
Abstract
This study investigated help-seeking intentions and use of mental health services within a sample of 1128 Mainland Chinese college students (630 males and 498 females; mean age = 20.01 years, SD = 1.48). Results of structural equation modeling and logistic regression analysis suggested that social-cognitive variables had significant effects both on students’ intentions to seek professional mental health care and their actual service use. To promote help-seeking, practitioners should consider marketing campaigns and psycho-education for students and communities, enhancing knowledge and acceptance of mental health problems and effective treatment options.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Compared with college students elsewhere, Mainland Chinese college students report even higher levels of psychological distress, and, despite increasing provision of mental health services (MHS) by most mainland universities, less willingness to access professional support (cf., Boey 1999; Guo et al. 2013; Li et al. 2008; Ministry of Education of the People's Republic of China 2001; Phillips et al. 2009; Wang et al. 2007). Correlates of service use have been examined in Hong Kong, Taiwan, Macao and with Chinese people living abroad (e.g., Chang 2008; Chin et al. 2015; Mak and Davis 2014); however, these findings may not generalize to Mainland Chinese students due to political and cultural differences (Boey 1999; Chen et al. 2014; Li et al. 2013; Wong and Li 2014). Indeed, differences in help-seeking attitudes have been found between overseas Chinese and Mainland Chinese college students (Goh et al. 2007). Further investigation of mental health help-seeking among college students in Mainland China is, therefore, needed (Clement et al. 2015; Li et al. 2008; Wu et al. 2014).
Several theoretical models are used to understand willingness and reluctance to undertake health-promoting behaviors including help-seeking. The Theory of Planned Behavior (TPB; Ajzen 1985, 1991) is one example. The TPB suggests that intention is an immediate determinant of actual behavior, and it is considered to be affected by three factors: attitudes, subjective norms, and perceived behavioral control (Ajzen 1991; Ajzen and Fishbein 2005; Ajzen and Madden 1986). In relation to MHS, a favorable attitude or evaluation of accessing professional support may imply greater willingness to seek professional psychological help. Subjective norms, including individuals’ perceptions of social expectations concerning professional psychological help, can also influence MHS use among college students: if significant others expect them to seek treatment, they will be more likely to do so. Similarly, the greater the degree of perceived behavioral control, or one’s predictions of personal control over utilizing MHS, the stronger the intention to access professional support (Mak and Davis 2014).
The TPB has a strong evidence base, with previous research, mostly in North America, having elucidated the mediating effect of attitudes on the relationships between various psychosocial variables (e.g., subjective norms) and help-seeking intentions (cf., Kim and Omizo 2003; Kim and Park 2009; Shaffer et al. 2006; Vogel et al. 2005; Yakunina and Weigold 2011). The significance of subjective norms and perceived behavioral control in the prediction of intentions has also received empirical support, based on research conducted in Hong Kong and Macao. The suggestion is that perceptions of significant others may exert particular influence on Chinese help-seeking patterns, because harmonious interpersonal relationships are highly valued in Chinese culture (Mak and Davis 2014; Mo and Mak 2009; Sue and Morishima 1982; Xie and Leong 2008). Indeed, research indicates that subjective norms not only directly affect help-seeking intentions among Hong Kong and Macao Chinese people, but also predict individual attitudes and perceived behavioral control concerning MHS usage (Mak and Davis 2014; Mo and Mak 2009). However, it is unknown whether the same findings apply to Mainland Chinese college students. Moreover, perceived behavioral control is considered to have direct effects on actual behavior (Ajzen 1985, 1991), although this has not been explored in the area of help-seeking.
Other significant predictors of help-seeking intentions include stigma concerns, anticipated benefits and anticipated risks. Both public stigma (externalized) and self-stigma (internalized) have been proposed as major barriers for Chinese people needing MHS (Corrigan 2004; Mak and Davis 2014; Wang et al. 2012). Notably, indirect effects of public stigma and self-stigma on help-seeking intentions have been demonstrated in various mediation models (Choi and Miller 2014; Vogel, Wade, & Hackler, 2007; Vogel et al. 2005; Yakunina and Weigold 2011); however, no previous research has evaluated this among Chinese college students. Similarly, indirect relationships between anticipated benefits (perceived benefits after receiving mental health treatment), anticipated risks (perceived risks of using MHS), and help-seeking intentions have been found in mediation models that include attitudes as a mediator (Shaffer et al. 2006; Vogel and Wester 2003; Vogel et al. 2005). But, to date, we have not identified any published studies investigating anticipated benefits and risks of mental health help-seeking in Chinese societies.
Although the TPB has been demonstrated as an effective theoretical framework for understanding a wide range of health behaviors (Armitage and Conner 2001; Godin and Kok 1996), a low correlation between intent and actual MHS use has been reported (Chin et al. 2015; Webb and Sheeran 2006; Wilson et al. 2008). Accordingly, researchers acknowledge the need to examine actual utilization (Chen et al. 2014; Kim and Park 2009; Li, Dorstyn, & Denson, 2014; Nam et al. 2013; Vogel, Wester, & Larson, 2007).
A key theoretical model of service utilization is Andersen’s Behavioral Model (Andersen 1995; Andersen and Newman 1973). According to Andersen (1995), individuals’ use or non-use of services is predicted and explained in terms of predisposing, enabling and need factors. Predisposing factors include socio-demographic characteristics (e.g., gender, culture and education) and people’s beliefs (i.e., attitudes, values, and knowledge) about disorders and treatments (Andersen 1995; Andersen and Newman 1973). The limited extant research on Chinese MHS utilization has observed that service use is independent of gender, but associated with higher educational levels (Chang 2008; Li et al. 2013; Shen et al. 2006). Furthermore, research with Asians living abroad has validated an indirect relationship between adherence to Asian cultural values and intent to seek mental health care (Choi and Miller 2014; Kim and Park 2009; Liao et al. 2005; Yakunina and Weigold 2011). Once again, this is unexplored in Mainland Chinese samples.
Enabling variables relate to family (e.g., residential area, health insurance, income, social support) and community resources (i.e., availability and accessibility of professional services; Andersen 1995; Andersen and Newman 1973). Previous studies in Mainland China have indicated that living in an urban area, higher family income and health insurance are each associated with higher use of services (Chen 2012; Gao et al. 2001; Li, Sun, Zhang, Shi, & Kolstad, 2014; Li et al. 2013; Liu et al. 2008; Park et al. 2005). In terms of social support, some researchers report that it is a negative predictor of service use: Chinese people are more likely to seek informal help from family and friends, in line with the Asian cultural value that personal issues should be resolved within the circle of significant others (Chang 2008; Chin et al. 2015; Huang et al. 2008; Kim et al. 1999). There is, however, also evidence suggesting that if significant others hold positive attitudes toward accessing MHS and encourage usage, then Chinese individuals are more likely to seek professional support, consistent with cultural norms of conformity to family expectations (Goh et al. 2007; Mak and Davis 2014; Wong and Li 2014). These potentially opposing social influences may challenge the development and evaluation of interventions promoting help-seeking.
Need variables, comprising perceived (individuals’ self-assessment of mental health status) and evaluated (professional diagnoses of mental illnesses) needs, are positively associated with service use in the Western literature (Andersen and Newman 1973; Andrade et al. 2014; Eisenberg et al. 2012; Zivin et al. 2009). However, few studies have addressed the effects of need variables within Chinese societies and their findings vary: positive correlations between level of illness severity, number of symptoms and willingness to use MHS have been reported (Chang 2008; Chen et al. 2014; Shen et al. 2006), whereas other studies have reported no significant association between illness severity and service usage (Chin et al. 2015; Li et al. 2013; Mak and Davis 2014).
In summary, mediated effects of attitudes, subjective norms, and perceived behavioral control on the relationships between different biopsychosocial variables (e.g., Asian cultural values) and help-seeking intentions have been identified. Moreover, as Ajzen and Fishbein (2005) propose, background variables such as gender, knowledge and culture, may have indirect effect on the prediction of intentions. However, previous research has failed to employ an integrated model to explore the interactions between these variables simultaneously.
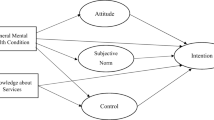
The current study, therefore, developed a model of Chinese students’ help-seeking intent by integrating Ajzen’s (1991) TPB and Andersen’s (1995) Behavioral models. Based on the available theoretical and empirical literature, we hypothesized that predisposing, enabling, and need variables, together with other influential factors identified by previous research, would predict student attitudes, subjective norms, and perceived behavioral control, which, in turn, would predict help-seeking intentions. Moreover, we considered that subjective norms would predict attitudes and perceived behavioral control (see Fig. 1). We also hypothesized that the relationships between the above-mentioned variables and help-seeking intentions would be mediated separately by attitudes, subjective norms, and perceived behavioral control.

The proposed explanatory model
In order to address the gap in the empirical literature relating to actual MHS use, our study additionally examined the predictive effects of various biopsychosocial variables on Chinese students’ actual utilization of MHS. We hypothesized that help-seeking intentions and perceived behavioral control, which have been proposed as being significant and direct predictors of actual behavior (Ajzen 1991), would predict service use before and after predisposing, enabling, and need variables were added successively. Moreover, predisposing, enabling, and need variables would also predict Chinese students’ use of MHS (see Table 1 for included variables).
Method
Participants
A total of 1128 students from universities in Shandong Province (part of the Eastern China region and totaling a population of 97,333,900) were recruited. This included 630 males (55.9%) and 498 females (44.1%), with ages ranging from 17 to 45 years (M = 20.01, SD = 1.48). The sample mainly consisted of undergraduate students (99.8%) across academic majors. Most participants self-identified as Han Chinese (98.4%) and grew up in Shandong (90.2%). Only 3.3% (n = 37) reported having used MHS in the preceding 12 months, and, of those, 54.1% (n = 20) had accessed university counseling services.
Measures
Demographic Information
Participants provided information concerning their age, gender, years in university, academic major, ethnic background, parents’ marital status and education levels, family residential area, household income, and health insurance.
Attitudes
The Attitudes Toward Seeking Professional Psychological Help Scale-Short Form (ATSPPH-SF) is a brief 10-item version of the 29-item ATSPPH (Fischer and Turner 1970), developed by Fischer and Farina (1995) to assess attitudes toward counseling. Items are responded to on a 4-point Likert scale ranging from 1 (disagree) to 4 (agree), with higher total scores indicating more positive attitudes. Psychometric properties, including a high test correlation with the original ATSPPH (r = .87), indicate a one month test-retest reliability of .80, and internal consistency ranging from .65 to .82 for Chinese college students (Chang 2008; Fang et al. 2011; Hao and Liang 2007; Wong and Li 2014; Yeh 2002). For the current study, the internal consistency of the Chinese translation (Wong and Li 2014) was .45.
Subjective Norms
A 10-item scale designed by Hammer and Vogel (2013), in accordance with Ajzen and Fishbein’s (2005) guidelines, was used to measure the factor of subjective norms. Items are rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores being indicative of more positive subjective norms. The internal consistency has been reported as .94 (Hammer and Vogel 2013). Cronbach’s alpha was .95 in the current sample.
Perceived Behavioral Control
A 3-item scale developed by Mo and Mak (2009) was used to assess the factor of perceived behavioral control. Each item is rated on a 6-point Likert scale (1 = strongly disagree to 6 = strongly agree). Higher scores reflect higher levels of behavioral control. The internal consistency has been reported as .77 among a sample of Hong Kong Chinese (Mo and Mak 2009). Cronbach’s alpha for the present sample was .87.
Public Stigma
The Perceptions of Stigmatization by Others for Seeking Help scale (PSOSH; Vogel et al. 2009) was included to measure students’ fear of being stigmatized by significant others for utilizing MHS. Five items are rated on a 5-point Likert scale (1 = Not at all to 5 = A great deal). Higher total scores represent greater public stigma concern. Construct validity has been demonstrated through positive relationships with self-stigma toward help-seeking (r = .37) and public stigma of mental illness (r = .20; Vogel et al. 2009). Internal consistency estimates ranged from .78 to .92 and the 3-week test-retest reliability was .82 (Cheng et al. 2013; Choi and Miller 2014; Vogel et al. 2009; Yakunina and Weigold 2011). Cronbach’s alpha was .89 in the current sample.
Self-Stigma
The 10-item Self-Stigma of Seeking Help Scale (SSOSH; Vogel et al. 2006) was used to assess participants’ self-stigma in the event of using MHS. Each item is rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Higher total scores reflect a higher level of perceived self-stigma. The SSOSH has demonstrated positive associations with anticipated risks (r = .47) and public stigma (r = .48), and negative relationships with anticipated benefits (r = −.45), attitudes toward counseling (r = −.63), and help-seeking intentions (r = −.38; Vogel et al. 2006). The internal consistency has ranged from .75 to .92 in various samples with a test-retest reliability of .72 (2 weeks; Chen et al. 2014; Cheng et al. 2013; Choi and Miller 2014; Tucker et al. 2013; Vogel et al. 2013a; Vogel et al. 2006; Wade et al. 2015). Cronbach’s alpha for the Chinese translation (Vogel et al. 2013a) was .60 in the present study.
Anticipated Benefits and Risks
The Disclosure Expectations Scale (DES) is an 8-item measure designed by Vogel and Wester (2003) to assess the anticipated benefits and risks of receiving mental health treatment. Each of the two factors is measured by four items rated on a 5-point Likert scale ranging from 1 (Not at all) to 5 (Very). Total scores are summed for each subscale, with higher scores reflecting more anticipated benefits or more anticipated risks. The benefits subscale has been shown to be positively associated with attitudes toward counseling, help-seeking intentions and self-disclosure, whereas negative correlations have been reported between the risks subscale and the above constructs (Vogel and Wester 2003). The internal consistency has ranged from .80 to .87 for the benefits subscale and from .74 to .82 for the risks subscale (Shaffer et al. 2006; Vogel et al. 2008a; Vogel et al. 2008b; Vogel and Wester 2003; Vogel et al. 2005). The 2-week test-retest reliability was .75 for benefits and .77 for risks (Shaffer et al. 2006). In the current study, Cronbach’s alphas were .81 (benefits) and .76 (risks).
Adherence to Asian Values
The Asian Values Scale (AVS; Kim et al. 1999) evaluates respondents’ adherence to Asian values, including emotional self-control, family recognition through achievement, obeying social norms, collectivism, humility, and filial piety. A total of 36 items are rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree); higher total scores denoting greater adherence to Asian values. The internal consistency has ranged from .78 to .86 and the 2-week test-retest reliability was .83 (Hamid et al. 2009; Kim et al. 1999; Kim and Omizo 2003; Liao et al. 2005; Shea and Yeh 2008). Evidence of construct validity has also been provided in previous research (Kim et al. 1999). Cronbach’s alpha obtained in this study was .68.
Social Support
The Social Provisions Scale (SPS; Cutrona and Russell 1987) is a 24-item self-report measure developed to assess the quality of perceived social support. Items are rated on a 4-point Likert scale (1 = strongly disagree to 4 = strongly agree). A total score is computed by summing all items, with higher scores indicating higher perceived social support. Adequate internal consistency (.85–.93) and test-retest reliability estimates (.84–.92) have been identified across samples (Cutrona and Russell 1987; Kahn and Williams 2003; Leech 2007; Vogel and Wester 2003; Vogel et al. 2005). With respect to construct validity, significant correlations with other self-report measures of social support have been demonstrated (Cutrona and Russell 1987). Cronbach’s alpha for the current sample was .88.
Psychological Distress (Symptoms)
The Hopkins Symptom Checklist-21 (HSCL-21; Green et al. 1988) is a self-report symptom inventory that has been widely used to measure psychological distress (including general feelings of distress, somatic distress, and performance difficulty) in relation to MHS utilization. Twenty-one items are rated on a 4-point Likert scale (1 = not at all to 4 = extremely), with higher scores suggesting greater distress. The HSCL-21 has been found to be associated with other measures of distress and to be effective in measuring changes in distress during therapy (Deane et al. 1992). High internal consistency has been reported in various samples ranging from .87 to .90 (Cepeda-Benito and Short 1998; Green et al. 1988; Leech 2007; Vogel et al. 2008b; Vogel and Wester 2003; Vogel et al. 2005). Cronbach’s alpha for the current sample was .95.
Psychological Distress (Severity)
The Kessler Psychological Distress Scale (K10) is a 10-item screening measurement of non-specific psychological distress used to assess the level of morbidity (Kessler et al. 2002; Kessler et al. 2003). Each statement is rated on a 5-point Likert scale ranging from 1 (none of the time) to 5 (all of the time); higher scores indicating higher level of severity of distress. Cronbach’s alphas have ranged from .80 to .92 in Chinese samples, and the validity of the K10 has been confirmed across studies conducted in China (Chen 2012; Chen and Zhu 2015; Shen et al. 2006; Wen et al. 2010; Zhou et al. 2008). Cronbach’s alpha was .95 in the present study.
Intention to Seek Professional Psychological Help
The 24-item Willingness to See a Counselor scale (WSC; Gim et al. 1990) is an extended version of Cash et al.’s (1975) 17-item Intention to Seek Counseling Inventory: the additional items addressing issues relevant to ethnic minority students. The WSC is used to assess college students’ intention to seek professional psychological help for a range of psychosocial concerns (Gim et al. 1990; Robertson and Fitzgerald 1992). Each item is rated on a 4-point Likert scale ranging from 1 (not willing) to 4 (willing), with higher scores representing stronger intent to seek MHS. Internal consistency has ranged from .92 to .94 among Asian and Asian American college students (Choi and Miller 2014; Kim and Omizo 2003; Kim and Park 2009). Cronbach’s alpha for the current sample was .96.
Use of Mental Health Services
The utilization of MHS was assessed by asking a single question: “In the past 12 months, have you taken any prescribed psychotropic medications (e.g., anti-depressants, anti-panic or anti-anxiety agents) or used any professional mental health services for your personal or emotional problems?” For the purpose of this study, MHS was broadly defined as involving community mental health services, counseling services, general practitioners, hospital emergency departments, inpatient and outpatient mental health-related care, psychiatrists, psychologists, psychotherapists, social workers, or telecounseling. If participants responded Yes, they were required to answer follow-up questions regarding the type of service, the frequency of contacts, the satisfaction of utilization, and their current use of services.
Open-Ended Questions
Four open-ended questions in relation to motivation, barriers, and benefits concerning professional psychological help-seeking, and suggestions for MHS delivery, were developed by the first author in order to elicit students’ own opinions concerning service utilization.
Procedure
The DES, SPS, WSC, AVS, HSCL-21, and subjective norms scale, originally developed in English, were translated into Mandarin Chinese by an accredited translation firm following translation and back-translation procedures. These Chinese versions were then pilot tested by two Chinese people who were fluent in English in order to check expression of language.
After receiving ethical approval from the relevant ethics subcommittee, widespread informal contact with staff members and students from universities in China was made by the first author. Participants were recruited via in-class announcements inviting them to voluntarily participate in online research about Chinese college students’ utilization of MHS. Students were also informed that they had equal chances to win a gift card valued at AUD $100.
The online survey (powered by SurveyMonkey™) contained two sections. The first compulsory section comprised an information sheet, consent form, demographic questionnaire, and the various psychosocial measures. The second, optional section, included the four open-ended questions. To minimize missing data, the online survey could only be submitted if all questions in the first section had been answered.
Data analyses were conducted using IBM SPSS Statistics 21. Structural Equation Modeling (SEM) utilized IBM SPSS Amos 21 (IBM Corp 2012).
Results
Descriptive Analyses
Descriptive statistics and correlations for the measures are presented in Table 2. In relation to the key variables that TPB considers as predictors of intentions (i.e., intentions to seek professional psychological help): attitudes, subjective norms and perceived behavioral control were significantly related to most or all other psychosocial variables, with small to medium associations demonstrated.
Testing the Structural Model of Help-Seeking Intentions
Several stages were involved in testing the model. Firstly, confirmatory factor analysis was conducted to develop and examine the adequacy of a measurement model (Anderson and Gerbing 1988; Byrne 2010; Martens 2005). Secondly, following the recommendation of Holmbeck (1997) and Martens (2005), the hypothesized structural model was compared with an alternative model to determine which one had a better fit to the data. Thirdly, the significance of the indirect effects was further examined using a bootstrap procedure (Shrout and Bolger 2002).
Item Parceling
To avoid violating the assumption of normality and to improve model fit by reducing the number of estimated parameters, item parcels were created as observed indicators for each of 9 latent variables (Bandalos 2002; Little et al. 2002; Russell et al. 1998). Three parcels were built for the following latent variables: adherence to Asian values, self-stigma, public stigma, social support, subjective norms, attitudes, and help-seeking intentions, respectively. Two parcels were created for anticipated benefits and risks. Consistent with Andersen (1995), single items of perceived need for psychological help and self-rated mental health status were utilized as observed indicators for perceived need. Likewise, illness symptoms and severity provided two indicators of evaluated need.
Normality
The maximum likelihood estimation, which assumes normality, was used. Although it is robust under the condition of excessive kurtosis, the normality of each observed variable was examined (Hoyle 1995; Kaplan 2009). As recommended by Field (2009), interpretations of skewness and kurtosis values were made in conjunction with histograms and probability-probability plots: all variables were approximately normally distributed. The large sample size also ensured that the normality assumption was reasonably robust for further analyses.
Fit Indices
Based on the literature (Hu and Bentler 1999; Kline 2005; Martens 2005), model fit was assessed using chi-square goodness-of-fit test (χ2), the comparative fit index (CFI), the root-mean-square error of approximation (RMSEA), and the standardized root-mean-square residual (SRMR). According to Hu and Bentler (1999), a CFI equal to or greater than .95; RMSEA equal to or smaller than .06; and SRMR equal to or smaller than .08 represent good model fit.
Measurement Model
The measurement model yielded a good fit to the data: χ2 (418, N = 1128) = 1356.31, p < .001; CFI = .96; RMSEA = .05 (90%CI = .04–.05); and SRMR = .05. All parcels significantly loaded on the latent variables (p < .001).
Structural Model
The hypothesized model demonstrated good data fit: χ2 (424, N = 1128) = 1371.45, p < .001; CFI = .96; RMSEA = .05 (90%CI = .04–.05); and SRMR = .05. As shown in Fig. 2, gender, evaluated need, anticipated benefits, anticipated risks and self-stigma emerged as significant predictors of attitudes. These predictors, along with subjective norms, explained 42% of the variance. Both evaluated need and anticipated risks also had significant effects on subjective norms, predicting 26% of its variance. Adherence to Asian values, social support, anticipated risks, self-stigma, public stigma, and subjective norms significantly predicted perceived behavioral control, accounting for 28% of the variance. Although attitudes and subjective norms were significantly related to intentions, perceived behavioral control was not. Furthermore, evaluated need, anticipated benefits, anticipated risks, and self-stigma directly predicted intentions. All of the predictors explained 37% of variance in help-seeking intent. It is noteworthy that perceived need failed to predict any of the four dependent variables.

The structural model. N = 1128. Values shown are standardized parameter estimates. Only significant structural paths are shown in the Figure. Item parcels, measurement errors, factors loadings, residual errors and inter-correlations between independent variables are omitted for clarity. *p < .05. **p < .01. ***p < .001
An alternative model was also examined by constraining to zero the direct paths from nine independent variables to help-seeking intentions (Path c; see Fig. 1). These results showed an adequate model fit: χ2 (433, N = 1128) = 1572.87, p < .001; CFI = .95; RMSEA = .05 (90%CI = .046–.051); and SRMR = .06. Given this, the two competing models (i.e., the proposed model and the alternative model) were further compared by performing a chi-square difference test. The significant chi-square statistic (Δχ2 (9) = 201.42, p < .001) indicated a better fit of the hypothesized model to the data. As this model was more effective in predicting help-seeking intentions, it was used in the subsequent bootstrap procedure.
Bootstrapping
To evaluate the significance of specific indirect effects, a bootstrap procedure was performed on 10,000 bootstrap samples. The 95% confidence intervals (CIs) for the identified indirect effect estimates were examined. If the 95% CI did not include the value of zero, it could be confirmed that the indirect effect was statistically significant at the p < .05 level (Shrout and Bolger 2002). Paths d and e (see Fig. 1) were constrained to zero in the following analyses in order to test the specific mediating effects of attitudes, subjective norms, and perceived behavioral control on the relationships between the nine biopsychosocial variables and help-seeking intentions. As indicated in Table 3, indirect effects from gender, evaluated need, anticipated benefits, anticipated risks, and self-stigma to intentions through attitudes were statistically significant. Subjective norms had a mediating effect on the associations between evaluated need, anticipated risks, and intentions. Additionally, adherence to Asian cultural values, social support, evaluated need, anticipated risks, self-stigma, and public stigma were indirectly and significantly related to intentions via perceived behavioral control.
Predictors of Actual Use of MHS
Logistic regression analysis was employed to investigate the role of help-seeking intentions, perceived behavioral control, predisposing, enabling, and need variables in the prediction of service usage, as it is inappropriate to include categorical variables (i.e., MHS utilization) in a structural model (Byrne 2010). Specifically, in order to explore changes in the contributions of help-seeking intentions and perceived behavioral control to the prediction of utilization when predisposing, enabling, and need variables were added into the model successively, all of the predictor variables were entered in four blocks.
Intentions and perceived behavioral control, which have been suggested as direct determinants of actual behavior (Ajzen 1985, 1991), were entered in Block 1. This model significantly predicted students’ use of MHS (χ2 (2) = 8.21, p = .017), with the two variables explaining 2.9% of variance in utilization (see Table 4). Seven predisposing variables were entered in Block 2. This model, with help-seeking intentions, perceived behavioral control, and predisposing variables, was also a significant fit of the data (χ2 (11) = 20.98, p = .034). However, adding predisposing variables to the model had no significant improvement in model fit (χ2 (9) = 12.77, p = .173). Importantly, help-seeking intention continued to significantly predict use. Subsequently, five enabling variables were included in Block 3. This model again significantly predicted usage (χ2 (17) = 32.94, p = .011), but there was also no significant improvement in model fit by adding enabling variables (χ2 (6) = 11.96, p = .063). Notably, help-seeking intention retained a significant and positive association with service use.
Finally, four need variables were entered in Block 4. The final model also significantly predicted MHS utilization (χ2 (21) = 75.10, p < .001). All of the predictors explained nearly 26% of variance in service use and the addition of need variables significantly improved the model fit (χ2 (4) = 42.15, p < .001). Help-seeking intention was no longer a significant predictor; instead, increased frequency of exposure to MHS-related information, lower level of self-rated mental health status, and higher level of perceived need were related to usage.
Qualitative Findings
Open-ended responses were translated by the first author. Themes related to the responses to each of the four open-ended questions were identified and coded in accordance with Braun and Clarke (2013). The five most frequently coded themes for each question are listed in Table 5. Severity of illness was most often described as the primary motivator for Chinese college students to seek professional support, whereas public stigma was the most frequently mentioned barrier. Based on responses concerning potential benefits of receiving MHS, it may be inferred that Chinese college students commonly understand mental health treatments as medical treatments for physical disorders. In terms of suggestions for future service delivery, publicizing information about available services and promoting psycho-education sessions were highly recommended.
Discussion
The aim of this study was to investigate help-seeking behavior among Mainland Chinese college students by integrating the TPB (Ajzen 1985) and Andersen’s (1995) Behavioral Model. The hypothesized model of help-seeking intentions exhibited a good fit to the data. Further examination of the indirect effects on intentions through attitudes, subjective norms, and perceived behavioral control provided partial support for the hypothesis that these three variables mediate the relationships between different biopsychosocial variables and help-seeking intentions. In addition, only five variables significantly predicted Chinese students’ service usage.
Consistent with previous research, the results indicated that gender, anticipated benefits, anticipated risks, self-stigma, and evaluated need significantly predicted attitudes, which in turn were positively related to help-seeking intentions (Ajzen and Sheikh 2013; Chang 2008; Chen et al. 2014; Choi and Miller 2014; Vogel et al. 2005; Wade et al. 2015; Yakunina and Weigold 2011; Yeh 2002). Notably, evaluated need was negatively associated with attitudes: students with a higher level of psychological distress tended to report less positive attitudes toward seeking professional support, consistent with previous studies among Chinese adolescents and Taiwanese students (Chang 2008; Chen et al. 2014). In Asian societies, individuals with mental illness are often negatively labelled and socially isolated. Receiving professional psychological support has been described as a contributor to this discrimination. Consequently, people with mental health issues may report negative attitudes toward accessing MHS (Hou and Zhang 2007; Kim et al. 2001; Kim and Omizo 2003; Sue and Morishima 1982).
Subjective norms were found to be a significant mediator of the relationship from evaluated need and anticipated risks to help-seeking intentions. Specifically, the model revealed that subjective norms were not only positively associated with intentions, but also positively related to attitudes and perceived behavioral control, consistent with previous research among Hong Kong and Macao Chinese people (Mak and Davis 2014; Mo and Mak 2009). It seems that significant others’ encouragement toward help-seeking not only impacts Chinese students’ intent to seek professional psychological help, but also shapes their attitudes toward and sense of control about using MHS. These findings demonstrate the importance of social expectations in encouraging Chinese students to use MHS. It is possible that, compared to individuals from other cultures, Chinese students are more likely to adhere to traditional values of conformity, deference, and respect for elders’ wishes. Therefore, they are more willing to seek professional support when significant others suggest it, despite maintaining negative attitudes to MHS (Kim et al. 2001; Kim and Omizo 2003; Mo and Mak 2009).
In relation to perceived behavioral control, the model identified that adherence to Asian values, social support, anticipated risks, self-stigma and public stigma significantly predicted this factor. Although perceived behavioral control did not contribute to students’ help-seeking intent, its mediating effects were identified through the bootstrapping procedure. One possible explanation is that in relation to Chinese students’ help-seeking for mental health purposes, external factors (e.g., family expectations) may be more influential than their own control. Hence, when perceived behavioral control was examined together with subjective norms, the latter may occupy a part of the former’s influence on help-seeking intentions (Mak and Davis 2014; Mo and Mak 2009). Ajzen and colleagues (1991; 2005) have, indeed, indicated that the weights of attitudes, subjective norms and perceived behavioral control in the prediction of intentions may vary across behaviors and populations.
For these Chinese students, evaluated need and self-stigma were negatively related to attitudes, but positively associated with help-seeking intentions. The positive relationship between evaluated need and intentions may reflect the need measures utilized in this study. The HSCL-21 and K10 both list symptoms of mental illness, when the measure of help-seeking intentions (i.e., WSC) lists specific problems that college students may encounter, hence the matching of symptoms (e.g., numbness or tingling in parts of your body) with problems (e.g., general anxiety) may increase the likelihood of identifying a positive association between evaluated need and help-seeking intentions. In addition, the positive relation between self-stigma and intentions may be due to the decline in self-esteem and/or self-confidence. Research has consistently shown that the internalization of stigma may result in reduced self-esteem and self-confidence (Chen et al. 2014; Corrigan 2004; Vogel et al. 2013b). Our qualitative findings indicated that being positive and being confident were two of the five major benefits that students attributed to MHS use; therefore, low self-esteem and self-confidence associated with self-stigma may directly motivate students to seek help.
Furthermore, help-seeking intentions, perceived behavioral control, frequency of exposure to MHS-related information, self-rated mental health status, and perceived need for help, demonstrated significant effects on service use. These results, together with the findings of the structural model, suggest that social-cognitive factors, more so than demographic characteristics, significantly explain Chinese college students’ mental health help-seeking. In particular, help-seeking intentions may contribute the most to the prediction and explanation of service use, given that intentions consistently predicted usage even after predisposing and enabling variables were entered into the model. Importantly, the current findings provided support for the TPB (Ajzen 1991, 2011; Ajzen and Fishbein 2005), which suggests that intention is the immediate determinant and significant predictor of behavior, and confirmed the efficacy of the TPB in explaining formal help-seeking behavior.
The present study identified some additional interesting results. Firstly, even though perceived need did not predict help-seeking intentions, it was significantly and positively related to service use. Moreover, in accordance with Western literature (Andrade et al. 2014; Eisenberg et al. 2012), perceived need displayed the strongest association with service use: students who reported perceived need for professional help were almost 5 times more likely to have used services than those who did not report a need. This may suggest that the impact of perceived need on use of MHS is direct, rather than operating through mediators. Previous research in China has also revealed that the recognition of need for professional help is an important facilitator to service use (Chen 2012; Chen and Zhu 2015). Similarly, a significant and negative effect of perceived behavioral control on service use was identified, although it was not related to intentions. This is consistent with an assumption of the TPB that perceived behavioral control can directly predict actual behaviors (Ajzen 1991, 2011). However, it should be noted that perceived behavioral control lost its influence on usage when predisposing, enabling, and need variables were entered. Future studies are needed to further investigate the interactions between these variables and perceived behavioral control.
Secondly, contrary to prior research (Chang 2008; Chin et al. 2015; Choi and Miller 2014; Kim and Omizo 2003; Liao et al. 2005), the current findings indicated that neither adherence to Asian values nor social support significantly impacted students’ help-seeking activities. One possible explanation is that Chinese college students’ lifestyle and awareness of mental health may have been influenced by Western values due to globalization and Internet development, which in turn may have impacted on their service use, independent of the extent of adhering to Asian cultural values. Previous research has found that Asian Americans who adhere to European cultural values are more willing to use MHS (Choi and Miller 2014).
Future research should investigate the predictive effect of adaptation to Western cultural values on Chinese students’ help-seeking behavior. Another explanation could be that the Asian cultural values scale utilized in this study was developed with Asian Americans and on the basis of shared Asian cultural values, thus, it may not include some specific cultural values held by Chinese people. Researchers should consider developing a specific measure of Chinese cultural values and examining its relationship with help-seeking.
Additionally, the non-significant findings for social support may reflect the loss of original social networks due to geographic isolation (Khawaja and Dempsey 2007; Yoon and Jepsen 2008). Indeed, 90% of our participants were living on campus, away from family and friends. Moreover, these non-significant findings, together with the identified significant effect of social expectations, suggest that rather than the quality of social support, it is family and friends’ expectations that influence Chinese students’ help-seeking. Future research on effective mental health interventions should incorporate the impact of social expectations.
Thirdly, evaluated need measured by using self-report psychometric screening scales did not predict students’ service utilization, whereas self-rated mental health status was significantly associated with use: students with a lower level of self-rated mental health status were more likely to have used MHS. These contradictory findings may be attributed to Chinese students’ misunderstanding of mental health issues and MHS. To illustrate, students might consider some physical impairments as symptoms of mental illness when rating their own mental health status, potentially exaggerating the therapeutic effect of psychological services on these impairments. Indeed, the majority of respondents in the current study provided vaguely worded statements about potential benefits of mental health treatments.
Finally, consistent with Plaistow et al. (2014), our study revealed that frequency of exposure to MHS-related information significantly predicted service use. This was also supported by our qualitative findings: students suggested that in order to promote help-seeking, education and mental health professionals should provide more information about mental health issues and services through campaigns (e.g., psycho-education seminars). Future research should expand this finding by exploring how different ways of providing information (through advertisements for the public or materials provided by counselors during treatment) influence students’ MHS use.
Limitations
The present findings must be interpreted in light of several limitations. Firstly, although the included measures are generally reliable and have been used often in previous studies across different populations, most were developed for North Americans, and some (i.e., ATSPPH-SF, SSOSH, and AVS) had lower reliability in the current study. Importantly, the validity of these measures was not compromised: they were carefully translated and back-translated by an accredited translation firm. Future research in Chinese populations would benefit from developing and employing culturally relevant scales. Moreover, the use of a single self-report item to assess MHS utilization in the preceding year excluded other potentially relevant information; for example, whether students attended alone or were accompanied by family. Previous reviews have observed that the effects of intentions and perceived behavioral control on behavior vary by how the behavior is measured – objectively or by self-report (Armitage and Conner 2001; Webb and Sheeran 2006). Therefore, future longitudinal and epidemiological research is suggested to document students’ use of MHS.
Secondly, the generalizability of the current findings may be limited due to participant recruitment procedures. Although the current sample was large and participants were recruited across majors and universities, the majority lived in Shandong Province and defined themselves as Han Chinese. Hence, it was not possible to examine within-group variability, although the literature indicates ethnic differences in Chinese students’ mental health status (Li et al. 2008). Future studies should consider expanding the scope of the research and replicating current findings with college students from other ethnic backgrounds and/or other geographical regions of China. In addition, future research could benefit from including additional variables (e.g., self-concealment; Cramer 1999), examining potential moderators (e.g., gender), and testing alternative models.
Thirdly, this study is not able to establish causal interpretations due to the cross-sectional design. Future research could use longitudinal data to explore and elucidate the causal relationships between identified biopsychosocial variables and Chinese college students’ use of MHS over time.
Implications
Despite the study’s limitations, its large size and reasonable gender ratio permitted complex multivariate analyses, enabling significant contributions to theory and practice. Theoretically, the results support the applicability of the TPB within Chinese populations, and indicate that researchers should consider adding pathways from subjective norms to attitudes and perceived behavioral control when investigating Chinese people’s help-seeking intentions. Moreover, the present findings also contributed to the limited knowledge regarding Chinese college students’ help-seeking behavior by integrating two influential theories in health psychology.
Practically, the study provides direction for education providers and mental health practitioners working with Chinese college students. Firstly, our findings suggest that community advertising and education would promote help-seeking. The resources of available MHS in Mainland China have substantially increased due to government initiatives and comprehensive mental health policies. For example, Chinese universities and schools are required to provide professional psychological support for students, with or without mental health issues (Ministry of Education of the People's Republic of China 2001). However, the current study indicates that many students are ill-informed about MHS and probably hold incorrect beliefs about disorders and treatments: almost half of our participants were unaware of available MHS. Therefore, education providers and mental health professionals should not only provide basic service information (e.g., location), but also work on correcting inaccurate beliefs. For this purpose, our participants recommended on-campus psycho-educational seminars and workshops that could explain mental disorders and symptoms, the types and processes of treatments, and the consequences of delayed diagnosis and treatment.
Furthermore, considering the significant influence of social expectations on Chinese college students’ help-seeking, psycho-educational campaigns should be also disseminated to the community, via mass media, to inform students’ families and friends about mental health and promote positive attitudes toward using professional services. Thus, stigma associated with mental illness and seeking professional psychological help could be reduced, in turn promoting help-seeking.
Mental health professionals may need to advance beyond face-to-face modes of service delivery, and use the Internet to provide help for students with mental health issues. Doing so can avoid stigma concerns about publicly accessing MHS, and enhance the likelihood of regular contacts with students, as recommended by our participants. Practitioners should also be sensitive to cultural differences. Rather than preferring Western theories, they could consider mindfulness and other approaches derived from Eastern cultures that may be more appropriate to Chinese populations (Tang et al. 2012). Family therapy approaches (e.g., structural family therapy) are also recommended because our findings highlighted the importance of family interaction in this context. Researchers have, indeed, observed that family therapy is effective for Mainland Chinese clients (e.g., Sim and Hu 2009; Xiong et al. 1994; Yang and Pearson 2002).
Conclusion
The current integrated model explained Chinese college students’ help-seeking behavior and indicated that social-cognitive factors are important predictors of students’ help-seeking intentions and their actual usage. Longitudinal research is recommended to further clarify these relationships.
References
Ajzen, I. (1985). From intention to action: a theory of planned behavior. In J. Kuhl & J. Beckmann (Eds.), Action-control: from cognition to behavior (pp. 11–39). New York: Springer.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179–211. doi:10.1016/0749-5978(91)90020-T.
Ajzen, I. (2011). The theory of planned behaviour: reactions and reflections. Psychology & Health, 26, 1113–1127. doi:10.1080/08870446.2011.613995.
Ajzen, I., & Fishbein, M. (2005). The influence of attitudes on behavior. In D. Albarracin, B. T. Johnson, & M. P. Zanna (Eds.), The handbook of attitudes (pp. 173–221). Mahwah: Erlbaum.
Ajzen, I., & Madden, T. J. (1986). Prediction of goal-directed behavior: attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology, 22, 453–474. doi:10.1016/0022-1031(86)90045-4.
Ajzen, I., & Sheikh, S. (2013). Action versus inaction: anticipated affect in the theory of planned behavior. Journal of Applied Social Psychology, 43, 155–162. doi:10.1111/j.1559-1816.2012.00989.x.
Andersen, R. M. (1995). Revisiting the behavioral model and access to medical care: does it matter? Journal of Health and Social Behavior, 36, 1–10. doi:10.2307/2137284.
Andersen, R. M., & Newman, J. F. (1973). Societal and individual determinants of medical care utilization in the United States. The Milbank Memorial Fund Quarterly. Health and Society, 51, 95–124. doi:10.2307/3349613.
Anderson, J. C., & Gerbing, D. W. (1988). Structural equation modeling in practice: a review and recommended two-step approach. Psychological Bulletin, 103, 411–423.
Andrade, L. H., Alonso, J., Mneimneh, Z., Wells, J. E., Al-Hamzawi, A., Borges, G., et al. (2014). Barriers to mental health treatment: results from the WHO world mental health surveys. Psychological Medicine, 44, 1303–1317. doi:10.1017/s0033291713001943.
Armitage, C. J., & Conner, M. (2001). Efficacy of the theory of planned behaviour: a meta-analytic review. British Journal of Social Psychology, 40, 471–499. doi:10.1348/014466601164939.
Bandalos, D. L. (2002). The effects of item parceling on goodness-of-fit and parameter estimate bias in structural equation modeling. Structural Equation Modeling: A Multidisciplinary Journal, 9, 78–102. doi:10.1207/S15328007SEM0901_5.
Boey, K. W. (1999). Help-seeking preference of college students in urban China after the implementation of the "open-door" policy. International Journal of Social Psychiatry, 45, 104–116. doi:10.1177/002076409904500203.
Braun, V., & Clarke, V. (2013). Successful qualitative research : a practical guide for beginnners. Los Angeles: SAGE Publications Ltd..
Byrne, B. M. (2010). Structural equation modeling with Amos: basic concepts, applications and programming (2nd ed.). Mahwah: Lawrence Erlbaum Associates.
Cash, T. F., Begley, P. J., McCown, D. A., & Weise, B. C. (1975). When counselors are heard but not seen: initial impact of physical attractiveness. Journal of Counseling Psychology, 22, 273–279. doi:10.1037/h0076730.
Cepeda-Benito, A., & Short, P. (1998). Self-concealment, avoidance of psychological services, and perceived likelihood of seeking professional help. Journal of Counseling Psychology, 45, 58–64. doi:10.1037/0022-0167.45.1.58.
Chang, H. (2008). Help-seeking for stressful events among Chinese college students in Taiwan: roles of gender, prior history of counseling, and help-seeking attitudes. Journal of College Student Development, 49, 41–51. doi:10.1353/csd.2008.0003.
Chen, J. (2012). Seeking help for psychological distress in urban China. Journal of Community Psychology, 40, 319–341. doi:10.1002/jcop.20513.
Chen, J., & Zhu, S. (2015). Online information searches and help seeking for mental health problems in urban China. Administration and Policy in Mental Health and Mental Health Services Research, 43, 535–545. doi:10.1007/s10488-015-0657-6.
Chen, H., Fang, X., Liu, C., Hu, W., Lan, J., & Deng, L. (2014). Associations among the number of mental health problems, stigma, and seeking help from psychological services: a path analysis model among Chinese adolescents. Children and Youth Services Review, 44, 356–362. doi:10.1016/j.childyouth.2014.07.003.
Cheng, H.-L., Kwan, K.-L. K., & Sevig, T. (2013). Racial and ethnic minority college students' stigma associated with seeking psychological help: examining psychocultural correlates. Journal of Counseling Psychology, 60, 98–111. doi:10.1037/a0031169.
Chin, W. Y., Chan, K. T. Y., Lam, C. L. K., Lam, T. P., & Wan, E. Y. F. (2015). Help-seeking intentions and subsequent 12-month mental health service use in Chinese primary care patients with depressive symptoms. BMJ Open, 5, 1–10. doi:10.1136/bmjopen-2014-006730.
Choi, N. Y., & Miller, M. J. (2014). AAPI college students' willingness to seek counseling: the role of culture, stigma and attitudes. Journal of Counseling Psychology, 61, 340–351. doi:10.1037/cou0000027.
Clement, S., Schauman, O., Graham, T., Maggioni, F., Evans-Lacko, S., Bezborodovs, N., et al. (2015). What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychological Medicine, 45, 11–27. doi:10.1017/S0033291714000129.
Corrigan, P. W. (2004). How stigma interferes with mental health care. American Psychologist, 59, 614–625. doi:10.1037/0003-066x.59.7.614.
Cramer, K. M. (1999). Psychological antecedents to help-seeking behavior: a reanalysis using path modeling structures. Journal of Counseling Psychology, 46, 381–387. doi:10.1037/0022-0167.46.3.381.
Cutrona, C. E., & Russell, D. W. (1987). The provisions of social relationships and adaptation to stress. Advances in Personal Relationships, 1, 37–67.
Deane, F. P., Leathem, J., & Spicer, J. (1992). Clinical norms, reliability and validity for the Hopkins symptom checklist-21. Australian Journal of Psychology, 44, 21–25. doi:10.1080/00049539208260158.
Eisenberg, D., Hunt, J., & Speer, N. (2012). Help seeking for mental health on college campuses: review of evidence and next steps for research and practice. Harvard Review of Psychiatry, 20, 222–232. doi:10.3109/10673229.2012.712839.
Fang, K., Pieterse, A., Friedlander, M., & Cao, J. (2011). Assessing the psychometric properties of the attitudes toward seeking professional psychological help scale-short form in mainland China. International Journal for the Advancement of Counselling, 33, 309–321. doi:10.1007/s10447-011-9137-1.
Field, A. (2009). Discovering statistics using SPSS. London: SAGE Publications.
Fischer, E. H., & Farina, A. (1995). Attitudes toward seeking professional psychological help: a shortened form and considerations for research. Journal of College Student Development, 36, 368–373.
Fischer, E. H., & Turner, J. L. (1970). Orientations to seeking professional help: development and research utility of an attitude scale. Journal of Consulting and Clinical Psychology, 35, 79–90. doi:10.1037/h0029636.
Gao, J., Tang, S., Tolhurst, R., & Rao, K. (2001). Changing access to health services in urban China: implications for equity. Health Policy and Planning, 16, 302–312. doi:10.1093/heapol/16.3.302.
Gim, R. H., Atkinson, D. R., & Whiteley, S. (1990). Asian-American acculturation, severity of concerns, and willingness to see a counselor. Journal of Counseling Psychology, 37, 281–285. doi:10.1037/0022-0167.37.3.281.
Godin, G., & Kok, G. (1996). The theory of planned behavior: a review of its applications to health-related behaviors. American Journal of Health Promotion, 11, 87–98. doi:10.4278/0890-1171-11.2.87.
Goh, M., Xie, B., Herting Wahl, K., Zhong, G., Lian, F., & Romano, J. (2007). Chinese students’ attitudes toward seeking professional psychological help. International Journal for the Advancement of Counselling, 29, 187–202. doi:10.1007/s10447-007-9038-5.
Green, D. E., Walkey, F. H., McCormick, I. A., & Taylor, A. J. W. (1988). Development and evaluation of a 21-item version of the Hopkins symptom checklist with New Zealand and United States respondents. Australian Journal of Psychology, 40, 61–70. doi:10.1080/00049538808259070.
Guo, Q., Huang, Y. Q., Liu, Z. R., & Wang, H. (2013). Psychological symptoms and associated risk factors in Chinese freshmen: a three-year follow-up study. Chinese Medical Journal, 126, 3499–3504. doi:10.3760/cma.j.issn.0366-6999.20131201.
Hamid, P. D., Simmonds, J. G., & Bowles, T. V. (2009). Asian Australian acculturation and attitudes toward seeking professional psychological help. Australian Journal of Psychology, 61, 69–76. doi:10.1080/00049530701867839.
Hammer, J. H., & Vogel, D. L. (2013). Assessing the utility of the willingness/prototype model in predicting help-seeking decisions. Journal of Counseling Psychology, 60, 83–97. doi:10.1037/a0030449.
Hao, Z., & Liang, B. (2007). Revision of the questionnaire of attitudes toward seeking professional psychological help. Chinese Journal of Clinical Psychology, 15, 1–4.
Holmbeck, G. N. (1997). Toward terminological, conceptual, and statistical clarity in the study of mediators and moderators: examples from the child-clinical and pediatric psychology literature. Journal of Consulting and Clinical Psychology, 65, 599–610. doi:10.1037/0022-006X.65.4.599.
Hou, Z.-J., & Zhang, N. (2007). Counseling psychology in China. Applied Psychology: An International Review, 56, 33–50. doi:10.1111/j.1464-0597.2007.00274.x.
Hoyle, R. (1995). The structural equation modeling approach: basic concepts and fundamental issues. In R. Hoyle (Ed.), Structural equation modeling: concepts, issues and applications (pp. 1–15). Newbury Park: SAGE.
Hu, L. t., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6, 1–55. doi:10.1080/10705519909540118.
Huang, C., Sousa, V. D., Tsai, C., & Hwang, M. (2008). Social support and adaptation of Taiwanese adults with mental illness. Journal of Clinical Nursing, 17, 1795–1802. doi:10.1111/j.1365-2702.2008.02310.x.
IBM Corp. (2012). IBM SPSS statistics for windows (version 21). Armonk: IBM Corp.
Kahn, J. H., & Williams, M. N. (2003). The impact of prior counseling on predictors of college counseling center use. Journal of College Counseling, 6, 144–154. doi:10.1002/j.2161-1882.2003.tb00235.x.
Kaplan, D. (2009). Structural equation modeling: foundations and extensions (2nd ed.). Los Angeles: Sage Publications.
Kessler, R. C., Andrews, G., Colpe, L. J., Hiripi, E., Mroczek, D. K., Normand, S. L., et al. (2002). Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine, 32, 959–976. doi:10.1017/S0033291702006074.
Kessler, R. C., Barker, P. R., Colpe, L. J., Epstein, J. F., Gfroerer, J. C., Hiripi, E., et al. (2003). Screening for serious mental illness in the general population. Archives of General Psychiatry, 60, 184–189. doi:10.1001/archpsyc.60.2.184.
Khawaja, N. G., & Dempsey, J. (2007). Psychological distress in international university students: an Australian study. Australian Journal of Guidance and Counselling, 17, 13–27. doi:10.1375/ajgc.17.1.13.
Kim, B. S. K., & Omizo, M. M. (2003). Asian cultural values, attitudes toward seeking professional psychological help, and willingness to see a counselor. The Counseling Psychologist, 31, 343–361. doi:10.1177/0011000003031003008.
Kim, P. Y., & Park, I. J. (2009). Testing a multiple mediation model of Asian American college students' willingness to see a counselor. Cultural Diversity and Ethnic Minority Psychology, 15, 295–302. doi:10.1037/a0014396.
Kim, B. S. K., Atkinson, D. R., & Yang, P. H. (1999). The Asian values scale: development, factor analysis, validation, and reliability. Journal of Counseling Psychology, 46, 342–352. doi:10.1037/0022-0167.46.3.342.
Kim, B. S. K., Atkinson, D. R., & Umemoto, D. (2001). Asian cultural values and the counseling process: current knowledge and directions for future research. The Counseling Psychologist, 29, 570–603. doi:10.1177/0011000001294006.
Kline, R. B. (2005). Principles and practice of structural equation modeling (2nd ed.). New York: Guilford.
Leech, N. L. (2007). Cramer's model of willingness to seek counseling: a structural equation model for counseling students. Journal of Psychology: Interdisciplinary and Applied, 141, 435–445. doi:10.3200/jrlp.141.4.435-448.
Li, H., Li, W., Liu, Q., Zhao, A., Prevatt, F., & Yang, J. (2008). Variables predicting the mental health status of Chinese college students. Asian Journal of Psychiatry, 1, 37–41. doi:10.1016/j.ajp.2008.09.003.
Li, N., Du, W., Chen, G., Song, X., & Zheng, X. (2013). Mental health service use among Chinese adults with mental disabilities: a national survey. Psychiatric Services, 64, 638–644. doi:10.1176/appi.ps.001232012.
Li, K., Sun, X., Zhang, Y., Shi, G., & Kolstad, A. (2014a). Mental health care in China: review on the delivery and policy issues in 1949–2009 and the outlook for the next decade. Acta Neuropsychiatrica, 26, 134–145. doi:10.1017/neu.2013.40.
Li, W., Dorstyn, D. S., & Denson, L. A. (2014b). Psychosocial correlates of college students’ help-seeking intention: a meta-analysis. Professional Psychology: Research and Practice, 45, 163–170. doi:10.1037/a0037118.
Liao, H.-Y., Rounds, J., & Klein, A. G. (2005). A test of Cramer's (1999) help-seeking model and acculturation effects with Asian and Asian American college students. Journal of Counseling Psychology, 52, 400–411. doi:10.1037/0022-0167.52.3.400.
Little, T. D., Cunningham, W. A., Shahar, G., & Widaman, K. F. (2002). To parcel or not to parcel: exploring the question, weighing the merits. Structural Equation Modeling: A Multidisciplinary Journal, 9, 151–173. doi:10.1207/S15328007SEM0902_1.
Liu, T. Q., Chee, N., Ma, H., Castle, D., Hao, W., & Li, L. J. (2008). Comparing models of mental health service systems between Australia and China: implications for the future development of Chinese mental health service. Chinese Medical Journal, 121, 1331–1338.
Mak, H., & Davis, J. M. (2014). The application of the theory of planned behavior to help-seeking intention in a Chinese society. Social Psychiatry and Psychiatric Epidemiology, 49, 1501–1515. doi:10.1007/s00127-013-0792-x.
Martens, M. P. (2005). The use of structural equation modeling in counseling psychology research. The Counseling Psychologist, 33, 269–298. doi:10.1177/0011000004272260.
Ministry of Education of the People's Republic of China. (2001). Opinions on strengthening the university students' psychological health education. Beijing: Ministry of Education of the People's Republic of China Retrieved from http://www.gov.cn/gongbao/content/2002/content_61930.htm.
Mo, P. K. H., & Mak, W. W. S. (2009). Help-seeking for mental health problems among Chinese: the application and extension of the theory of planned behavior. Social Psychiatry and Psychiatric Epidemiology, 44, 675–684. doi:10.1007/s00127-008-0484-0.
Nam, S. K., Choi, S. I., Lee, J. H., Lee, M. K., Kim, A. R., & Lee, S. M. (2013). Psychological factors in college students' attitudes toward seeking professional psychological help: a meta-analysis. Professional Psychology:Research and Practice, 44, 37–45. doi:10.1037/a0029562.
Park, L., Xiao, Z., Worth, J., & Park, J. M. (2005). Mental health care in China: recent changes and future challenges. Harvard Health Policy Review, 6, 35–45.
Phillips, M. R., Zhang, J., Shi, Q., Song, Z., Ding, Z., Pang, S., et al. (2009). Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001–05: an epidemiological survey. The Lancet, 373, 2041–2053. doi:10.1016/S0140-6736(09)60660-7.
Plaistow, J., Masson, K., Koch, D., Wilson, J., Stark, R. M., Jones, P. B., & Lennox, B. R. (2014). Young people's views of UK mental health services. Early Intervention in Psychiatry, 8, 12–23. doi:10.1111/eip.12060.
Robertson, J. M., & Fitzgerald, L. F. (1992). Overcoming the masculine mystique: preferences for alternative forms of assistance among men who avoid counseling. Journal of Counseling Psychology, 39, 240–246. doi:10.1037/0022-0167.39.2.240.
Russell, D. W., Kahn, J. H., Spoth, R., & Altmaier, E. M. (1998). Analyzing data from experimental studies: a latent variable structural equation modeling approach. Journal of Counseling Psychology, 45, 18–29. doi:10.1037/0022-0167.45.1.18.
Shaffer, P. A., Vogel, D. L., & Wei, M. (2006). The mediating roles of anticipated riks, anticipated benefits, and attitudes on the decision to seek professional help: an attachment perspective. Journal of Counseling Psychology, 53, 442–452. doi:10.1037/0022-0167.53.4.442.
Shea, M., & Yeh, C. J. (2008). Asian American students' cultural values, stigma, and relational self-construal: Correlates of attitudes toward professional help seeking. Journal of Mental Health Counseling, 30, 157–172. doi:10.17744/mehc.30.2.g662g5l2r1352198.
Shen, Y.-C., Zhang, M.-Y., Huang, Y.-Q., He, Y.-L., Liu, Z.-R., Cheng, H., et al. (2006). Twelve-month prevalence, severity, and unmet need for treatment of mental disorders in metropolitan China. Psychological Medicine, 36, 257–267. doi:10.1017/S0033291705006367.
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychological Methods, 7, 422–445. doi:10.1037//1082-989X.7.4.422.
Sim, T., & Hu, C. (2009). Family therapy in the Forbidden City: a review of Chinese journals from 1978 to 2006. Family Process, 48, 559–583. doi:10.1111/j.1545-5300.2009.01302.x.
Sue, S., & Morishima, J. K. (1982). The mental health of Asian Americans. San Francisco: Jossey-Bass.
Tang, T. T. T., Reilly, J., & Dickson, J. M. (2012). Attitudes toward seeking professional psychological help among Chinese students at a UK university. Counselling and Psychotherapy Research, 12, 287–293. doi:10.1080/14733145.2012.659747.
Tucker, J. R., Hammer, J. H., Vogel, D. L., Bitman, R. L., Wade, N. G., & Maier, E. J. (2013). Disentangling self-stigma: Are mental illness and help-seeking self-stigmas different? Journal of Counseling Psychology, 60, 1–13. doi:10.1037/a0033555.
Vogel, D. L., & Wester, S. R. (2003). To seek help or not to seek help: the risks of self-disclosure. Journal of Counseling Psychology, 50, 351–361. doi:10.1037/0022-0167.50.3.351.
Vogel, D. L., Wester, S. R., Wei, M., & Boysen, G. A. (2005). The role of outcome expectations and attitudes on decisions to seek professional help. Journal of Counseling Psychology, 52, 459–470. doi:10.1037/0022-0167.52.4.459.
Vogel, D. L., Wade, N. G., & Haake, S. (2006). Measuring the self-stigma associated with seeking psychological help. Journal of Counseling Psychology, 53, 325–337. doi:10.1037/0022-0167.53.3.325.
Vogel, D. L., Wester, S. R., & Larson, L. M. (2007a). Avoidance of counseling: psychological factors that inhibit seeking help. Journal of Counseling & Development, 85, 410–422. doi:10.1002/j.1556-6678.2007.tb00609.x.
Vogel, D. L., Wade, N. G., & Hackler, A. H. (2007b). Perceived public stigma and the willingness to seek counseling: the mediating roles of self-stigma and attitudes toward counseling. Journal of Counseling Psychology, 54, 40–50. doi:10.1037/0022-0167.54.1.40.
Vogel, D. L., Gentile, D. A., & Kaplan, S. A. (2008a). The influence of television on willingness to seek therapy. Journal of Clinical Psychology, 64, 276–295. doi:10.1002/jclp.20446.
Vogel, D. L., Wade, N. G., & Hackler, A. H. (2008b). Emotional expression and the decision to seek therapy: the mediating roles of the anticipated benefits and risks. Journal of Social and Clinical Psychology, 27, 254–278. doi:10.1080/00207590600878665.
Vogel, D. L., Wade, N. G., & Ascheman, P. L. (2009). Measuring perceptions of stigmatization by others for seeking psychological help: reliability and validity of a new stigma scale with college students. Journal of Counseling Psychology, 56, 301–308. doi:10.1037/a0014903.
Vogel, D. L., Armstrong, P. I., Tsai, P.-C., Wade, N. G., Hammer, J. H., Efstathiou, G., et al. (2013a). Cross-cultural validity of the self-stigma of seeking help (SSOSH) scale: examination across six nations. Journal of Counseling Psychology, 60, 303–310. doi:10.1037/a0032055.
Vogel, D. L., Bitman, R. L., Hammer, J. H., & Wade, N. G. (2013b). Is stigma internalized? The longitudinal impact of public stigma on self-stigma. Journal of Counseling Psychology, 60, 311–316. doi:10.1037/a0031889.
Wade, N. G., Vogel, D. L., Armistead-Jehle, P., Meit, S. S., Heath, P. J., & Strass, H. A. (2015). Modeling stigma, help-seeking attitudes, and intentions to seek behavioral healthcare in a clinical military sample. Psychiatric Rehabilitation Journal, 38, 135–141. doi:10.1037/prj0000131.
Wang, P. S., Aguilar-Gaxiola, S., Alonso, J., Angermeyer, M. C., Borges, G., Bromet, E. J., et al. (2007). Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. The Lancet, 370, 841–850. doi:10.1016/S0140-6736(07)61414-7.
Wang, X., Huang, X., Jackson, T., & Chen, R. (2012). Components of implicit stigma against mental illness among Chinese students. PloS One, 7, 1–6. doi:10.1371/journal.pone.0046016.
Webb, T. L., & Sheeran, P. (2006). Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychological Bulletin, 132, 249–268. doi:10.1037/0033-2909.132.2.249.
Wen, M., Fan, J., Jin, L., & Wang, G. (2010). Neighborhood effects on health among migrants and natives in shanghai, China. Health & Place, 16, 452–460. doi:10.1016/j.healthplace.2009.12.001.
Wilson, C. J., Deane, F., Marshall, K., & Dalley, A. (2008). Reducing adolescents’ perceived barriers to treatment and increasing help-seeking intentions: effects of classroom presentations by general practitioners. Journal of Youth and Adolescence, 37, 1257–1269. doi:10.1007/s10964-007-9225-z.
Wong, D. F. K., & Li, J. C. M. (2014). Cultural influence on shanghai Chinese people's help-seeking for mental health problems: implications for social work practice. British Journal of Social Work, 44, 868–885. doi:10.1093/bjsw/bcs180.
Wu, C. Y., Liu, S. I., Chang, S. S., & Sun, F. J. (2014). Surveys of medical seeking preference, mental health literacy, and attitudes toward mental illness in Taiwan, 1990-2000. Journal of the Formosan Medical Association, 113, 33–41. doi:10.1016/j.jfma.2013.03.004.
Xie, D., & Leong, F. T. L. (2008). A cross-cultural study of anxiety among Chinese and Caucasian American university students. Journal of Multicultural Counseling and Development, 36, 52–63. doi:10.1002/j.2161-1912.2008.tb00069.x.
Xiong, W., Phillips, M. R., Hu, X., Wang, R., Dai, Q., Kleinman, J., & Kleinman, A. (1994). Family-based intervention for schizophrenic patients in China: a randomised controlled trial. The British Journal of Psychiatry, 165, 239–247. doi:10.1192/bjp.165.2.239.
Yakunina, E. S., & Weigold, I. K. (2011). Asian international students' intentions to seek counseling: integrating cognitive and cultural predictors. Asian American Journal of Psychology, 2, 219–224. doi:10.1037/a0024821.
Yang, L. H., & Pearson, V. J. (2002). Understanding families in their own context: schizophrenia and structural family therapy in Beijing. Journal of Family Therapy, 24, 233–257. doi:10.1111/1467-6427.00214.
Yeh, C. J. (2002). Taiwanese students' gender, age, interdependent and indenpendent self-construal, and collective self-esteem as predictors of professional psychological help-seeking attitudes. Cultural Diversity and Ethnic Minority Psychology, 8, 19–29. doi:10.1037//1099-9809.8.1.19.
Yoon, E., & Jepsen, D. (2008). Expectations of and attitudes toward counseling: a comparison of Asian international and U.S. graduate students. International Journal for the Advancement of Counselling, 30, 116–127. doi:10.1007/s10447-008-9050-4.
Zhou, C., Chu, J., Wang, T., Peng, Q., He, J., Zheng, W., et al. (2008). Reliability and validity of 10-item Kessler scale (K10) Chinese version in evaluation of mental health status of Chinese population. Chinese Journal of Clinical Psychology, 16, 627–629.
Zivin, K., Eisenberg, D., Gollust, S. E., & Golberstein, E. (2009). Persistence of mental health problems and needs in a college student population. Journal of Affective Disorders, 117, 180–185. doi:10.1016/j.jad.2009.01.001.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interests
The authors report no conflicts of interests.
Rights and permissions
About this article

Cite this article
Li, W., Denson, L.A. & Dorstyn, D.S. Help-Seeking Intentions and Behaviors among Mainland Chinese College Students: Integrating the Theory of Planned Behavior and Behavioral Model of Health Services Use. Int J Adv Counselling 39, 125–148 (2017). https://doi.org/10.1007/s10447-017-9287-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10447-017-9287-x