
Abstract
Aim
Computer vision syndrome (CVS) is a major occupational threat in the twentyfirst century, leading to decreased sleep quality, reduced work efficiency, and depression. This study aimed to assess the prevalence of CVS and the associated risk factors among undergraduate students of the American University of Armenia (AUA).
Subject and methods
An online survey was conducted among 143 students aged 18 years and above in June 2021. Participants provided information about their socio-demographics, health, smoking, duration of computer/video display terminal (VDT) device use, daily hours of computer use before and during the SARS-CoV-2 pandemic, and protective habits while using the computer/VDT devices. The Computer Vision Syndrome Questionnaire was used to assess the presence of CVS.
Results
The mean age of participants was 19.7 (SD ± 1.37). The majority of participants were women (79.4%). Allergy was the most prevalent chronic disease in the sample (17.5%). Almost 62.2% of participants reported having refractive errors (REs). About 9.0% of the study sample were current smokers. Daily hours of computer use before and during SARS–CoV-2 pandemic were 5.5 and 10.0 respectively. Only 10.7% of participants were taking breaks every 20 minutes while using computer/VDT devices. The prevalence of CVS was 78.3%. The most commonly reported symptoms of CVS were eye redness (74.6%), headache (72.5%), itching eye (71.2%), burning eye (70.5%), tearing eye (66.7%), and blurred vision (63.4%). In the adjusted analysis, the presence of REs, sitting position, viewing distance in using the computer/VDT devices, and voluntary blinking were associated with CVS.
Conclusion
This study found a high prevalence of CVS in the study population. Following the recommendations on correct sitting position and viewing distance while using computer/VDT devices might reduce the prevalence of CVS in the target population. The interventions should particularly focus on the students with REs who are disproportionately affected by CVS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The great advancements in information technology and increasing use of digital devices, observed globally over the past decades, have given rise to a number of symptoms that have been termed computer vision syndrome (CVS) (Sheppard and Wolffsohn 2018; Rosenfield 2011). According to the American Optometric Association (AOA), CVS, also known as digital eye strain (DES), is a complex of eye and vision-related symptoms experienced due to sustained use of computers, laptops, smartphones, tablets, e-readers, and other digital devices, which are collectively called the devices with video display terminals (VDT) (Computer vision syndrome | AOA n.d.). CVS is one of the leading occupational hazards of the twenty-first century, affecting about 90% of computer users (Akowuah et al. 2021; Smaldone et al. 2007; Wimalasundera 2009). Nowadays, students spend many hours in front of their computer screens. The use of computers, laptops, tablets, and other digital devices is becoming increasingly common among students in educational institutions (Cantó-Sancho et al. 2021). Wang et al. found that CVS affected 77.1% of undergraduate students and 69.1% of medical students enrolled in the University of Illinois at Chicago in 2021 (Wang et al. 2023), while Noreen and Umar found that CVS was reported in 98.7% of undergraduate students from Pakistan in 2020 (Noreen and Umar 2021). Numerous studies have investigated the prevalence of CVS and associated factors. However, most of these studies concentrated on Western populations, while no studies have explored the effect of VDT use on eye health in the Armenian population. This study aimed to assess the prevalence of CVS and explore factors contributing to it among the undergraduate students of the American University of Armenia (AUA).
The symptoms associated with CVS are grouped into four categories: 1) visual symptoms such as slowness of focus change, double vision, and blurred vision, 2) ocular surface-related symptoms such as irritated eyes, watery eyes, dry eyes, and issues with contact lens use (Akkaya et al. 2018; Iqbal et al. 2021), 3) asthenopic symptoms such as eye strain, tired eyes, glare sensitivity, and sore eyes, and 4) extra-ocular symptoms such as headache, neck pain, shoulder pain, and lower back pain (Dhar-Munshi et al. 2019; Computer vision syndrome 2022). In addition to eye health-related problems, the excessive use of computer/VDT devices has been shown to lead to other conditions, such as sleep disorders, anxiety, insomnia, stress, depression, and musculoskeletal disorders (Hakala et al. 2010; Sirajudeen et al. 2018).
Risk factors contributing to the development and worsening of the symptoms of CVS include insufficient lighting of the computer screen (such as inappropriate screen brightness/contrast, glare, and inappropriate viewing angle). Staring at screens for extended periods can cause eye strain and fatigue, leading to symptoms such as dry eyes, blurred vision, and headaches. Screens emit blue light, which may disrupt the sleep–wake cycle and contribute to CVS symptoms. Additionally, constant focusing and refocusing on-screen content can strain the eye muscles. Reduced blinking while looking at screens can lead to dry eyes and irritation. In addition, 3D screens affect accommodation and convergence abilities (Pavel et al. 2023). Other factors contributing to the worsening of the CVS symptoms include improper brightness in the working area (not sufficient illumination for employees to see their work, and improper lighting design, such as illumination levels and colour spectrum, contributing to eye strain and fatigue), long duration of the computer use, improper viewing distances of the screen, poor or abnormal seating position, use of blue-light-emitting devices, smoking, refractive errors (REs), and some medications (COX-2 inhibitors, anti-epileptic drugs, anti-hypertensive drugs) (Sun 2010; Peragallo et al. 2013; Kozeis 2009; Ranganatha and Jailkhani 2019; Madhan 2009; Hilton et al. 2004). To reduce the CVS symptoms, the AOA recommended taking a break after every 20 minutes of work by looking at an object located at least 20 feet away for a duration of 20 seconds (Computer vision syndrome | AOA n.d.). Significant reduction of CVS symptoms can be achieved by using either spectacles or contact lenses that specifically block blue light emissions from the VDT devices (Sheppard 2018).
The SARS-CoV-2 pandemic reinforced the use of digital devices across the globe. Several studies have reported the increased use of VDT and associated issues with eye health (Peiris et al. 2020; Bahkir 2020). For example, around 68% of the undergraduate medical students in Malaysia reported that the CVS symptoms had occurred or started to become worse after the SARS-CoV-2 pandemic, when academic classes switched to online mode (Peiris et al. 2020). A study conducted among Stanford University students reported that students spent about 50.2% and 77.6% of their daytime staring at a laptop, tablet, or phone in an average week before and during SARS-CoV-2 pandemic respectively (Safranek 2020; Laurinavicius 2022).
In the last few decades, there has been a significant increase in Internet use in Armenia. According to the report published by the National Statistical Service of the Republic of Armenia, as of December 2018, 72.4% of the population has been using the Internet, a substantial increase from 0.1% recorded in 2000 (Armenia Internet Usage and Telecommunications Reports 2019). According to recent estimates, the E-participation index of Armenia was 0.5674 in 2018, which was higher than the world average E-participation index of 0.5491 in the same year, suggesting high accessibility of the Internet and digital device usage (United Nations 2018). The high accessibility of the Internet directly reflects the frequent use of computers and other VDT devices (Armenia Internet Usage and Telecommunications Reports 2019).
Methods
Study population and setting
This cross-sectional study was conducted among AUA undergraduate students aged 18 years and above. Overall, 143 out of 1,474 undergraduate students (American University of Armenia 2020–2021 Factsheet n.d.) participated in the online survey in June 2021. AUA is an international university with a student body of 2,005, located in the capital city of Armenia, offering both graduate and undergraduate degree programs (American University of Armenia 2022).
Study instrument
A structured self-administered questionnaire was developed to collect information about participants’ socio-demographic characteristics (age, gender, study program, and socio-economic status), health characteristics [medication use, presence of chronic non-communicable diseases, eye diseases, and refractive error (RE)], smoking status, seating position, and screen distance while using computer/other VDT devices, the presence of glare on the computer/other VDT device screen, lifetime duration of computer/other VDT devices use, weekly hours of computer/other VDT devices use at present, and time spent on a computer/other VDT devices daily before and during SARS-CoV-2 pandemic. Protective habits while using computer/other VDT devices such as taking breaks, wearing eyeglasses containing anti-reflecting and/or blue light filter coating, voluntary blinking, lighting condition of working area, adjusting the contrast of the computer/other VDT devices with the surrounding brightness, using an anti-glare/blue light filter for the computer/other VDT devices screen, and using lubricant eye drops were also explored.
To assess the time spent on computer/other VDT devices before and during SARS-CoV-2 pandemic restrictions, participants were asked to specify the average number of hours of computer/other VDT devices use per day before/during the restrictions which were enacted due to SARS-CoV-2 pandemic (around March/April 2020). The Computer Vision Syndrome Questionnaire (CVS-Q) was used to assess the presence of CVS among the study population. The CVS-Q questionnaire is a valid and reliable tool used to assess visual health in computer workers in both clinical trials and research studies (Seguí et al. 2015). It measured the frequency of the following 16 symptoms: burning eyes, itching eyes, feeling of a foreign body in the eyes, tearing eyes, excessive blinking, eye redness, eye pain, heavy eyelids, dryness in eyes, blurred vision, double vision, difficulty in focusing for near vision, increased sensitivity to light, colored halos around objects, feeling that sight is worsening, and headache. The response option scores ranged from zero (never) to two (often/always) (Seguí et al. 2015). If the participants reported having symptoms “occasionally,” or “often/always,” they were asked to rate the intensity of the symptoms, choosing between the options “moderate” (one) or “intense” (two). The frequency and intensity of a symptom were multiplied to obtain the score for each symptom. The total score summed the scores of all sixteen symptoms. If the total score was ≥ 6, the participants were categorized as having CVS (Seguí et al. 2015).
Data collection
The study team generated online survey link using the Achemer tool (https://www.alchemer.com/). The head of the AUA student council shared the link among AUA undergraduate students via e-mail, asking them to complete the questionnaire. The link was sent out on June 4; after which the student council sent weekly reminders to increase the participation rate. The database with the survey data, which did not contain any identifiers, was transferred to the SPSS statistical package after the data collection was completed.
Ethical considerations
This study obtained ethical approval from the Institutional Review Board of the American University of Armenia (Protocol #: AUA-2020-004).
Analysis
The outcome variable of interest was the presence of CVS. Frequencies and proportions along with means and standard deviations were used for the descriptive analysis. Simple and multivariable logistic regression analysis explored associations between risk factors and CVS. The multivariable analysis included all variables that were found to be associated with CVS at the p < 0.05 level in the simple logistic regression analysis. We used the two-sample t-test to assess the difference between daily hours of computer/other VDT devices use before and during SARS-CoV-2 pandemic among people with and without CVS. SPSS version 23.0 was used to analyse the data (SPSS inc., Chicago, IL, USA).
Results
Socio-demographic and health characteristics
The mean age of participants was 19.7 (SD = 1.4). The vast majority of participants were female (79.4%). About 51% of participants reported their family’s standard of living above average. Allergy (seasonal allergy, dust allergy, pollen allergy, allergic rhinitis) was the most prevalent chronic condition in the sample (17.5%). Nearly 7.7% of respondents reported having eye diseases such as acute, chronic or allergic conjunctivitis, eye teaming disorder, amblyopia, and nystagmus. Almost 62.2% of participants reported having RE; the majority were myopic (Table 1).
CVS prevalence and symptoms
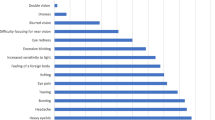
The prevalence of CVS was 78.3%. The most commonly reported CVS symptoms in our study population included eye redness (74.6%), headache (72.5%), itching eye (71.2%), burning eye (70.5%), tearing eye (66.7%) and blurred vision (63.4%) (Fig. 1).

Prevalence of CVS symptoms in the study sample
VDT use habits and characteristics
Not positioning their face at the level of a computer screen while using computer/other VDT devices was reported by 51.5% of participants. The majority of participants (69.6%) reported viewing distance of less than 50cm between the computer/other VDT devices screen and their eyes. Only 10.7% of participants followed the habit of taking a regular break every 20 minutes while using the computer/other VDT devices. About 72% of the students reported having the habit of adjusting the screen contrast in accordance with the room brightness. The mean lifetime duration of using computer/other VDT devices was about 8.4 years (SD = 3.82), while the mean weekly hours of computer use at the present time were about 60.3 hours (SD = 25.0) (Table 2).
Daily hours of computer use significantly increased during the SARS-CoV-2 pandemic in both groups (with CVS and without CVS) (Supplementary Table 1). About 69.7% of all students reported that the frequency and intensity of the CVS symptoms increased after the restrictions due to the SARS-CoV-2 pandemic (severe lock-down) in Armenia (March–April 2020).
Simple and multivariable logistic regression analysis
In the simple logistic regression analysis, female gender, study program, the presence of RE, siting position and the viewing distance in using computer/VDT devices, weekly hours of computer/other VDT devices use in the present, the frequency of taking breaks from using computer/VDT devices and having a habit of voluntary blinking were significantly associated with the CVS (Table 3). In the adjusted model, the presence of RE (OR = 3.64 95% CI: 1.20–11.0, p = 0.02), inappropriate siting position (the face is not at the level of computer screen) (OR = 3․35, 95% CI: 1.10–10․2, p = 0.03) and the viewing distance (≤ 50 cm) (OR = 3․27, 95% CI: 1.09–9․87, p = 0.03) in using computer/VDT devices, and having the habit of voluntary blinking (OR = 8․73, 95% CI: 1.49–51․1, p = 0.02) maintained significant associations with CVS, while the effect of other factors disappeared (Table 4).
Discussion
This study assessed the prevalence of CVS and explored the factors associated with it among undergraduate students in Armenia — a country for which no information on CVS has been previously available in the literature. The rate of CVS in our study was 78.3%, which is higher when compared to most of the estimates from the studies conducted in other populations, including Spanish university students in 2020 (76.6%) (Cantó-Sancho et al. 2021), Chinese medical students during the SARS-CoV-2 pandemic in 2021 (50.8%) (Wang et al. 2021), and computer users in Ethiopia in 2022 (73.2%) (Adane et al. 2022). Our study findings are most comparable to the results of the study conducted among Indian students in 2019, where the CVS rate reached 86.7% (Gammoh 2021; Ranganatha and Jailkhani 2019). Poor knowledge and improper practice in using computer/VDT devices might explain the high CVS prevalence in our study sample. The elevated CVS prevalence in most of the countries might also be due to the timing of the study, which coincided with the SARS-CoV-2 pandemic, a period marked by widespread digitalization across every field of life.
The substantial increase in the time spent on the computer/other VDT devices as a result of SARS-CoV-2 pandemic is a concerning finding, which is in line with other reports on this topic (Peiris et al. 2020; Bahkir and Grandee 2020). This vast change in the habits of the student population (and possibly other segments of the population as well) should be mitigated by increasing awareness about the associated risks to eye health, and interventions promoting safer VDT use.
In our study, students who had REs reported a high rate of CVS, which is consistent with the literature. Muma et al., in a study conducted among students from Maseno University in Kenya in 2019, found that students, who had visual acuity < 6/18 had a higher risk for developing CVS (p = 0.02) than those who had normal vision (Muma et al. 2020). In the same study, students who had REs reported more symptoms of CVS compared to those who did not have REs (70% vs 24%). The presence of RE such as myopia, hyperopia, or astigmatism increases the eyestrain while using VDT devices and further worsens the CVS symptoms (Muma et al. 2020). According to the American Academy of Ophthalmology, having slight RE abruptly exacerbates the CVS symptoms (Computer vision syndrome n.d.). We did not specifically check the presence of uncorrected refractive errors (URE) in our study, which could contribute to this association (Muma et al. 2020). Future studies should focus on the association of UREs with the CVS.
Those students who reported not having their face at the level of the screen (inappropriate sitting position) and viewing distance of ≤ 50 cm while using computer/VDT devices, had higher odds of CVS than those who reported correct practices in the adjusted analysis in our study. These findings are consistent with the literature. Adane et al. reported that CVS is significantly associated with inappropriate sitting position (the face is not at the level of computer screen and sitting in bent back position) among the computer users in Ethiopia (Adane et al. 2022). Several studies reported that a viewing distance of less than 50 cm between the eye and VDT device screen can aggravate the CVS symptoms (Jaschinski et al. 1998; Reddy et al. 2013). Boadi-Kusi et al. suggested that increasing awareness about CVS and practicing good ergonomic positions while using computers/other VDT could lessen the increasing prevalence of CVS and its burden (Boadi-Kusi et al. 2020). Improper sitting position while using computer/other VDT devices produces ocular discomfort and tension, which forces the eye to become more focused and causes a spasm of eye muscles, eventually resulting in CVS. Extended viewing of the monitor at a close distance leads to fatigue of convergence, which results in eye strain and CVS (Charpe and Kaushik 2009).
Surprisingly, voluntary blinking was associated with higher odds of CVS in the adjusted analysis in our study. Students who had a voluntary blinking habit had higher odds of having CVS than those who did not have such a habit. Meanwhile, according to the AOA recommendations, having regular voluntary blinking habits and taking a brief pause by looking at distant objects between prolonged screen-time relaxes the eye muscles, thereby decreasing the frequency and intensity of CVS significantly (Computer vision syndrome | AOA n.d.). In contrast, Portello & Rosenfield reported that increased blinking rate did not significantly reduce CVS symptoms, even in those who have reported high score of CVS (Portello & Rosenfield 2010). Since our study was cross-sectional, it is hard to ascertain if voluntary blinking results in CVS or CVS itself leads to excessive blinking. Also, since we used a self-administered questionnaire to assess voluntary blinking, it is possible that some of the participants missed the exact meaning of the question and reported both voluntary and involuntary blinking habits. Future studies could further explore the causal link.
We would like to acknowledge several limitations. The rate of CVS in our study might be overestimated because people with CVS might have been more interested in participating in the survey than those without the symptoms. Also, since we focused on the students of one educational institution, our study findings have limited generalizability to the entire student population in Armenia, and might not be generalizable to other age groups. Another limitation of our study could be the small sample size and the use of non-validated questions for some variables.
We found a high prevalence of CVS in the study sample. Following the recommendations on the sitting position and viewing distance while using computer/VDT devices might reduce the prevalence of CVS in the student population. Public health programs increasing awareness about CVS symptoms, and following protective measures such as a proper ergonomic position while using the computer/other VDT devices and following the AOA 20–20–20 rule (taking a 20-second break to view something 20 feet away every 20 minutes) might alleviate digital eyestrain and mitigate CVS. We also recommend including people with RE (corrected and uncorrected) in such interventions and focusing on the link between RE and CVS in future investigations.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author [AG] on reasonable request.
Code availability
Not applicable
References
Adane F, Alamneh YM, Desta M (2022) Computer vision syndrome and predictors among computer users in Ethiopia: a systematic review and meta-analysis. Trop Med Health 50:1–12. https://doi.org/10.1186/S41182-022-00418-3/FIGURES/5
Akkaya S, Atakan T, Acikalin B, Aksoy S, Ozkurt Y (2018) Effects of long-term computer use on eye dryness. Northern Clin Istanbul 5:319. https://doi.org/10.14744/NCI.2017.54036
Akowuah PK, Augustine NN, Ankamah-Lomotey S, Frimpong AA, Fummey J, Boadi P, Osei-Poku K, Adjei-Anang J (2021) Digital device use, computer vision syndrome, and sleep quality among an African undergraduate population. Adv Public Health 2021:6611348. https://doi.org/10.1155/2021/6611348
American University of Armenia (2022) Accessed 26 June 2022. https://aua.am
American University of Armenia 2020–2021 Factsheet (n.d.) Accessed 26 June 2022. https://ira.aua.am/files/2021/09/2020-2021-Factsheet.ENG_-1.pdf
Armenia Internet Usage and Telecommunications Reports (2019) Accessed 26 June 2022. https://www.internetworldstats.com/asia/am.htm#links
Bahkir FA, Grandee SS (2020) Impact of the COVID-19 lockdown on digital device-related ocular health. Indian J Ophthalmol 68:2378–2383. https://doi.org/10.4103/ijo.IJO_2306_20
Boadi-Kusi SB, Abu SL, Acheampong GO, Adueming POW, Abu EK (2020) Association between poor ergophthalmologic practices and computer vision syndrome among university administrative staff in Ghana. J Environ Public Health 2020:7516357. https://doi.org/10.1155/2020/7516357
Cantó-Sancho N, Sánchez-Brau M, Ivorra-Soler B, Seguí-Crespo M (2021) Computer vision syndrome prevalence according to individual and video display terminal exposure characteristics in Spanish university students. Int J Clin Pract 73:e13681. https://doi.org/10.1111/ijcp.13681
Charpe NA, Kaushik V (2009) Computer vision syndrome (CVS): recognition and control in software professionals. J Hum Ecol 28:67–69
Computer vision syndrome (digital eye strain) — EyeWiki (2022) Accessed 26 June 2022. https://eyewiki.aao.org/Computer_Vision_Syndrome_(Digital_Eye_Strain)
Computer vision syndrome | AOA (n.d.) Accessed 26 June 2022. https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/computer-vision-syndrome?sso=y
Dhar-Munshi S, Souad A, Munshi S (2019) Computer vision syndrome: an update. British J Neurosci Nurs 15(Sup2):S10–S11. https://doi.org/10.12968/bjnn.2019.15.sup2.s10
Gammoh Y (2021) Digital eye strain and its risk factors among a university student population in Jordan: a cross-sectional study. Cureus 13(2):e13575. https://doi.org/10.7759/CUREUS.13575
Hakala PT, Saarni LA, Ketola RL, Rahkola ET, Salminen JJ, Rimpela AH (2010) Computer-associated health complaints and sources of ergonomic instructions in computer-related issues among Finnish adolescents: a cross-sectional study. BMC Public Health 10:11. https://doi.org/10.1186/1471-2458-10-11
Hilton EJR, Sarah L, Hosking BT (2004) The effect of antiepileptic drugs on visual performance. Seizure 13(2):113–128. https://doi.org/10.1016/S1059-1311(03)00082-7
Iqbal M, Said O, Ibrahim O, Soliman A (2021) Visual sequelae of computer vision syndrome: a cross-sectional case-control study. J Ophthalmol 2021:6630286. https://doi.org/10.1155/2021/6630286
Jaschinski W, Heuer H, Kylian H (1998) Preferred position of visual displays relative to the eyes: a field study of visual strain and individual differences. Ergonomics 41(7):1034–1049. https://doi.org/10.1080/001401398186586
Kozeis N (2009) Impact of computer use on children’s vision. Hippokratia 13:230–231
Laurinavicius T (2022) Screen time statistics 2022: average usage of mobile, social media & TV. Best Writing. https://bestwriting.com/blog/screen-time-statistics
Madhan MR (2009) Computer vision syndrome. Nurs J India 100(10):236–237
Muma SL, Omondi D, Jaramogi A, Odinga O, Ogola PO (2020) Association between visual acuity, ocular pathology and refractive error with computer vision syndrome: cross sectional university study in Kenya. Research Square (published online). https://doi.org/10.21203/RS.3.RS-125167/V1
Noreen K, Umar M (2021) Computer vision syndrome (CVS) and Its associated risk factors among undergraduate medical students in midst of COVID-19. Pakistan J Ophthalmol 37(1):102–108
Pavel IA, Bogdanici CM, Donica VC, Anton N, Savu B, Chiriac CP, Pavel CD, Salavastru SC (2023) Computer vision syndrome: an ophthalmic pathology of the modern era. Medicina (Kaunas) 59(2):412. https://doi.org/10.3390/medicina59020412
Peiris V, Mahendran PS, Faiz MA, Rajasekharan R, Ameresekera K (2020) Prevalence and associated factors of computer vision syndrome among undergraduate students of Malaysia during the COVID 19 pandemic. Int J Biomed Clin Sci 5:399–407
Peragallo J, Biousse V, Newman NJ (2013) Ocular manifestations of drug and alcohol abuse. Curr Opin Ophthalmol 24(6):566–573. https://doi.org/10.1097/ICU.0b013e3283654db2
Portello JK, Rosenfield M (2010) Effect of blink rate on computer vision syndrome. Investig Ophthalmol Vis Sci 51(13):950
Ranganatha SC, Jailkhani S (2019) Prevalence and associated risk factors of computer vision syndrome among the computer science students of an engineering college of Bengaluru — a cross-sectional study. Galore Int J Health Sci Res 4 (3):10–15
Reddy SC, Low CK, Lim YP, Low LL, Mardina F, Nursaleha MP (2013) Computer vision syndrome: a study of knowledge and practices in university students. Nepalese J Ophthalmol 5(2):161–168. https://doi.org/10.3126/nepjoph.v5i2.8707
Rosenfield M (2011) Computer vision syndrome: a review of ocular Causes and potential preatments. Ophthalmic Physiol Optics 31(5):502–515. https://doi.org/10.1111/j.1475-1313.2011.00834.x
Safranek C (2020) Stanford students now spend four-fifths of the waking day staring at a screen; is this the new college normal? The Stanford Daily. https://stanforddaily.com/2020/07/08/stanford-students-now-spend-four-fifths-of-the-waking-day-staring-at-a-screen-is-this-the-new-college-normal/
Seguí MM, Cabrero-García J, Crespo A, Verdú J, Ronda E (2015) A reliable and valid questionnaire was developed to measure computer vision syndrome at the workplace. J Clin Epidemiol 68:662–673. https://doi.org/10.1016/j.jclinepi.2015.01.015
Sheppard AL, Wolffsohn JS (2018) Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol 3:e000146. https://doi.org/10.1136/bmjophth-2018-000146
Sirajudeen MS, Muthusamy H, Alqahtani M, Waly M, Jilani AK (2018) Computer-related health problems among university students in Majmaah region, Saudi Arabia. Biomed Res 29(11):2405–2415
Smaldone A, Honig JC, Byrne MW (2007) Sleepless in America: inadequate sleep and relationships to health and well-being of our nation’s children. Pediatrics 119(1):S29–S37
Sun BC (2010) Computer vision syndrome. Ophthalmol China 19:289–293. https://doi.org/10.3329/fmcj.v10i1.27923
United Nations (2018) United Nations e-Government Knowledge Database. United Nations, New York. Accessed 26 June 2022. https://publicadministration.un.org/egovkb/en-us/Data/Country-Information/id/8-Armenia
Wang L, Wei X, Deng Y (2021) Computer vision syndrome during SARS-CoV-2 outbreak in university students: a comparison between online courses and classroom lectures. Front Public Heal 9:696036. https://doi.org/10.3389/FPUBH.2021.696036/BIBTEX
Wang C, Joltikov KA, Kravets S, Edward DP (2023) Computer vision syndrome in undergraduate and medical students during the COVID-19 pandemic. Clin Ophthalmol 17:1087–1096. https://doi.org/10.2147/OPTH.S405249
Watson S (2021) Computer vision syndrome: causes, symptoms and treatments. WebMD. Accessed 21 March 2023, 2022https://www.webmd.com/eye-health/computer-vision-syndrome#1
Wimalasundera S (2009) Computer vision syndrome. Galle Med J 11:25. https://doi.org/10.4038/gmj.v11i1.1115
Acknowledgments
We are thankful to the study participants for their support during the implementation of the study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Rishba Getzie Peter, Aida Giloyan, Tsovinar Harutyunyan and Varduhi Petrosyan. The first draft of the manuscript was written by Rishba Getzie Peter and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Approval was obtained from the Institutional Review Board of the American University of Armenia. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable
Conflicts of interest/competing interests
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Peter, R.G., Giloyan, A., Harutyunyan, T. et al. Computer vision syndrome (CVS): the assessment of prevalence and associated risk factors among the students of the American University of Armenia. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-02138-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-02138-2