
Abstract
Purpose
To determine factors significantly correlated with the failure of macular reattachment by pars plana vitrectomy (PPV) without laser photocoagulation of the optic disc margin to treat optic disc pit (ODP) maculopathy.
Design
Retrospective, interventional case series.
Methods
We reviewed the medical records of 35 consecutive patients with ODP maculopathy who underwent PPV without laser photocoagulation. PPV with the creation of a posterior vitreous detachment (PVD) was performed in 34 eyes. An epiretinal membrane and internal limiting membrane present in the other eye with a PVD were removed. Patients were followed for 12–193 months (mean 58 months) after surgery. The main outcome measures were the postoperative rate of retinal reattachment and best-corrected visual acuity. The preoperative clinical characteristics of the successful cases were compared to those of the unsuccessful cases.
Results
A complete retinal reattachment was attained in 31 of 35 eyes and it required about one year. The 4 other eyes that did not achieve a macular reattachment after the primary PPV underwent additional therapies. The factors that were significantly associated with a failure of a retinal reattachment after primary PPV were the presence of a retinal detachment connected to the optic disc (P < 0.001) and the presence of preoperative headaches (P = 0.030).
Conclusions
Clinicians should be aware that the presence of a preoperative macular detachment connected to the optic disc margin and preoperative headaches are indicators for an unsuccessful outcome of PPV without laser photocoagulation in eyes with ODP maculopathy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A congenital optic disc pit (ODP) is an abnormality of the optic nerve head and usually appears as a grayish or black circular depression on the optic disc [1,2,3]. ODPs are commonly found at the inferotemporal region of the optic disc [1,2,3]. Histological studies show a focal defect in the peripapillary sclera and lamina cribrosa with a herniation of poorly differentiated retinal tissue alongside the optic nerve [4, 5]. The tissue adjoins the subarachnoid space with vitreous herniating posteriorly through the area where the lamina cribrosa is absent [4, 5].
Although patients with ODPs are usually asymptomatic, visual disturbances can occur due to ODP maculopathy manifested as retinoschisis or macular detachment [2,3,4,5,6,7]. Optical coherence tomographic (OCT) images show that fluid from the ODP can pass into the retina and create multiple intraretinal spaces, retinoschisis, connected to the ODP [7,8,9]. A detachment of the outer layers of the retina occurs later as a secondary phenomenon in most eyes with ODP maculopathy [6]. A spontaneous resolution of retinoschisis or macular detachment with improvement in vision is reported [10, 11]. However, the majority of ODP maculopathy cases have a poor prognosis with a gradual worsening and a final visual acuity (VA) of 20/200 or + worse [3].
A large number of treatments has been used to treat eyes with ODP including laser photocoagulation [12,13,14], gas tamponade [15, 16], macular buckling surgery [17], and pars plana vitrectomy (PPV) [18,19,20,21,22,23,24,25,26,27]. However, none has been established as the optimal treatment. The predominant treatment of ODP maculopathy has been PPV combined with laser photocoagulation at the optic disc margin. In addition, some authors report that the creation of a PVD without laser treatment was effective in reattaching the retina [19, 21, 23, 25]. However, there were still some cases in which a retinal reattachment could not be achieved by PPV without laser treatment. Although other surgical adjuvant procedures including the stuffing of the ODP with a rolled ILM-flap have been proposed for better results [26, 27], we have to differentiate between cases of ODP maculopathy refractory to PPV with/without laser treatment to determine the additional surgical techniques needed to prevent possible further complications. It is important to determine the preoperative factors present in the unsuccessful eyes to allow clinicians to adjust their surgical techniques for the primary treatment of eyes with ODP maculopathy.
The purpose of this study was to determine the factors significantly correlated with failure of PPV without laser photocoagulation at the optic disc margin to enable surgeons to reattach the retina in eyes with ODP maculopathy.
Subjects and methods
This was a retrospective study of 35 eyes of 35 consecutive patients with ODP maculopathy treated at the Kyorin Eye Center between 1994 and 2019. All patients received a detailed explanation of the surgical and ophthalmic examination procedures, and all signed an informed consent form. The procedures used in this study conformed to the tenets of the Declaration of Helsinki, and the protocol of this study was approved by the Institutional Review Committee of Kyorin University School of Medicine. All of the eyes underwent primary PPV without laser photocoagulation for the treatment of ODP maculopathy. The clinical data from 17 of these ODP patients published with a different emphasis by the authors are included [19, 21]. The exclusion criteria included a prior PPV and other causes of retinoschisis or macular detachment including glaucoma and myopic traction maculopathy. Patients with < 12 months of postoperative follow-up were also excluded.
The decimal best-corrected visual acuity (BCVA) was recorded and converted to the logarithm of the minimum angle of resolution (logMAR) units for statistical analyses. Indirect fundus ophthalmoscopy and slit-lamp biomicroscopy with a 90-diopter non-contact lens were performed before and after surgery. The OCT images of the eyes were obtained with the Stratus OCT™ device (Carl Zeiss Meditec, Inc), OCT 4000 CirrusⓇ (Carl Zeiss Meditec, Inc.), SpectralisⓇ (Heidelberg Engineering), or swept-source OCT (SS-OCT; DRI OCT-1 AtlantisⓇ, TOPCON Corporation). Longitudinal OCT images parallel to and cross sections vertical to the optic disc pit and margin of the retinal detachment (RD) and retinoschisis were used to evaluate the retinal architectural before and after surgery. The size of the ODP was presented as the ratio of the vertical diameter of the ODP to the vertical diameter of the optic disc in the fundus photographs.
The preoperative clinical characteristics of the 35 patients with ODP maculopathy are shown in Table 1. The men/women ratio was 18/17, and the mean age at the time of surgery was 29.6 ± 13.9 years with a range of 8–56 years. One of the affected eyes with ODP maculopathy was highly myopic at – 12.0 diopters (D; Patient 20), but the others did not have severe refractive errors. The preoperative decimal BCVA was 0.28 ± 0.45 (mean ± standard deviation; 0.55 ± 0.35 logMAR units) with a range of 0.07–1.0. All patients complained of a worsening vision, a central scotoma, or metamorphopsia in the affected eye for several months prior to surgery. Eight patients (22.9%) had recurrent headaches and/or deep ocular pain in the affected eye. The pain usually developed at the time when the vision began to decrease, and required medication to ease the pain. Patient 6 had been treated for the ODP maculopathy with laser photocoagulation to the edge of the ODP, but none of the other patients had received any prior treatment. The presence of both retinoschisis and macular detachment was confirmed in the preoperative OCT images in 27 of 35 eyes (77.1%). Six eyes (17.1%) had only retinoschisis and 2 eyes (5.7%) had only macular detachment. Seven eyes had a RD connected to the optic disc margin (20.0%), and a PVD was not present preoperatively in 34 eyes. The presence or absence of a PVD was evaluated by preoperative fundus examinations and confirmed intraoperatively. The remaining eye (Patient 34) had a glial ring of PVD with an ERM at the posterior pole. Vitreomacular traction was not observed in any eyes preoperatively either by ophthalmoscopyor OCT imaging.
PPV was performed on all patients with ODP maculopathy who had a worsening of the BCVA associated with a progression of the retinoschisis and/or macular detachment as confirmed by the OCT images. Surgery was performed by two surgeons (AH or MI) between 1994 and 2019, and the patients were followed postoperatively for 12–193 months with a mean of 58 months. PPV was performed with the intention of releasing the vitreous traction at the ODP. Twenty-gauge (20G) vitrectomy was performed in the first 15 eyes, 25G vitrectomy in 14 eyes, and 27G vitrectomy in 6 eyes. Thirty-four eyes had no PVD before the surgery and one eye (Patient 34) had a PVD with an epiretinal membrane (ERM) on the macula. A PVD was created by suction over the optic disc or near the area of the retinoschisis with a vitreous cutter or microhooked needle in all 34 eyes. To limit the damage to the retina in the area of the ODP maculopathy by the surgical manipulations, special attention was given to separating the posterior hyaloid membrane carefully over the area of the retinoschisis, macular detachment, and ODP. Triamcinolone acetonide was used intraoperatively to make the posterior cortical vitreous more visible [28]. Brilliant blue G (BBG) staining was used to determine the status of the internal limiting membrane (ILM) [29], i.e., whether it was separated from the retina preoperatively or intraoperatively. The ILM was removed after creating the PVD in 2 eyes (Patients 19 and 21), because the ILM was preoperatively separated from the surface of retina in the OCT images. The ERM and ILM were removed in an eye with a PVD that was present before the PPV (Patient 34). Twenty percent sulfur hexafluoride (SF6) gas was used to tamponade the retina in the first 12 eyes, and air tamponade was used in two eyes that had a high elevation of the macular detachment (Patient 26) or a complication of a peripheral retinal break that occurred during the PPV (Patient 34). Laser photocoagulation at the margin of the optic disc was not performed during the primary procedure in any of the eyes. Combined cataract surgery and intraocular lens (IOL) implantation with PPV were performed in two patients (Patients 16 and 34).
One patient reported severe headaches disappearing immediately after the PPV. Since then, we started to question all patients about episodes of headaches during the follow-up period for the ODP maculopathy. While it was difficult to evaluate the headaches quantitatively, the presence of headaches was defined as headaches that required oral medications.
Success was defined as a complete resolution of the subretinal fluid (SRF) and marked reduction of macular retinoschisis in the OCT images postoperatively. The clinical characteristics of the successful cases including those detected by OCT images were compared to those of the unsuccessful cases after primary PPV without laser application. The significance of the correlations between the preoperative factors and the success of the PPV was determined.
Statistical analyses
Continuous variables are expressed as the means ± standard deviations. The Mann–Whitney U tests and Wilcoxon rank sum tests were used for the nonparametrically distributed data. Categorical variables are expressed as percentages, and group differences were analyzed using Fisher’s exact probability tests. The significance of the correlations between categorical variables was determined by Spearman’s correlation coefficient by rank test. The data were analyzed with the IBM-SPSS software version 23 (IBM-SPSS). A P-value of < 0.05 was considered statistically significant.
Results
Anatomic results of pars plana vitrectomy (PPV)
A complete retinal reattachment was achieved after the primary PPV in 31 of 35 eyes (88.6%) although nearly 1 year (mean; 12.9 months) was required to attain this state in some of the eyes (Table 2). The postoperative OCT images showed that a sharp contour of the retinal elevation adjacent to the optic disc and inner retinoschisis separation were reduced at the early phase after the PPV. However, outer retinoschisis improved slowly in most eyes (Fig. 1). The macular detachment decreased gradually with a complete absorption of the SRF after 8 to 19 months (average, 13 months). The outer segments of the photoreceptors began to thicken and rearrange into a regular alignment even with a persistent macular detachment after the PPV. A limited defect of the outer segments of the photoreceptors and the ellipsoid zone remained even after a complete retinal reattachment. The degree of excavation of the ODPs was not always obvious preoperatively, but when the retina was reattached, the pits were easily observed as being darker and deeper than the surrounding areas (Fig. 1).

Clinical findings of Patient 22 with optic disc pit (ODP) maculopathy. A Preoperative fundus photograph of the right eye showing a temporal ODP associated with a large oval shaped macular elevation (black arrows) with cystic fovea. The ODP has blurred margins at the temporal edge. The preoperative decimal best-corrected visual acuity (BCVA) was 0.07. b Preoperative optical coherence tomographic (OCT) image showing a multilayer retinoschisis connected to the ODP. A sharp elevation of the neural retina is present at the margin of the ODP. A retinal detachment is present around the fovea. c OCT image shows a decrease in the separation of the retinoschisis 3 months after pars plana vitrectomy (PPV) with the creation of a posterior vitreous detachment (PVD). The decimal BCVA has improved to 0.1. d OCT image showing that the retinoschisis and foveal detachment are decreased 10 months after the PPV. The outer segments of the photoreceptors are thickened and arranged regularly within the subfoveal lesions. The decimal BCVA was 0.2. e and f Fundus photograph and OCT image at 24 months postoperatively showing a complete reattachment with the margin of the ODP appearing clearer (e). A limited defect of the ellipsoid zone remained after the complete retinal reattachment (f). The decimal BCVA was 0.5
The effects of a gas tamponade during vitrectomy for retinal reattachment was also evaluated. The rate of retinal reattachment of the cases with SF6 gas tamponade during vitrectomy (10 of 10 cases, 100%) was not significantly different from that of the cases without gas tamponade (19 of 23 cases, 82.6%, P = 0.22, Fisher's exact probability test). One eye developed a macular hole (MH) (Patient 12) at 3 months following the primary vitrectomy, and one eye (Patient 2) developed retinal atrophy as a complication. The findings in two eyes were excluded from the statistical analyses. The differences in the intervals until complete reattachment between the eyes with and without gas tamponade were not significant (P = 0.17, Mann–Whitney U test). The surgical manipulation of the ILM peeling (Patients 19, 21, and 34) did not shorten the duration reaching a complete retinal reattachment. One eye (Patient 12) developed a MH at 3 months after the PPV during the reduction of the retinoschisis; this patient required a second vitrectomy with ILM peeling and gas tamponade. The MH was closed with complete retinal reattachment after the absorption of the gas and the BCVA improved with time.
Four patients (11.4%) did not have a complete retinal reattachment after the primary PPV (Patients 17, 20, 23, and 24). The initial gradual reduction in the height of the RD was observed for several months after the PPV in all 4 eyes. However, the rate of reduction of the elevated macular detachment was moderate with more than 6 months without visual improvement or a worsening of vision. Then, we decided to perform the reoperation as described below.
Patient 17 required 3 additional treatments including gas tamponade, PPV with ILM peeling, and laser photocoagulation at the edge of the ODP for a complete retinal reattachment. The highly myopic eye of Patient 20 had visual disturbances for more than 2 years. This patient had severe headaches that had developed at the time of the worsening of vision. OCT images showed a high elevation RD connected to the optic disc without retinoschisis and a decimal BCVA of 0.2. After the PPV, the RD began to decrease but did not attain a complete retinal reattachment for more than 2 years. She moved to the USA and received surgery with a revision of the ILM peeling and perfluoropropane (C3F8) gas tamponade without laser treatment at 3 years after the initial PPV. The retina reattached completely after the gas resorption and vision was 0.1. The other 2 eyes with failed retinal reattachment after the primary PPV (Patients 23, 24) developed an unusual bullous RD during the course of the additional treatments (Figs. 2, 3). The preoperative OCT images showed that the RD was connected to the optic disc in both eyes. Preoperatively, Patient 24 had recurrent headaches which completely disappeared after the primary PPV. Patient 23 had severe headaches during the course of the additional treatments. The RD completely reattached after several additional treatments including ILM peeling, laser photocoagulation at the edge of the optic disc, and gas tamponade.

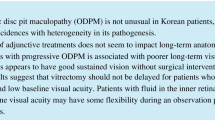
Clinical findings from Patient 23 with an optic disc pit (ODP) and macular detachment that was unsuccessfully treated. This 17-year-old young woman complained of reduced vision in her right eye of 3 months duration. a Fundus photograph of the right eye at the initial visit shows a temporal ODP associated with a round-shaped area of retinal elevation from the optic disc (black arrows). The preoperative decimal BCVA was 0.07. b Optical coherence tomographic (OCT) image at the initial visit shows a deep excavation with two horizontal septa in the ODP and retinal detachment connected to the optic disc. The outer retinal layer is slightly separated. Vitreous fibers can be seen attached to the septa in the pit. c OCT image at 15 months after the pars plana vitrectomy (PPV) with the creation of a PVD shows a decrease of the retinal detachment (RD). The decimal BCVA was slightly improved to 0.2. d About 2 years after the PPV, the subretinal fluid (SRF) is still present. A second PPV with 20% sulfur hexafluoride gas tamponade was performed. However, one month later, a bullous total RD developed with recurrent severe headaches. We performed a 3rd PPV with encircling scleral buckling to reduce the peripheral vitreous traction, SRF drainage, laser photocoagulation at the optic disc margin, and a gas tamponade. e The retinal elevation is markedly decreased but persisted around the macula. Additional laser photocoagulations were added twice at the optic disc margin. f and g Two years later, the RD has resolved, and the retina has remained attached for more than 2 years. The decimal BCVA was 0.1

Clinical findings of a 24-year-old man with a 5-month history of reduced vision in his left eye (Patient 24, unsuccessful case). He reported that he had recurrent headaches which developed at the time his vision began to decrease. a Preoperative fundus photograph of the left eye shows a temporal optic disc pit (ODP) associated with a round-shaped macular detachment (black arrow). The preoperative decimal BCVA was 0.6. b Preoperative optical coherence tomographic (OCT) image shows a deep ODP with a retinal detachment (RD) connected to the cavity of the ODP without retinoschisis (yellow arrow). Pars plana vitrectomy (PPV) with creation of a PVD was performed. However, the RD did not change remarkably for more than one year and the decimal BCVA decreased to 0.2. c and d At 15 months after the PPV, a bullous RD (black arrows) developed (white arrow shows the inverted image of retina) and connected to the ODP cavity (yellow arrows). We performed a 2nd PPV with internal limiting membrane peeling at the posterior pole, drained the subretinal fluid (SRF) through an intentional retinal break. Then 20% sulfur hexafluoride gas was used to tamponade the retina. However, the RD recurred after the resorption of the gas tamponade. Then, a 3rd PPV was performed with SRF drainage, laser photocoagulation at the temporal optic disc margin, and silicone oil tamponade. e and f The retina was reattached with the silicone oil tamponade. Four months later, the silicone oil was removed, and the retina remained attached for more than 5 years after the last PPV. The decimal BCVA reduced to 0.2
One patient had a recurrence of the RD after retinal reattachment obtained by the primary PPV (Patient 18). At 5 years after the initial surgery, he suffered a blunt ocular trauma to the affected eye during a soccer game. The OCT images at the regular follow-up examination showed a slight elevation of the macula connected to optic disc margin. The patient was followed without additional treatment. The RD decreased gradually over 3 years without a change in the BCVA.
Risk factors for unsuccessful reattachment
Comparisons of the preoperative characteristics of the successfully reattached group to that of the unsuccessful reattached group after the primary PPV without laser treatment are shown in Table 3. The age, preoperative BCVA, and size of the ODP were not significantly different between the two group (P = 0.78, 0.76, 0.63, respectively, Mann–Whitney U test). A connection of the RD to the optic disc in the OCT images was observed in all 4 unsuccessfully reattached eyes and in 3 of 31 successfully reattached eyes (100.0% vs 9.7%, P < 0.001; Fisher’s exact probability test). The factors that were significantly correlated with the connection of the RD to the optic disc could not be identified by multivariate analysis. The RD of Patient 25 with the connection of the RD to the optic disc was successfully reattached after the PPV but required 19 months until a complete reattachment was achieved. This was the longest duration in this series.
Preoperative headaches were present in 3 of 4 eyes in the unsuccessful group and 5 of 31 eyes in the successful group (75.0% vs 16.1%; P = 0.030, Fisher’s exact probability test). Five of 8 eyes with preoperative headaches had RD connected to the optic disc (63%, correlation coefficient = 0.75, P < 0.001, Spearman’s correlation coefficient by rank test). These preoperative headaches disappeared after the primary PPV in all patients with or without a retinal reattachment. The other unsuccessful eye without preoperative headaches had severe transient headaches during the additional postoperative treatments.
Best-corrected visual acuity (BCVA)
The BCVA continued to improve after the primary PPV in most of the successful eyes in spite of the presence of some residual retinoschisis and macular detachment (Tables 1 and 2). The improvement coincided with a better appearance of the photoreceptor outer segments in the OCT images (Fig. 1). The mean final decimal BCVA was 0.69 ± 0.44 (0.16 ± 0.36 logMAR units). A preoperative decimal BCVA of 0.5 or better was present in 10 of 35 eyes (28.6%) and 0.7 or better in 4 eyes (11.4%). Postoperatively, a decimal BCVA of 0.5 or better was found in 31 of 35 eyes (88.6%) and 24 eyes (68.6%). The final decimal BCVA in 31 successfully reattached eyes was 0.82 ± 0.51 (0.09 ± 0.29 logMAR units) better than that in the 4 unsuccessful reattached eyes with a decimal BCVA (0.18 ± 0.52 (0.75 ± 0.29 logMAR units), P = 0.003, Mann–Whitney U test). The final BCVA in the successfully reattached eyes was significantly better than the preoperative BCVA (decimal BCVA: 0.28 ± 0.46 (0.55 ± 0.33 logMAR units), P < 0.001, Wilcoxon rank sum test). The final BCVA in 4 unsuccessful reattached eyes was not significantly different from the preoperative BCVA (decimal BCVA: 0.30 ± 0.36 (0.52 ± 0.45 logMAR units), P = 0.14, Wilcoxon rank sum test).
Complications
The intraoperative and postoperative complications are shown in Table 2. An inferior-temporal visual field defect due to the gas tamponade in Patient 1 and retinal damage by fluorescein dye-assisted PVD in Patient 2 have already been reported [19]. Patient 12 developed a macular hole with a complete retinal reattachment at 3 months after the PPV, that required additional surgery. Patient 3 and 34 developed an iatrogenic peripheral retinal break during the creation of the PVD that was treated successfully with laser photocoagulation. Patient 18 had a recurrence of the macular detachment 5 years postoperatively due to an ocular trauma. A cataract developed and was treated successfully with cataract phacoemulsification and IOL implantation in Patients 7, 14, 19, and 25.
Discussion
Our results show that PPV without laser treatment for ODP maculopathy led to a retinal reattachment in 88.6% of the patients although about 1 year was necessary until complete reattachment in some of these eyes. In addition, the postoperative BCVA was excellent compared to other reports [22,23,24, 30]. However, 4 eyes did not achieve a retinal reattachment after the primary PPV, and 3 of the 4 eyes required multiple treatments until the retina was finally reattached. The final BCVA was not significantly better than the preoperative BCVA in the unsuccessfully reattached eyes.
The results also identified the factors significantly associated with the unsuccessful reattachment after the primary PPV without laser photocoagulation. The eyes with the RD connected to the edge of optic disc and/or in patients with preoperative headaches were significantly correlated with the unsuccessfully reattached retinas.
Although in most eyes with ODP the subretinal fluid originates from the retinoschisis space, the eyes with a RD connected to the edge of optic disc had a direct pathway for the fluid to pass from the ODP cavity into the subretinal space. In these cases, there was a pathway for the movement of fluid from the ODP to the subretinal space through the opening at the edge of the optic disc. Thus, even after the vitreous traction was removed from the ODP rim, a small amount of fluid still had easy access to the subretinal space. The pressure gradients that develop between the intraocular and extraocular spaces can play a role in the pathogenesis of maculopathy associated with congenital disc anomalies [14, 30]. Thus, changes in the intraocular and extraocular pressure even after the PPV might have caused turbulent flow around the deeply excavated ODP lesion to cause the formation of the bullous RD through the opening between ODP and subretinal space in our 2 cases. Similar bullous RDs have been reported in eyes with the morning glory syndrome [31] or as a complication following radial optic neurotomy for the treatment of central retinal vein occlusion [32].
Rayat et al. report that 9 of 10 eyes that underwent repeat surgery had evidence of a direct communication between the subfoveal space and the ODP [33]. The longest duration of retinal reattachment after primary PPV in our cohort was 19 months in one eye (Patient 25) which also had the RD connected to the optic disc. In addition, one eye with recurrence of the ODP maculopathy had a RD connected to the edge of the optic disc. These findings suggest that the retinal adhesion to the retinal pigment epithelium at the margin of the disc might not be strong even after the retinal reattachment by PPV without laser photocoagulation (Table 3).
The preoperative headaches were one factor significantly correlated with unsuccessful reattachments. Five of 8 eyes associated with headaches had RD connected to the disc. If the headaches were due to the acute changes in the intracranial pressure, the direct communication between the subretinal space and subarachnoid space might contribute to the dynamic fluid flow around the ODP during the development of RD faster or be more severe. Headaches associated with optic disc anomalies are reported in a case of total RD associated with the morning glory syndrome, and the eye was treated by surgical removal of a window of dura from the optic nerve sheath [31]. In all 8 of our cases with preoperative headache, the headaches disappeared after the initial PPV. The release of the vitreous traction may have reduced the entrance space for the dynamic flow.
In the four unsuccessfully reattached eyes, several treatments were required before the retina was finally reattached. The development of the laser photocoagulation scar at the edge of the optic disc was probably the main contributor to the final reattachment in 3 of the 4 eyes. Our findings indicated that laser treatment and gas tamponade following the PPV with the creation of a PVD were appropriate treatments for eyes that had direct communication between the ODP space and subretinal space. These procedures led to a closure of the pathway for fluid seepage. On the other hand, for the initial treatment of eyes without these risk factors, it would be better to combine a less invasive method together with a creation of a PVD without laser treatment. Ooto et al. report good surgical outcomes by vitrectomy with inner retinal fenestration without laser treatment [24]. There are reports that ODPs can be successfully treated by stuffing the ODPs with rolled ILM flaps, scleral tissue, and other available tissues [26, 27, 34,35,36]. These methods may be useful for eyes with preoperative factors that are found to be significantly correlated with an unsuccessful reattachment as refractory or complicated cases.
Our study has several limitations including its retrospective nature, a lack of controls, and not being a multicenter study. However, this is the first report to show the factors significantly correlated with the failure of PPV without laser treatment.
In conclusion, the results indicate that PPV without laser treatment for ODP maculopathy led to a retinal reattachment in 88.6% of the patients although about 1 year was necessary until complete reattachment in some of the eyes. In addition, the postoperative BCVA was excellent compared to other reports. Three of the 4 eyes that did not have a retinal reattachment after the primary PPV required multiple treatments until the retina was finally reattached. The presence of a retinal detachment connected to the optic disc and/or preoperative headaches were indications for an unsuccessful reattachment after the primary PPV without laser treatment.
References
Kranenburg EW. Crater-like holes in the optic disc and central serous retinopathy. Arch Ophthalmol. 1960;64:912–24.
Brown GC, Shields JA, Goldberg RE. Congenital pits of the nerve head: II. Clin Stud Hum Ophthalmol. 1980;87:51–65.
Sobol WM, Blodi CF, Folk JC, Weingeist TA. Long-term visual outcome in patients with optic nerve pit and serous retinal detachment of the macula. Ophthalmology. 1990;97:1539–42.
Ferry AP. Macular detachment associated with congenital pit of the optic nerve head. Pathologic findings in two cases simulating malignant melanoma of the choroid. Arch Ophthalmol. 1963;70:346–57.
Irvine AR, Crawford JB, Sullivan JH. The pathogenesis of retinal detachment with morning glory disc and optic pit. Retina. 1986;6:146–50.
Lincoff H, Lopez R, Kreissig I, Yannuzzi L, Cox M, Burton T. Retinoschisis associated with optic nerve pits. Arch Ophthalmol. 1988;106:61–7.
Rutledge BK, Puliafito CA, Duker JS, Hee MR, Cox MS. Optical coherence tomography of macular lesions associated with optic nerve head pits. Ophthalmology. 1996;103:1047–53.
Imamura Y, Zweifel SA, Fujiwara T, Freund KB, Spaide RF. High-resolution optical coherence tomography findings in optic pit maculopathy. Retina. 2010;30:1104–12.
Hirakata A, Hida T, Ogasawara A, Iizuka N. Multilayered retinoschisis associated with optic disc pit. Jpn J Ophthalmol. 2005;49:414–6.
Bonnet M. Serous macular detachment associated with optic nerve pits. Graefes Arch Clin Exp Ophthalmol. 1991;229:526–32.
Polunina AA, Todorova MG, Palmowski-Wolfe AM. Function and morphology in macular retinoschisis associated with optic disc pit in a child before and after its spontaneous resolution. Doc Ophthalmol. 2012;124:149–55.
Tobe T, Nishimura T, Uyama M. Laser photocoagulation for pit-macular syndrome. Ganka-Rinshoiho. 1991;85:124–30 (in Japanese).
Cox MS, Witherspoon CD, Morris RE, Flynn HW. Evolving techniques in the treatment of macular detachment caused by optic nerve pits. Ophthalmology. 1988;95:889–96.
Jain N, Johnson MW. Pathogenesis and treatment of maculopathy associated with cavitary optic disc anomalies. Am J Ophthalmol. 2014;158:423–35.
Lincoff H, Yannuzzi L, Singerman L, Kreissig I, Fisher Y. Improvement in visual function after displacement of the retinal elevations emanating from optic pits. Arch Ophthalmol. 1993;111:1071–9.
Lincoff H, Kreissig I. Optical coherence tomography of pneumatic displacement of optic disc pit maculopathy. Br J Ophthalmol. 1998;82:367–72.
Theodossiadis GP. Treatment of maculopathy associated with optic disk pit by sponge explant. Am J Ophthalmol. 1996;121:630–7.
Postel EA, Pulido JS, McNamara JA, Johnson MW. The etiology and treatment of macular detachment associated with optic nerve pits and related anomalies. Trans Am Ophthalmol Soc. 1998;96:73–88.
Hirakata A, Okada AA, Hida T. Long-term results of vitrectomy without laser treatment for macular detachment associated with an optic disc pit. Ophthalmology. 2005;112:1430–5.
Spaide RF, Fisher Y, Ober M, Stoller G. Surgical hypothesis: inner retinal fenestration as a treatment for optic disc pit maculopathy. Retina. 2006;26:89–91.
Hirakata A, Inoue M, Hiraoka T, McCuen BW 2nd. Vitrectomy without laser treatment or gas tamponade for macular detachment associated with an optic disc pit. Ophthalmology. 2012;119:810–8.
Steel DHW, Suleman J, Murphy DC, Song A, Dodds S, Rees J. Optic disc pit maculopathy: A two-year nationwide prospective population-based study. Ophthalmology. 2018;125:1757–64.
Abouammoh MA, Alsulaiman SM, Gupta VS, Mousa A, Hirakata A, Berrocal MH, et al. Pars plana vitrectomy with juxtapapillary laser photocoagulation versus vitrectomy without juxtapapillary laser photocoagulation for the treatment of optic disc pit maculopathy: the results of the KKESH International Collaborative Retina Study Group. Br J Ophthalmol. 2016;100:478–83.
Ooto S, Mittra RA, Ridley ME, Spaide RF. Vitrectomy with inner retinal fenestration for optic disc pit maculopathy. Ophthalmology. 2014;121:1727–33.
Bottoni F, Cereda M, Secondi R, Bochicchio S, Staurenghi G. Vitrectomy for optic disc pit maculopathy: a long-term follow-up study. Graefes Arch Clin Exp Ophthalmol. 2018;256:675–82.
Theodossiadis G, Theodossiadis P, Chatziralli I. Thoughts and challenges for the current treatment of optic disc pit maculopathy. Semin Ophthalmol. 2020;35:232–6.
Michalewska Z, Nawrocka Z, Nawrocki J. Swept-source OCT and swept-source OCT angiography before and after vitrectomy with stuffing of the optic pit. Ophthalmol Retina. 2020;4:927–37.
Sakamoto T, Miyazaki M, Hisatomi T, Nakamura T, Ueno A, Itaya K, et al. Triamcinolone-assisted pars plana vitrectomy improves the surgical procedures and decreases the postoperative blood-ocular barrier breakdown. Graefes Arch Clin Exp Ophthalmol. 2002;240:423–9.
Hisatomi T, Notomi S, Tachibana T, Oishi S, Asato R, Yamashita T, et al. Brilliant Blue G double staining enhances successful internal limiting membrane peeling with minimal adverse effect by low cellular permeability into live cells. Retina. 2015;35:310–8.
Johnson TM, Johnson MW. Pathogenic implications of subretinal gas migration through pits and atypical colobomas of the optic nerve. Arch Ophthalmol. 2004;122:1793–800.
Chang S, Haik BG, Ellsworth RM, St Louis L, Berrocal JA. Treatment of total retinal detachment in morning glory syndrome. Am J Ophthalmol. 1984;97:596–600.
Strauss RW, Priglinger SG, Alge CS, Grueterich M, Haritoglou C. Persistent serous retinal detachment after radial optic neurotomy. Clin Exp Ophthalmol. 2006;34:718–20.
Rayat JS, Rudnisky CJ, Waite C, Huang P, Sheidow TG, Kherani A, et al. Long-term outcomes for optic disk pit maculopathy after vitrectomy. Retina. 2015;35:2011–7.
Mohammed OA, Pai A. Inverted autologous internal limiting membrane for management of optic disc pit with macular detachment. Middle East Afr J Ophthalmol. 2013;20:357–9.
Travassos AS, Regadas I, Alfaiate M, Silva ED, Proença R, Travassos A. Optic pit: novel surgical management of complicated cases. Retina. 2013;33:1708–14.
Nakashizuka H, Furuya K, Onoe H, Wakatsuki Y, Machida Y, Kitagawa Y, et al. Anterior lens capsule transplantation for acquired optic disc pit maculopathy. Ophthalmic Surg Lasers Imaging Retina. 2019;50:649–52.
Acknowledgements
The authors thank Professor Emeritus Duco Hamasaki of the Bascom Palmer Eye Institute, University of Miami, Miami, Florida, for discussions and thorough editing of the manuscript. Supported in part by Research Grant 17K11431 from the Japan Society for the Promotion of Science, Tokyo, Japan. Previous presentation Presented in part at the XXXIInd Meeting of the Club Jules Gonin, 2020.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
M. Sano, None; A. Hirakata, Grant, Lecture fee (Santen, Alcon, Novartis, Senju, Bayer), Grant (HOYA), Lecture fee (Nikon, Kowa, Nidek); Y. Kita, None; Y. Itoh, None; T. Koto, Lecture fee (Santen, Bayer, Novartis, HOYA, Ellex, Pfizer, Kowa, AMO); M. Inoue, Grant, Lecture fee (Alcon), Lecture fee (Novartis, Santen, Senju, Bayer, HOYA, ZEISS, Kowa).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Corresponding Author: Akito Hirakata
About this article

Cite this article
Sano, M., Hirakata, A., Kita, Y. et al. Risk factors for failure of resolving optic disc pit maculopathy after primary vitrectomy without laser photocoagulation. Jpn J Ophthalmol 65, 786–796 (2021). https://doi.org/10.1007/s10384-021-00866-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-021-00866-0