R. Cardiovascular effects of Cocaine. Circulation. 2010;122(24):2558–69.
DeFilippis EM, Singh A, Divakaran S, Gupta A, Collins BL, Biery D, et al. Cocaine and Marijuana Use among Young adults with myocardial infarction. J Am Coll Cardiol. 2018;71(22):2540–51.
Gan WQ, Buxton JA, Scheuermeyer FX, Palis H, Zhao B, Desai R, et al. Risk of cardiovascular diseases in relation to substance use disorders. Drug Alcohol Depend. 2021;229:109132. Pt A).
Das L, Kutscher E. Stimulant Use disorders in the United States—Is another epidemic on the Horizon? JAMA Health Forum. 2022;1(12).
O’Brien P, Henke RM, Schaefer MB, Lin J, Creedon TB. Adverse events among adult Medicaid enrollees with opioid use disorder and co-occurring substance use disorders. Drug Alcohol Depend. 2021;221:108555.
Yu X, Westra JR, Giordano TP, Berenson AB, Baillargeon JG, Kuo YF. Assessing comorbidities and survival in HIV-infected and uninfected matched Medicare enrollees. AIDS. 2021;35(10):1667–75.
Yang X, Zhang J, Chen S, Weissman S, Olatosi B, Li X. Comorbidity patterns among people living with HIV: a hierarchical clustering approach through integrated electronic health records data in South Carolina. AIDS Care. 2021;33(5):594–606.
Shah ASV, Stelzle D, Lee KK, Beck EJ, Alam S, Clifford S, et al. Global Burden of Atherosclerotic Cardiovascular Disease in people living with HIV: systematic review and Meta-analysis. Circulation. 2018;138(11):1100–12.
Coghill AE, Shiels MS, Suneja G, Engels EA. Elevated Cancer-specific mortality among HIV-Infected patients in the United States. J Clin Oncol. 2015;33(21):2376–83.
Croxford S, Miller RF, Post FA, Harding R, Lucas SB, Figueroa J, et al. Cause of death among HIV patients in London in 2016. HIV Med. 2019;20(9):628–33.
Barve S, Kapoor R, Moghe A, Ramirez JA, Eaton JW, Gobejishvili L, et al. Focus on the liver: alcohol use, highly active antiretroviral therapy, and liver disease in HIV-infected patients. Alcohol Res Health. 2010;33(3):229–36.
Oldfield BJ, Muñoz N, McGovern MP, Funaro M, Villanueva M, Tetrault JM, et al. Integration of care for HIV and opioid use disorder. AIDS. 2019;33(5):873–84.
Kraemer KL, McGinnis KA, Fiellin DA, Skanderson M, Gordon AJ, Robbins J, et al. Low levels of initiation, engagement, and retention in substance use disorder treatment including pharmacotherapy among HIV-infected and uninfected veterans. J Subst Abuse Treat. 2019;103:23–32.
Parcesepe AM, Lancaster K, Edelman EJ, DeBoni R, Ross J, Atwoli L, et al. Substance use service availability in HIV treatment programs: data from the global IeDEA consortium, 2014–2015 and 2017. PLoS ONE. 2020;15(8):e0237772.
Connery HS. Medication-assisted treatment of opioid use disorder: review of the evidence and future directions. Harv Rev Psychiatry. 2015;23(2):63–75.
Taylor JL, Wakeman SE, Walley AY, Kehoe LG. Substance use disorder bridge clinics: models, evidence, and future directions. Addict Sci Clin Pract. 2023;18(1):23.
Magill M, Ray L, Kiluk B, Hoadley A, Bernstein M, Tonigan JS, et al. A meta-analysis of cognitive-behavioral therapy for alcohol or other drug use disorders: treatment efficacy by contrast condition. J Consult Clin Psychol. 2019;87(12):1093–105.
Goulet JL, Fultz SL, Rimland D, Butt A, Gibert C, Rodriguez-Barradas M, et al. Aging and infectious diseases: do patterns of comorbidity vary by HIV status, age, and HIV severity? Clin Infect Dis. 2007;45(12):1593–601.
Acknowledgements
The OneFlorida Clinical Research Consortium was funded by the Patient-Centered Outcomes Research Institute number CDRN-1501-26692 and RI-CRN-2020-005; in part by the OneFlorida Cancer Control Alliance, funded by the Florida Department of Health’s James and Esther King Biomedical Research Program #4KB16. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology, the OneFlorida Clinical Research Consortium, the University of Florida’s Clinical and Translational Science Institute, the Florida Department of Health, or the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
Liu Y - study design, data analysis, writing-original draft. Manavalan P - data interpretation, writing-original draft. Siddiqi K - data interpretation, writing-original draft. Cook RL - supervision, data interpretation, writing-editing. Prosperi M – study design, supervision, funding, writing-editing.
Corresponding author
Ethics declarations
Funding
This work was supported by the National Institute of Allergy and Infectious Diseases (NIAID) under Award Number R01AI145552 (Co-PIs: Salemi, Prosperi) and National Institute on Alcohol Abuse and Alcoholism (NIAAA) U24 core Southern HIV and Alcohol Research Consortium (SHARC) grant – U24AA022002 (PI: Cook). Liu Y, Siddiqi K, Cook RL, and Prosperi M received research funding from the Merck Investigator Studies Program.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, Y., Manavalan, P., Siddiqi, K. et al. Comorbidity Burden and Health Care Utilization by Substance use Disorder Patterns among People with HIV in Florida. AIDS Behav 28, 2286–2295 (2024). https://doi.org/10.1007/s10461-024-04325-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-024-04325-y