
Abstract
Contraceptive preferences of women at risk for HIV acquisition are not well documented. We report on contraceptive choices among women residing in small townships in southwestern Uganda. This was part of preparatory efforts for recruitment into the Ring Study, a phase 3 microbicide trial, between July 2013 and October 2014. Clinicians provided contraceptives per a woman’s choice. HIV testing and screening for other sexually transmitted infections were done at first contact and at screening for the trial. Contraceptive choice was summarized by demographics and regression analysis to show factors associated with use of the injectable method. Of 6725 women contacted, 489 were prescreened. Of these 489 women, most (306, 63%) were already using contraception. Injectables were most preferred (58.7%), followed by implants (23.9%). Women living with a regular sexual partner preferred the injectable method (61.0%, P = 0.06), compared with other methods. Women at risk for HIV infection are willing to initiate use of modern contraceptives, which may reduce study dropout during intervention trials due to unintended pregnancy. Registration no: NCT01539226.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Annually, women in sub-Saharan Africa experience more than 14 million unintended pregnancies due to improper use of short-acting contraceptives [1]. Approximately 775,000 women in Uganda have unintended pregnancies every year due to low uptake of contraception [2]. Although there has been an increase in the use of modern contraceptives, there is still an unmet need for contraception in many developing countries. In Uganda, unmet need for contraception, both traditional and modern, remains high at 28% despite a decline from 34% in 2011 [3]. Women at high risk for acquiring HIV face a high burden of sexually transmitted infections (STI) and unintended pregnancies, with little access to sexual and reproductive health services [4]. An increase in access to and use of effective modern contraceptives is needed among this key population in order to improve their reproductive health [5].
HIV intervention studies target women at high risk for HIV for enrollment in clinical trials. The use of modern contraceptives has become a key inclusion criterion for enrollment [6, 7]. Modern contraceptives are recommended because the effect of trial-investigational products on embryos or fetuses is unknown [8]. Furthermore, the recent UNAIDS guidelines issued a call for comprehensive and sustainable HIV prevention programs emphasizing reliable and affordable access to health-related services, including contraceptives [9]. In order to adequately plan for contraception needs during trial participation, there is an urgent need to assess contraceptive preference among women at risk for HIV, especially in high-risk settings [10]. Promotion and provision of contraception prior to trial onset may also create a pool of women at high risk who can be enrolled in trials. Consistent contraception use may limit trial dropout due to unintended pregnancies [8]. A few studies among this population demonstrated low levels of contraceptive use resulting in unintended pregnancy and abortion [11, 12]. Studies have mostly focused on the influence of community factors and female education in contraceptive use [13, 14], and most have been conducted among women who fully participated in prevention trials [8, 15,16,17]. Other studies related to contraception among women at high risk have investigated the association of family planning methods with HIV incidence [18,19,20], and have not necessarily focused on broader participant characteristics, other than sex-worker status, that influence contraceptive use and the incidence of pregnancy.
We report findings on contraceptive choice and the association with participant characteristics in a cohort of women at risk for HIV who resided in small townships in southwestern Uganda before enrollment in a multicenter, phase 3 microbicide trial. The trial (also known as the Ring Study) is part of collaborative work between the Medical Research Council/Uganda Virus Research Institute (MRC/UVRI), Uganda Research Unit on AIDS, and International Partnership for Microbicides (IPM) that evaluated the safety and efficacy of a dapivirine vaginal ring among healthy, HIV-negative women who were at high risk. The trial recruitment and follow-up procedures have been reported elsewhere [21].
Methods
Study Setting and Population
This study was conducted in preparation for a multicenter, phase 3 microbicide trial (the Ring Study) that evaluated the safety and efficacy of a dapivirine vaginal ring among HIV-uninfected women in Uganda. The microbicide trial recruited healthy, HIV-uninfected women between the ages of 18 and 45 years who were using modern contraception: either depot medroxyprogesterone acetate (DMPA) for at least 6 months or other methods, such as combined oral contraceptives (COC), implants, intrauterine contraceptive devices (IUCD), or surgical sterilization, for at least 3 months prior to screening for the trial.
To identify women at high risk for HIV, we approached those who were residing in 37 small townships in the three neighboring districts of Masaka, Kalungu, and Lyantonde along the Trans-African Highway in Uganda between July 2013 and October 2014. The districts are about 120 km from Kampala, the capital of Uganda. Women working in bars, hotels, restaurants, small shops, hair salons, and other small-scale businesses were prescreened for the study via a door-to-door approach. Trained counselors supported by local community mobilizers offered HIV counseling and testing. During the counseling sessions, information about age and current contraceptive use was collected. Reasons for not using contraception were not collected. Those who were found to be HIV positive at this stage were referred to antiretroviral therapy providers for treatment and care. Women who tested HIV negative and were using modern contraception, or were willing to initiate a method, were invited to the research center for HIV risk assessment and a study screening.
At the research-center screening visit, women using contraception were assessed by trained nurses about the duration of use. Contraceptive use was promoted and provided to those who were not using any method but were willing to initiate one of their choosing. Acceptable contraceptive methods included COC, injectable DMPA, implant (etonogestrel-Implanon® or levonogestrel-Jadelle®), IUCD (Copper T-380A), and surgical sterilization. Condoms were provided but were not considered an acceptable contraceptive method for enrollment in the Ring Study. Sources of contraceptives included the research center and referral to a provider in the community—the nearby Marie Stopes Clinic—for implants, IUCDs, and surgical sterilization. HIV risk was assessed via face-to-face interview using a standardized questionnaire. High risk for HIV acquisition was defined by the presence of any two of the following in the past 3 months: (1) history of STI, (2) self-reported unprotected sex with multiple sex partners or a new partner, and (3) frequent use of recreational drugs (e.g., marijuana, alcohol). During the assessment, those who were diagnosed with an STI were offered treatment using the Uganda national STI syndromic management guidelines [22]. After this screening visit, women were given appointments to return when recruitment into the microbicide trial began. At the recruitment visit, they were evaluated for contraception compliance (at least 6 months for DMPA and at least 3 months for the other methods), a requirement for the Ring Study.
Laboratory Testing
Serial HIV-antibody rapid tests were done using Alere Determine™ HIV-1/2 (Alere Medical Co Ltd, Matsuhidai, Matsudo-shi, Chiba, Japan), followed by OraQuick-ADVANCE® Rapid HIV-1/2 Test (OraQuick-OraSure Technologies Inc, Pennsylvania, USA) to confirm a positive Determine result, with Uni-Gold™ HIV (Trinity Biotech, Ireland) as the tiebreaker. The tests were run by a laboratory technician. A participant was considered to be HIV positive if two antibody rapid tests showed positive results.
Additionally, cervico-vaginal samples were taken and tested for T. vaginalis (OSOM® Trichomonas Test, Sekisui Diagnostics LLC, USA) and C. trachomatis/N. gonorrhoeae (Cobas® Amplicor CT/NG PCR test, Roche Diagnostic Systems, Branchburg, New Jersey, USA), and blood samples were taken for syphilis testing using rapid plasma reagin (RPR) (Wampole® Impact RPR Test Kit, Alere™, Pennsylvania, USA). A positive RPR was confirmed using the Treponema pallidum particle agglutination assay (TPPA) (Serodia TP.PA, Fujirebio Inc, Pennsylvania, USA). A participant was reported to have syphilis if both the RPR and TPPA results were positive. Treatment was provided to those who tested positive for any STI according to the Centers for Disease Control and Prevention (CDC) STD treatment guidelines for 2010 [23].
Statistical Methods
Data on demographic characteristics, sexual behaviors, contraceptive use or agreement to initiate contraception, dates of first and subsequent contacts, and STI test results including HIV status were recorded in Microsoft Excel 2016. Data were exported to STATA version 14 (StataCorp, College Station, Texas, USA) for statistical analysis. All participants who completed at least two visits by the time of enrollment in the microbicide trial were included in this analysis. Participant characteristics were summarized using frequencies and percentages and stratified by contraceptive choice. The proportion of women who indicated a preference for DMPA was used as the referent method in this analysis because most of the participants preferred this method. We used log-binomial regression models to estimate unadjusted and adjusted prevalence proportion ratios (PPR) and 95% confidence intervals (CI) of factors associated with use of DMPA. When the proportion of a primary outcome is greater than 10%, odds ratios can give biased estimates of proportion ratios, so this led to the choice of log-binomial regression instead of logistic regression [24]. Only factors for which the association attained a statistical significance at the 15% level [25] using a likelihood ratio test (LRT) in a univariate analysis were considered for the multivariable model. Only participant age was included a priori. In the final multivariable model, factors were removed using a backward elimination algorithm if removing them did not make the fit of the model significantly worse at the 5% level in an LRT.
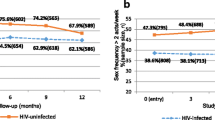
In a secondary investigation, HIV incidence was determined between the initial participant contact date and the later visit date to the research center. Overall HIV incidence was computed as the number who were HIV positive divided by the total person-years at risk. Person-years at risk were calculated as the sum of time from the first date of contact to the date of last HIV-uninfected result date, or to the estimated date of HIV infection, for each participant. Date of HIV infection was estimated as the midpoint of the interval between the last HIV-uninfected result date and the first HIV-infected result date. We did not investigate factors associated with HIV incidence because our study was not empowered to test these associations.
Ethical Considerations
The study protocol was approved by the UVRI Research Ethics Committee and the Uganda National Council of Science and Technology (UNCST). Written informed consent was obtained from women who were willing to be screened. Those who tested HIV positive were referred to an antiretroviral therapy provider of their choice for care and treatment.
Results
Study Screening Profile
Overall, 6725 women were prescreened between July 2013 and October 2014 (Fig. 1). Of these, 780 (12%) were excluded due to HIV infection. Of the 5456 who were HIV uninfected, 325 were excluded based on age (52 women were younger than 18 years, and 273 were older than 45 years). Only 8% (489) were already using modern contraception, or were willing to initiate contraception, and attended the study screening to be assessed for HIV risk. This screening visit typically occurred within 8 months (interquartile range 5–9 months) of the prescreening visit. Of those using contraception or willing to initiate a method, 34% (164) were excluded from the study mainly because of low risk for HIV or refusal to participate due to lack of interest or partner challenges. Of the remaining 325 women who returned for a second visit to confirm contraceptive uptake, 322 were invited into the Ring Study.

Study profile of women screened for contraception use and HIV risk in preparation for microbicide trial in South Western Uganda (July 2013–October 2014)
Baseline Characteristics and Contraception Choices
Table 1 shows the distribution of study participants’ characteristics and contraceptive choices. About half (45%) were aged 25–34 years, 53% had attained primary education, 43% were married, and most (83%) had a main partner. Approximately 39% of the women were bar or hotel/restaurant attendants, 27% owned a small-scale business, 16% were unemployed and 11% worked in a hair salon. The majority of women had had an STI (80%), had had unprotected sex (85%), or had a new partner (78%), and most had used alcohol or recreational drugs (61%). More than half of the women (181, 56%) tested positive for at least 1 STI. Approximately two-thirds (322 of 489, 66%) of the women screened and invited into the Ring Study, were already using or willing to initiate a method of contraception (Fig. 1). The main method used by these women was injectable DMPA (59%), followed by implant (24%) and COC (12%). Of the 489 women screened, 183 who were not using any method chose options in very similar proportion to their counterparts who were already using contraception: DMPA, 106 women (58%); implant, 40 (22%); COC, 33 (18%); and IUCD, 4 (2%). Nine women seroconverted in 206.6 person-years, for an overall HIV incidence of 4.4 per 100 person-years (95% CI 2.3–8.4).
Choice of DMPA and Associated Factors
The choice of DMPA did not differ significantly by participant characteristic, except for whether or not a woman had a main sexual partner. Of those who had a main sexual partner, 61% preferred DMPA, compared with 47% for those who did not (P = 0.06) (Table 2). In the adjusted log-binomial regression models, having a main sexual partner remained of borderline statistical significance (adjusted prevalence proportion ratio [aPPR] = 0.77, 95% CI 0.57–1.04).
Discussion
In this study, we observed that contraception use was high among women who were residing in the small townships in this region and at high risk for HIV infection (63%), compared with the general population (35%) [3]. We observed a higher preference for injectable progesterone contraceptive method (i.e., DMPA), followed by implant and COC. This was similar among women who were already using contraceptives at the time of screening and among women who agreed to initiate contraceptives for the Ring Study; it also conforms to findings from the Uganda Demographic and Health Survey [3]. Preference for DMPA may be due to its free availability in the region and the perception that it is convenient and easy to use [26]. Although other modern contraceptive methods are commonly used in certain regions in eastern and southern Africa, injectables are very popular, representing 40% of contraceptive use [27]. However, concerns have been raised about an increased risk for HIV acquisition with the use of hormonal contraceptives, though this has not been consistent across studies and may be related to methodological limitations rather than to actual increased risk [28, 29]. Based on a review of the current literature and convening of experts on the topic, the World Health Organization has recommended that hormonal contraceptive use (including progesterone-only injectables such as DMPA) among women at high risk for HIV be combined with condom use and other risk reduction strategies [30]. As DMPA was the most prevalent contraceptive used by our study population, following these guidelines carefully will be important in future studies.
We also found that had a main sexual partner was associated with a woman’s contraceptive preference, as those who had a main partner preferred DMPA, compared with other methods. This could be because DMPA offers privacy and is easy and convenient to use [31]. A study in Nigeria found that DMPA was the most-preferred method because women did not want to reveal to their partners that they were using contraceptives [32]. DMPA also might be preferred because the privacy it allows may help minimize disagreements between partners [33].
Study Limitations
This was a preparatory study for screening participants for a microbicide trial. The selection of women during the first contact visit was a convenience sample from areas thought to be associated with higher-risk behavior, and many did not come to the study clinic for further screening. Therefore, the contraceptive use among women in this study needs to be interpreted with caution and may not represent use among the general population. As a preparatory study, no data were collected on the side effects of contraceptives. It was also not possible to determine whether women switched from 1 method to another, and pregnancy rates could not be estimated because these data were collected once and only HIV status was reassessed prior to screening for the main study. We did not investigate the reason(s) for a contraceptive preference. Furthermore, we did not investigate the reasons for refusing to initiate contraceptive use even when the methods were freely provided. This information would have been useful to contraceptive providers in the community. Uptake of DMPA could have been high because it was offered on-site and immediately; women had to go off-site for other methods.
Conclusion
Women at risk for HIV acquisition in this community are willing to initiate modern contraceptives, with a high preference for the injectable contraceptive DMPA. Use of modern contraceptives may reduce intervention trial discontinuation due to pregnancy. Further studies using qualitative methods are needed to better understand why this key population prefers the injectable method.
References
Hubacher D, Mavranezouli I, McGinn E. Unintended pregnancy in sub-Saharan Africa: magnitude of the problem and potential role of contraceptive implants to alleviate it. Contraception. 2008;78(1):73–8.
Singh S, Moore A, Bankole A, Mirembe F, Wulf D. Unintended pregnancy and induced abortion in Uganda: causes and consequences. New York: Guttmacher Institute; 2006.
Statistics UBo. Uganda Demographic and Health Survey: Key Indicators Report. Directorate of Population and Social Statistics, Uganda Bureau of Statistics; 2016.
Scorgie F, Nakato D, Harper E, et al. ‘We are despised in the hospitals’: sex workers’ experiences of accessing health care in four African countries. Cult Health Sex. 2013;15(4):450–65.
Kaida A, Laher F, Strathdee SA, et al. Contraceptive use and method preference among women in Soweto, South Africa: the influence of expanding access to HIV care and treatment services. PLoS ONE. 2010;5(11):e13868.
Karim QA, Karim SSA, Frohlich JA, et al. Effectiveness and safety of tenofovir gel, an antiretroviral microbicide, for the prevention of HIV infection in women. Science. 2010;329(5996):1168–74.
Abaasa A, Gafos M, Anywaine Z, et al. Uptake of hormonal contraceptives and correlates of uptake in a phase III clinical trial in rural South Western Uganda. Reprod Health. 2017;14(1):36.
Reid SE, Dai JY, Wang J, et al. Pregnancy, contraceptive use, and HIV acquisition in HPTN 039: relevance for HIV prevention trials among African women. J Acquir Immune Defic Syndr. 2010;53(5):606.
UNAIDS guidance note on HIV and sex work; 2009. http://www.unaids.org/en/media/unaids/. Accessed 22 August 2016.
Decker MR, Yam EA, Wirtz AL, et al. Induced abortion, contraceptive use, and dual protection among female sex workers in Moscow, Russia. Int J Gynecol Obstet. 2013;120(1):27–31.
Delvaux T, Crabbe F, Seng S, Laga M. The need for family planning and safe abortion services among women sex workers seeking STI care in Cambodia. Reprod Health Matters. 2003;11(21):88–95.
Erickson M, Goldenberg SM, Ajok M, Muldoon KA, Muzaaya G, Shannon K. Structural determinants of dual contraceptive use among female sex workers in Gulu, northern Uganda. Int J Gynecol Obstet. 2015;131(1):91–5.
Stephenson R, Baschieri A, Clements S, Hennink M, Madise N. Contextual influences on modern contraceptive use in sub-Saharan Africa. Am J Public Health. 2007;97(7):1233.
Emina JB, Chirwa T, Kandala N-B. Trend in the use of modern contraception in sub-Saharan Africa: does women’s education matter? Contraception. 2014;90(2):154–61.
Callahan R, Nanda K, Kapiga S, et al. Pregnancy and contraceptive use among women participating in the FEM-PrEP trial. JAIDS J Acquir Immune Defic Syndr. 2015;68(2):196–203.
Akello CA, Bunge KE, Nakabiito C, et al. Contraceptive use and pregnancy incidence among women participating in an HIV prevention trial. J Womens Health. 2017;26(6):670–6.
Sibeko S, Baxter C, Yende N, Karim QA, Karim SSA. Contraceptive choices, pregnancy rates, and outcomes in a microbicide trial. Obstet Gynecol. 2011;118(4):895.
Delvaux T, Buve A. Hormonal contraception and HIV acquisition—what is the evidence? What are the policy and operational implications? Eur J Contracept Reprod Health Care. 2013;18(1):15–26.
Morrison CS, Chen P-L, Kwok C, et al. Hormonal contraception and the risk of HIV acquisition: an individual participant data meta-analysis. PLoS Med. 2015;12(1):e1001778.
Morrison CS, Pai-Lien C, Cynthia K, et al. Hormonal contraception and HIV acquisition: reanalysis using marginal structural modeling. AIDS (London, England). 2010;24(11):1778.
Nel A, van Niekerk N, Kapiga S, et al. Safety and efficacy of a dapivirine vaginal ring for HIV prevention in women. N Engl J Med. 2016;375(22):2133–43.
Health Mo. Uganda national guidelines for the syndromic management of sexually transmitted infections. STD Control Unit of the STD/AIDS Control programme. Ministry of Health, Uganda; 2010.
Centers for disease control and prevention. sexually transmitted diseases treatment guidelines. In: Services UDoHaH, editor. Office of surveillance, epidemiology, and laboratory services, centers for disease control and prevention (CDC), U.S. Department of Health and Human Services, MMWR 2010;59. No. RR-12.
Skove T, Deddens J, Petersen MR, Endahl L. Prevalence proportion ratios: estimation and hypothesis testing. Int J Epidemiol. 1998;27(1):91–5.
Royston P, Ambler G, Sauerbrei W. The use of fractional polynomials to model continuous risk variables in epidemiology. Int J Epidemiol. 1999;28(5):964–74.
Sutherland EG, Otterness C, Janowitz B. What happens to contraceptive use after injectables are introduced? An analysis of 13 countries. Int Perspect Sex Reprod Health. 2011;37(4):202–8.
United Nations. World Contraceptive Patterns. In: Affairs DoEaS, Division P, editors. New York: United Nations; 2013.
Polis CB, Curtis KM, Hannaford PC, et al. An updated systematic review of epidemiological evidence on hormonal contraceptive methods and HIV acquisition in women. AIDS (London, England). 2016;30(17):2665.
Polis CB, Phillips SJ, Curtis KM. Hormonal contraceptive use and female-to-male HIV transmission: a systematic review of the epidemiologic evidence. AIDS. 2013;27(4):493–505.
World Health Organization. Hormonal contraceptive eligibility for women at high risk of HIV. Department of Reproductive Health and Research, World Health Organization. 2017:20.
Chaudhuri S, Rai B, Giri R, Yadav A, Giri S. Acceptability of depot medroxyprogesterone in women attending general outpatient department: a cross sectional study. Health Renaiss. 2017;13(2):7–13.
Amu H, Nyarko SH. Trends in contraceptive practices among women in reproductive age at a health facility in Ghana: 2011–2013. Contracept Reprod Med. 2016;1(1):2.
Kabagenyi A, Jennings L, Reid A, Nalwadda G, Ntozi J, Atuyambe L. Barriers to male involvement in contraceptive uptake and reproductive health services: a qualitative study of men and women’s perceptions in two rural districts in Uganda. Reprod Health. 2014;11(1):21.
Acknowledgements
International Partnership for Microbicides’ (a not-for-profit product-development partnership) work is made possible by generous support from many donors including: the Bill and Melinda Gates Foundation, Irish Aid, the Ministry of Foreign Affairs of Denmark, the Ministry of Foreign Affairs of the Netherlands, the Norwegian Agency for Development Cooperation, the U.K. Department for International Development, the American people through the U.S. Agency for International Development, and the President’s Emergency Plan for AIDS Relief. We thank the study team who worked tirelessly in planning, recruitment and data collection for this study; Anatoli Kamali, Anita Kabarambi, Eugene Ruzagira, Ubaldo Bahemuka, Margaret Kalibbala Lutwama, Sarah Nakato, Faith Ruth Naddunga, Beatrice Kimono Washi, Leah Mbabazi, Agnes Nakazzi Bukenya, Juliet Kyomugisha, Sophie Nalutaaya, Vincent Basajja, Sylvia Masawi, Henry Ssemaganda, Irene Nassuuna, Victoria Mugwaneza, Josephine Bayigga, Jael Nakalema, Richard Mawogole, Joseph Kitumba. Penelope Akankunda, Faith Namutosi, Angel Nansere, Richard Rwanyonga, Benjamin Twefeho, Paul Mayanja, Jennifer Nabatanzi, Kenneth Collin Mawanda, Aeron Namirembe, Kenneth Kugonza, Emanuel Aling, Paul Taire and Andrew Walungama Kiyingi. We also thank Janine Martins, IPM for reviewing the manuscript. We wish to acknowledge the support from the University of California, San Francisco’s International Traineeships in AIDS Prevention Studies (ITAPS), U.S. NIMH, and R25 MH064712. We thank Matt Price, Rhoderick Machekano, Krysia Lindan and Wenjing Zheng for reviewing the manuscript under this program.
Funding
The study was funded and sponsored by the International Partnership for Microbicides (www.ipmglobal.org) (IND # 110,659). For this manuscript, the funder participated in study design and manuscript review, but had no role in data analysis.
Author information
Authors and Affiliations
Contributions
SK, AA, MO, AN designed the study and AA did the analysis. GA contributed to the writing and editing of the manuscript. SK and MO directed the work. All authors contributed to the interpretation of the results and critically commented and provided revisions to the manuscript.
Corresponding author
Ethics declarations
Competing interests
All authors declare that they have no conflict of interest.
Ethical Approval
All study participants provided written informed consent before recruitment. The study was approved by the Uganda Virus Research Institute Research Ethics Committee and Uganda National Council for Science and Technology.
Rights and permissions
About this article

Cite this article
Kusemererwa, S., Abaasa, A., Onyango, M. et al. Contraceptive Preference Among Women at Risk of HIV Acquisition in a Preparatory Screening Study for a Phase III Microbicide Trial in South Western Uganda. AIDS Behav 22 (Suppl 1), 131–138 (2018). https://doi.org/10.1007/s10461-018-2177-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-018-2177-3