
Summary
Osteogenesis imperfecta (OI) is an extremely heterogeneous group of heritable connective tissue disorders. Most of the affected patients carry autosomal dominant mutations in the genes encoding for collagen type I, the most abundant protein of the bone extracellular matrix. The resulting phenotypes are extremely broad and have been classified by Sillence and colleagues into four groups according to clinical, radiological and genetic criteria.
More recently, proteins have been described that interact directly or indirectly with collagen biosynthesis and their deficiency result in rare forms of mostly autosomal recessive OI sharing phenotypic features of ‘classical’ types but lacking primary defects in type I collagen. Consequently the Sillence classification has been gradually expanded to include novel forms based on the underlying mutations. The goal of this article is to revisit the actual OI classification and to outline current approaches in categorizing the disorder.
Zusammenfassung
Osteogenesis imperfecta (OI) ist eine äußerst heterogene Gruppe von erblichen Erkrankungen des Bindegewebes. Die meisten der betroffenen Patienten sind Träger dominanter Mutationen in den Genen für Kollagen Typ I, dem häufigsten Protein der extrazellulären Matrix. Die sich daraus ergebenden Phänotypen sind sehr vielfältig und wurden von Sillence und Kollegen in vier Gruppen entsprechend klinischen, radiologischen und genetischen Kriterien eingeteilt.
In den letzten Jahren wurden neue Proteine beschrieben, die direkt oder indirekt mit der Kollagenbiosynthese wechselwirken. Sehr seltene Mutationen, die Störungen in diesen Proteinen hervorrufen, führen in der Regel zu autosomal-rezessiven Sonderformen mit einem ähnlichen klinischen Bild wie in den „klassischen“ Formen von OI, aber ohne primären Kollagendefekt. Deshalb wurde die Sillence Klassifikation schrittweise erweitert, um auch diese neuen Formen zu berücksichtigen, die durch ihre Mutation definiert sind. Das Ziel dieses Artikels ist es, den derzeitigen Stand der OI Klassifikation zu präsentieren und zu diskutieren.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Many new forms of osteogenesis imperfecta (OI) or ‘brittle bone disease’ have been discovered in the last decade. The hallmarks of the disease are bone fragility, spine and limb deformities as well as chronic pain depending on severity. The traditional nomenclature, due to Sillence, defines OI types according to the severity of the disease. The newly discovered forms and especially the growing knowledge about the diverse genetic backgrounds of the disorder have been challenging this classification. The Sillence nomenclature has been substantially enlarged with a gradual paradigm shift from a phenotypic to a genotypic classification. The aim of this article is to revisit the OI classification from a historical perspective and to highlight the most recent discoveries in the area.
From single observations to one disease
Starting at the end of the seventeenth century, reports on conditions associated with abnormally fragile bones began to appear.
In 1788, Olof Jakob Ekman, a Swedish military surgeon described a family in which four generations suffered from a hereditable bone fragility condition that he called ‘osteomalacia congenita’ [1]. Some decades later, the French pathologist Lobstein reported in his ‘Traité d´anatomie pathologique générale’ (1833) on three children from one family affected by ‘fragilitas ossium’ that he termed as ‘osteopsathyrosis idiopathica’. Remarkably he also noted that more organs were affected without however giving further details.
In 1849, the Dutch anatomist Wilhem Vrolik depicted an infant with shorten and deformed extremities who died 3 days after birth: ‘In the skeleton is manifest injury by a multitude of fractures, which no one rib nor any of the long bones spared: several, indeed, even display two or three fractures … Undoubtedly, this singular condition of the skeleton is attributable to imperfect ossification’ [2, 3]. So middle of the nineteenth century, a disease called ‘Osteogenesis imperfecta congenita’ was defined as a condition inherently different from rickets or the postnatal acquired ‘English Disease’ which was spreading over the century of the industrial revolution and where bones fragility was a secondary effect due to ‘Britain’s gloomy skies and dark winters’ [4].
For about half a century, ‘osteopsathyrosis idiopathica’ and ‘osteogenesis imperfecta congenita’ remained two different diseases until the Swiss pathologist Emil Looser provided 1906 histological evidences that both entities were manifestations of the same disorder. He recognized that OI was a rare systemic condition of unknown aetiology characterized by ‘imperfect development of bone’ and made the very first classification into two types according to the time point when the first fracture occurred: congenita (type Vrolik) with fractures already in the perinatal period and tarda (type Ekman–Lobstein) when the fractures occurred after the first year. This very first classification of OI was later on modified by Seedorf who subclassified OI tarda into OI tarda gravis when the first fractures occurred within the first year of life because of subsequent development of severe skeletal deformities and OI tarda levis when the fractures occurred later [1].
Secondary features associated with this form of bone fragility were gradually recognized
Eddowes suggested 1900 that sclera and bone abnormalities might be linked since ‘the framework of both organs are formed by fibrous tissues’. Peters, a German ophthalmologist first described blue sclerae as an ‘inherited anomaly due to thinness of fibrous tissue’ and afterward, he realized that these patients also suffered from abnormal bone fragility (1913). Hearing impairment and deafness as well as, hypermobility and hyperlaxity of the joints and finally dental abnormalities (dentinogenesis imperfecta) causing teeth discoloration and tooth decay and loss were subsequently described to be also associated with the disease (reviewed by [1]).
Four distinct syndromes called OI
The advances in molecular and radiological diagnosis achieved during the following decades allowed a deeper understanding of the genetic underpinning OI. The disease became defined very similar as it is today: a hereditary, highly variable disorder characterized by osteopenia and increased bone fractures caused by molecular abnormalities in type I collagen, the main component of the organic bone matrix. Moreover, it appeared clearly that abnormalities manifested in all tissues where the principal matrix protein was type I collagen: dentin, sclera and ligaments. Radiological evaluation allowed documenting size, shape of the bones as well as number of fractures.
Based on the observations of 180 affected patients, the Australian physician David Sillence [5] suggested in 1979 a new classification reflecting the broad spectrum of the mode of inheritance, as well as the clinical and radiological manifestations of OI.
The original Sillence classification
OI type I: dominantly inherited OI with blue sclera
OI type II: lethal perinatal with radiographically crumpled femora and beaded ribs
OI type III: progressively deforming OI
OI type IV: dominantly inherited OI with normal sclera.
The Sillence classification has received wide acceptance and is still currently used as a grading of clinical severity of OI. However, the criteria used for the original classification were modified since then. The main reason therefore is that the Sillence nomenclature was proposed 4 years before the genetic origin of OI was identified. In fact, 1983 appeared the very first evidence on a collagen defect leading to OI [6]. Many more collagen-gene defects were rapidly identified and up to now more than 1500 causative mutations have been reported [7]. These findings led to the definition of OI as collagen-related disorder [7, 8]:
-
OI is mostly associated with mutations in COL1A1 and COL1A2 the genes encoding for the type I collagen chains.
-
All mutations are transmitted as autosomal dominant traits.
-
In the vast majority of the cases, the mutations led to abnormalities in the primary structure of the collagen type I molecule. The phenotypic consequences are extremely variable encompass the wide spectrum of clinical severity from mild to lethal forms.
-
A small group of mutations led to a decreased quantity of otherwise normal type I collagen. The phenotypic consequence is the mildest form of the disease.
The hallmark of all mutations is decreased bone mass and increased bone fragility. Accessory characteristics like spine and limb deformities, growth impairment and chronic pain were used for the:
The actualized Sillence classification (reviewed by [8])
OI type I: mild form. Patients have no bone deformities, normal or near normal stature.
OI type II: extremely severe form is perinatal lethal.
OI type III: most severe form in children surviving the neonatal time, severely deforming, extreme short stature.
OI type IV: intermediate form between type I and type III: mild to moderate bone deformities and variable short stature.
Of note, the Sillence classification is gradual, describes a continuum spectrum of severity with many overlaps. Moreover, secondary features like hearing impairment, blue (or grey) sclera, tooth abnormalities (dentinogenesis imperfecta), Wormian bones (accessory skull bones surrounded by suture lines) are extremely variable and may not always represent reliable classification criteria [9, 10].
A further limitation of the Sillence classification is that in about 10 % of patients having a clinical diagnosis of OI with no mutations in the genes encoding for collagen could be identified. Moreover, in many of these cases there was strong evidence for an autosomal recessive inheritance because of recurrence of OI in pedigrees from unaffected parents. So, additional causes of OI were suspected for a couple of years.
The expanded Sillence classification
That the Sillence classification would not cover the complete range of the disease was confirmed in 2000–2002 by the group of Francis H. Glorieux and colleagues from the Shriner’s hospital in Montreal, Canada. They presented three groups of patients with clinical diagnosis OI having distinctive skeletal and bone histological features in comparison to the patients classified previously by Sillence. The underlying genetic defect remained unknown at that time, but it was clear that none of these individuals showed evidence for a collagen primary sequence defect. Moreover, in two of the three clinical entities an autosomal recessive inheritance was found. To clearly underline the difference to the ‘classical’ forms of OI with collagen-gene defects, these additional groups were defined as ‘new’ forms of OI, with intact primary structure of collagen type I and categorized as OI type V, type VI and type VII corresponding to the chronological order when the cases were reported. Consequently, in 2004, an expanded Sillence classification was suggested [11].
The remarkable point of the expanded Sillence classification is that the ‘new forms’ of OI are not anymore defined according to clinical severity but according to a still unexplained aetiology.
Discovery of new pathways leading to OI
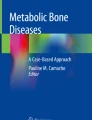
The discovery of new pathways leading to OI are intimately linked with the progress in understanding the complex molecular biology of collagen synthesis [7, 12, 13] (Fig. 1). Basically, type I collagen is a triple helical molecule, a heterotrimer consisting of two alpha 1 and one alpha 2 chains, that are first synthesized as single chains and post-translational become folded and extensively modified. During these intracellular processes, numerous amino acids are hydroxylated and glycosylated by specific enzymes. In addition, these events are ‘assisted’ by so called ‘molecular chaperones’ controlling the proper collagen folding or inducing specific cellular responses—termed endoplasmic-reticulum (ER) stress—to misfolded proteins (reviewed by [14, 15]). Subsequently, a procollagen molecule consisting of the core triple helical domain of 1014 amino acids and flanked at each end by globular propeptides is secreted into the pericellular space where the terminal propeptides are removed by specific extracelluar proteinases leading to fibril assembly and the formation of enzymatic cross-links. Finally, the mature collagen fibril becomes incorporated in the bone matrix and mineralized (see Fig. 1). In principle, each of these steps are highly controlled processes and any defect or malfunction may result in OI.

Overview of collagen formation and modification: Single proCOL1A1 and proCOL1A2 polypeptide chains are synthesized and transported into the endoplasmic reticulum where the chains become assembled, folded and extensively modified. Subsequently, the procollagen molecule is secreted into the pericellular space and the terminal propeptides are removed by specific proteinases. The mature triple helical procollagen molecule becomes incorporated and stabilized into the matrix by formation of covalent crosslinks. Moreover the collagen fibrils bind also to growth factors and cytokines forming a functional scaffold supporting matrix mineralization [7, 17]
This means that the aforementioned phenotypic characteristics are not necessarily caused by mutations in the collagen molecule itself. In fact, an OI phenotype can also result from defects in proteins involved in the post-translational modification of collagen, from malfunction of collagen chaperones, or from alteration in signalling proteins responding to intracellular ER stress and leading to dysfunctional osteoblast. Moreover some rare forms of OI are originated by deficiencies of proteins involved in the extracellular cleavage of the collagen propeptide during final fibril assembly, in the formation of cross-linking bonds between fibrils and in the regulation of the mineralization process [16, 17].
The first evidence therefore came in 2006 when Roy Morello reported that recessive OI type VII was caused by a defect in the gene encoding for cartilage associated protein (CRTAP) [18]. CRTAP was identified as a part of an enzymatic complex involved in the intracellular processing of the collagen type I triple helix: the prolyl 3-hydroxylation complex. This complex is located intracellularly within the endoplasmic reticulum and plays an important role in the post-translational modification of specific proline residues in the unfolded collagen chains [19]. Moreover, the prolyl 3-hydroxylation complex was found to consist of three subunits that assemble in the ratio 1:1:1, where CRTAP is the helper protein, prolyl 3-hydroxylase 1 (P3H1) the proper enzyme and cyclophylin B (CyPB) a chaperone for collagen synthesis (reviewed by [17]). These proteins are crucial for a proper collagen folding and mutations in each unit were identified to cause OI. The latter two variants were termed as OI type VIII and OI type IX respectively [20–23].
OI type X and OI type XI were subsequently identified and found to be caused by other proteins interfering with intracellular collagen processing and extracellular cross-linking [24], reviewed by [17, 25]).
The list of the discovery of new genes leading to new rare forms of OI is since then continuously growing (see a short overview in Table 1) raising many new questions about the underlying molecular mechanisms [26].
OI classification: quo vadis?
It is obvious that the discussion of an actual classification of OI became immensely complicated by the discovery of new genes, leading to OI. Actually there is a confusing coexistence between the Sillence classification into four groups based on clinical characteristics and inheritance pattern versus a continuously expanding classification based on the addition of the many causative genes having important clinical overlap with the ‘classical’ Sillence forms. Different approaches are currently under discussion.
Plotkin [27] suggested in 2004 to define as OI only cases caused by mutations in the genes encoding type I pro-collagen whereas mutations in other genes would lead to ‘syndromes with congenital brittle bones resembling OI’.
Van Dijk [28] suggested in 2010 to adopt a revised Sillence classification from OI type I to OI type VI but removing the forms which have clinical and radiographical features indistinguishable from OI Type II, III and IV. This concept is basically in line with the advice of an international expert group delineating a ‘Revision of the Nosology and Classification of Genetic Skeletal Disorders’ that agreed to retain the Sillence classification as the prototypic and universally accepted way to classify the degree of severity in OI and to free it from any direct molecular reference [29].
However, more recently, Van Dijk and Sillence himself proposed to add OI type V to the four groups of the original classification and to include again coloured sclerae as a classification criteria [8]:
OI type 1: mild form, non-deforming OI with blue sclera. Patients have low bone mass, increased bone fragility and susceptibility to hearing impairment. Autosomal dominant inheritance.
OI type 4: moderate or variable form. Patients have recurrent fractures, variable degrees of bone deformities, but normal sclerae and mostly no hearing impairment. Either autosomal dominant or recessive inheritance.
OI type 3: Progressively deforming. Bone fractures already at birth or as infants, severe osteopenia, deforming, growing impairment, progressive kyphoscoliosis and hearing loss during adulthood. Sclera might be blue at birth and becomes less blue with age. Either autosomal dominant or recessive inheritance.
OI type 2: perinatal lethal. Either autosomal dominant or recessive inheritance.
OI type 5: OI with calcification in the intraosseous membranes. (The causative mutation in BRIL was very recently discovered [30].) Autosomal dominant inheritance.
An alternative OI categorization based on connected metabolic mechanisms allowing an accurate genetic counselling and possibly in the future therapy options, is currently discussed by Joan C. Marini et al. [31] (see also Table 1):
-
Autosomal dominant mutations leading to a decrease in quantity of type I collagen (OI type I)
-
Autosomal dominant mutations leading to a defect in the structure of type I collagen (OI types II, III, IV)
-
Mutations leading to abnormal matrix mineralization: autosomal dominant type V, autosomal recessive type VI (abnormally high accumulation of osteoid observed in histological sections)
-
Autosomal recessive mutations leading to defects in collagen modification: mutation in the 3-hydroxylation complex (OI types VII, VIII, IX)
-
Autosomal recessive mutations leading to defects in collagen chaperones and foldases. (OI types X, XI).
-
Defects in extracellular collagen processing (cleaving the C-propeptide from type I procollagen: mutations in BMP1 and mutations in C-propeptide cleavage site).
-
Defects in osteoblast development: autosomal recessive mutations in SP7/Osterix, WNT1, TRIC-B, OASIS, PLS3 [25, 32] (see Table 1).
In conclusion, it can be stated that the genetic discoveries of the last years have generated a shift in paradigm where osteogenesis imperfecta is in the great majority of the cases an autosomal dominant inherited disease caused by mutations in the genes encoding for collagen type I, while rare mostly recessive forms are caused by defects in proteins interacting directly or indirectly post-translationally with collagen. The amazing dynamic of successive discovery of novel genes and associated novel pathways leading to OI and to OI-like syndromes undermines a traditional static classification. Hopefully, the increasing knowledge in pathophysiology will help in the near future to develop new therapeutic approaches beyond any formal categorization.
References
Weil UH. Osteogenesis imperfecta: historical background. Clin Orthop Relat Res. 1981;159:6–10.
Baljet B. Aspects of the history of osteogenesis imperfecta (Vrolik’s syndrome). Ann Anat. 2002;184:1–7.
De Rooy L, Knepper S. Forces of form: the Vrolik museum. Amsterdam; 2009.
O’Riordan JL, Bijvoet OL. Rickets before the discovery of vitamin D. Bonekey Rep. 2014;3:478.
Sillence DO, Senn A, Danks DM. Genetic heterogeneity in osteogenesis imperfecta. J Med Genet. 1979;16:101–16.
Chu ML, Williams CJ, Pepe G, Hirsch JL, Prockop DJ, Ramirez F. Internal deletion in a collagen gene in a perinatal lethal form of osteogenesis imperfecta. Nature. 1983;304:78–80.
Forlino A, Cabral WA, Barnes AM, Marini JC. New perspectives on osteogenesis imperfecta. Nat Rev Endocrinol. 2011;7:540–57.
Van Dijk FS, Sillence DO. Osteogenesis imperfecta: clinical diagnosis, nomenclature and severity assessment. Am J Med Genet A. 2014;164A:1470–81.
Rauch F, Lalic L, Roughley P, Glorieux FH. Genotype-phenotype correlations in nonlethal osteogenesis imperfecta caused by mutations in the helical domain of collagen type I. Eur J Hum Genet. 2010;18:642–7.
Semler O, Cheung MS, Glorieux FH, Rauch F. Wormian bones in osteogenesis imperfecta: correlation to clinical findings and genotype. Am J Med Genet A. 2010;152 A:1681–7.
Rauch F, Glorieux FH. Osteogenesis imperfecta. Lancet. 2004;363:1377–85.
Bishop N. Characterising and treating osteogenesis imperfecta. Early Hum Dev. 2010;86:743–6.
van Dijk FS, Cobben JM, Kariminejad A, Maugeri A, Nikkels PG, van Rijn RR, Pals G. Osteogenesis Imperfecta: a review with clinical examples. Mol Syndromol. 2011;2:1–20.
Makareeva E, Aviles NA, Leikin S. Chaperoning osteogenesis: new protein-folding disease paradigms. Trends Cell Biol. 2011;21:168–76.
Ishikawa Y, Bachinger HP. A molecular ensemble in the rER for procollagen maturation. Biochim Biophys Acta. 2013;1833:2479–91.
Avery NE, Bailey AJ. Restraining cross-links responsible for the mechanical properties of collagen fibers: natural and artificial. In: Fratzl P, editor. Collagen Structure and Mechanics. New-York: Springer; 2008. pp. 81–110.
Eyre DR, Weis MA. Bone collagen: new clues to its mineralization mechanism from recessive osteogenesis imperfecta. Calcif Tissue Int. 2013;93:338–47.
Morello R, Bertin TK, Chen Y, Hicks J, Tonachini L, Monticone M, Castagnola P, Rauch F, Glorieux FH, Vranka J, Bachinger HP, Pace JM, Schwarze U, Byers PH, Weis M, Fernandes RJ, Eyre DR, Yao Z, Boyce BF, Lee B. CRTAP is required for prolyl 3- hydroxylation and mutations cause recessive osteogenesis imperfecta. Cell. 2006;127:291–304.
Marini JC, Cabral WA, Barnes AM, Chang W. Components of the collagen prolyl 3-hydroxylation complex are crucial for normal bone development. Cell Cycle. 2007;6:1675–81.
Barnes AM, Chang W, Morello R, Cabral WA, Weis M, Eyre DR, Leikin S, Makareeva E, Kuznetsova N, Uveges TE, Ashok A, Flor AW, Mulvihill JJ, Wilson PL, Sundaram UT, Lee B, Marini JC. Deficiency of cartilage-associated protein in recessive lethal osteogenesis imperfecta. N Engl J Med. 2006;355:2757–64.
Baldridge D, Schwarze U, Morello R, Lennington J, Bertin TK, Pace JM, Pepin MG, Weis M, Eyre DR, Walsh J, Lambert D, Green A, Robinson H, Michelson M, Houge G, Lindman C, Martin J, Ward J, Lemyre E, Mitchell JJ, Krakow D, Rimoin DL, Cohn DH, Byers PH, Lee B. CRTAP and LEPRE1 mutations in recessive osteogenesis imperfecta. Hum Mutat. 2008;29:1435–42.
van Dijk FS, Nesbitt IM, Zwikstra EH, Nikkels PG, Piersma SR, Fratantoni SA, Jimenez CR, Huizer M, Morsman AC, Cobben JM, van Roij MH, Elting MW, Verbeke JI, Wijnaendts LC, Shaw NJ, Hogler W, McKeown C, Sistermans EA, Dalton A, Meijers-Heijboer H, Pals G. PPIB mutations cause severe osteogenesis imperfecta. Am J Hum Genet. 2009;85:521–7.
Pyott SM, Schwarze U, Christiansen HE, Pepin MG, Leistritz DF, Dineen R, Harris C, Burton BK, Angle B, Kim K, Sussman MD, Weis M, Eyre DR, Russell DW, McCarthy KJ, Steiner RD, Byers PH. Mutations in PPIB (cyclophilin B) delay type I procollagen chain association and result in perinatal lethal to moderate osteogenesis imperfecta phenotypes. Hum Mol Genet. 2011;20:1595–609.
Schwarze U, Cundy T, Pyott SM, Christiansen HE, Hegde MR, Bank RA, Pals G, Ankala A, Conneely K, Seaver L, Yandow SM, Raney E, Babovic-Vuksanovic D, Stoler J, Ben-Neriah Z, Segel R, Lieberman S, Siderius L, Al-Aqeel A, Hannibal M, Hudgins L, McPherson E, Clemens M, Sussman MD, Steiner RD, Mahan J, Smith R, Anyane-Yeboa K, Wynn J, Chong K, Uster T, Aftimos S, Sutton VR, Davis EC, Kim LS, Weis MA, Eyre D, Byers PH. Mutations in FKBP10, which result in Bruck syndrome and recessive forms of osteogenesis imperfecta, inhibit the hydroxylation of telopeptide lysines in bone collagen. Hum Mol Genet. 2013;22:1–17.
Marini JC, Blissett AR. New genes in bone development: what’s new in osteogenesis imperfecta. J Clin Endocrinol Metab. 2013;98:3095–103.
Glorieux FH, Moffatt P. Osteogenesis imperfecta, an ever-expanding conundrum. J Bone Miner Res. 2013;28:1519–22.
Plotkin H. Syndromes with congenital brittle bones. BMC Pediatr. 2004;4:16.
Van Dijk FS, Pals G, Van Rijn RR, Nikkels PG, Cobben JM. Classification of osteogenesis imperfecta revisited. Eur J Med Genet. 2010;53:1–5.
Warman ML, Cormier-Daire V, Hall C, Krakow D, Lachman R, LeMerrer M, Mortier G, Mundlos S, Nishimura G, Rimoin DL, Robertson S, Savarirayan R, Sillence D, Spranger J, Unger S, Zabel B, Superti-Furga A. Nosology and classification of genetic skeletal disorders: 2010 revision. Am J Med Genet A. 2011;155 A: 943–68.
Lazarus S, Moffatt P, Duncan EL, Thomas GP. A brilliant breakthrough in OI type V. Osteoporos Int. 2014;25:399–405.
Marini JC, Reich A, Smith SM. Osteogenesis imperfecta due to mutations in non-collagenous genes: lessons in the biology of bone formation. Curr Opin Pediatr. 2014;26:500–7.
Fahiminiya S, Majewski J, Al-Jallad H, Moffatt P, Mort J, Glorieux FH, Roschger P, Klaushofer K, Rauch F. Osteoporosis caused by mutations in PLS3: clinical and bone tissue characteristics. J Bone Miner Res. 2014;29:1805–14.
Rauch F, Moffatt P, Cheung M, Roughley P, Lalic L, Lund AM, Ramirez N, Fahiminiya S, Majewski J, Glorieux FH. Osteogenesis imperfecta type V: marked phenotypic variability despite the presence of the IFITM5 c.-14 C > T mutation in all patients. J Med Genet. 2013;50:21–4.
Homan EP, Rauch F, Grafe I, Lietman C, Doll JA, Dawson B, Bertin T, Napierala D, Morello R, Gibbs R, White L, Miki R, Cohn DH, Crawford S, Travers R, Glorieux FH, Lee B. Mutations in SERPINF1 cause osteogenesis imperfecta type VI. J Bone Miner Res. 2011;26:2798–803.
Christiansen HE, Schwarze U, Pyott SM, AlSwaid A, Balwi M A, Alrasheed S, Pepin MG, Weis MA, Eyre DR, Byers PH. Homozygosity for a missense mutation in SERPINH1, which encodes the collagen chaperone protein HSP47, results in severe recessive osteogenesis imperfecta. Am J Hum Genet. 2010;86:389–98.
Barnes AM, Cabral WA, Weis M, Makareeva E, Mertz EL, Leikin S, Eyre D, Trujillo C, Marini JC. Absence of FKBP10 in recessive type XI osteogenesis imperfecta leads to diminished collagen cross-linking and reduced collagen deposition in extracellular matrix. Hum Mutat. 2012;33:1589–98.
Puig-Hervas MT, Temtamy S, Aglan M, Valencia M, Martinez-Glez V, Ballesta-Martinez MJ, Lopez-Gonzalez V, Ashour AM, Amr K, Pulido V, Guillen-Navarro E, Lapunzina P, Caparros-Martin JA, Ruiz-Perez VL. Mutations in PLOD2 cause autosomal-recessive connective tissue disorders within the Bruck syndrome–osteogenesis imperfecta phenotypic spectrum. Hum Mutat. 2012;33:1444–9.
Hoyer-Kuhn H, Semler O, Schoenau E, Roschger P, Klaushofer K, Rauch F. Hyperosteoidosis and hypermineralization in the same bone: bone tissue analyses in a boy with a homozygous BMP1 mutation. Calcif Tissue Int. 2013;93:565–70.
Lapunzina P, Aglan M, Temtamy S, Caparros-Martin JA, Valencia M, Leton R, Martinez-Glez V, Elhossini R, Amr K, Vilaboa N, Ruiz-Perez VL. Identification of a frameshift mutation in osterix in a patient with recessive osteogenesis imperfecta. Am J Hum Genet. 2010;87:110–4.
Laine CM, Joeng KS, Campeau PM, Kiviranta R, Tarkkonen K, Grover M, Lu JT, Pekkinen M, Wessman M, Heino TJ, Nieminen-Pihala V, Aronen M, Laine T, Kroger H, Cole WG, Lehesjoki AE, Nevarez L, Krakow D, Curry CJ, Cohn DH, Gibbs RA, Lee BH, Makitie O. WNT1 mutations in early-onset osteoporosis and osteogenesis imperfecta. N Engl J Med. 2013;368:1809–16.
Shaheen R, Alazami AM, Alshammari MJ, Faqeih E, Alhashmi N, Mousa N, Alsinani A, Ansari S, Alzahrani F, Al-Owain M, Alzayed ZS, Alkuraya FS. Study of autosomal recessive osteogenesis imperfecta in Arabia reveals a novel locus defined by TMEM38B mutation. J Med Genet. 2012;49:630–5.
Symoens S, Malfait F, D’Hondt S, Callewaert B, Dheedene A, Steyaert W, Bachinger HP, De Paepe A, Kayserili H, Coucke PJ. Deficiency for the ER-stress transducer OASIS causes severe recessive osteogenesis imperfecta in humans. Orphanet J Rare Dis. 2013;8:154.
Acknowledgements
The authors are very grateful to Prof. Dr. Peter Fratzl (Max- Planck Institute of Colloids and Interfaces, Golm, Germany) for the long-standing cooperation and the helpful discussion during the preparation of this manuscript. The work at the Ludwig Boltzmann Institute of Osteology was supported by the AUVA (Austrian Social Insurance for Occupational Risk) and the WGKK (Social Health Insurance Vienna).
Conflict of interest
All authors state that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fratzl-Zelman, N., Misof, B., Roschger, P. et al. Classification of osteogenesis imperfecta. Wien Med Wochenschr 165, 264–270 (2015). https://doi.org/10.1007/s10354-015-0368-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10354-015-0368-3