
Abstract
HIV self-testing (HIVST) is an effective method to expand HIV testing coverage worldwide. We analyze the results of HIVST and sexual behaviors of first-time testers among Men who have sex with men (MSM) who participated in a secondary distribution of HIVST kits. A total of 589 participants were recruited, including 173 first-time testers and 416 non-first-time testers. The first-time testers were mainly of Han ethnicity (aOR 1.88, 95% CI 1.10, 3.24), more likely to be HIV positive (aOR 7.18, 95% CI 2.37, 21.72), and had higher income (aOR 2.01, 95% CI 1.10, 3.69). Both groups were less likely to have anal sex with male partners (χ2: 146.24, P < 0.01), (χ2: 582.72, P < 0.01) or have sex with female partners (χ2: 19.01, P < 0.01), (χ2: 35.74, P < 0.01) after HIVST. We should expand HIVST among MSM and other key populations to identify first-time testers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acquired immunodeficiency syndrome (AIDS) is a major global public health issue. According to the report of the Joint United Nations Program on HIV/AIDS (UNAIDS), there were 37.7 million people living with HIV (PLWH) worldwide in 2020, but only 84% of PWH knew their HIV status [1], which means about 6.1 million PLWH did not know their HIV status in 2020 [1]. In addition, the main route of HIV transmission is sexual transmission. The main group of sexual transmission is Men who have sex with men (MSM) [1]. Furthermore, MSM represent a significant (23%) and increasing proportion of PLWH globally, which poses enormous global challenges for public health systems [1].
In China, MSM are a high-risk population for HIV. The overall prevalence of HIV among MSM in China from 2001 to 2018 was estimated to be 5.7% [2], but these individuals had low rates of ever testing (49.7%) [3, 4]. HIV self-testing has the potential to increase testing coverage among MSM. In 2016, the WHO issued the Guidelines on HIV self-testing and partner notification: supplement to consolidated guidelines on HIV testing services to support the implementation and scaling-up of ethical, effective, acceptable and evidence-based approaches to HIV self-testing [5]. HIV self-testing has a variety of advantages, including being convenient, affordable, and relatively quick, in addition to the affordance of privacy [6]. In 2017, China published policy to promote HIV self-testing, and people can buy HIV self-test kits online [7]. HIV self-testing proportion among web-based Chinese MSM showed substantial increases [8].
With the advancement of social media and the rapid development of the Internet, the pattern in which MSM find sexual partners has changed dramatically [9], which has led to ways of making friends that are more concealed, more convenient, and more diverse [10]. MSM are at substantial risk for HIV infection in nearly all contexts studied globally [11]. HIV/syphilis self-test kits meet MSM requirements. MSM can apply for free dual HIV/syphilis self-test kits online. Some studies have shown that the application of Internet + HIV self-testing is a highly acceptable method of HIV testing [6, 12]. To increase the HIV testing rate and expand coverage among key populations, the WHO encourages innovative and flexible HIV testing strategies [5]. A study has shown that social media-based secondary distribution of HIV self-test kits could expand the scope of HIV testing to discover more first-time testers [13]. A study suggested that MSM who have never been tested for HIV might engage in higher risk behaviors than MSM who have been previously tested [14].
Our study is a secondary analysis of a larger trial to compare socio-behavioral characteristics between first-time and non-first-time HIV testers among Chinese MSM. The aim of this study was to analyze the population characteristic-related and sexual behavior-related factors associated with HIV testing for the first time and the factors associated with HIV testing among MSM. We also explored the changes of high-risk sexual behaviors. This study can provide scientific evidence for HIV prevention.
Methods
Participants
From June 2018 to September 2019, a total of 639 MSM were recruited by the Zhuhai MSM social organization, Zhuhai Xutong Volunteer Service Center (hereafter referred to as Zhuhai Xutong), and 589 individuals met the requirements of this study. The inclusion criteria for the study subjects included: (1) men who were 16 years or older; (2) born biologically male; (3) ever had sex with men; (4) were willing to provide a contact number; (5) agreed to participate in the follow-up investigation after 3 months; (6) were willing to return HIVST results. HIV self-testers were divided into two groups: (1) first-time HIV testers; (2) non-first-time HIV testers [13].
Design and Data Collection
This implementation study was conducted in Zhuhai, China. The Zhuhai Center for Diseases Control (CDC) and a gay community-led organization (Zhuhai Xutong Voluntary Services Center; hereafter, Xutong), initiated a social media-based online system in 2016 for MSM to apply for free dual HIV/syphilis self-test kits. MSM were able to apply for HIVST kits using Xutong’s public WeChat account. WeChat is a multi-functional social app which can be used for messaging, public surveys, and monetary transactions [13]. All participants were asked to report their self-test results and upload a result photograph for verification. All results were reviewed by trained Xutong volunteers who followed up as needed for result verification or linkage to care. MSM who apply for HIV/syphilis self-test kits were informed that they could distribute the kits to other social contacts, including partners or friends (referred to as “Secondary Distribution”). MSM who had never been tested for HIV that were defined as first-time testers.
Our study used an electronic questionnaire designed by us to conduct an anonymous survey and tests with the informed consent of MSM. We collected information about the MSM socio-demographic characteristics (including age, education, income, marital status, residence, and occupation), sexual behaviors, and HIV testing history. Testing items of the kits included HIV antibodies and syphilis antibodies. Three months after HIV self-testing, MSM completed a follow-up questionnaire about their sexual behaviors.
Statistical Analysis
The statistical analysis was performed using SPSS (Version 25, IBM, New York). Chi-square test or Fishers’ Exact tests were used to compare the socio-demographic characteristics, sexual behaviors, and HIV test results of the MSM between first-time HIV testers and non-first-time HIV testers. A binary logistic regression model was used to further analyze the factors associated with first-time HIV testing. P < 0.05 was considered statistically significant.
Results
Population Characteristics
A total of 639 HIV self-testers were recruited for this study. Of these, 50 (7.8%) were excluded due to uploading photograph of the test result incorrectly, and 589 (91.2%) MSM were included in this study. Among them, 29.4% (173/589) were first-time HIV testers. The median age of participants was 28 years old. A majority of participants were single (79.5%), had a non-agricultural household registration (59.9%), non-students (84.4%), had an education level of college and above (78.3%), were employed (95.9%), and were identified as homosexual (69.3%).
Compared with non-first-time testers, first-time testers were more likely to be students (χ2: 7.48, P < 0.01). There was a difference in sexual orientation (χ2: 12.02, P < 0.01) and personal income (χ2: 14.53, P < 0.01) between first-time testers and non-first-time testers. There was no difference in age, marital status, residence, household registration location, ethnicity, education, and employment status (P > 0.05) between two groups (Table 1).
Sexual Behaviors and HIV Test Results of MSM
Compared with non-first-time testers, first-time testers were less likely to have anal sex with a male partner (62.40% vs 83.70%, χ2: 31.49, P < 0.01) and had casual male partners in the past 6 months (15.60% vs 31.30%, χ2: 15.29, P < 0.01). Fewer first-time testers than non-first-time testers reported willingness for HIV testing once every 3 months (42.20% vs 53.40%, χ2: 6.10, P < 0.05).
There was a significant difference in the prevalence of HIV between first-time testers and non-first-time testers (7.50% vs 1.20%, χ2: 16.43, P < 0.01). The prevalence of syphilis was similar among first-time testers and non-first-time testers (Table 2).
Factors Associated with First-Time HIV Testing
The binary logistic regression model was used to analyze the factors associated with first-time HIV testing. Without any factors adjusted, the Han ethnicity (OR 1.92, 95% CI 1.11, 3.34), high personal income (OR 2.02, 95% CI 1.09, 3.73) and HIV positive results (OR 7.73, 95% CI 2.48, 24.15) were the factors associated with first-time HIV testing. Anal sex with a male partner in the past 6 months (OR 0.40, 95% CI 0.25, 0.65) was a factor associated with first-time HIV testing (Table 3).
After adjusting for age and marital status, compared with non-first-time testers, first-time testers had lower odds of having had anal sex with a male partner in the past 6 months (aOR 0.40, 95% CI 0.25, 0.64). Meanwhile, the first-time testers were mainly of Han ethnicity (aOR 1.88, 95% CI 1.10, 3.24), had a high income (aOR 2.01, 95% CI 1.10, 3.69), and were more likely to be HIV positive (aOR 7.18, 95% CI 2.37, 21.72) (Table 3).
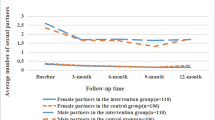
Changes in Sexual Behaviors After HIV Self-testing Distributed Through this Project
After HIV self-testing, both first-time testers and non-first-time testers were less likely to have anal sex with a male partner [ (62.40% vs 1.80%) (χ2: 146.24, P < 0.01)]; [ (83.70% vs 8.90%) (χ2: 582.72, P < 0.01)] and have sex with a female partner [ (13.30% vs 1.16%) (χ2: 19.01, P < 0.01)]; [ (8.90% vs 0.24%) (χ2: 35.74, P < 0.01) (Table 4).
Discussion
The WHO has established the target of 95% PLWH being detected by HIV testing within all demographics, groups, and geographies [1]. However, factors related to the results and behaviors of first-time HIV testers remain underexplored. We hope to expand HIV testing coverage and identify more untested people, as well as understand sexual behavior changes of MSM after HIVST.
Our findings are similar to those of other studies in that first-time testers accounted for a certain proportion of MSM [15]. This suggests that HIVST can help identify key sub-groups of certain characteristics to target for reaching more hidden MSM who have never tested before. The majority of MSM in our study had a college degree or above (78.3%), and there was no significant difference in educational background between the first-time and non-first-time testers. But the first-time testers were less willing to participate in follow-up HIV self-testing compared with non-first-time testers, which is probably related to their low awareness of HIV risks and protection. Studies have shown that education level has become a factor in the willingness of young people to engage in HIV testing [16, 17]. In our study, the sexual activity of first-time testers was generally lower than that of non-first-time testers. Other studies have indicated that first-time HIV testers tended to perceive themselves to be at lower risk of HIV infection and have low awareness of HIV prevention and treatment [15]. Thus, they were less willing to follow-up on their HIVST.
In China, the prevalence of HIV among young men who have sex with men (YMSM) is high (5.0%), while YMSM receive a lower proportion of HIV testing [18]. We found that 22.0% (38/173) of first-time HIV testers were students in this study, which was a higher percentage than other studies reported. A study found that the proportion of MSM students who had previous HIV testing (first-time) was 3.66% [19]. This may be related to MSM students considering themselves to be safe, so that they are willing to choose other students at school as their sexual partners. However, a study has shown that YMSM were at higher risk of HIV infection compared to other MSM due to their significant risk behaviors and false perception of a low HIV risk, which led to lower detection rate than that of other MSM [20, 21]. In our study, the proportion of students who tested HIV for the first time was higher, which may be due to their high level of HIV-related knowledge, the higher acceptance of HIVST among students, or the rise of students' sexual needs and higher HIV risk-awareness compared to the time during which the aforementioned previous study was conducted. Our team's previous study observed that students were more willing to receive HIV education, and that they had a higher acceptance of HIVST, as well as a stronger inclination to receive sexual information through peer education [22]. Given that the proportion of students was high among first-time testers, it is necessary to organize students to carry out innovative peer education and provide HIV-related online counseling and testing, as well as other AIDS prevention services [22] through new social media platforms to improve their risk awareness and testing willingness.
This study also suggested that non-first-time HIV testers had a higher frequency of anal sex with men in the past 6 months before the study. They were also more likely to have casual sexual partners in the past 6 months before the study. If MSM engaged in HIV testing and found that they were HIV-negative, they may perceive themselves to be safe and continue to search for sexual partners, which was consistent with the results of previous research [23]. This finding suggests that we should establish a complete mechanism for HIV testing and the notification of results for MSM. Thereby, they could improve their HIV awareness and reduce their risk of HIV infection and other sexually transmitted diseases.
Moreover, we found that first-time HIV testers had a higher HIV-positive rate than non-first-time testers. And those who had anal sex with a male partner were more likely to be non-first-time testers. A study reported that people’s self-reported barriers to taking a test included perceiving themselves to be at low HIV risk, fear of a positive diagnosis, an unawareness where to get tested, and fear of discrimination [24]. That may be why first-time testers are not willing to participate HIV testing and their HIV positive rate was higher than non-first-time testers. Some studies have demonstrated that MSM who engaged in high-risk sexual behaviors were more willing to seek out counseling and testing for HIV [25,26,27]. When high-risk sexual behavior occurs, non-first-time testers can take the initiative to take HIV testing and counseling [28]. Meanwhile, MSM who were highly educated and earned a relatively high-income had greater health awareness [29, 30]. However, most first-time testers had a high income and were less willing to participate in HIV testing in the future compared to non-first-time testers. This suggests that we should expand the publicity of HIV self-testing kits and make it easier for people to access related information, so as to improve awareness of HIV testing, increase the frequency of HIV testing, identify more first-time testers and reduce the risk of HIV transmission.
This study also found that there was a change in sexual behavior after HIV self-testing. Specifically, after HIV self-testing, the engagement in anal sex with male partners and female partners was decreased among all participants. This was similar to the finding of another study that the surveyed subjects would increase their safe sexual behaviors or reduce their sexual activity within a short time after an HIV test [31]. A previous study indicated that HIV testing was related to high-risk sexual behaviors [32]. Some participants attended clinics in the public health sector or related NGOs for HIV/Syphilis testing or purchased self-test kits after engaging in condomless sex. It may be that MSM are concerned about HIV infection after high-risk sexual behaviors; thus, they reduce their sexual behaviors after HIV testing. A study suggested that an additional benefit of HIVST may be the option to test at the point of sex, and then making a decision regarding whether or not to have sex based on the test results [33]. This suggested that HIVST could reduce high-risk sexual behaviors among MSM, but long-term changes in their risky sexual behaviors require further study.
This study has certain limitations. First, participants in this study were recruited on the Internet, and follow-up investigations were also conducted online using a well-established MSM social platform. Therefore, this study may not be representative of the MSM who do not use social media. Second, some questions about sexual behaviors in the questionnaire were rather sensitive. This may result in a social desirability reporting bias, especially given the stigma surrounding HIV and MSM. Finally, further exploration of the feasibility and acceptability of secondary distribution of self-test kits among MSM with lower economic status should be considered for future research.
In conclusion, compared with first-time HIV testers, non-first-time HIV testers were more active in terms of their sexual behaviors and had greater awareness of HIV testing. First-time HIV testers had a higher HIV-positive rate than non-first-time testers. After HIV self-testing, the high-risk sexual behaviors of all participants were decreased. Further implementation studies are needed to discover more “first-time testers” and change the sexual behaviors among MSM and other key populations through HIV self-testing.
References
UNAIDS. UNAIDS DATA 2021. 2021; https://www.unaids.org/sites/default/files/media_asset/JC3032_AIDS_Data_book_2021_En.pdf.
Dong MA-O, Peng B, Liu ZF, et al. The prevalence of HIV among MSM in China: a large-scale systematic analysis. (1471–2334 (Electronic)).
Xu JJ, Han MJ, Jiang YJ, et al. Prevention and control of HIV/AIDS in China: lessons from the past three decades. (2542–5641 (Electronic)).
Chao HJJHW. Incidence of new HIV infection and its influencing factors among men who have sex with men in China: a meta-analysis. Prev Med. 2022;34(01):70–7.
World Health Organziation. Guidelines on HIV self-testing and partner notification: supplement to consolidated guidelines on HIV testing services.
Figueroa C, Johnson C, Verster A, Baggaley R. Attitudes and acceptability on HIV self-testing among key populations: a literature review. AIDS Behav. 2015;19(11):1949–65.
Bao HY, Xiong Y, Marley M, Tang WM. [Current status of HIV self-testing application]. (0254–6450 (Print)).
Wu D, Cheng WB, Xiong Y, Lu Y, Ni YX, Tang WM. [Changing trends of HIV testing and HIV self-testing in men who have sex with men on a gay social networking app]. (0254–6450 (Print)).
Bien CH, Best Jm Fau - Muessig KE, Muessig Ke Fau - Wei C, Wei C Fau - Han L, Han L Fau - Tucker JD, Tucker JD. Gay apps for seeking sex partners in China: implications for MSM sexual health. (1573–3254 (Electronic)).
Sze WN, Kwan TH, Kei LKC, Chui LJY, Shan LS. Delineation of chemsex patterns of men who have sex with men in association with their sexual networks and linkage to HIV prevention. Int J Drug Policy. 2020;75:102591.
Marshall BDL, Goedel WC, King MRF, et al. Potential effectiveness of long-acting injectable pre-exposure prophylaxis for HIV prevention in men who have sex with men: a modelling study. (2352–3018 (Electronic)).
Ngure K, Heffron R, Mugo N, et al. Feasibility and acceptability of HIV self-testing among pre-exposure prophylaxis users in Kenya. J Int AIDS Soc. 2017;20:21234.
Wu DA-O, Zhou Y, Yang N, et al. Social Media-Based Secondary Distribution of Human Immunodeficiency Virus/Syphilis Self-testing Among Chinese Men Who Have Sex with Men. (1537–6591 (Electronic)).
Dailey AF, Hoots BE, Hall HI, et al. Vital Signs: Human Immunodeficiency Virus Testing and Diagnosis Delays - United States. (1545–861X (Electronic)).
Jin X, Xu JJ, Smith MK, et al. An internet-based self-testing model (easy test): cross-sectional survey targeting men who have sex with men who never tested for HIV in 14 Provinces of China. J Med Internet Res. 2019;21(5):e11854.
Zhang J, Gao Y, Li D, Li T, Yang Y. Willingness and influencing factors on HIV testing among college young students in Daxing District, Beijing. Chin J Aids STD. 2021;27(7):763–6.
Yu B, Yang S, Pei R, Huang Y. Ways and willingness of HIV testing of college students and influencing factors in Sichuan province. Chin J Aids STD. 2021;27(2):141–5.
Cao Y, Meng XY, Weng H, Peng MJ, Yan H, Li SY. Prevalence of AIDS-related sexual behaviors and HIV infection status in young men who have sex with men in China: a meta-analysis. Zhonghua liu xing bing xue za zhi = Zhonghua liuxingbingxue zazhi. 2016;37(7):1021–7.
Zhou Y, Lin K, Dai W, et al. Analysis of HIV testing and associated factors among college students in Zhuhai. Chin J Aids STD. 2020;26(11):1193–6.
Khawcharoenporn T, Mongkolkaewsub S, Naijitra C, Khonphiern W, Apisarnthanarak A, Phanuphak N. HIV risk, risk perception and uptake of HIV testing and counseling among youth men who have sex with men attending a gay sauna. AIDS Res Therapy. 2019;16:1–11.
Gao M, Xiao C, Cao Y, Yu B, Li S, Yan H. Associations between sexual sensation seeking and AIDS-related knowledge, attitudes and behaviors among young men who have sex with men in China. Psychol Health Med. 2017;22(5):596–603.
Yawei ZYYYDW. Willingness and demands for AIDS-related health education among college students in Zhuhai. Mod Prev Med. 2021;48(05):902–6.
Ijadunola KT, Abiona TC, Odu OO, Ijadunola MY. College students in Nigeria underestimate their risk of contracting HIVAIDS infection. Eur J Contracept Reprod Health Care. 2007;12(2):131–7.
Ye R, Liu C, Tan S, et al. Factors associated with past HIV testing among men who have sex with men attending university in China: a cross-sectional study. (1449–8987 (Electronic)).
Cheng WB, Egan JE, Liu Q, Xu HF, Stall R, Friedman MR. Psychosocial correlates of HIV testing frequency among men who have sex with men in Guangzhou, China. AIDS Behav. 2020;24(2):363–72.
Jin W, Cheng W, Zhong F, et al. Willingness and correlated factors of HIV self-testing used for sexual partners among HIV-infected MSM in Guangzhou. Chin J Aids STD. 2019;25(5):472–5.
Jiang J, Pan XH, Yang JZ, et al. Willingness for HIV test and associated factors among 535 college students who had sex in Zhejiang province. Zhonghua liu xing bing xue za zhi = Zhonghua liuxingbingxue zazhi. 2016;37(10):1356–60.
Leblanc NM, Andes KL. An exploration of men’s knowledge, attitudes, and perceptions of HIV, HIV Risk, and willingness to test for HIV in Yendi District, Northern Ghana. JANAC J Assoc Nurses AIDS Care. 2015;26(3):281–95.
Xiao D, Wang X, Li Y, et al. Factors associated with the willingness to HIV test in men who have sex with men in Fengtai district of Beijing. China Prev Med. 2021;22(7):513–6.
Jiao KD, Wei R, Li HC, et al. HIV testing frequency and associated factors among five key populations in ten cities of China: a cross-sectional study. BMC Infect Dis. 2022;22(1):1–12.
Tang W, Huang W, Lu H, et al. What happens after HIV self-testing? Results from a longitudinal cohort of Chinese men who have sex with men. BMC Infect Dis. 2019;19(1):1–7.
Choi KWY, Choi EPH, Chow EPF, et al. The experience of using dating applications for sexual hook-ups: a qualitative exploration among HIV-negative men who have sex with men in Hong Kong. (1559–8519 (Electronic)).
Stevens DR, Vrana CJ, Dlin RE, Korte JE. A global review of HIV self-testing: themes and implications. AIDS Behav. 2018;22(2):497–512.
Acknowledgements
We are very grateful to all the participants who participated in this study.
Funding
This work was supported by the Medical Science and Technology Foundation of Guangdong Province [Grant Number 20201110143347920].
Author information
Authors and Affiliations
Contributions
Conceptualization, YF and HL; Methodology, ZG and MC; Software, YW and HT; Validation, MD and SH; Formal analysis, JL and YF; Data curation, YZ and MD; Writing—original draft preparation, YF and HL; Writing—review and editing, YF and HL; Visualization, SZ and HL; upervision, YZ; Project administration, WM and WT; Funding acquisition, WM and WT; All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
All authors have declared no conflicts of interest.
Ethical Approval
Prior to launching the study, ethical approval was obtained from the institutional review board of the Zhuhai Municipal Center for Diseases Prevention and Control in China (ZHCDC2018014).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lyu, H., Feng, Y., Zhou, Y. et al. Factors Associated with First-Time HIV Testing Among MSM via Secondary Distribution of HIV Self-test Kits in Zhuhai, China. AIDS Behav 27, 1942–1949 (2023). https://doi.org/10.1007/s10461-022-03927-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-022-03927-8