
Abstract
Compression therapy with stockings or bandages is the most common treatment for venous or lymphatic disorders. The objective of this study was to investigate the influence of bandage mechanical properties, application technique and subject morphology on the interface pressure, which is the key of this treatment. Bandage stretch and interface pressure measurements (between the bandage and the leg) were performed on 30 healthy subjects (15 men and 15 women) at two different heights on the lower leg and in two positions (supine and standing). Two bandages were applied with two application techniques by a single operator. The statistical analysis of the results revealed: no significant difference in pressure between men and women, except for the pressure variation between supine and standing positions; a very strong correlation between pressure and bandage mechanical properties (p < 0.00001) and between pressure and bandage overlapping (p < 0.00001); a significant pressure increase from supine to standing positions (p < 0.0001). Also, it showed that pressure tended to decrease when leg circumference increased. Overall, pressure applied by elastic compression bandages varies with subject morphology, bandage mechanical properties and application technique. A better knowledge of the impact of these parameters on the applied pressure may lead to a more effective treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Compression bandage is a common treatment for venous or lymphatic pathologies such as venous ulcers or lymphedema. In such diseases, bandages are preferred in the first step of the treatment by compression, instead of stockings. Indeed, during the first days of the treatment, the patients’ leg shape changes a lot and the same compression bandage can be applied on the leg with different geometries, whereas a new stocking size would be needed to accommodate these changes. Once the leg shape is stable, the treatment by compression is usually performed with socks or stockings. Bandages are also used when the patient’s pathology prevents the use of any other treatment (for example after a knee arthroplasty). Moreover, it is easier for a caregiver to apply bandages than stockings on patients’ legs, especially with patients with impaired mobility. Consequently, compression bandage and stockings are complementary.
The bandage, tight on the limb, applies a pressure on the external surface of the limb which is then transmitted to the internal tissues and to the veins.23,27 Numerous studies have proven the effect of compression therapy on venous and lymphatic system,1,19,31 whether compression is performed with bandages or stockings.5
The efficacy of the treatment mainly depends on the level of pressure which is applied on the limb.14,24 This level of pressure depends on several parameters such as:
-
The bandage mechanical properties
-
The bandage components (padding layer, cohesive bandage,…)
-
The bandage stretch
-
The local curvature of the limb on which the bandage is applied
-
The application technique (spiral or figure of eight)
-
Other parameters such as friction between the different layers, mechanical properties of the limb soft tissues,…
Better understanding how these parameters impact the level of applied pressure would lead to an improved treatment with compression bandage.
A well-known theoretical relationship between the tension, T, of the bandage (force needed to stretch the bandage, which is given by the bandage mechanical properties and the applied stretch), the local curvature, r c, of the limb and the locally applied pressure, P, is given by the Laplace’s Law:
However, it has been shown that this law is not sufficient to explain the pressure distribution over a limb,2,28 hence the need for an experimental investigation of the pressure applied by compression bandage on the lower leg.
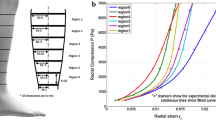
Several measurements of the pressure applied by bandages were carried out, with various types of bandages, at different measurement points and on a wide range of subjects in different body positions.7,8,17 In order to standardize the way to perform pressure measurements, recommendations have been published to proceed to interface pressure measurements.24 Measurement points have been identified on the lower leg24 such as (Fig. 1):
-
Measurement point B1: corresponding to the height where the Achilles’ tendon turns into the gastrocnemius muscle.
-
Measurement point C: corresponding to the height where the calf circumference is the largest.

Location of measurement points B1 (where the Achilles’ tendon turns into the gastrocnemius muscle) and C (where the calf circumference is the largest).
The pressure sensors used for the measurements should meet some requirements: for example to be thin and flexible.24 Different types of sensors exist but some have proven to be more reliable than others22 (Kikuhime® and Picopress® for example).
Most of the measurement campaigns which were performed on men and women did not take the gender difference into account.16,17 However the leg morphology has an influence on the applied pressure. Indeed, the leg morphology varies from a subject to another and maybe even more especially from a female subject to a male subject.12 Other groups investigated the impact of the application technique on the interface pressure6 and they also measured the stretch of the applied bandage. However, as the aim of this previous study was to compare the pressure applied by different application techniques, it was carried out for a single bandage type. Other studies were focused on the influence of bandage mechanical properties and position (supine, standing, sitting) on the interface pressure,3,8,11,26 but as far as we know, none of them measured the stretch of the applied bandage, though it is one of the main parameters which controls the interface pressure.
This shows the need of performing other pressure measurements in order to simultaneously evaluate the influence of all following parameters on the interface pressure: bandage mechanical properties, application technique, subjects’ gender and morphology and position (supine or standing).
Within this context, the objective of the present study is to perform a complete campaign including bandage stretch and pressure measurements in order to test the following hypotheses:
-
The applied pressure is proportional to the bandage elastic modulus (or the force needed to stretch the bandage)
-
The applied pressure is proportional to the bandage overlapping (50 or 66% overlapping means that respectively 2 or 3 bandage layers cover the leg)
-
The interface pressure significantly decreases when the subjects’ leg circumference increases.
Moreover, these measurements result to a quantitative evaluation of the pressure differences among female and male subjects and of the pressure increase between the supine and the standing positions.
Methods
Briefly, stretch and pressure measurements were performed on healthy male and female subjects in order to estimate the gender influence. Subjects were chosen in order to have a wide range of morphologies. Two different elastic bandages, with different mechanical properties, were applied on the subject’s leg with two application techniques with the aim of evaluating the influence of mechanical properties, application technique and position (supine or standing) on the interface pressure.
Bandages
Two commercially available elastic bandages, which differ in their mechanical properties, were applied on the subjects’ leg by the same experienced operator: the Biflex® 16 (B16) and the Biflex® 17 (B17) (Thuasne, Levallois-Perret, France) which is stiffer (Table 1). Bandage elastic modulus (K), in N/mm, is defined as follows:
where L is the length of the stretched bandage and L 0 its initial length (Fig. 2). Both bandages were 10 cm wide. They were applied on the leg with a target stretch of 1.3, in accordance with the manufacturer’s recommendations and visual calibration marker (Fig. 2). This visual calibration marker is a rectangle which turns into a square when the bandage stretch is equal to 1.3. It gives a visual indication to the bandager that the stretch is in accordance with the manufacturer’s recommendations. The stretch is defined as the ratio between the length of the stretched bandage and its initial length (stretch = L/L 0). Bandage can be applied in the form of a spiral with a 50 or a 66% overlap, which means that at each turn, the bandage layer on top covers the bandage layer below respectively by 50 or 66% (Figs. 2 and 3). For a 50 or 66% overlapping technique, the leg is covered by respectively 2 or 3 bandage layers. The value of the overlap is usually prescribed by medical doctors. Lines were drawn on the bandage to help the bandager to apply the bandage with the correct overlap: one at 50% and one at 33% of the bandage width, for respectively a 50 and a 66% overlapping technique (Fig. 2).

Bandage stretch and application technique in the form of a spiral; A visual marker (a rectangle which turns into a square when the bandage stretch is about 1.3) helps to apply the bandage with the correct stretch; lines are drawn to help to apply the bandage with the correct overlap.

Bandage applied in the form of a spiral with a 50% (a) or 66% (b) overlapping technique and locations of the sensors (c).
Pressure Sensors
The interface pressure was measured with pneumatic pressure sensors Picopress® (MicroLab Elettronica, Ponte S. Nicolo, Italy). This pressure sensor is a convenient device which was used in several previous pressure measurements studies.7,13,18
As a preliminary study, the accuracy, the linearity and the hysteresis of the sensors were tested. To achieve this, the sensor was placed at the bottom of a water column. First, the column was filled with water and a measure was taken every 10 mmHg (13.6 cmH2O) from 0 to 147 mmHg (199.9 cmH2O). Then the column was emptied and a measure was taken every 10 mmHg. This allowed characterizing the hysteresis of the sensor, which is given by the following equation:
where \(y_{ + } \left( {x_{i} } \right)\) and \(y_{ - } \left( {x_{i} } \right)\) are the measured pressure value for a theoretical applied pressure equal to \(x_{i}\), respectively during the loading and the unloading phases. The second test consisted in applying 20 different pressure values, which were randomly determined and allowed characterizing the sensor linearity. The coefficient of determination R 2 was used as the indicator of the linear dependence between the theoretical and the measured pressure. The closer to 1 the coefficient R 2 was, the more linear the sensor was.
These tests were performed for the Picopress® device and the two sensors which were used in the study (respectively at measurement points B1 and C).
The tests showed that R 2 was almost equal to 1 for both sensors (R 2 = 0.9999) and that the hysteresis was slightly higher for the sensor located at measurement point B1 (1.0%) than for the other sensor located at measurement point C (0.0%).
The tests performed on the sensors showed that these sensors were very reliable and, hence, suitable for the present work, which was in accordance with the tests conducted by Partsch et al.22
Experimental Protocol
Subject Selection
Pressure measurements were carried out on 30 healthy subjects, 15 women and 15 men, following informed consent (Table 2). This protocol was approved by the local ethics committee.
The subjects’ selection was made with regards to their circumference at measurement point B1 (Fig. 1) in order to be equally distributed in 3 groups of circumference at B1 height.
For this, a list of 205 women and one of 147 men were built and alphabetically ordered. Six groups (three for women and three for men) were created, depending on the subjects’ circumference at measurement point B1:
-
Circumference ≤ 29 cm
-
Circumference > 29 & < 32 cm
-
Circumference ≥ 32 cm.
Then 5 subjects were randomly selected in each group. The only criteria for subject selection were their gender and their circumference at point B1.
Once the subjects were chosen, the order in which they would take part in the study was randomly determined.
Pressure Measurements
Two sensors were positioned on the medial side of the right leg at heights corresponding to the measurement points B1 and C (Fig. 3). Measurement point B1 was chosen following the recommendations of a consensus paper on interface pressure measurements24 and measurement point C was chosen because it corresponds to a part of the calf which is mainly composed of soft tissues. All bandages were applied by the same trained operator. Four types of bandages were applied in the form of a spiral (Fig. 3):
-
B16 with a 50% overlap (B16—2 layers)
-
B16 with a 66% overlap (B16—3 layers)
-
B17 with a 50% overlap (B17—2 layers)
-
B17 with a 66% overlap (B17—3 layers).
The order in which the bandages were applied was randomly determined for each subject.
The bandage was applied in the supine position, after a rest time of 5–10 min (time needed to set the sensors on the subject’s leg). Immediately after the bandage application, the stretch of the bandage around the measurement points B1 and C was measured thanks to a mark printed on the bandage every 100 mm (Fig. 2). The distance between three consecutive marks (initially equal to 200 mm) was measured using a measuring tape once the bandage had been applied on the leg, around the locations of measurement points B1 and C, providing the stretch of the bandage (for example, if the distance was equal to 252 mm, the stretch of the bandage at this location was 252/200 = 1.26).
After bandage application, the subject waited for 2 min in the supine position with the foot slightly raised in order to prevent any contact between the calf and the examination bed. After this time, three successive measurements were acquired. The mean value of the three measurements was considered as the pressure value.
Then the subject was asked to stand up and waited for 2 min before the measures were taken again.
Statistical Analysis
For all results, the values are given with their 95% confidence interval and all histograms represent the mean value and the 95% confidence interval.
Parametric tests (analysis of variance (ANOVA)) were used to evaluate all differences between two samples (whose size n ≥ 30), except to analyse the effect of leg circumference on the pressure (the samples were too small: n < 30).
For the small samples (n < 30), the Kruskal–Wallis one-way analysis of variance was used and then the individual effects were tested with a Mann–Whitney U test (\(\alpha = \frac{0.05}{\text{Number of tests}}\)).
To evaluate the linear correlation between two samples, the coefficient of determination R 2 was computed, which equals the square of the Pearson correlation coefficient between the experimental data and the values from the linear regression. The variable t, which is approximately distributed as a Student’s distribution with n − 2 degrees of freedom for a zero correlation, was used to test the significance of the coefficient of determination R 2: \(t = \sqrt {R^{2} *\frac{n - 2}{{1 - R^{2} }}}\).
The coefficient of determination was used to characterize the linear correlation between the following parameters:
-
the pressure applied by a B16 and the one applied by a B17
-
the pressure applied by 2 layers and the one applied by 3 layers
-
the pressure at measurement point B1 and the one at point C
-
the pressure in the supine position and the one in the standing position.
Difference was considered as significant if p < 0.05.
Results
Bandage Stretch
Considering all bandages together, mean stretch was equal to 1.30 ± 0.007, in accordance with the manufacturer’s recommendations (Fig. 4a). However, the results demonstrated that, irrespective of bandage type (B16 or B17), stretch at point B1 was significantly lower (p < 0.0001) than at point C. Mean stretch at point B1 was lower than recommended (1.27 ± 0.009). Conversely, at point C, mean stretch was higher than recommended (1.33 ± 0.008).

Stretch of the applied bandages (a) and mean pressure values (in the supine position) at measurement point B1 for the different bandages (b).
Also, B17 was applied with a significantly lower stretch than B16 (p < 0.03), respectively 1.29 ± 0.009 and 1.31 ± 0.01.
No significant difference in stretch was observed at point C between bandage applied with 50 and 66% overlapping. Conversely, at point B1, bandages applied with 66% overlapping exhibit higher stretch compared to bandages applied with 50% overlapping (p < 0.002), respectively 1.29 ± 0.012 and 1.26 ± 0.012.
Pressure Values for the Different Bandages
Considering all bandage types, body positions and measurement points, interface pressure increased significantly (p < 0.0001) with bandage overlapping. Interface pressure applied by bandages with 66% overlap were higher than pressure applied by bandages with 50% overlap (Fig. 4b). Similarly, interface pressure increased significantly (p < 0.0001) with bandage elastic modulus: pressures applied by B17 were higher than pressures applied by B16 with the same application technique.
There was no significant difference (p > 0.05) between interface pressure measured with B16 applied with 3 layers and B17 applied with 2 layers.
Gender Influence
There was no overall significant difference between male and female in terms of pressure values and pressure gradient (p > 0.05).
However, pressure variations between supine and standing positions were significantly different between male and female (p < 0.01). These variations were higher for males irrespective of bandage type and measurement point but the difference between sex remained low: the pressure variations between the two positions were +11% for women and +14% for men.
Influence of Bandage Mechanical Properties
The correlations between the pressures exerted by the B16 and the B17 were significant at all measurements points, in all positions and for both application techniques (p < 0.0001) (Fig. 5a). The pressure exerted by the B17 was about 1.5 times as high as the pressure exerted by the B16 whereas the ratio of elastic moduli was 1.95.

Evaluation of the influence on the applied pressure of the bandage mechanical properties (a), application technique (b), and position (d) considering both measurement points; Evaluation of the pressure difference between measurement points B1 and C (c).
Influence of Application Technique
The correlation between the pressures exerted by any bandage applied with 66% overlap and the same bandage applied with 50% overlap was significant at all measurement points and in all positions (p < 0.01) (Fig. 5b).
Influence of Measurement Point (Degressivity)
The results demonstrated that, irrespective of bandage type, application method and body position, the elastic bandages followed the principle of pressure gradient along the length of the limb (Fig. 5c). The measured pressures decreased significantly (p < 0.0001) from point B1 to point C, which means that bandages are degressive (decreasing pressure from the ankle to the knee). Pressures measured at point B1 were about 7% higher than pressures measured at point C.
Influence of Position
The interface pressure increased significantly (p < 0.0001) from the supine position to the standing position, at point B1 and at point C, irrespective of bandage type and application method (Fig. 5d). On average, interface pressures in standing position were 12% higher than in supine position.
Pressure and Circumference
Irrespectively of bandage type, application method and body position, interface pressures tended to decrease when circumference at measurement point B1 increased (Fig. 6). Differences were always significant (p < 0.05) between circumferences at B1 below 29 cm and over 32 cm.

Influence of the leg circumference on the interface pressure at point B1 (o: p < 0.05, *: p < 0.02)—3 groups of subjects were created regarding their leg circumference at measurement point B1.
Discussion
The main strength of the study is to provide a unified investigation of the influence of several parameters on the applied pressure. It quantifies the influence of parameters which were usually not taken into account. Among the most significant results, it was shown with our measurements that the bandage stretch is the key to a better control of the treatment. This data should be provided and considered in every future study on compression bandages. It was also shown that the relationship between applied pressure and elastic modulus of the bandage is not linear, which disputes once again the Laplace’s law in the context of compression bandages.
The objective of the present study was to perform a complete campaign of stretch and interface pressure measurements carried on 30 subjects in order to test the following hypotheses:
Hypothesis 1
The applied pressure is proportional to the bandage elastic modulus
Hypothesis 2
The applied pressure is proportional to the bandage overlapping
Hypothesis 3
The interface pressure significantly decreases when the subjects’ leg circumference increases.
All bandages were applied by the same trained operator and the stretch of the applied bandage was close to the manufacturer’s recommendations. It was noticed, however, that the actual stretch was not constant over the leg and was influenced by the bandage mechanical properties. It was shown that the interface pressure proportionally increased with the elastic modulus (Hypothesis 1) and the overlapping (Hypothesis 2) of the bandage and that it tended to decrease when the leg circumference increased (Hypothesis 3). Moreover, no significant difference was observed between men and women except for the pressure increase between the supine and standing position, which was larger for men. These results lead to a more detailed analysis of the quantified respective influence of the different parameters on the interface pressure, hence an improved understanding of the treatment. The following discussion is structured around three topics: the bandage itself, the subject and its position.
Even though the bandage stretch greatly impacts the level of interface pressure, it was noticed in previous studies4,9 that the bandage tension varied a lot with the bandager, even for experienced bandager. However each bandager seemed to be constant and repeatable in applying bandages.25,30 In this study, all bandages were applied by one trained bandager. This is why the observed trends only reflect one bandager’s application technique and cannot be generalized straightaway.
Nevertheless, the maximum, minimum and mean stretches (respectively 1.45, 1.18 and 1.30) measured in the present study were in the vicinity of the target value of 1.3. This showed that the calibration marker (a rectangle which turns into a square when the stretch is equal to 1.3 (Fig. 2) was effective in having a bandage stretch close to 1.3.10 However, the stretch was not constant over the leg, with larger stretch at point C than at point B1, suggesting an influence of the leg’s diameter on the bandager application technique. Moreover, the stretch was larger for the B16 than for the B17, which could be explained by the fact that the B16 was less stiff, so was easier to stretch, thus providing a different feedback to the operator. Measuring the stretch has shown that its control during bandage application can still be improved.
The results revealed a very strong correlation between the pressure and the bandage mechanical properties (p < 0.00001). The ratio between the pressure exerted by the B17 and that exerted by the B16 was about 1.5. This result raised an important question. Indeed, the ratio between the forces necessary for a 1.3 stretch was equal to 1.95 (force for the B16 = 0.069 N mm−1; force for the B17 = 0.135 N mm−1), which should induce a ratio of 1.95 in pressure according to Laplace’s Law as the pressure is supposed to be directly proportional to the force needed to stretch the bandage. Even though the measured stretch was lower for the B17 than for the B16, the relative difference in the stretch (1.3 ± 0.9% of the stretch) is not sufficient to explain the difference between the experimental ratio (1.48, p < 0.00001) and the expected ratio (1.95), as this ratio is equal to 1.93 considering the slight difference in stretch. It is hypothesized that this difference is due to friction between the bandages and/or the application gesture. However, these are complex phenomena and need to be further investigated.
This study highlighted a strong correlation between the interface pressure and the bandage overlapping (p < 0.00001). The impact of the application technique on the pressure seemed to be in accordance with what was expected. Indeed, the ratio between the pressure applied by a 3-layer bandage and the one applied by a 2-layer bandage should be equal to 3/2 = 1.5. The experimental ratio was about 1.5 (p < 0.00001), which is in accordance with the theory.
The second group of parameters which impacts the interface pressure is directly related to the subjects: their gender and morphology. In this study, pressure measurements were performed on both men and women subjects and the only significant difference between these two populations was for the pressure increase between the supine and the standing position. However the results were not treated separately for men and for women because it has been considered that the difference (3% of the pressure values) was small enough to merge the results. Nonetheless, it may be hypothesized that this small difference is due to the difference in musculature between men and women, which leads to a difference in the geometry variation between the supine and the standing position.
Considering both populations altogether, it was shown that the pressure tended to decrease when the leg circumference increased, which is in general agreement with the Laplace’s law, as the pressure is supposed to be inversely proportional to the radius of curvature. Also, the circumference at point C was larger than the circumference at point B1, hence the fact that the bandage was degressive (the pressure at point B1 is higher than the pressure at point C). However, in the Laplace’s law, only the local radius of curvature has an influence of the pressure. A larger circumference is only the sign of a global radius estimate but it does not consider local radius values. In that sense, our results showed that the level of pressure can vary significantly from a subject to another and that it depends on their leg geometry.
Eventually, the impact of the subject position was investigated: the pressure increased when moving from the supine to the standing position. Due to gravity, the leg geometry changes from the supine to the standing position (Fig. 7). The bandage is applied in the supine position. After bandage application, when the subject stands up, the leg circumference tends to increase,15 which leads to an increase in the bandage stretch and induces a pressure increase. This change in geometry from the supine to standing positions may be a consequence of the muscle group tendency to fall down (because of gravity) and of the increase of hydrostatic blood pressure. The observed pressure difference can be used to characterize the stiffness of the bandage as described in the literature.20 In this study, for which elastic bandages were used, the pressure increase is equal to 6.10 ± 0.54 mmHg. This is in accordance with the previous classification given by Partsch et al.,21 where elastic bandages should display an increase below 10 mmHg.

Difference in leg geometry between supine and standing positions.
Limitations
The subjects in this study were all healthy subjects whose mean age was lower than the mean age of pathologic patients using compression bandage. An interesting perspective will be to carry out the same measurements on pathologic subjects. Moreover, the pressure measurements were performed almost right after the bandage application, therefore neglecting the behavior of compression bandage over time (slipping of the bandage, pressure loss, …). Also, all measurements were static measurements.
All the tests that have been performed on the sensors were performed on a flat surface whereas they were used on a curved surface. This type of sensor was already tested on curved surfaces and showed some imprecisions: they tend to slightly overestimate pressure values.29 However, the largest radius of curvature used in this study was 55 mm whereas the approximated radius of curvature of the limbs in this study went from 40 to 70 mm (for measurement points B1 and C). The influence of curvature on the pressure measured by Picopress, in the range of limb curvature, should be further investigated.
Moreover, an on-going work aims to study the modification in the radius of curvature due to the sensor. Indeed, even though its thickness is very small, its 2 mL volume may induce a local variation in the radius of curvature, which may affect the local value of interface pressure.
All bandages were applied by the same person in order to prevent large variations in the bandage application. However, it would have been interesting to evaluate the variation in the application between different bandagers.
Conclusion
This study aimed at an objective evaluation of the influence of bandage mechanical properties, application technique and subject morphology on the interface pressure applied on the lower leg by elastic compression bandages and the influence of these parameters on the stretch actually applied by the bandager. It has revealed a very strong correlation between the applied pressure and the bandage mechanical properties but also between the pressure and the application technique. In a previous study,20 Partsch has raised the question of the control of the application technique and our study corroborates this claim. A better control of the stretch and the application technique will lead to a better control of the pressure applied by compression bandages. This study also shows the limit of the Laplace’s law in explaining the level of interface pressure and raises some questions about parameters which have not been taken into account yet, such as the friction between the bandage layers. An interesting future direction will address dynamic measurements of the pressure applied by a single compression bandage or the superimposition of 2 compression bandages. These measurements could be performed on pathologic subjects.
References
Agu, O., G. Hamilton, and D. Baker. Graduated compression stockings in the prevention of venous thromboembolism. Br. J. Surg. 86(8):992–1004, 1999.
Al Khaburi, J., A. A. Dehghani-Sanij, E. A. Nelson, and J. Hutchinson. Effect of bandage thickness on interface pressure applied by compression bandages. Med. Eng. Phys. 34(3):378–385, 2012.
Benigni, J. P., J. F. Uhl, A. Cornu-Thénard, and E. Blin. Compression bandages: influence of techniques of use on their clinical efficiency and tolerance. Int. Angiol. 27(1):68–73, 2008.
Bhattacharya, S., T. Shaikh, and R. Purushottam Solao. Development of prototype bandage lapper for constant tension bandaging required for effective medical-clinical treatments. J. Tissue Viability 21(2):54–63, 2012.
Brizzio, E., F. Amsler, B. Lun, and W. Blättler. Comparison of low-strength compression stockings with bandages for the treatment of recalcitrant venous ulcers. J. Vasc. Surg. 51(2):410–416, 2010.
Coull, A., D. Tolson, and J. McIntosh. Class-3c compression bandaging for venous ulcers: comparison of spiral and figure-of-eight techniques. J. Adv. Nurs. 54(3):274–283, 2006.
Damstra, R. J., and H. Partsch. Prospective, randomized, controlled trial comparing the effectiveness of adjustable compression Velcro wraps versus inelastic multicomponent compression bandages in the initial treatment of leg lymphedema. J. Vasc. Surg. Venous Lymphat. Disord. 1(1):13–19, 2013.
Danielsen, L., S. Munk Madsen, L. Henriksen, J. Sindrup, and L. J. Petersen. Subbandage pressure measurements comparing a long-stretch with a short-stretch compression bandage. Acta Derm. Venereol. 78:201–204, 1998.
Hafner, J., W. Lüthi, H. Hänssle, G. Kammerlander, and G. Burg. Instruction of compression therapy by means of interface pressure measurement. Dermatol. Surg. 26(5):481–488, 2000.
Hanna, R., S. Bohbot, and N. Connolly. A comparison of interface pressures of three compression bandage systems. Br. J. Nurs. Mark Allen Publ. 17(20):S16–S24, 2008.
Hirai, M., K. Niimi, H. Iwata, et al. A comparison of interface pressure and stiffness between elastic stockings and bandages. Phlebology 24(3):120–124, 2009.
Huston, R. L. Principles of Biomechanics. Boca Raton: CRC Press, 2009.
Lattimer, C. R., E. Kalodiki, M. Kafeza, M. Azzam, and G. Geroulakos. Quantifying the degree graduated elastic compression stockings enhance venous emptying. Eur. J. Vasc. Endovasc. Surg. 47(1):75–80, 2014.
Milic, D. J., S. S. Zivic, D. C. Bogdanovic, et al. The influence of different sub-bandage pressure values on venous leg ulcers healing when treated with compression therapy. J. Vasc. Surg. 51(3):655–661, 2010.
Mosti, G., and V. Mattaliano. Simultaneous changes of leg circumference and interface pressure under different compression bandages. Eur. J. Vasc. Endovasc. Surg. 33(4):476–482, 2007.
Mosti, G., and H. Partsch. Inelastic bandages maintain their hemodynamic effectiveness over time despite significant pressure loss. J. Vasc. Surg. 52(4):925–931, 2010.
Mosti, G., and H. Partsch. Bandages or double stockings for the initial therapy of venous oedema? A randomized, controlled pilot study. Eur. J. Vasc. Endovasc. Surg. 46(1):142–148, 2013.
Mosti, G., and H. Partsch. Improvement of venous pumping function by double progressive compression stockings: higher pressure over the calf is more important than a graduated pressure profile. Eur. J. Vasc. Endovasc. Surg. 47(5):545–549, 2014.
O’Meara, S., N. Cullum, E. A. Nelson, and J. C. Dumville. Compression for venous leg ulcers. In: Cochrane Database of Systematic Reviews, edited by The Cochrane Collaboration, and S. O’Meara. Chichester: Wiley, 2012.
Partsch, H. The use of pressure change on standing as a surrogate measure of the stiffness of a compression bandage. Eur. J. Vasc. Endovasc. Surg. 30(4):415–421, 2005.
Partsch, H. The static stiffness index: a simple method to assess the elastic property of compression material in vivo. Dermatol. Surg. 31(6):625–630, 2005.
Partsch, H., and G. Mosti. Comparison of three portable instruments to measure compression pressure. Int. Angiol. 29(5):426–430, 2010.
Partsch, B., and H. Partsch. Calf compression pressure required to achieve venous closure from supine to standing positions. J. Vasc. Surg. 42(4):734–738, 2005.
Partsch, H., M. Clark, S. Bassez, et al. Measurement of lower leg compression in vivo: recommendations for the performance of measurements of interface pressure and stiffness: consensus statement. Dermatol. Surg. 32(2):224–232, 2006; (discussion 233).
Raj, T. B., M. Goddard, and G. S. Makin. How long do compression bandages maintain their pressure during ambulatory treatment of varicose veins? Br. J. Surg. 67(2):122–124, 1980.
Rimaud, D., R. Convert, and P. Calmels. In vivo measurement of compression bandage interface pressures: the first study. Ann. Phys. Rehabil. Med. 57(6–7):394–408, 2014.
Rohan, P.-Y., P. Badel, B. Lun, D. Rastel, and S. Avril. Prediction of the biomechanical effects of compression therapy on deep veins using finite element modelling. Ann. Biomed. Eng. 43(2):314–324, 2015.
Thomas, S. The use of the Laplace equation in the calculation of sub-bandage pressure. Eur. Wound Manage. Assoc. 3:21–23, 2003.
Thomas, S. Practical limitations of two devices used for the measurement of sub-bandage pressure: implications for clinical practice. J. Wound Care. 23(6):300–313, 2014.
Thomas, S., and P. Fram. Laboratory-based evaluation of a compression-bandaging system. Nurs. Times. 99(40):24–28, 2003.
The International Lymphoedema Framework. Best Practice for the Management of Lymphoedema, 2nd edn.
Conflict of interest
Thuasne is a compression bandage manufacturer.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Amit Gefen oversaw the review of this article.
Rights and permissions
About this article

Cite this article
Chassagne, F., Martin, F., Badel, P. et al. Experimental Investigation of Pressure Applied on the Lower Leg by Elastic Compression Bandage. Ann Biomed Eng 43, 2967–2977 (2015). https://doi.org/10.1007/s10439-015-1352-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-015-1352-1