
Abstract
Purpose
To investigate the predictive factors of polyp regression after intravitreal ranibizumab injections for polypoidal choroidal vasculopathy (PCV).
Methods
Sixty-nine eyes (69 patients) with treatment-naïve PCV received an initial series of 3-monthly intravitreal ranibizumab injections, followed by as-needed injections. Polyp regression was determined after 6 months from baseline by means of indocyanine angiography and correlated with clinical characteristics at baseline.
Results
After treatment, 26.1 % (18 out of 69 eyes) achieved complete polyp regression and 73.9 % (51 out of 69 eyes) showed persistent polyps. The mean logarithm of the minimum angle of resolution (logMAR) of best-corrected visual acuity (BCVA) was significantly improved in both groups (P = 0.02). No statistically significant difference in BCVA improvement was observed between the groups. However, the proportion of subjects with BCVA improvement by more than three lines was significantly higher in the polyp regression group (P = 0.02). Univariate analysis of the baseline characteristics identified the number of polyps (P = 0.02), the total polyp area (P = 0.009) and the polyp pattern (P = 0.01) as predictive factors for polyp regression. Multivariate logistic regression identified the total polyp area (P = 0.01) as an independent predictor for polyp regression after intravitreal ranibizumab injections.
Conclusions
The regression of polypoidal lesions in PCV patients after intravitreal ranibizumab injections was associated with a smaller total polyp area. This result could be helpful in predicting polypoidal changes after ranibizumab treatment and in deciding the best treatment strategy for PCV patients.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Polypoidal choroidal vasculopathy (PCV) is characterized by the presence of a branching vascular network in association with polypoidal choroidal vascular lesions that cause subretinal leakage, subretinal hemorrhage and pigment epithelial detachment (PED) [1]. PCV is generally considered as a subtype of neovascular age-related macular degeneration (AMD) [2] and accounts for 23–54 % of neovascular AMD in Asian populations [3, 4].
An abnormally branching vascular network terminating in polypoidal lesions is one clinical characteristic that distinguishes PCV from typical neovascular AMD [1, 4, 5]. When exudates or hemorrhage develop beneath the polypoidal lesions, they become detached from Bruch’s membrane, and PED develops [6]. Polypoidal lesions in PCV patients are a major causative factor of exudative and hemorrhagic complications, and regression of polyps is associated with the resolution of retinal fluid [7, 8]. In addition, the presence of polyps in an active disease represents a risk of rupture and leakage [6–8]. Therefore, regression of polypoidal lesions could be important for the visual prognosis of PCV patients.
There are several effective ways to treat PCV: photodynamic therapy (PDT) with verteporfin, intravitreal injection of anti-vascular endothelial growth factor (VEGF) or a combination of both [7, 9]. Intravitreal anti-VEGF injections are effective in reducing the exudation and hemorrhage associated with PCV, hence stabilizing vision [10, 11]. However, it is reported that the rate of polyp regression is 28–33 % in patients treated with anti-VEGF monotherapy, which is inferior to that of PDT only or PDT combined with anti-VEGF (72–90 %) [9, 10, 12, 13].
Although intravitreal anti-VEGF agents are commonly used to treat PCV, the clinical factors associated with polyp regression following anti-VEGF treatment are unknown. Identification of the clinical characteristics associated with polypoidal complex response to anti-VEGF agents before initiating PCV treatment may be helpful in selecting the appropriate treatment strategy. If polyps regress after anti-VEGF monotherapy, it would be beneficial to administer anti-VEGF without PDT as a baseline treatment. The purpose of this study was to determine the predictive clinical factors of polyp regression in PCV patients after ranibizumab treatment.
Methods
We retrospectively reviewed the medical records of 69 consecutive patients with PCV who were treated with intravitreal ranibizumab injections at the Retina Center of Kim’s Eye Hospital in Konyang University College of Medicine from August 2010 through October 2012. This study was approved by the Institutional Review Board of Kim’s Eye Hospital, Konyang University College of Medicine. The clinical research in this study followed the tenets of the Declaration of Helsinki.
Inclusion and exclusion criteria
Inclusion criteria included the following: (1) age >50 years; (2) confirmation of PCV with fluorescein angiography (FA) and indocyanine angiography (ICGA), performed using a confocal laser scanning system (HRA-2, Heidelberg Engineering, Dossenheim, Germany) at the first visit; (3) no previous treatment; (4) treatment with an anti-VEGF agent (ranibizumab); (5) the availability of an ICGA examination performed at 6 months after beginning the ranibizumab treatment. We only included patients whose ICGA revealed the presence of characteristic polypoidal structures at the border of the branching choroidal vascular networks.
The exclusion criteria included the following: (1) prior treatment with PDT; (2) treatment combined with PDT; (3) other concomitant ocular diseases, such as diabetic retinopathy, high myopia, vein or artery occlusion, or epiretinal membrane; (4) other ocular diseases that could affect visual acuity; (5) previous vitreoretinal surgery. No limits on visual acuity were set as either inclusion or exclusion criteria.
Assessments
ICGA was performed at baseline and at 6 months after the beginning of the ranibizumab injection for all patients. ICGA was used to determine polyp regression, total polyp area, polyp pattern, largest polyp size, greatest linear dimension (GLD), area of the abnormal branching vascular network and choroidal vascular hyperpermeability.
Choroidal vascular hyperpermeability was evaluated in the late phase of ICGA, approximately 10–15 min after dye injection following previous reports [14–16]. Choroidal vascular hyperpermeability was defined as multifocal hyperfluorescence seen in the middle and late ICGA phases. The diagnosis of PCV and the presence of choroidal vascular hyperpermeability were evaluated by two independent investigators (H.J.C. and H.S.K.). When the evaluation was inconsistent, the senior investigator (T.G.L) made the final decision.
Patients were divided into two groups: a polyp regression group and a polyp persistent group after treatment. Partial polyp regressions were included in the persistent group. The areas of individual polyps excluding the hypofluorescent halo were measured manually using the software provided with the HRA-2 hardware and summed, thereby deriving the total polyp area. The abnormal branching vascular network area was also measured based on the ICGA. The GLD considered the entire PCV vascular lesion, including the polypoidal lesion, branching vascular network vessels and any type 2 choroidal neovascularization (CNV). The pigment epithelial detachment, without underlying vascular components, was not included in the GLD measurement.
The polypoidal lesion pattern was evaluated as a solitary polyp or a cluster of polyps. According to the observation by Yuzawa and associates [17], a cluster of polypoidal lesions in this study was defined as follows: (1) large reddish-orange aneurysmal dilation with the longest axis of 1500 μm or longer on a fundus photograph; (2) a hyperfluorescence corresponding to the aneurysmal dilation on late-phase ICGA; (3) sprouting of numerous polyps of diverse sizes showing an appearance similar to grapes in the earlier ICGA phase.
Best-corrected visual acuity (BCVA) was assessed using a Snellen chart at baseline and at each monthly follow-up visit after the initiation of intravitreal ranibizumab injection treatment. For statistical analysis, the Snellen BCVA was converted to a logarithm of the minimum angle of resolution (logMAR).
Central macular thickness was measured by spectral domain optical coherence tomography (SD-OCT, Spectral OCT/SLO®, OTI Ophthalmic Technologies Inc., Miami, FL, USA), assessed by measuring the retinal thickness of the 1-mm central retina, which was obtained by a macular scan. Only well-centered scans without overt algorithm failure messages, an incorrect threshold line and segmentation errors were selected for analysis. The frequency of complete resolution of retinal fluid (termed "dry macula") detected by OCT was also evaluated at 6 months from baseline.
Intravitreal ranibizumab treatment
Intravitreal injections of ranibizumab (0.5 mg/0.05 ml Lucentis, Genentech Inc., South San Francisco, CA, USA) were administered to all patients following the same treatment and retreatment protocols. After performing the initial 3 monthly loading injections, retreatment for each patient was performed as needed, based on the presence of any of the following: (1) visual deterioration of more than 2 Snellen lines (>0.2 logMAR); (2) evidence of persistent fluid or hemorrhage involving the macula on OCT at least 1 month after the previous injection; (3) newly developed macular hemorrhage; (4) evidence of an active PCV lesion, as seen on FA, ICGA or OCT.
Statistical analysis
SPSS software version 12.0 (SPSS Inc., Chicago, IL, USA) was used for all of the statistical analyses. Frequencies were compared between the groups by using the chi-squared or Fisher’s exact test. Comparative statistical analysis was performed using unpaired t-tests. To investigate the baseline clinical characteristics (baseline BCVA, GLD, size of the vascular network, number of polyps, size of the largest polyp, total polyp area, presence of subretinal hemorrhage, presence of PED, presence of type 2 CNV and presence of choroidal vascular hyperpermeability) related to polyp regression after ranibizumab treatment, multivariate logistic regression analysis was performed. Forward and backward stepwise regression was performed using the likelihood-ratio model, in which change in the likelihood-ratio statistic, based on the maximum partial likelihood estimates for the covariate, was used for variable selection. A p value less than 0.05 was considered statistically significant, and all tests were two-sided.
Results
A total of 69 eyes of 69 PCV patients (45 men, 24 women) who underwent treatment with intravitreal ranibizumab injections were enrolled in the study. All patients were South Korean, and the average age for the entire study group was 67.4 ± 7.2 years. According to the presence of polyps after treatment, subjects were categorized into two subgroups: the polyp regression group (18 eyes, 26.1 %) and the persistent polyp group [51 eyes, 73.9 %; partial regression was found in 16 eyes (23.2 %) and no regression was found in 35 eyes (50.7 %)] (Table 1).
When comparing baseline characteristics between the groups, the mean number of polyps was higher in the persistent polyp group than in the polyp regression group (P = 0.05). The mean total polyp area was larger in the persistent group (P = 0.002). The polypoidal lesion pattern was significantly different between the groups; a cluster type of pattern was more frequent in the persistent group (P = 0.03) (Table 1).
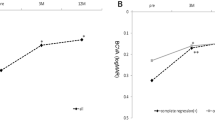
Baseline BCVA was 0.71 ± 0.45 logMAR (Snellen equivalent, 20/102) in the polyp regression group and 0.68 ± 0.41 logMAR (Snellen equivalent, 20/95) in the persistent polyp group. There was no significant difference in baseline BCVA between the groups (P = 0.32). There was no significant difference between the two groups with respect to age, sex, mean baseline central macular thickness, PCV location, mean GLD, mean size of the abnormal vascular network, mean size of the largest polyp, incidence of subretinal hemorrhage, incidence of PED, incidence of type 2 CNV and the incidence of choroidal vascular hyperpermeability (Table 1).
After treatment, logMAR BCVA was significantly decreased to 0.58 ± 0.42 (Snellen equivalent, 20/76) in the polyp regression group (P = 0.02) and to 0.59 ± 0.41 (Snellen equivalent, 20/77) in the persistent group (P = 0.02) at 6 months from baseline. Mean logMAR changes and mean central macular thickness changes from baseline were not different between the groups (Table 2). However, improvements in the logMAR BCVA values by ≥0.3 (>3 lines gain) and presence of dry macula observed in the polyp regression group were significantly higher than those observed in the persistent group (P = 0.02 and P = 0.03, respectively; Table 2). The mean number of injections showed no statistical difference between groups (Table 2).
Table 3 demonstrates the relationship between polyp regression and the clinical observations at baseline. By univariate analysis, the number of polyps, total polyp area and polyp pattern were significantly related to polyp regression (P = 0.02, 0.001, and 0.01, respectively). Forward and backward stepwise logistic regression analysis found that the total polyp area was the independent factor related to polyp regression after ranibizumab treatment (P = 0.01). None of the patients showed regression of more than 0.5 mm2 of the total polyp area. The largest regressed polyp area observed was 0.34 mm2.
No complications associated with injections, including endophthalmitis, traumatic lens injury or retinal detachment, were observed. Further, no systemic adverse events occurred in patients treated with intravitreal ranibizumab injections.
Several representative cases with or without polyp regression after ranibizumab injections are shown in Fig. 1.

Several indocyanine angiography (ICGA) images from cases with polypoidal choroidal vasculopathy (PCV) with or without polyp regression after intravitreal ranibizumab injections. a–d Cases from the polyp regression group. e–h Cases from the polyp persistent group. a ICGA image OD of a 65-year-old male with PCV. The total polyp area is 0.32 mm2. b ICGA showing complete polyp regression after intravitreal ranibizumab injections (total injection number: 4) c ICGA image OS of a 72-year-old male with PCV. The total area of the polyp is 0.12 mm2. d ICGA showing complete polyp regression after monthly ranibizumab injections (total injection number: 3). e ICGA image OS of a 52-year-old male with PCV. The total polyp area is 0.49 mm2. f ICGA showing persistent polyp after ranibizumab injections (total injection number: 4). g ICGA image OD of a 57-year-old male with PCV. The area of the total polyp is 0.58 mm2. h ICGA showing partial regression of the polyp after ranibizumab injections (total injection number: 5)
Discussion
Polypoidal lesions are thought to be the main source of the exudative change and hemorrhagic complications in PCV [5, 6]. In addition, the presence of polypoidal lesions might be associated with the development of retinal and subretinal hemorrhage risks [6, 7]. Moreover, polypoidal lesions are associated with the expansion of branching vascular lesions. The branching vascular PCV network expands by simple proliferation and hypertrophy of the vascular components, by conversion of the polypoidal lesion into the advancing edge of a vascular channel or by the unfolding of a cluster of polypoidal lesions and subsequent transformation into widening vascular tubular components [3]. Therefore, the polyp changes after anti-VEGF treatment could be important in treating PCV patients and predicting prognosis.
Currently, either alone or in combination with PDT, intravitreal anti-VEGF injections are a common treatment for PCV. Their application for polyp regression is still limited [9–13]. It has been demonstrated that smaller lesions and a smaller branching vascular network are associated with polyp regression after PDT [18]. However, there is no sufficient reported evidence to allow for a prediction of post anti-VEGF monotherapy results, and the mechanism by which anti-VEGF could regress polypoidal lesions of PCV has not yet been fully elucidated. In fact, there is no evidence that anti-VEGF directly induces polyp regression. One possible mechanism is that polyp regression is associated with decreased exudation or hemorrhage from the abnormal branching vascular network [19]. The abnormal branching vascular network is thought to be the main causative factor for developing polyps [5, 6]. Anti-VEGF could decrease exudation and hemorrhage from PCV, especially from the abnormal branching vascular network [20], which could induce polyp regression. On the other hand, PDT might represent another mechanism of polyp regression. Clinical and experimental evidence indicates that PDT could have an occlusive effect on nonproliferative vessels of choroidal origin, including normal vessels [20, 21]. This vaso-occlusive effect of PDT might result in more efficient polyp regression in PCV patients than anti-VEGF.
Although PDT has an advantage in regard to polyp regression, visual outcomes of the anti-VEGF monotherapy group and anti-VEGF combined with the PDT group show no significant differences [10, 12, 13]. Moreover, severe visual loss due to extensive subretinal hemorrhage is not uncommon after PDT; complications such as subretinal hemorrhage or vitreous hemorrhage may occur in as many as 31 % of patients treated with PDT [22]. Therefore, if polyps were predicted to regress with only anti-VEGF, anti-VEGF monotherapy without PDT could be a valuable and safe treatment option in treating PCV patients.
In the current study, among the various baseline characteristics, the total polyp area was the only factor significantly associated with polyp regression after ranibizumab treatment. Other baseline angiographic information, including the polyp pattern, size of the largest polyp and number of polyps was not predictive of polyp regression. Considering the previous reports that developing polyps are associated with an exudative and hemorrhagic tendency of the branching vascular lesion [5–7], it could be suggested that a large polyp area might reflect the more active nature of the disease and more severe exudative or hemorrhagic tendency of the PCV lesion. Our results suggest that, if the total polyp area is large at baseline, anti-VEGF therapy combined with PDT can be considered as an alternative treatment to anti-VEGF monotherapy.
It is reported that even when the entire vascular lesion is coagulated and the polyp regresses completely with PDT, the polypoidal lesion often recurs, resulting in decreased visual acuity [19, 20]. The reason may be that the abnormal branching vascular PCV network itself has exudative and hemorrhagic tendencies [16, 20]. Therefore, after complete polyp regression, careful follow-up with frequent OCT or angiographic evaluation is required for detection of newly developed exudative or hemorrhagic changes. In addition, the association of polyp regression and visual outcome and its clinical significance in PCV patients require further investigation.
This study has several limitations, including the retrospective nature of the work. It covers a relatively short time span. In the current study, 26.1 % of all patients showed polyp regression, a similar rate to that of other reports [7–12]. Moreover, according to the prospective randomized EVEREST study [10], the polyp regression rate after administration of ranibizumab monotherapy was similar at 3, 4, 5 and 6 months from baseline. Furthermore, the regression rate in this study was similar to that in other studies with 12- or 24-month follow-up periods and more frequent anti-VEGF injections [11, 23]. Thus, the polyp regression rate observed in the current study may not change drastically with more follow-ups.
In conclusion, polypoidal lesion regression in PCV patients after ranibizumab treatment was associated with a smaller total polypoidal lesion area. This result may be helpful in predicting polypoidal changes after anti-VEGF treatment and selecting the appropriate treatment strategy for PCV patients. In patients with small polyps, anti-VEGF monotherapy without PDT could be a better treatment option.
References
Yannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina. 1990;10:1–8.
Laude A, Cackett PD, Vithana EN, Yeo IY, Wong D, Koh AH, et al. Polypoidal choroidal vasculopathy and neovascular age-related macular degeneration: same or different disease? Prog Retin Eye Res. 2010;29:19–29.
Yannuzzi LA, Ciardella A, Spaide RF, Rabb M, Freund KB, Orlock DA. The expanding clinical spectrum of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol. 1997;115:478–85.
Yannuzzi LA, Wong DWK, Storzolini BS, Goldbaum M, Tang KC, Spaide RF, et al. Polypoidal choroidal vasculopathy and neovascularized age-related macular degeneration. Arch Ophthalmol. 1999;117:1503–10.
Spaide RF, Yannuzzi LA, Slakter JS, Sorenson J, Orlach DA. Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina. 1995;15:100–10.
Tsujikawa A, Sasahara M, Otani A, Gotoh N, Kameda T, Iwama D, et al. Pigment epithelial detachment in polypoidal choroidal vasculopathy. Am J Ophthalmol. 2007;143:102–11.
Chan WM, Lam DS, Lai TY, Liu DT, Li KK, Yao Y, et al. Photodynamic therapy with verteporfin for symptomatic polypoidal choroidal vasculopathy: one-year results of a prospective case series. Ophthalmology. 2004;111:1576–84.
Sho K, Takahashi K, Yamada H, Wada M, Nagai Y, Otsuji T, et al. Polypoidal choroidal vasculopathy: incidence, demographic features, and clinical characteristics. Arch Ophthalmol. 2003;121:1392–6.
Koh A, Lee WK, Chen LJ, Chen SJ, Hashad Y, Kim H, et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina. 2012;32:1453–64.
Hikichi T, Higuchi M, Matsushita T, Kosaka S, Matsushita R, Takami K, et al. One-year results of three monthly ranibizumab injections and as-needed reinjections for polypoidal choroidal vasculopathy in Japanese patients. Am J Ophthalmol. 2012;154:117–24.
Lai TY, Lee GK, Luk FO, Lam DS. Intravitreal ranibizumab with or without photodynamic therapy for the treatment of symptomatic polypoidal choroidal vasculopathy. Retina. 2011;31:1581–8.
Sagong M, Lim S, Chang W. Reduced-fluence photodynamic therapy combined with intravitreal bevacizumab for polypoidal choroidal vasculopathy. Am J Ophthalmol. 2012;153:873–82.
Guyer DR, Yannuzzi LA, Slankter JS, Sorenson JA, Ho A, Orlock D. Digital indocyanine green angiography of central serous chorioretinopathy. Arch Ophthalmol. 1994;112:1057–62.
Koizumi H, Yamagishi T, Yamazaki T, Kinoshita S. Relationship between clinical characteristics of polypoidal choroidal vasculopathy and choroidal vascular hyperpermeability. Am J Ophthalmol. 2013;155:305–13.
Jirarattanasopa P, Ooto S, Nakata I, Tsujikawa A, Yamashiro K, Oishi A, et al. Choroidal thickness, vascular hyperpermeability, and complement factor H in age-related macular degeneration and polypoidal choroidal vasculopathy. Invest Ophthalmol Vis Sci. 2012;53:3663–72.
Yuzawa M, Mori R, Kawamura A. The origins of polypoidal choroidal vasculopathy. Br J Ophthalmol. 2005;89:602–7.
Lee WK, Kim KS, Kim W, Lee SB, Jeon S. Responses to photodynamic therapy in patients with polypoidal choroidal vasculopathy consisting of polyps resembling grape clusters. Am J Ophthalmol. 2012;154:355–65.
Honda S, Miki A, Yanagisawa S, Matsumiya W, Nagai T, Tsukahara Y. Comparison of the outcomes of photodynamic therapy between two angiographic subtypes of polypoidal choroidal vasculopathy. Ophthalmologica. 2014;. doi:10.1159/000360308.
Saito M, Iida T, Kano M. Intravitreal ranibizumab for polypoidal choroidal vasculopathy with recurrent or residual exudation. Retina. 2011;31:1589–97.
Schmidt-Erfurth UM, Michels S, Kusserow C, Jurklies B, Augustin AJ. Photodynamic therapy for symptomatic choroidal hemangioma: visual and anatomic results. Ophthalmology. 2002;109:2284–94.
Lee WK, Lee PY, Lee SK. Photodynamic therapy for polypoidal choroidal vasculopathy: vaso-occlusive effect on the branching vascular network and origin of recurrence. Jpn J Ophthalmol. 2008;52:108–15.
Hirami Y, Tsujikawa A, Otani A, Yodoi Y, Aikawa H, Mandai M. Hemorrhagic complications after photodynamic therapy for polypoidal choroidal vasculopathy. Retina. 2007;27:335–41.
Hikichi T, Higuchi M, Matsushita T, Kosaka S, Matsushita R, Takami K, et al. Results of 2 years of treatment with as-needed ranibizumab reinjection for polypoidal choroidal vasculopathy. Br J Ophthalmol. 2013;97:617–21.
Conflicts of interest
H. J. Cho, None; S. Y. Han, None; H. S. Kim, None; T. G. Lee, None; J. W. Kim, None.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Cho, H.J., Han, S.Y., Kim, H.S. et al. Factors associated with polyp regression after intravitreal ranibizumab injections for polypoidal choroidal vasculopathy. Jpn J Ophthalmol 59, 29–35 (2015). https://doi.org/10.1007/s10384-014-0349-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-014-0349-x