
Abstract
Using respondent-driven sampling (RDS), an integrated biological behavioral survey among men that have sex with men (MSM) enrolled 457 participants in Maputo [63.0 % were MSM who had sex with women (MSMW)], 538 in Beira (36.2 % MSMW) and 330 in Nampula-Nacala (54.8 % MSMW) in 2011. Analysis suggests that MSM who have sex only with men (MSMO) had increased odds of having HIV (aOR 2.7) compared to MSMW. HIV among MSMO associated with age, self-reported STI (aOR 4.2), having a single male anal partner (aOR 3.8) and having transactional sex with a man (aOR 3.5) in the past year. Among MSMW, HIV associated with age, lower education (aOR 32.5), being uncircumcised (aOR 3.1) and having transactional sex with a woman (aOR 6.0) in the past year. Findings confirm that MSMO and MSMW have distinct HIV risks in Mozambique; HIV programs for MSM in Southern Africa should take such differences into consideration.
Resumen
Por uso de muestreo dirigido por los participantes (RDS), el estudio biológico y conductual integrado entre los hombres que tienen sexo con hombres (HSH) registro 457 participantes en Maputo (63,0 % HSHM), 538 en Beira (36,2 % HSHM) y 330 en Nampula-Nacala (54,8 % HSHM). El análisis revelo que los HSH que tienen sexo apenas con otros hombres (HSHO) tenían probabilidad más alta de tener VIH que los HSHM (ORa: 2,7). VIH entre los HSHO se asoció con la edad, el auto-relato de ITS (ORa: 4,2), tener un único compañero sexual anal en los últimos 12 meses (ORa: 3,8) y sexo transaccional con un hombre (ORa: 3,5). Entre los HSHM, el VIH se asoció con la edad, menor escolaridad (ORa: 32,5), nunca haber sido circuncidado (ORa: 3,1) y sexo transaccional con una mujer (ORa: 6,0). Los resultados confirman que los HSHO y HSHM tienen riesgos de VIH distintos. Los programas del VIH para los HSH en la África Austral debían tomar en consideración estas particularidades.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Mozambique has a generalized HIV epidemic with a prevalence of 13.1 % among adult women and 9.2 % among adult men in 2009 [1]. While the epidemic is predominantly the result of heterosexual transmission, men who have sex with men (MSM) have been recognized in the National Strategic Plan for HIV/AIDS 2010–2014 (NSP III) as a key population potentially disproportionately affected by HIV in the country [2]. Several studies in Africa have also found men who have sex with men (MSM) to be at higher risk for HIV and as much as four times more likely to have HIV than the general population [3–6]. In addition to the high prevalence of HIV, studies from Botswana, Namibia, Malawi, Senegal, South Africa, and Uganda have noted high prevalence of risk behaviors, such as unprotected anal intercourse between men [5–9], which are generally not addressed in HIV prevention messages in the region.
MSM are not a homogenous group. Men who have sex with men and women (MSMW) represent an important subgroup of MSM. Studies among MSM in sub-Saharan Africa (SSA) have reported that approximately half of MSM had sex with both men and women in a predetermined period before each survey, being 12 months: 74.1 % in Senegal [6] 46.2 % in Cameroon [10], 46.4 % in Swaziland [11], 56.2 % in Cote d’Ivoire [12] and 6 months: 60.9 % in South Africa [8], 46.7 % in Malawi [13], 37.6 % in Botswana [14], 50.7 % in Namibia [7] and past 2 months: 48.1 % in Nigeria [15]. Yet, most studies of MSM in SSA fail to distinguish between men who have sex only with men (MSMO) and men who have sex with men and women in their analysis of HIV risks. Several studies outside of Africa have found that there are important differences between MSMW and MSMO in relation to HIV risk behaviors and use of health and prevention services [16–23]. In a context where HIV prevalence among women is high and often higher than among men, as is the case in Mozambique and much of SSA, prevention and treatment interventions for MSM should consider the unique acquisition and transmission risks among men and between men and women.
To our knowledge, few studies have directly compared HIV risks between MSMO and MSMW in sub-Saharan Africa [15, 24–26]. A cross-sectional convenience sample of MSM in Malawi, Namibia and Botswana found that bisexual partnerships were associated with lower likelihood of prior HIV testing and greater likelihood of having received money for casual sex [24]. A cohort study in Kenya and a cross-sectional survey among MSM in Nigeria both found that MSMO had higher prevalence of HIV than MSMW and that MSMW had greater odds of being an insertive anal partner than MSMO [15, 26]. The current study is the first of its kind in Mozambique and in the region to provide insight into the prevalence of HIV and associated risk factors among MSMO compared with MSMW. The results of this study will add to our understanding of the HIV epidemic among MSM in the context of a generalized epidemic predominantly based on heterosexual transmission. Results can guide the development of prevention and care programs geared towards MSMO, MSMW and their female partners.
Methods
We conducted cross-sectional surveys in 2011 using respondent-driven sampling (RDS) in three cities of Mozambique (Maputo, Beira and Nampula-Nacala) [27]. RDS is a variant of long chain-referral sampling which can produce point estimates representative of the target population [28]. Sampling began with the purposeful selection of MSM “seeds” based on social network size and agreed-upon demographic characteristics (e.g., age, educational level, residential area). Four seeds were initially selected in Maputo, Beira and Nampula-Nacala. Seeds participated in the survey and were subsequently encouraged to refer three MSM from their social networks using study-issued coupons. The MSM recruited by the seeds formed the first wave of recruitment and each of them was instructed to refer three more MSM, and this continued until we observed sample stability (i.e., the point at which the sample composition remained stable across the key demographic and behavioral characteristics) and we approached the target sample size of 500 in each site. We recruited men aged 18 or older who had oral or anal sex with another man in the 12 months preceding the survey.
Informed consent was obtained from all participants for behavioral interviews and for collection of dried blood spot samples for HIV testing. Participants were also given the opportunity to learn their serostatus via on-site rapid HIV testing. Dried blood spot samples were tested at the central laboratory of the National Institute of Health of Mozambique (Instituto Nacional de Saúde). HIV antibody screening was performed using Vironostika HIV Uniform II plus O (Biomerieux SA, France). Non-reactive samples were considered negative, and reactive samples were confirmed using Murex HIV 1.2.O (Murex Biotech Limited, Great Britain). Reactive samples were considered positive, and samples with discordant results were retested using Genscreen HIV 1/2 Version 2 (Bio-Rad, France) which determined the final result. The survey protocol was approved by the National Bioethics Committee for Health of Mozambique, the University of California, San Francisco, and the Center for Global Health of the U.S. Centers for Disease Control and Prevention, Atlanta.
Measures
The survey included questions about demographic characteristics, symptoms and treatment of sexually transmitted infections (STI), circumcision status, transactional sex with men and women (defined as having received or given money, goods or services in exchange for sex), alcohol consumption, history of HIV testing, and utilization of health and prevention services. The survey also included a sexual partner “matrix” (i.e., partner by partner, question by question) that included specific questions on sexual behaviors and condom use among sexual partners in the last 12 months (up to a maximum of five partners), that has been used to collect risk behavior data with MSM in other African settings [5, 8]. To measure problematic consumption of alcohol we used the “Excessive Alcohol Consumption—AUDIT-C (Alcohol Use Disorders Identification Test)” and set the cut-off at ≥4 [29]. A participant was classified as having had an STI or STI symptom if he responded positively to any of these three questions: “In the last 12 months has a doctor or other health professional told you that you had a sexually transmitted disease?”, “Sometimes it happens that men have an abnormal discharge from the penis. Have you had an abnormal discharge from the penis in the last 12 months?” or “Sometimes it happens that men have a sore or ulcer on the penis region. Have you had a wound on the penis or anus in the last 12 months?”. Unprotected sex (vaginal or anal) was defined as not having used a condom at least once during sex with one of the last five partners, and disaggregated by type of sex (insertive anal, receptive anal or vaginal).
Statistical Analysis
For the purpose of this analysis, we excluded participants who when queried about their last five partners did not report anal sex with a man in the previous 12 months. We classified participants as MSMW if they reported having had vaginal or anal sex with a woman and also having had anal sex with a man among their last five partners in the previous 12 months. Participants were classified as MSMO if they reported having had anal sex only with a man among their last five partners in the previous 12 months. All analyses were conducted at the individual participant level, not at the partner level.
Point estimates and 95 % confidence intervals were produced using RDS Analysis Tool (RDSAT) version 7.1 (www.respondentdrivensampling.org), where we also ran diagnostics to assure that the underlying assumptions of RDS had been met [28]. Bivariate analyses and multivariable logistic regression was conducted in R 3.1.1 using individualized weights imported from RDSAT. These weights were based on the outcome of interest for the specific analysis. Weighted χ2 [30] was used to test for differences between MSMW and MSMO in each survey city. Comparisons with significance of p < 0.05 were considered significant. Data from all three sites were merged and analyzed using weighted logistic regression to detect associations with HIV status using city specific weights and retaining survey city dummy variables for control. Models were run jointly to include both groups of interest and then separately so as to assess certain variables specific to the MSMW group. Variables associated with HIV considered for modeling were selected a priori based on the literature; those with a high number of missing values, as well as those with high correlation were not included. Variables were retained in the model based on theoretical importance and using the Akaike Information Criterion (AIC) and possible interactive effects of variables were also examined. A fully interacted model with MSMO versus MSMW binary variable was run to detect differences between the groups (MSMO and MSMW) of which Wald test Z and p value’s are reported in Table 4.
Results
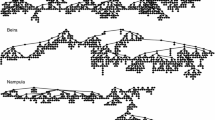
Recruitment took place from June to November 2011, lasting 18 weeks in Maputo and Beira and 22 weeks in Nampula-Nacala. Men participating in the survey were given coupons to distribute to MSM in their network. In total, we recruited six seeds in Maputo (one of which was MSMW), three in Beira (one of which was MSMW), and eight in Nampula-Nacala (three of which were MSMW). Participants distributed 2596, 1857 and 2210 coupons in each site respectively, of which 519 (20 %), 727 (39 %) and 443 (20 %) coupons were returned to the study site by potential participants. Among these potential participants, 496 men in Maputo, 583 in Beira and 353 in Nampula-Nacala participated in the study. Of MSMO survey participants 62.3 % (450/722) recruited other MSMO and of MSMW survey participants 62.5 % (433/693) recruited other MSMW. For the purpose of this analysis, 39 participants were excluded in Maputo, 45 in Beira and 23 in Nampula-Nacala for not having reported any anal sex with a man among their last five partners in the sexual partner matrix. Additionally, 49 participants in Maputo and two in Beira and Nampula-Nacala were excluded because they did not consent to giving a blood sample and therefore have no HIV test result. Figure 1 shows the recruitment chains in the three sites by MSMO and MSMW status.

Respondent-driven sampling recruitment diagrams of men that have sex with men only and men that have sex with men and women, Mozambique, 2011
Demographic and Clinical Characteristics
A comparison of demographic and clinical characteristics between MSMO and MSMW is shown in Table 1. MSMW comprised a large proportion of the sample (63.0 % in Maputo, 36.2 % in Beira and 54.8 % in Nampula-Nacala). HIV prevalence (Table 1) was significantly higher among MSMO than MSMW in Maputo [14.1 %, 95 % confidence interval (CI) 6.4–24.5 vs. 6.2 %, 95 % CI 2.7–10.0, p < 0.01) and Nampula-Nacala (6.4 %, 95 % CI 0.7–14.5 vs. 1.7 %, 95 % CI 0.0–4.1, p = 0.02). While in Beira the opposite was true with prevalence being greater among MSMW than MSMO (12.7 %, 95 % CI 6.0–19.7 vs. 6.9 %, 95 % CI 3.9–10.4, p = 0.03).
In Maputo and Beira, a greater percentage of MSMW than MSMO were employed versus unemployed in the past 12 months (72.1 vs. 40.4 %, p < 0.01 and 59.9 vs. 35.7 %, p < 0.01, in each site respectively). In those same sites, the proportion of MSMO who were students versus not students in the 12 months preceding the survey was greater than among MSMW (76.5 vs. 58.0 %, p < 0.01 in Maputo and 75.2 vs. 67.7 %, p = 0.04 in Beira); while, in Nampula-Nacala a greater percentage of MSMO than MSMW had only primary school level education or lower (41.4 vs. 28.4 %, p = 0.03).
In all three study sites, self-identification as homosexual was significantly higher among MSMO than among MSMW, and 56.6, 74.2 and 70.7 % of MSMO in Maputo, Beira and Nampula-Nacala, respectively, self-identified as homosexual. Additionally, in Beira, a greater percentage of MSMW than MSMO had ever been married with a woman (5.8 vs. 1.8 %, p = 0.02).
Only in Maputo did we find a significant difference between MSMO and MSMW in terms of contact with HIV outreach workers, with 30.1 % of MSMO having had contact with HIV outreach workers in the past 12 months versus 42.7 % of MSMW (p = 0.02). Similarly, in Maputo, a lower percentage of MSMO than MSMW had ever tested for HIV, though this difference did not reach statistical significance (44.3 vs. 55.7 %, p = 0.05).
MSM network sizes were significantly smaller (p < 0.05 based on Wilcoxon rank sum test on unweighted data) among MSMW than among MSMO in Maputo and Nampula-Nacala [median of 6 (IQR 3–12) for MSMO vs. 3 (IQR 2–7) for MSMW in Maputo, median of 5 (IQR 3–7) for MSMO vs. 4 (IQR 3–6) for MSMW in Nampula-Nacala].
In all three sites the percentage having had an STI or STI symptoms in the past 12 months was greater among MSMW than MSMO, but only significantly so in Beira (19.0 vs. 11.7 %, p = 0.01). In terms of HIV risk perception, both in Maputo and Beira, more MSMO than MSMW perceived themselves to have low or no risk of acquiring HIV.
Sexual Risk Behaviors with Other Men
A comparison of sexual behaviors of MSMO versus MSMW with male partners in the past 12 months can be found in Table 2. In all three sites, the number of male anal sex partners that MSMO had in the last 12 months was significantly different than MSMW, with 23.3 % of MSMO versus 9.2 % of MSMW having three or more partners in Maputo (p < 0.01), 16.8 versus 9.8 % in Beira (p = 0.03) and 11.6 versus 5.8 % in Nampula-Nacala (p = 0.01).
More MSMO than MSMW had receptive anal intercourse in that time period; and, similarly, more MSMO than MSMW had unprotected receptive anal intercourse (21.7 vs. 6.7 %, p < 0.01, in Maputo, 15.4 vs. 8.4 %, p = 0.02, in Beira and 32.3 vs. 24.6 %, p = 0.03, in Nampula-Nacala). MSMO were also more likely to have had unprotected insertive anal intercourse than MSMW in Maputo and Beira (41.6 vs. 30.7 %, p = 0.03 and 32.1 vs. 23.8 %, p = 0.05, respectively).
A greater percentage of MSMW than MSMO had received money, goods or services in exchange for sex, with a man (55.7 vs. 39.2 %, p < 0.01, in Maputo and 37.5 vs. 20.6 %, p < 0.001, in Beira) and had a casual or transactional relationship with a male partner (94.5 vs. 72.7 %, p < 0.001, in Maputo and 72.8 vs. 56.3 %, p < 0.01, in Beira). MSMO in Maputo were more likely than MSMW to have given money, goods or services in exchange for sex with a man (14.4 vs. 4.4 %, p < 0.01). MSMW were less likely than MSMO to have had a permanent or stable relationship with a man (13.3 vs. 51.3 %, p < 0.01, in Maputo, 38.6 vs. 66.8 %, p < 0.01, in Beira and 45.0 vs. 59.3 % in Nampula-Nacala, p < 0.01).
Sexual Risk Behaviors with Women
Sexual risk behaviors of MSMW with female partners in the past 12 months are shown in Table 3. At least one in five MSMW had three or more female sex partners in the past 12 months (27.4 % in Maputo, 17.9 % in Beira and 25.4 % in Nampula-Nacala). The majority (>96.4 %) of MSMW had vaginal intercourse in the past 12 months, while 37.4, 24.9 and 37.6 % in each site respectively had anal intercourse with a female partner in that same time period. Unprotected sexual intercourse with a woman was reported by MSMW, with 65.7 % in Maputo, 37.9 % in Beira and 75.6 % in Nampula-Nacala having had unprotected vaginal intercourse in the past 12 months and 15.5, 8.2 and 19.6 % in those sites respectively having had unprotected anal intercourse in that same time period. In Maputo 12.1 % of MSMW had a permanent or stable female partner in the past 12 months while in Beira 38.2 % had such a partner and in Nampula-Nacala 42.2 % of MSMW had such a partner. Additionally, 53.5, 59.3 and 39.6 % of MSMW (in Maputo, Beira and Nampula-Nacala, respectively) had an occasional female sexual partner in the past 12 months.
Risk Factors Associated with HIV Among MSMO and MSMW
Bivariate and multivariate associations with HIV among MSMO and MSMW can be found in Table 4. In bivariate analysis, survey city, age, being a student, being employed, having had an STI and having moderate to high perceived risk of HIV were positively associated with HIV among both MSMO and MSMW, while having had insertive anal intercourse with a man was negatively associated. Self-identification as homosexual, having ever been married or in a conjugal relation with a woman and having had only one male anal sex partner in past 12 months was associated with HIV among MSMO, but not among MSMW. Speaking a language other than Portuguese, having primary education or lower and being uncircumcised was associated with HIV among MSMW, but not among MSMO. Additionally, among MSMW, HIV was also associated with having given or received money, goods or services in exchange for sex with a woman.
In a fully interacted multivariable analysis (not shown), MSMO had nearly three times the odds (OR 2.7, 95 % CI 1.6–4.9) of having HIV versus MSMW, even when controlling for city, age and other demographic and behavioral variables included in Table 4.
In the multivariable model of the MSMO specific sub-group (Table 4), HIV was associated with older age [adjusted odds ratio (aOR) 1.4 per year 95 % CI 1.3–1.6, p < 0.01], report of an STI in the past 12 months (aOR 4.2, 95 % CI 1.6–10.5, p < 0.01), having had a single male anal sex partner (aOR 3.7, 95 % CI 1.6–9.6, p = 0.01), having received money, goods or services in exchange for sex with a man (aOR 3.5, 95 % CI 1.4–9.1, p = 0.01), and with lower risk of HIV infection for those surveyed in Nampula-Nacala (aOR 0.2, 95 % CI 0.1–0.7, p = 0.01, compared to the reference city Maputo). Among MSMW, HIV was associated with older age [aOR 1.3 (per year), 95 % CI 1.2–1.4, p < 0.01], not having been circumcised (aOR 3.1, 95 % CI 1.2–8.3, p = 0.02), having both given and received money, goods or services in exchange for sex with a woman in the past 12 months (aOR 6.0, 95 % CI 1.8–20.5, p < 0.01) and having primary education or lower (aOR 3.5, 95 % CI 1.3–9.8, p = 0.01). Having had insertive anal sex with a man was associated with a lower odds of having HIV among MSMO (aOR 0.3, 95 % CI 0.1–0.8, p = 0.02) as well as among MSMW (aOR 0.1, 95 % CI 0.0–0.6, p < 0.01).
Discussion
We compared demographic characteristics and HIV risks between two subgroups of MSM in Mozambique. Similarly to other studies in sub-Saharan Africa, where MSMW account for between 37.6 and 74.1 % of MSM [5, 6, 14, 26, 31–33], we found that approximately half of MSM in Maputo, Beira and Nampula-Nacala have sexual relations with both men and women, and that this subgroup of MSM has significantly different demographic characteristics and HIV risk behaviors from men who have sex only with men even though we observed cross-recruitment between the two groups in our RDS surveys. The fact that these differences were evident in all three survey sites (Maputo, Beira and Nampula-Nacala) furthers the argument for considering the specific needs of each subgroup in HIV prevention and care, in Mozambique, as well as in other sub-Saharan African countries.
The quantitative evidence in our study reinforces conclusions from a qualitative study conducted among MSM in Maputo which found that sexual networks of MSM overlap with sexual networks of the general population given the fact that segments of the MSM population have sex with both men and women [34].
The high percentage of MSMW having unprotected sex with male and female partners constitutes a high risk of HIV transmission. One direction may be from women to men considering HIV prevalence among adult women (15–49 y.o.) is higher than it is among men (15–49 y.o.) in Mozambique, being 20.5 versus 12.3 %, respectively, in Maputo City, 17.8 versus 12.6 % in Sofala Province (of which Beira is the capital), and 5.5 versus 3.3 % in Nampula Province [1].
MSMW, including men who openly identify themselves as “gay”, as well as those who identify themselves as heterosexual, tend to maintain their identity and same-sex behavior hidden from their family, friends, and female sexual partners in an environment where same-sex behavior is stigmatized. Therefore, it may be difficult to reach them with HIV prevention messages specifically designed for MSM, especially considering that the only HIV prevention programs for MSM in Mozambique are currently provided through a single LGBT organization.
There is evidence that MSMW may be socially isolated from other MSM and may not receive MSM community-based prevention interventions [35]. Our study found that MSMW tend to me more hidden; that is, they have smaller MSM networks, are less likely to be connected to the country’s sole LGBT organization and are less likely to reveal MSM related behaviors to health workers. As such, in the absence of relevant information, this group may be inadvertently increasing the long-term risk of HIV infection both for themselves and their male and female partners. Nevertheless, the fact that our study was successful in recruiting MSMW, through the provision of anonymous services in a discreet location, provides evidence that this group is reachable through careful and inconspicuous contact.
The practice of transactional sex may also constitute an important risk factor in a context where a considerable proportion of both MSMO and MSMW have had recent paid or transactional sex. Our study found that between 2 and 3 in five MSMW received money, goods or services in exchange for sex with a man in the past 12 months, and approximately one in five MSMW received money, goods or services in exchange for sex with a woman in that same period.
While MSMO were less likely to have received money, goods or services for sex with a man than MSMW, they were more likely to have given money, goods or services in exchange for sex with a man. Transactional male–male relationships have been linked to poverty and social inequality and involve power differences in condom use negotiation. A meta-analysis found transactional sex to be associated with a significant increase in HIV prevalence (OR 1.7) among MSM in SSA [36].
Interestingly in multivariable analysis of factors associated with HIV among MSMW, we found those who both gave and received money, goods or services for sex with a woman had significantly greater odds of having HIV, while those who only paid for sex had decreased odds, compared to the reference group of no transactional sex. A cohort study of MSM in Kenya similarly found payment for sex to be a protective factor for HIV acquisition among MSM [37]. This result could be explained by an increased ability to negotiate condom use among those who are only paying for sex.
Not being circumcised was associated with higher prevalence of HIV among MSMW while this association was not detected among MSMO. While studies have found insufficient ecological evidence of circumcision lowering the risk of HIV infection among MSM [38] in parts of the US, Canada, Australia and England, circumcision among MSMW in sub-Saharan Africa could be a protective factor in a generalized epidemic with high prevalence among women and high bisexual behavior. At a minimum and for the present, MSM, because of the high prevalence of sex with women, should not be excluded from programs promoting circumcision among men in the region.
We found that among both MSMW and MSMO, insertive anal intercourse with a man was associated with lower risk of HIV infection. This result is not surprising considering that insertive only anal sex carries lower risk for HIV infection than receptive and combined (insertive and receptive) anal sex [39, 40]. Nevertheless, while HIV risk is considerably lower for insertive versus receptive anal sex (11 vs. 138 per 10,000 exposures), it is greater than for insertive penile vaginal (8 per 10,000 exposures) [41], and in Mozambique MSM may incorrectly perceive that anal intercourse (receptive or insertive), as opposed to vaginal intercourse, does not carry risk for HIV; this belief has been documented in a qualitative study of MSM in Maputo that found some MSM do not associate the practice of anal sex with men with transmission of HIV [34]. A lack of specific messages and programs may contribute to the low perception of risk, as little information is communicated about anal sex in existing HIV prevention programs in Mozambique.
Not only do most HIV prevention materials in Mozambique lack information on the HIV risk associated with unprotected anal sex, but most HIV prevention materials are printed in Portuguese. Our findings reveal that those MSMW who were not fluent in Portuguese had higher odds of being HIV infected. HIV prevention programs should consider the development of orally communicated MSM-specific prevention messages in other local languages tailored to the prevention needs of MSMW.
An important limitation of this study is that the samples were drawn from urban MSM populations and may not be generalizable to Mozambican MSM populations outside of these three urban settings. Non-response bias may also limit generalizability. Additionally, the study was not powered to specifically compare MSMO and MSMW, and true associations could be masked. Lastly, due to the nature of survey (via face-to-face interviews) our results may suffer from social desirability bias with respect to self-reported risk behaviors.
Despite these limitations the study findings have important implications for HIV prevention programs in Mozambique, given the high prevalence of HIV in both MSMO and MSMW and the proportion that this group represents in the adult population, estimated at 1–2 % of the total male population aged ≥15 years in the survey cities [42]. As in other studies conducted among MSM in the region, the results of our study suggest the urgent need to address the HIV prevention and treatment needs of MSM. The risk factors and demographic characteristics associated with HIV prevalence among MSMO and MSMW are different. These differences also suggest the need to consider MSMW and MSMO as distinct subgroups and design HIV prevention and care programs that cater to each separately.
References
Instituto Nacional de Saude (INS), Instituto Nacional de Estatistica (INE) and ICF Macro. Inquérito Nacional de Prevalência, Riscos Comportamentais e Informação sobre HIV e Sida em Moçambique 2009. Mozambique; 2010.
Mozambican Council of Ministers (Conselho de Ministros de Moçambique). Strategic Plan for the National Response towards HIV and Aids, 2010–2014 (Plano Estratégico Nacional de Resposta ao HIV e SIDA, 2010–2014). 2010.
Angala P, Parkinson A, Kilonzo N, Natecho A, Taegtmeyer M. Men who have sex with men (MSM) as presented in VCT data in Kenya. In: XVI international AIDS conference 2006. p. 13–8.
Baral S, Sifakis F, Cleghorn F, Beyrer C. Elevated risk for HIV infection among men who have sex with men in low- and middle-income countries 2000–2006: a systematic review. PLoS Med. 2007;4:e339.
Kajubi P, Kamya MR, Raymond HF, Chen S, Rutherford GW, Mandel JS, et al. Gay and bisexual men in Kampala, Uganda. AIDS Behav. 2008;12:492–504.
Wade AS, Kane CT, Diallo PAN, Diop AK, Gueye K, Mboup S, et al. HIV infection and sexually transmitted infections among men who have sex with men in Senegal. AIDS Lond Engl. 2005;19:2133–40.
Baral S, Trapence G, Motimedi F, Umar E, Iipinge S, Dausab F, et al. HIV prevalence, risks for HIV infection, and human rights among men who have sex with men (MSM) in Malawi, Namibia, and Botswana. PLoS One. 2009;4:e4997.
Lane T, Raymond HF, Dladla S, Rasethe J, Struthers H, McFarland W, et al. High HIV prevalence among men who have sex with men in Soweto, South Africa: results from the Soweto men’s study. AIDS Behav. 2011;15:626–34.
Lane T, Osmand T, Marr A, Shade SB, Dunkle K, Sandfort T, et al. The Mpumalanga men’s study (MPMS): results of a baseline biological and behavioral HIV surveillance survey in two MSM communities in South Africa. PLoS One. 2014;9:e111063.
Park JN, Papworth E, Billong SC, Elat JB, Kassegne S, Grosso A, et al. Correlates of prior HIV testing among men who have sex with men in Cameroon: a cross-sectional analysis. BMC Public Health. 2014;14:1220.
Baral SD, Ketende S, Mnisi Z, Mabuza X, Grosso A, Sithole B, et al. A cross-sectional assessment of the burden of HIV and associated individual- and structural-level characteristics among men who have sex with men in Swaziland. J Int AIDS Soc. 2013;16:18768.
Hakim AJ, Aho J, Semde G, Diarrassouba M, Ehoussou K, Vuylsteke B, et al. The epidemiology of HIV and prevention needs of men who have sex with men in Abidjan, Cote d’Ivoire. PLoS One. 2015;10:e0125218.
Wirtz AL, Kamba D, Jumbe V, Trapence G, Gubin R, Umar E, et al. A qualitative assessment of health seeking practices among and provision practices for men who have sex with men in Malawi. BMC Int Health Hum Rights. 2014;14:20.
Tafuma TA, Merrigan MB, Okui LA, Lebelonyane R, Bolebantswe J, Mine M, et al. HIV/sexually transmitted infection prevalence and sexual behavior of men who have sex with men in 3 districts of Botswana: results from the 2012 biobehavioral survey. Sex Transm Dis. 2014;41:480–5.
Sheehy M, Tun W, Vu L, Adebajo S, Obianwu O, Karlyn A. High levels of bisexual behavior and factors associated with bisexual behavior among men having sex with men (MSM) in Nigeria. AIDS Care. 2014;26:116–22.
Brooks R, Rotheram-Borus MJ, Bing EG, Ayala G, Henry CL. HIV and AIDS among men of color who have sex with men and men of color who have sex with men and women: an epidemiological profile. AIDS Educ. Prev. Off. Publ. Int. Soc. AIDS Educ. 2003;15:1–6.
Gorbach PM, Murphy R, Weiss RE, Hucks-Ortiz C, Shoptaw S. Bridging sexual boundaries: men who have sex with men and women in a street-based sample in Los Angeles. J Urban Health Bull N Y Acad Med. 2009;86(Suppl 1):63–76.
Harawa N, Wilton L, Wang L, Mao C, Kuo I, Penniman T, et al. Types of female partners reported by black men who have sex with men and women (MSMW) and associations with intercourse frequency, unprotected sex and HIV and STI prevalence. AIDS Behav. 2014;18:1548–59.
Maulsby C, Sifakis F, German D, Flynn CP, Holtgrave D. HIV risk among men who have sex with men only (MSMO) and men who have sex with men and women (MSMW) in Baltimore. J Homosex. 2013;60:51–68.
Mercer CH, Hart GJ, Johnson AM, Cassell JA. Behaviourally bisexual men as a bridge population for HIV and sexually transmitted infections? Evidence from a national probability survey. Int J STD AIDS. 2009;20:87–94.
Ramakrishnan L, Ramanathan S, Chakrapani V, Goswami P, Deshpande S, Yadav D, et al. Comparison of sexual risk, HIV/STI prevalence and intervention exposure among men who have sex with men and women (MSMW) and men who have sex with men only (MSMO) in India: implications for HIV prevention. AIDS Behav. 2015;19(12):2255–69.
Tieu H-V, Spikes P, Patterson J, Bonner S, Egan JE, Goodman K, et al. Sociodemographic and risk behavior characteristics associated with unprotected sex with women among black men who have sex with men and women in New York City. AIDS Care. 2012;24:1111–9.
Wheeler DP, Lauby JL, Liu K, Van Sluytman LG, Murrill C. A comparative analysis of sexual risk characteristics of Black men who have sex with men or with men and women. Arch Sex Behav. 2008;37:697–707.
Beyrer C, Trapence G, Motimedi F, Umar E, Iipinge S, Dausab F, et al. Bisexual concurrency, bisexual partnerships, and HIV among Southern African men who have sex with men. Sex Transm Infect. 2010;86:323–7.
Larmarange J, Wade AS, Diop AK, Diop O, Gueye K, Marra A, et al. Men who have sex with men (MSM) and factors associated with not using a condom at last sexual intercourse with a man and with a woman in Senegal. PLoS One. 2010;5(10):e13189. doi:10.1371/journal.pone.0013189.
Sanders EJ, Graham SM, Okuku HS, van der Elst EM, Muhaari A, Davies A, et al. HIV-1 infection in high risk men who have sex with men in Mombasa, Kenya. Aids. 2007;21:2513–20.
Nalá R, Cummings B, Horth R, Inguane C, Benedetti M, Chissano M, et al. Men who have sex with men in Mozambique: identifying a hidden population at high-risk for HIV. AIDS Behav. 2015;19:393–404.
Salganik MJ, Heckathorn DD. Sampling and estimation in hidden populations using respondent-driven sampling. Sociol Methodol. 2004;34:193–240.
Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA, et al. The audit alcohol consumption questions (audit-c): an effective brief screening test for problem drinking. Arch Intern Med. 1998;158:1789–95.
Pasek J, Tahk with some assistance from A, Culter some code modified from R-core. A contributions by G, Schwemmle M. weights: weighting and weighted statistics [Internet]. 2014. http://CRAN.R-project.org/package=weights.
Dahoma M, Johnston LG, Holman A, Miller LA, Mussa M, Othman A, et al. HIV and related risk behavior among men who have sex with men in Zanzibar, Tanzania: results of a behavioral surveillance survey. AIDS Behav. 2011;15:186–92.
Hladik W, Barker J, Ssenkusu JM, Opio A, Tappero JW, Hakim A, et al. HIV infection among men who have sex with men in Kampala, Uganda—a respondent driven sampling survey. PLoS One. 2012;7:e38143.
Merrigan M, Azeez A, Afolabi B, Chabikuli ON, Onyekwena O, Eluwa G, et al. HIV prevalence and risk behaviours among men having sex with men in Nigeria. Sex Transm Infect. 2011;87:65–70.
da Silva D, Joseph D, Gune E, Mussa F, Wheeler J, Benedetti M, et al. Study about vulnerability and risk to HIV infection among men who have sex with men in Maputo City. Maputo: LAMBDA, PSI, Pathfinder International, UNFPA; 2010.
Kumta S, Lurie M, Weitzen S, Jerajani H, Gogate A, Row-kavi A, et al. Bisexuality, sexual risk taking, and HIV prevalence among men who have sex with men accessing voluntary counseling and testing services in Mumbai, India. J Acquir Immune Defic Syndr. 2010;53:227–33.
Oldenburg CE, Perez-Brumer AG, Reisner SL, Mimiaga MJ. Transactional sex and the HIV epidemic among men who have sex with men (MSM): results from a systematic review and meta-analysis. AIDS Behav. 2015;19(12):2177–83.
Sanders EJ, Okuku HS, Smith AD, Mwangome M, Wahome E, Fegan G, et al. High HIV-1 incidence, correlates of HIV-1 acquisition, and high viral loads following seroconversion among men who have sex with men in Coastal Kenya. AIDS Lond Engl. 2013;27:437–46.
Millett GA, Flores SA, Marks G, Reed JB, Herbst JH. Circumcision status and risk of HIV and sexually transmitted infections among men who have sex with men: a meta-analysis. JAMA. 2008;300:1674–84.
Baggaley RF, White RG, Boily M-C. HIV transmission risk through anal intercourse: systematic review, meta-analysis and implications for HIV prevention. Int J Epidemiol. 2010;39:1048–63.
Meng X, Zou H, Fan S, Zheng B, Zhang L, Dai X, et al. Relative risk for HIV infection among men who have sex with men engaging in different roles in anal sex: a systematic review and meta-analysis on global data. AIDS Behav. 2015;19:882–9.
Patel P, Borkowf CB, Brooks JT, Lasry A, Lansky A, Mermin J. Estimating per-act HIV transmission risk: a systematic review. AIDS Lond Engl. 2014;28:1509–19.
National Institute of Health of Mozambique (INS), Centers for Disease Control and Prevention (CDC), University of California San Francisco (UCSF), Population Services International (PSI), International Training and Education Center for HIV (I-TECH), Pathfinder International. Final Report: the Integrated Biological and Behavioral Survey among Men who have Sex with Men, Mozambique, 2011 [Internet]. San Francisco: INS, CDC, UCSF, PSI, I-TECH and Pathfinder; 2013. http://globalhealthsciences.ucsf.edu/gsi/IBBS-MSM-Final-Report.pdf.
Acknowledgments
The authors would like to thank the study participants for accepting to be part of this study, the study field team and members of the integrated biological and behavioral surveillance Mozambique technical working group for their dedication in the study planning and execution processes, as well as all implementing institutions for their support in all phases of the study. This research has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the US Department of Health and Human Services and the Centers for Disease Control and Prevention (CDC) Mozambique Country Office under the terms of Cooperative Agreement Number U2GPS001468. The views expressed in this report do not necessarily reflect the views of the US Centers for Disease Control and Prevention or the U.S. Government.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sathane, I., Horth, R., Young, P. et al. Risk Factors Associated with HIV Among Men Who Have Sex Only with Men and Men Who Have Sex with Both Men and Women in Three Urban Areas in Mozambique. AIDS Behav 20, 2296–2308 (2016). https://doi.org/10.1007/s10461-016-1390-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-016-1390-1