
Abstract
Purpose
The current study examined attitudes and behavior of first degree emergency medical technician (paramedic) students at Ben-Gurion University of the Negev in Israel toward DUI (driving under the influence).
Methods
Students were asked to complete an anonymous, self-administered, multiple-choice questionnaire and a demographic questionnaire.
Results
We found that 42% of respondents (n = 59) had driven after drinking, and 56% of them had driven after more than one drink in the past year. Furthermore, 70% of the students had been designated drivers in the past year, 31% of whom had drunk-driven. No significant difference was found between past volunteers at MDA* and those who did not volunteer regarding the number of DUI events or the amount of alcohol consumed, but those who did volunteer drank more when engaging in DUI.
Conclusion
Our findings are worrisome and may reveal the strength of social norms for consumption of alcohol on one hand and the lack of suitable education regarding the dangers of alcohol in the health care department on the other hand.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Motor vehicle accidents (MVA) are the eighth leading cause of death globally, killing approximately 1.24 million people a year. It is also the leading cause of death among young people aged 15–29 years. Furthermore, according to the World Health Organization, an additional 20–50 million people a year are injured in MVAs (World Health Organization 2013). The spectrum of injury ranges from those who need urgent treatment to those who do not need it at all (Peden et al. 2004; Lozano et al. 2012).
Drivers under the influence of alcohol are 30% more likely to be involved in an MVA (Shinar 2007; Engström et al. 2008; Fillmore et al. 2008; Jones and Holmgren 2009; Moan et al. 2013).
Crashes involving drinking and driving often exhibit a number of characteristics: Driving under the influence (DUI) or driving while intoxicated (DWI) crashes often involve high speed and a single vehicle running off the road; they occur more often at night (when more alcohol is consumed) and generally on weekends or during periods of high leisure activity (US Department of Transportation 2013).
Studies suggest that 30% of the total fatalities from car crashes are alcohol related (Shinar 2007; Engström et al. 2008; Moan et al. 2013). Drivers between the ages of 21–34 years comprise the highest proportion of the fatally injured who are found to be intoxicated at the time of the MVA (Rivara et al. 2007).
DUI is determined by the blood alcohol content (BAC). MVA is considered to be alcohol-related if at least one driver involved in the crash is found to have had a BAC of 0.01 g/dl or higher (National Highway Traffic Safety Administration 2013; World Health Organization 2013). Each country has its own legislation marking the BAC limit for DUI. In the US and the UK, for example, the BAC is 0.08 g/dl, while in most European Union (EU) states, the BAC has changed to 0.05 g/dl (World Health Organization 2013). Therefore, the definition and registration of DUI vary accordingly. Young adults driving with a BAC level of 0.05 g/dl are more than twice as likely to have a road traffic crash as more experienced drivers (World Health Organization 2013). How is this possible?
The physiological effects of alcohol on drivers have been researched in numerous studies. It has been found that its absorption from the digestive system is dependent on the type of alcoholic beverage, the amount consumed, the speed of drinking and other variables affecting stomach emptying. Further, the effects become progressively worse as the BAC increases (Shinar 2007; Jones and Holmgren 2009). Alcohol affects the brain’s frontal lobe, responsible for abstract reasoning, sustained and selective attention, reaction time, mental flexibility, motor programming and executive control of action, resistance to interference, inhibitory control and environmental autonomy. These brain impairments intensify with the increase in alcohol consumption, even at a BAC of 0.01% (Domingues et al. 2009). Other studies have established that the brain, and especially the frontal lobe, keeps developing and its function keeps improving during early adulthood, up to the end of the 3rd decade of life. This results in the underdevelopment of these brain functions among the young population of drivers. Consequently, their impulse control and abstract thinking are deficient (Sowell et al. 1999). These findings match other research asserting the effect of alcohol on young adults (aged 18–21 years) is greater than on older adults (Shinar 2007; Fillmore et al. 2008; Liang and Huang 2008). Young adults in the 20–29-year age group have a three times estimated risk compared with drivers aged 30 years and older at all BAC levels (Peden et al. 2004).
DUI is most prevalent among university-based youth worldwide (LaBrie et al. 2011); therefore, DUI among college students is a serious international health concern (Kenney et al. 2013). On the other hand, traffic enforcement and anti-drinking and driving laws worldwide seem to have a great deal of influence on the incidence of drunk driving, but none on students’ attitudes and beliefs in this matter, on the other. Evidence of connections between the level of police enforcement and both driving behavior and the number of car accidents has been provided in many studies, proving that students are more likely to drive under the influence of alcohol in countries where the police and law enforcements are poor (Shinar 2007; Liang and Huang 2008). Moreover, countries that legislated zero-tolerance DUI laws experienced a decreased incidence of these behaviors by about of 14–17% (Liang and Huang 2008). Drinking alcoholic beverages is a common characteristic of social meetings, and its onset age is continually decreasing. Young drivers are well aware of the negative influence of alcohol and driving; however, they consciously keep adopting this behavior (LaBrie et al. 2011; Dhami and García-Retamero 2012).
Different forms of population-based interventions attempting to decrease the incidence of DUI have been tested all around the world. A leading intervention is the designated driver program, requiring individuals to plan who will drive whom after drinking, with the one single purpose of the designated driver consuming zero alcohol. When this intervention was examined, it was found that the designated drivers had not totally abstained from drinking, but drank less than they usually do (Shinar 2007; Rivara et al. 2007).
It has been found that young drivers who have had a negative DUI experience in their younger years are more likely to correctly estimate their ability to drive with regard to the amount of alcohol consumed than those who have not had any negative drunk-driving experience. Furthermore, they were also less inclined to DUI than drivers with no bad experience (DeMartini et al. 2011; Cartwright and Asbridge 2011; Vassallo et al. 2007; Jones and Holmgren 2009). Accordingly, their attitudes toward drinking and driving were more positive and forgiving (Rivara et al. 2007; LaBrie et al. 2011).
On the other side of the divide, a negative influence of exposure to crisis situations has been found in a vast number of studies on the working and volunteering staff of emergency medical technicians (EMTs), firefighters and others in the first aid (emergency services) field. Approximately half of the adults researched suffered, to varying degrees, from these experiences, which can be summarized as post-traumatic stress disorder (PTSD) (Allison et al. 1987; Donnelly 2012; Wagner et al. 1998). These effects are compounded by the feeling of a lack of control and helplessness in helping others (Bryant and Harvey 1996). Youth corps operated by those organizations are also exposed to the same difficulties. The emergency medical services (EMS) recruit adolescents to volunteer at different emergency organizations around the world. They usually start their practice at the age of 15–16 years. The teenagers undergo strict training to become professional and effective assistants to the regular ambulance staff when joining them on emergency calls [BRAVO Volunteer Ambulance Services (n.d); Chappaqua Volunteer Ambulance Youth Corps (n.d); Saint John Ambulance (n.d); New City Volunteer Ambulance Youth Corps (n.d)].
In Israel, road accidents constitute about one tenth of all Magen David Adom (MDA) calls and an estimated quarter (25%–27%) of all trauma patients admitted to hospitals (Shemer 2004); they are also one of the main causes of death among younger drivers. Israeli law allows a blood alcohol level of 0.05 g/dl (Goldschmidt 2009). Despite the relatively low total amount of alcohol consumed in Israel compared with other developed countries, levels among young populations worldwide are similar (Neumark et al. 2007; Gittelman, Pisahov, Karmel, & Handel 2012).
The MDA, the only Israeli national EMS, has over 10,000 volunteers, 4000 of whom are teenagers aged 15–18 (Littman-Ovadia and Steger 2010; Jaffe and Sasson 2014).These teenage volunteers undergo a 60-h ambulance first responder training, after which they join standard ambulance teams as apprentice. Afterwards, as they progress, they may continue their training in an advanced First Responder course that qualifies them to join the mobile intensive care ambulances. All training is usually undergone by the teenage volunteers during the above-mentioned 3-year period as adolescents. All volunteers are committed to a minimum of one 8-h shift weekly. During their time spent on ambulances, the teenagers witness different types of emergencies such as cardio-cerebral incidents, myocardial infarcts, labor and delivery, mass casualties, natural disasters and MVAs. While doing so, the teen volunteers experience the negative and often fatal consequences of drinking alcohol and driving (Allison et al. 1987; Ellis and Sorene 2008). A study published by MDA found that teenage volunteers tend to suffer more frequently from various levels of PTSD than older volunteers and workers (Jaffe et al. 2012).
Given all the above information, we assumed that students who have witnessed general negative outcomes of DUI, and specifically as MDA adolescent volunteers, would have more negative attitudes and behaviors toward DUI.
Methods
Participants were first-degree paramedic students in the Department of Health Science of the Ben-Gurion University of the Negev. Approval for the research was granted by the faculty’s ethics committee, and approval to use an original questioner was received from the authors. The students were approached during classes with obligatory attendance and were asked to complete an anonymous, self-administered questionnaire that was collected within 20 min.
The questionnaire used was based on the Israeli National Road Safety Authority’s alcohol and drugs questionnaire (Goldveg and Sofer 2013), which was adapted for use in this research after permission was received from the authors. The original questionnaire included a total of 44 questions, both research-related and demographic, while our questionnaire included 40 questions. The demographic questions asked the participants to indicate their age, gender, native language and whether they had volunteered in MDA as adolescents (for a minimum of 6 months). The research questions concerned driving habits (frequency of driving), drinking (frequency of drinking alcohol, place of drinking and preferred alcoholic drinks, for example), DUI habits and opinions (how many DUI events in the past year, driving with others in the car, assumed number of drinks that will still enable driving properly, the time of appointing the designated driver, avoiding driving after drinking too much) and attitudes regarding DUI (law enforcement, advertisements against DUI). All questioners were answered without students’ identification and so were anonymized immediately.
All questions were multiple choice, facilitating a wide variety of responses and covering aspects such as: types of alcohol consumed, places where a person has had a drink and driven, the actions taken when deciding not to DUI and others.
The data were processed using SPSS Statistics 20.
All the students attending classes on the day of the sample (n = 59) responded to the questionnaires, making it a 100% response rate. The respondents’ average age was 23.37 years (SD 2.81; range 18.5–29 years, variance 7.9); 39 were male (66%) and 20 were female (34%); 23.7% of the sample was 20 years old and younger; 81% were 25 years old and younger (see Table 1).
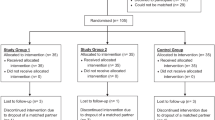
In the second stage of the data processing, the sample was divided into two groups—those who had volunteered at MDA as adolescents (research group; n = 21, 42.9%) and those who had not (review group) (n = 28, 56.1%). Ten students did not respond to that question and therefore were excluded from the analysis. Age (a mean of 23.69 years for the research group and of 23.13 years for the review group) and gender (males: 16 for the research group and 14 for review group; female: 5 and 14, respectively) variables (Table 2). The groups differed demographically only by gender—the research group had significantly more males than females.
Statistical significance was set at 95% (α = 0.05) when using chi-square tests to compare the two groups’ behaviors and attitudes toward DUI.
Results
The first part of the analysis involved processing the sample as a whole to compare the Israeli statistics of alcohol consumption and DUI to those that are found in the US and Europe. In total, we found that 42% of our sample had drunk-driven in the past year. Most students who reported drinking more than once a week (n = 16), and more than 50% of those who drank more frequently than once a month (n = 26), had also driven while intoxicated in the past year (Table 1).
When analyzed by age, the students in the sample did DUI in the past year (χ2 = 74.188, df-48, p < 0.01), while the most common ages were 24–26 years. Males drank more than females and also drove while intoxicated more frequently than females. On the other hand, females’ estimation of their ability to drink (more than one drink) and drive was higher than the males’ (60% and 43%, respectively) (Table 1).
Seventy percent of the students had been designated drivers during the past year, 31% of whom had driven drunk, with men drinking more than women on these occasions (Table 1).
When asked, 80% of the students believed that there is a high risk of MVA for those who engage in DUI (n = 47). Also, 90% of the students had answered that increasing law enforcement has a great effect on decreasing the DUI occurrence (n = 53).
When attitudes were examined and compared with actual behaviors, it was found almost significantly (χ2 = 16.681, p = 0.054) that the students drank the same amounts of alcohol as their estimate when asked how many drinks they think they could drink and still be able to drive—being more than one or between one and two drinks. The same was found for the assumed number of beverages that would allow the driver to drink and still perform safely as a designated driver (χ2 = 12.588, p < 0.05).
No significant difference was found between the research and review group regarding behaviors and attitudes toward DUI (Table 2).
Although not significant statistically, we found that the research group was more likely to drive under the influence and also drink more alcoholic beverages doing so (Table 2).
Overall, the past volunteers (research group) assumed they were better able to drive after drinking a larger number of alcoholic drinks. Hence, past volunteers had a higher estimation of their ability to DUI.
Discussion
The findings above primarily indicate that there is no difference in alcohol consumption and engaging in DUI between our sample, consisting of health-science students, and the general student population researched in other studies, which presented alcohol binge drinking at least once a week to once a month and driving under the influence of alcohol at least once in the past year (Vassallo et al. 2007; Rivara et al. 2007; Jones and Holmgren 2009; Dhami et al. 2011; LaBrie et al. 2011; Moan et al. 2013).
We found that males tend to drink more than females. This finding is similar to that found in the research literature. However, in previous studies, females were found to be affected by smaller amounts of alcohol than males, and their reaction time was also found to be more prolonged (Shinar 2007: Siliquini et al. 2011). We found that females had a slightly higher estimation of their competence to drive intoxicated compared with males (assumed number of drinks that can be consumed and still enable safe DUI). Females had drunk the same amounts as males, contradicting the findings noted in the literature (Dhami and García-Retamero 2012).
Our findings match the existing data in Israel (Israeli National Road Safety Authority 2011). It is a disturbing fact that more than half of the students had drunk-driven at least once in the past year. In this study, we concluded that Israeli students are aware of the DUI problem, with its potential negative effects and outcomes, and that they nevertheless consciously prefer to engage in this activity rather than avoid it (Dhami et al. 2011; Karam et al. 2007; LaBrie et al. 2011).
In their study, LaBrie et al. (2011) stated that students who consume alcohol more frequently are more predisposed to DUI than those who drink less frequently. The results of our study support that claim. However, this study was conducted at a campus located in the center of the city, where most student accommodations and drinking places are within walking distance. Nonetheless, when they go back to their parents’ homes during holidays and sometimes for weekends, they need a vehicle to get to their drinking places. Consequently, this study may not reveal the actual severity of the problem.
We found a positive comprehension of police and law enforcement and the potential decrease in DUI by the students, as was found in other studies in developed countries (Shinar 2007; Liang and Huang 2008; Stanojević et al. 2013).
In Israel, because of the obligatory army service, most of the young adults experience the “away from home college” phase at the ages of 22–23 years, unlike the youth in most other countries, who leave for college at the age of 18 years. This difference impacts the differences in attitudes: at the age of 23 years, the young adults in countries with no obligatory army service begin their adults life and become more responsible (and engage less in DUI and risky behaviors), while in Israel they only enter “collage stage” at this age. This fact can explain the mean age differences of the students. In some cases, youngsters are able to study prior to their military service, at the age of 18, and are known as Atuda’im (“student soldiers”) (Weinstock and Zviling-Beiser 2009). The average age of the students in our research was 23 years, suggesting that probably at least a fifth of them are Atuda’im. This fact allows us to directly compare our results with those obtained in the literature (Liang and Huang 2008; Jones and Holmgren 2009; LaBrie et al. 2011; Shinar 1995).
Young drivers who have had a negative DUI experience in their youth, such as volunteering at MDA, were not affected by it enough to change their DUI patterns. Moreover, our results may also indicate that these young drivers were even more prone to DUI than those who had not been exposed to negative experiences in this area. Past volunteers consumed more alcoholic beverages before sitting behind the wheel and engaged in that behavior more often.
Young drivers who had had a negative DUI experience in their youth (exposure to MVAs as MDA volunteers) were more likely to correctly estimate their ability to drive relative to the amount of alcohol consumed. They also had more negative attitudes toward DUI than those who had no negative drunk-driving experience (Vassallo et al. 2007; Jones and Holmgren 2009; LaBrie et al. 2011). In our study, we found that although the review group estimated their capability to DUI after consuming a greater number of drinks, they had actually drunk less when driving and had abstained more from driving when they felt that they had drunk too much compared to the research group. In research carried out among firefighters and paramedics in the US, it was found that 56% were engaging in binge drinking at least once a month, while almost a tenth of those who had drunk any amount of alcohol in the past month had also driven drunk (Haddock et al. 2012).
Jewell and Hupp (2005) found that different types of interventions aimed at reducing the prevalence of DUI are only successful in the short term and that their effectiveness decreases within 4 weeks of the intervention event. Therefore, we assumed that a similar process occurs after a negative DUI experience, although it may take a longer time to diminish. During the process of literature collection and review writing, we did not find any publications concerning the effects of negative experiences of DUI, such as volunteering in MDA and its parallel organizations around the world, on teenagers’ opinions and attitudes toward DUI. Contrary to our assumption, volunteering in MDA even relatively worsened the DUI behavior of the young adults in our research compared to the non-volunteers, who represented the normal population in the study.
Limitations
We used a convenience sample that may not evenly represent both the total student population and the paramedic students. In addition, the number of responders is relatively small (n = 59), but given the fact that this is a pilot study, it may be adequate. It is of great importance that future research studies a greater number of cases, in a number of countries, if possible.
The reliabilty, sensitivity and validity of the questionnaire employed have not been shown in the current study. We used self-administered questionnaires, which are known to be less credible. However, they were filled out anonymously—a method that is known to improve credibility.
As discussed, the students in this study had lived close to their drinking places, a fact that may mask the actual severity of the problem.
Conclusions and practical implications
Driving under the influence of alcohol has become a great international health care problem, causing an increasing number of morbidity and mortality cases, especially among young adults. A large variety of intervention programs have been attempted aiming to reduce the incidence of this phenomenon. As found in this study, it appears that even paramedic students, who are being trained to treat DUI victims in their first and most critical minutes after injury, are blind and indifferent where their own behaviors and attitudes are concerned. Moreover, paramedic students who had already experienced the possible negative outcomes of alcohol on driving, having witnessed and treated patients after MVAs, are also oblivious in their attitudes toward DUI. Our findings are distressing and may reveal the severity of the social norm on the one hand and the lack of suitable education regarding the dangers of alcohol in the health care department on the other. Other health care students, such as nursing students, may have the same attitudes and behaviors toward DUI. Their quality of interventions and education for patients, as done in the emergency department, for example, may be harmed as a result of this personal conflict. Eventually, this conflicting behavior may encourage their circle of friends, family and even patients to act similarly by choosing to believe that “it won’t happen to them.”
This study is a pilot study that presents disturbing outcomes, revealing the need for further research. Health care staff are expected and encouraged to carry out interventions regarding alcohol consumption and DUI in order to reduce its incidence.
References
Allison EJ, Whitley TW, Revicki DA, Landis SS (1987) Specific occupational satisfaction and stresses that differentiate paid and volunteer EMTs. Ann Emerg med 16:676–679
BRAVO Volunteer Ambulance Services (n.d). http://www.bravoambulance.org/index.php/history. Accessed 20 May 2014
Bryant RA, Harvey AG (1996) Posttraumatic stress reactions in volunteer firefighters. J Trauma Stress 9:51–62
Cartwright J, Asbridge M (2011) Passengers’ decisions to ride with a driver under the influence of either alcohol or cannabis. J Stud Alcohol Drugs 72:86–95
Chappaqua Volunteer Ambulance Youth Corps (n. d). http://www.chappaquaambulance.org/content/participate-youth-corps-member. Accessed 20 May 2014
DeMartini KS, Carey KB, Lao K, Luciano M (2011) Injunctive norms for alcohol-related consequences and protective behavioral strategies: effects of gender and year in school. Addict Behav 36:347–353. doi:10.1016/j.addbeh.2010.12.009
Dhami MK, García-Retamero R (2012) Spanish young adults’ perceptions of the costs and benefits of risky driving behaviors. Span J Psychol 15:638–647
Dhami MK, Mandel DR, Garcia-Retamero R (2011) Canadian and Spanish youths’ risk perceptions of drinking and driving, and riding with a drunk driver. Int J Psychol 46:81–90. doi:10.1080/00207594.2010.526121
Domingues SCA, Mendonça JB, Laranjeira R, Nakamura-Palacios EM (2009) Drinking and driving: a decrease in executive frontal functions in young drivers with high blood alcohol concentration. Alcohol 43:657–664. doi:10.1016/j.alcohol.2009.10.001
Donnelly E (2012) Work-related stress and posttraumatic stress in emergency medical services. Prehospital Emerg Care 16:76–85. doi:10.3109/10903127.2011.621044
Ellis DY, Sorene E (2008) Magen David Adom--the EMS in Israel. Resuscitation 76:5–10. doi:10.1016/j.resuscitation.2007.07.014
Engström I, Gregersen NP, Granström K, Nyberg A (2008) Young drivers—reduced crash risk with passengers in the vehicle. Accid Anal Prev 40:341–348. doi:10.1016/j.aap.2007.07.001
Fillmore MT, Blackburn JS, Harrison ELR (2008) Acute disinhibiting effects of alcohol as a factor in risky driving behavior. Drug Alcohol Depend 95:97–106. doi:10.1016/j.drugalcdep.2007.12.018
Gittelman, V., Pisahov, P., Karmel, R., & Handel M (2012) Driving Under the Influence of Alcohol: National Observation Review 2011. In: Ran Naor Cent. Traffic Saf. Res. http://tri.technion.ac.il/files/2016/08/%D7%A0%D7%94%D7%99%D7%92%D7%94-%D7%AA%D7%97%D7%AA-%D7%94%D7%A9%D7%A4%D7%A2%D7%AA-%D7%90%D7%9C%D7%9B%D7%95%D7%94%D7%95%D7%9C-%D7%A1%D7%A7%D7%A8-%D7%AA%D7%A6%D7%A4%D7%99%D7%95%D7%AA-%D7%90%D7%A8%D7%A6%D7%99-2011.pdf
Goldschmidt R (2009) Alcohol Tests to Drivers, comparative review. In: Ha-kneset, Res. Inf. Cent. http://www.knesset.gov.il/mmm/data/pdf/m02202.pdf.
Goldveg R, Sofer S (2013) Driving Under the Influence-2012 (Hebrew). http://www.rsa.gov.il/meidamechkar/MechkarimSkarim/documents/alkohol2012.pdf
Haddock CK, Jahnke SA, Poston WSC, Jitnarin N, Kaipust CM, Tuley B, Hyder ML (2012) Alcohol use among firefighters in the Central United States. Occup med (Chic ill) 62:661–664. doi:10.1093/occmed/kqs162
Israeli National Road Safety Authority (2011) Trends in traffic safety 2001–2010. (Hebrew)
Jaffe E, Sasson U (2014) First generation immigrant adolescents’ motives to volunteer. Mod Manag Sci Eng 2:p10
Jaffe E, Sasson U, Knobler H, Aviel E, Goldberg A (2012) Volunteers and the risk of posttraumatic stress disorder. Nonprofit Management and Leadership 22:367–377. doi:10.1002/nml.20059
Jewell J, Hupp SDA (2005) Examining the effects of fatal vision goggles on changing attitudes and behaviors related to drinking and driving. J Prim Prev 26:553–565
Jones AW, Holmgren A (2009) Age and gender differences in blood-alcohol concentration in apprehended drivers in relation to the amounts of alcohol consumed. Forensic Sci Int 188:40–45. doi:10.1016/j.forsciint.2009.03.010
Karam E, Kypri K, Salamoun M (2007) Alcohol use among college students: an international perspective. Curr Opin Psychiatry 20:213–221. doi:10.1097/YCO.0b013e3280fa836c
Kenney SR, LaBrie JW, Lac A (2013) Injunctive peer misperceptions and the mediation of self-approval on risk for driving after drinking among college students. J Health Commun 18:459–477. doi:10.1080/10810730.2012.727963
LaBrie JW, Kenney SR, Mirza T, Lac A (2011) Identifying factors that increase the likelihood of driving after drinking among college students. Accid Anal Prev 43:1371–1377. doi:10.1016/j.aap.2011.02.011
Liang L, Huang J (2008) Go out or stay in? The effects of zero tolerance laws on alcohol use and drinking and driving patterns among college students. Health Econ 17:1261–1275. doi:10.1002/hec.1321
Littman-Ovadia H, Steger M (2010) Character strengths and well-being among volunteers and employees: toward an integrative model. J Posit Psychol 5:419–430. doi:10.1080/17439760.2010.516765
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, AlMazroa MA, Alvarado M, Anderson HR, Anderson LM, Andrews KJ, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, Courville de Vaccaro K, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FJR, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Memish ZA, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Venkat Narayan KM, Nasseri K, Norman P, O'Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Panozo Rivero A, Perez Padilla R, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA III, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, Rodriguez De León F, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJL (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet 380:2095–2128. doi:10.1016/S0140-6736(12)61728-0
Moan IS, Ph D, Norström T, Storvoll EE (2013) Alcohol use and drunk driving: the modifying effect of impulsivity. 114–119.
Neumark YD, Lopez-Quintero C, Grinshpoon A, Levinson D (2007) Alcohol drinking patterns and prevalence of alcohol-abuse and dependence in the Israel national health survey. Isr J Psychiatry Relat Sci 44:126–135
New City Volunteer Ambulance Youth Corps (n.d). http://www.newcityems.org/youthcorps/. Accessed 20 May 2014
Peden M, World Health Organisation (2004) World Report on Road Traffic Injury Prevention http://apps.who.int/iris/bitstream/10665/42871/1/9241562609.pdf
Rivara FP, Relyea-Chew A, Wang J, Riley S, Boisvert D, Gomez T (2007) Drinking behaviors in young adults: the potential role of designated driver and safe ride home programs. Inj Prev 13:168–172. doi:10.1136/ip.2006.015032
Saint John Ambulance (n.d). http://www.sja.org.uk/sja/young-people/cadets.aspx. Accessed 20 May 2014
Shemer J (2004) Traffic accidents—the national killer. Harefuah 143:90–91 168
Shinar D (2007) Traffic safety and human behavior. Elsevier, Oxford, UK
Shinar D (1995) Drinking and driving of pub patrons in Israel. Accid Anal Prev 27:65–71
Siliquini R, Bert F, Alonso F, Berchialla P, Colombo A, Druart A, Kedzia M, Siliquini V, Vankov D, Villerusa A, Manzoli L, TEN-D Group (TEN-D by Night Group) (2011) Correlation between driving-related skill and alcohol use in young-adults from six European countries: the TEN-D by night project. BMC Public Health 11:526. doi:10.1186/1471-2458-11-526
Sowell ER, Thompson PM, Holmes CJ, Jernigan TL, Toga AW (1999) In Vivo Evidence for Post-Adolescent Brain Maturation in Frontal and Striatal Regions 2:859–861
Stanojević P, Jovanović D, Lajunen T (2013) Influence of traffic enforcement on the attitudes and behavior of drivers. Accid Anal Prev 52:29–38. doi:10.1016/j.aap.2012.12.019
United States Department of Transportation (2013). Sober Driving During the Holidays. National Highway traffic safety administration https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0CB4QFjAA&url=http://www.nhtsa.gov/staticfiles/numbers/Safety_In_Numbers_Drive_Sober_811871.pdf&ei=jLN1VMzEIauygPA2YD4Dg&usg=AFQjCNHWX8IztHyCm4vwP3IiQZOELzHmwQ&.
Vassallo S, Smart D, Sanson A, Harrison W, Harris A, Cockfield S, McIntyre A (2007) Risky driving among young Australian drivers: trends, precursors and correlates. Accid Anal Prev 39:444–458. doi:10.1016/j.aap.2006.04.011
Wagner D, Heinrichs M, Ehlert U (1998) Prevalence of symptoms of posttraumatic stress disorder in German professional firefighters. Am J Psychiatry 155:1727–1732. doi:10.1176/ajp.155.12.1727
Weinstock M, Zviling-Beiser H (2009) Separating academic and social experience as potential factors in epistemological development. Learn Instr 19:287–298. doi:10.1016/j.learninstruc.2008.05.004
World Health Organization (2013) Global status report on road safety 2013: supporting a decade of action. http://www.who.int/violence_injury_prevention/road_safety_status/2013/report/en/
Acknowledgment
We acknowledge the assistance of Dr. Adi Ronen from the Faculty of Engineering Sciences in Ben-Gurion University of the Negev, who passed away prematurely during the writing of this article. His research focused on the influence of various substances on physiological performance and subjective feeling on task performing. Dr. Ronen will be greatly missed by his colleagues, students and friends.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study. The questionnaires were given to the students following an explanation. Responding to the questionnaire was considered consent to participate.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Additional information
* Magen David Adom (MDA), the Israeli national Emergency Medical Service
Rights and permissions
About this article

Cite this article
Domrev-Benkovich, A., Ronen, A. & Grinstein-Cohen, O. Does experience change anything? Attitudes of paramedic students regarding drinking and driving. J Public Health 25, 465–472 (2017). https://doi.org/10.1007/s10389-017-0814-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-017-0814-3