
Summary
Background
The aim of this study was to evaluate the short- and long-term results and risk factors of liver surgery in patients over the age of 70 following liver resection for colorectal liver metastases.
Methods
A total of 650 patients with an average age of 63.8 ± 9.3 years were evaluated. We compared groups of patients younger and older than 70 years of age. Time of hospitalisation, 30-day postoperative morbidity and mortality, overall and recurrence-free survival, the number and largest diameter of metastases, small and large liver resections, and the interval between primary colorectal and liver surgery were evaluated according to the results of liver resections.
Results
Length of hospitalisation, 30-day postoperative morbidity and mortality, and long-term results did not differ between groups of patients. Pulmonary embolism and confusion had a higher incidence in patients ≥70 years old (p < 0.02 and 0.05, respectively). Diameter of the largest metastasis ≥50 mm was a negative prognostic factor for long-term results in patients ≥70 years old (p < 0.04, HR 1.7, 95% CI 1.0–2.9 and p < 0.03, HR 1.5, 95% CI 1.0–2.3, respectively). Large liver resections had worse long-term results in patients ≥70 years old (p < 0.01, HR 2.1, 95% CI 1.2–3.8 and p < 0.05, HR 1.5, 95% CI 0.9–2.3, respectively).
Conclusion
Our results confirm the safety of liver resections for colorectal liver metastases in elderly patients. Parenchymal sparing surgery should be the method of choice. Very early and intensive postoperative mobilisation and respiratory and mental rehabilitation is essential.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
-
The original article focuses on the short- and long-term results of liver resections for colorectal liver metastases in elderly patients.
-
It evaluates the risk factors and long-term results of liver surgery, with the aim of further optimising the surgical treatment of liver metastases in patients over the age of 70.
Introduction
The increase in the elderly population has been remarkable in recent years. The average age is increasing significantly in industrialised countries. Life expectancy at birth in the European Union (EU) was estimated to be 80.9 in 2017, reaching 83.5 for women and 78.3 for men. Between 2002 and 2017, life expectancy in the EU increased by 3.2 years, from 77.7 to 80.9 years (2.6 years for women and 3.8 years for men) [1]. The population is ageing all over the world, and the number of individuals over the age of 70 is expected to reach almost one quarter of the population in developed countries by 2025 [2].
Malignancies are generally diseases of the elderly due to a combination of the accumulation of lifestyle risk factors and long-term exposure to carcinogens. It is estimated that approximately 58% of all cancers and 69% of cancer deaths in the EU occur in people over the age of 70; in fact, the incidence of cancer is more than 11-times higher in people over 70. The most commonly diagnosed cancers worldwide are lung (1.4 million), breast (1.2 million) and colorectal cancers (1 million) [3].
Colorectal liver metastases (CLM) are a leading cause of cancer-related morbidity and mortality in the most developed countries. In approximately 20% of cases, CLM are diagnosed synchronously with primary colorectal carcinoma. In 30–50% of patients, CLM develop metachronously at various intervals after resection of the colorectal carcinoma. Radical liver resection is the only treatment that gives patients a chance of long-term survival. Unfortunately, only 15–20% of CLM are resectable at the time of diagnosis.
In many studies dealing with the epidemiology of ageing and CLM development, 33–50% of all patients with CLM were over the age of 70. However, only 8–20% of all patients who underwent surgery for CLM were over the age of 70 [4,5,6]. This difference could be due to the preference for palliative treatment of CLM in the geriatric population and considerations regarding radical liver surgery in older patients. The main reason for such a treatment approach could be a fear of cardiovascular, respiratory, renal, or metabolic comorbidities in elderly patients and the fact that advancing age carries a greater likelihood of decompensation during general anaesthesia and major liver surgery. When balancing the benefits of surgical resection for the treatment of CLM against the risks of surgery, many clinicians are reluctant to recommend liver resection in the elderly. However, the quality of life of older people in the population associated with their mental and physical activity has increased in recent years and is significantly better than it was a decade or more ago. For this reason, there is an expansion in the indication for liver surgery for the ageing population, and age should no longer be a limiting factor for liver resection.
The main aim of this study was to evaluate the long-term results of liver surgery in patients ≥70 years old in comparison to the results for younger patients. A secondary aim was to ascertain whether certain general risk factors of CLM play a role in the long-term results of liver surgery in elderly patients.
Methods
Approval for this study was received from the Institutional Ethics Committee. The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. We obtained written informed consent from all patients who participated in this study. 671 consecutive patients who underwent surgery to treat CLM between 2002 and 2020 were evaluated. 21 patients were excluded due to the incompleteness of data in medical records that were necessary for statistical processing; thus, 650 patients remained in the sample group. There were 177 patients in the ≥70 age group and 473 patients <70 years old. The average age of the entire group of patients was 63.8 ± 9.3 years, with a median of 64.7. The average ages of the ≥70 and <70 groups were 74.3 ± 3.6 and 58.4 ± 8.2 years, respectively. In the group of patients ≥70 years old, there were 102 men and 75 women; in the group <70 years old, there were 267 men and 206 women. The median for monitoring was 1.5 years (0–17.1 years).
In both groups, we evaluated the period of hospitalisation, 30-day postoperative morbidity and mortality, and overall (OS) and recurrence-free survival (RFS) following liver resection. There was an assessment of the impact of the number and largest diameter of CLM for a given patient, small (<3 liver segments) and large (≥3 segments) resections, and the interval between primary colonic surgery and surgery for CLM on the long-term results of liver surgery in both groups of patients. The average number and largest diameter of CLM in the group of patients ≥70 years old was 2.2 ± 1.6 and 4.2 ± 2.4 cm, respectively, and in the group <70 years old, 2.6 ± 2.1 and 3.9 ± 2.7 cm, respectively. Large liver resections were performed in 85 patients (48.1%) and small liver resections in 92 (51.9%) patients in the ≥70 age group; in 234 patients (49.4%) and 239 (50.6%) patients, respectively, in the <70 age group (Table 1). Patients were selected for each type of procedure by a multidisciplinary team according to the overall state of patients evaluated according to the anaesthesiological risk score (American Society of Anaesthesiologists, ASA), PACE test (physical activity facilitation for elders) and the number, diameter and location of the CLM in the liver on the basis of multidetector computed tomography (MDCT) with contrast enhancement, magnetic resonance imaging (MRI) or hybrid methods (positron-emission tomography with 18-fluorodeoxyglucose [FDG PET CT], positron-emission tomography with magnetic resonance imaging [PET MRI]). In indicated cases (insufficient future liver remnant volume, neoadjuvant oncological treatment, major liver surgery), we performed CT volumetry of the liver and a functional liver examination using an indocyanine green retention (ICG) test. The wishes of the patient concerning surgery were respected. Patients with ASA class IV, primary non-resectable CLM or with non-resectable extrahepatic metastases were excluded from the study.
The statistical analysis was performed using SAS software (SAS Institute Inc., Cary, NC, USA). Basic statistical data such as the average, standard deviation, variance, median, interquartile spread, and minimum and maximum were calculated for the measured parameters in the entire cohort and in individual groups and subgroups. The difference in continuous variables between the examined groups was tested using a Kruskal–Wallis Test. The analysis of overall survival (OS) and recurrence-free survival (RFS) rates was calculated using Kaplan–Meier survival curves. The impact of individual factors was tested using a log-rank test, Gehan–Wilcoxon test and Cox regression model. The statistically strongest cut-off for individual factors met the condition of highest attained score of the Cox regression model. Statistical significance was designated at the threshold alpha = 5%.
Results
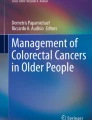
The length of hospitalisation was 11.3 ± 7.4 days for patients ≥70 and 11.1 ± 6.8 days for patients <70 (p < 0.9); 30-day postoperative morbidity was 14.6% and 13.4% (p < 0.8), and mortality 2.9% and 0.8% (p < 0.2) in patients ≥70 and <70 years old, respectively. The causes of mortality during the first 30 days in both groups were all cardiopulmonary insufficiency, except for one patient in the ≥70 age group who died of haemorrhagic shock. The highest mortality rate was observed after large liver resections: 4.6% and 2.3% (p < 0.1) of patients in the ≥70 and <70 groups, respectively. The causes of morbidity during the first 30 days did not differ between the two groups, with the exception of pulmonary embolism and confusion, for which patients ≥70 years of age had a higher incidence (p < 0.02 and 0.05 respectively; Table 2). The 1‑, 3‑ and 5‑year OS after resection was 90.6, 64.9 and 57.0%, respectively, for patients ≥70 years old and 91.6, 68.6 and 52.6%, respectively, for patients <70 years old (p < 0.7; hazard ratio, HR, 1.1; 95% confidence interval, CI, 0.7–1.5; Fig. 1). The 1‑, 3‑ and 5‑year RFS was 58.8, 22.1 and 16.7, respectively, for patients ≥70 and 58.7, 24.2 and 17.1 for patients <70 (p < 0.7, HR 1.0, 95% CI 0.8–1.3; Fig. 2). A diameter of the largest CLM ≥50 mm was a negative prognostic factor for OS and RFS for patients ≥70 years old (p < 0.04, HR 1.7, 95% CI 1.0–2.9, p < 0.03, HR 1.5, 95% CI 1.0–2.3, respectively; Figs. 3 and 4). Large liver resections also resulted in lower OS and RFS rates in patients ≥70 years old (p < 0.01, HR 2.1, 95% CI 1.2–3.8, p < 0.05, HR 1.5, 95% CI 0.9–2.3, respectively; Figs. 5 and 6). In contrast, the number of CLM, the interval between primary surgery for colorectal cancer and liver resection for CLM and small liver resections were not significant for the OS and RFS rates of both groups.

Overall survival of patients ≥70 years old after liver resection

Recurrence-free survival of patients ≥70 years old after liver resection

Overall survival depending on the diameter of colorectal liver metastases (CLM)

Recurrence-free survival depending on the diameter of colorectal liver metastases (CLM)

Overall survival depending on the type of liver resection

Recurrence-free survival depending on the type of liver resection
Discussion
Recent data clearly indicate that the number of people in our population over the age of 70 is increasing. In the Czech Republic, the percentage of the population over the age of 70 reached 18.7% in 2017. We can expect the number of elderly patients to increase further in the near future. These patients will create more and more cases in the area of hepatobiliary surgery. The problem is that older patients not only develop CLM, but also have other serious comorbidities that can affect surgical procedures.
Radical liver resection is the gold standard method for treatment of CLM. The 5‑year patient survival rate is between 35 and 60% [7, 8]. Untreated patients with CLM rarely survive longer than 1 year. Patients treated with modern oncological therapy without liver surgery can live for 22–24 months. The 30-day mortality rate for liver resections in specialised liver centres is below 5% due to the use of advanced resection techniques and modern trends in anaesthesiology and intensive care [9, 10].
Accurate preoperative diagnosis is extremely important in elderly patients, who often have various concomitant diseases. Modern techniques include ultrasonography and contrast-enhanced ultrasonography (CEUS), intraoperative ultrasonography, MDCT with contrast enhancement and volumetric evaluation, and MRI with a contrast agent. FDG PET CT or PET MRI are useful for staging the metastatic process. The use of this large array of diagnostic tools is important, especially for the differential diagnosis of haemangioma, focal steatosis, focal nodular hyperplasia and small lesions, and for staging liver tumours for accurate and careful preoperative patient selection to avoid unnecessary surgeries in elderly patients and to ensure that patients experience the maximum benefit from liver surgery. Radiodiagnostic methods are important for the evaluation of the number and location of liver tumours; for identifying possible hilar lymph node involvement, vascular invasion and the presence of extrahepatic disease; and for performing liver volumetry. All this information is essential for surgeons to assess tumour resectability and the anticipated extent of resection in elderly patients [11,12,13], for whom it is very important to perform a preoperative frailty evaluation as a risk factor of older patients undergoing liver surgery. Frailty evaluation is important not only for the actual operation, but also for ensuring comprehensive perioperative care for elderly patients. The goal is to reduce serious operative and postoperative complications associated with long hospitalisation, significant economic costs, a deterioration in the quality of life of elderly patients and their postoperative mortality [14, 15].
Careful preoperative evaluation of a patient’s state of health is very important, especially in elderly patients and before liver surgery, which had a 2.9% mortality rate in our group of elderly patients. An evaluation of cardiopulmonary status (standard chest x‑ray, electrocardiogram, echocardiography with estimation of ventricular kinetics and ejection fraction), a renal function test and complete blood chemistry tests should be performed as part of the basic examination of patients over the age of 70. In case of a positive medical history of coronary artery disease, additional cardiological examination is indicated. Preoperative assessment of the functional (ASA test), cognitive and emotional status of elderly patients using the PACE test and the Brief Fatigue Inventory (BFI) is also very important.
Special pathophysiological considerations have to be taken into account for elderly patients. As the body ages, the liver undergoes physiological changes, resulting in decreased size and reduced blood flow (by as much as 45%) in octogenarians. The number of hepatocytes is also reduced, and hepatocyte morphology and function deteriorate. The functional reserve of the liver and its regeneration capacity are diminished. The synthesis of proteins and clotting factors may be impaired. The acute-phase protein response is also inhibited. The inhibition of this response can be a cause of the increased rate of postoperative infection in elderly patients [16]. Postoperative hepatic failure after liver resection also occur more often in patients over the age of 70 [17, 18]. Therefore, liver cirrhosis (Child–Pugh stages B and C) and other conditions associated with seriously deteriorated liver function are contraindications for liver resection in the elderly. We recommend assessing liver function (e.g., indocyanine green retention test) in each patient over 70 years old before performing major liver surgery. If the retention rate of intravenous ICG application is less than 14% after 15 min, tolerance of large resection is good. If the retention rate is greater than 20%, the patient should not undergo major liver surgery. If the retention rate is between 14 and 20%, the elderly patient can undergo liver surgery if the future remnant liver volume (FRLV) will be more than 50% [19,20,21]. The FRLV is another very important factor for safe surgery in elderly patients. The FRLV is measured by three-dimensional CT volumetry, generally using a special software program. If the FRLV is lower than 30% for the healthy liver tissue, lower than 40% after extensive chemotherapy in patients with steatohepatitis or cirrhosis, staged procedures are indicated assuming the patient’s overall good condition [22, 23]. Because of this policy, we had zero liver insufficiency in the group of patients ≥70 and a rate of only 0.6% in the <70 age group.
The liver resection technique has changed significantly in recent years from the high blood demand finger-fracture or Kelly fracture techniques to more gentle liver resection using ultrasonic dissection devices, argon lasers, bipolar electrocoagulation devices and harmonic scalpel. In the majority of liver resections, blood transfusions are no longer necessary. Current techniques for liver surgery are liver-sparing procedures (in view of repeated liver procedures), with an emphasis on radical procedures with margin-negative R0 resections [24,25,26]. During parenchymal transection, we use either intermittent complete portal ischemia (Pringles manoeuvre should be applied in elderly patients for 15–20 min with 5–10 min of reperfusion) or selective portal ischemia (extrahepatic ligation or clip application). Resectable extrahepatic metastases (e.g., lung, nodular disease, peritoneal implants) are not contraindications for liver surgery in elderly patients. Current literature [27, 28] reports a median survival after liver surgery and extrahepatic disease resection of 20 months, 3‑year OS higher than 40% and 3‑year RFS around 12%. Untreated patients with CRLM and extrahepatic disease had a median survival of 6.4 months and a 3-year survival of 1% in case of non-resectable tumours [29,30,31]. Also, repeated liver resections in patients over the age of 70 in good health are not contraindicated and can be performed with acceptable morbidity and mortality rates that are very similar to those for primary liver surgeries [19, 32, 33].
Our study compared the short- and long-term results of liver resection in patients over 70 years old and in patients under the age of 70. The type of procedure was chosen based on each patient’s general physical and mental status. There were no significant differences in the 30-day mortality and morbidity rates between the two age groups except for a higher incidence of pulmonary embolism and postoperative confusion in patients over 70 years old. These phenomena are common in elderly patients in surgical units and most likely not specific to the liver procedures performed in our group of patients. However, in view of the significant incidence of pulmonary embolisms and postoperative confusion in patients ≥70 years old, it will be necessary to place even greater emphasis on very early postoperative mobilisation and respiratory and mental rehabilitation of elderly patients in addition to other prophylactic measures. We also recommend that artificial lung ventilation be terminated immediately after the end of the operation, unless essential for other reasons. Long-term results were worse for patients ≥70 years old with the presence of CLM ≥50 mm in diameter and large liver resections. It is a question whether this result is given by the shorter life expectancy of patients over the age of 70 or by the influence of the aforementioned risk factors.
However, our study has some limitations. It is a retrospective, monocentric study. In terms of risk factors, we monitored the basic clinical factors common in clinical practice. It would be of interest to take into account molecular risk factors too, which are, for example, histopathological and genetic characteristics of primary and secondary tumours and, in particular, serum indicators of tumour growth. We are currently working on this study. From the perspective of OS it would be helpful to censor the results in view of the death of patients with CLM, which would be appropriate for the long-term results of patients ≥70 years of age, where mortality for other reasons increases with age.
Conclusion
Liver surgery for CLM in elderly patients is feasible and safe and offers long-term survival with a high quality of life fully comparable with younger patients. However, liver resection in patients ≥70 years old should be tailored to the specific patient according to his or her overall state of health, liver function, FRLV and severity of various comorbidities, especially cardiopulmonary functions. Parenchymal sparing surgery should be method of choice in elderly patients. Early postoperative mobilisation and respiratory and mental rehabilitation are very important for these patients from the aspect of postoperative complications.
References
European Comission. Population: demography, population projections, census, asylum & migration. 2020. https://ec.europa.eu/eurostat/web/population.
Lee CW, Chan KM, Tsai HI, Hsieh YC, Lin CY, Kuo YC, et al. Hepatic resection for hepatocellular carcinoma in the octogenarian: Is it justified? Aging (Albany NY). 2019;11(5):1537–50. https://doi.org/10.18632/aging.101854.
Wabitsch S, Haber PK, Ekwelle N, Kästner A, Krenzien F, Benzing C, et al. Minimally invasive liver surgery in elderly patients—a single-center experience. J Surg Res. 2019;239:92–7. https://doi.org/10.1016/j.jss.2019.01.058.
Franco I, de’Angelis N, Canoui-Poitrine F, Le Roy B, Courtot L, Voron T, et al. Feasibility and safety of laparoscopic right colectomy in oldest-old patients with colon cancer: results of the CLIMHET study group. J Laparoendosc Adv Surg Tech A. 2018;28(11):1326–33. https://doi.org/10.1089/lap.2018.0040.
Zhao LY, Huo RR, Xiang X, Torzilli G, Zheng MH, Yang T, et al. Hepatic resection for elderly patients with hepatocellular carcinoma: a systematic review of more than 17,000 patients. Expert Rev Gastroenterol Hepatol. 2018;12(10):1059–68. https://doi.org/10.1080/17474124.2018.1517045.
Kuipers EJ, Grady WM, Lieberman D, Seufferlein T, Sung JJ, Boelens PG, et al. Colorectal cancer. Nat Rev Dis Primers. 2015;1:15065. https://doi.org/10.1038/nrdp.2015.65.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394:1467–80. https://doi.org/10.1016/S0140-6736(19)32319-0.
Kumari S, Semira Ch, Lee M, Lee B, Wong R, Nott L, et al. Resection of colorectal liver metastases in older patients. ANZ J Surg. 2020;90(5):796–801. https://doi.org/10.1111/ans.15750.
Jones BD, Jones R, Dunne DFJ, Astles T, Fenwick SW, Poston GJ, et al. Patient selection and perioperative optimisation in surgery for colorectal liver metastases. Eur Surg. 2018;50:87–92. https://doi.org/10.1007/s10353-018-0539-8.
Okamura Y, Sugiura T, Ito T, Yamamoto Y, Ashida R, Uesaka K. The short- and long-term outcomes in elderly patients with hepatocellular carcinoma after curative surgery: a case-controlled study with propensity score matching. Eur Surg Res. 2018;59(5–6):380–90. https://doi.org/10.1159/000494733.
Mastoraki A, Tsakali A, Papanikolaou IS, Danias N, Smyrniotis V, Arkadopoulos N. Outcome following major hepatic resection in the elderly patients. Clin Res Hepatol Gastroenterol. 2014;38(4):462–6. https://doi.org/10.1016/j.clinre.2014.01.009.
Mohamed F, Kallioinen M, Braun M, Fenwick S, Shackcloth M, Davies RJ. Management of colorectal cancer metastases to the liver, lung or peritoneum suitable for curative intent: summary of NICE guidance. Br J Surg. 2020; https://doi.org/10.1002/bjs.11609.
de’Angelis N, Baldini C, Brustia R, Pessaux P, Sommacale D, Laurent A, et al. Surgical and regional treatments for colorectal cancer metastases in older patients: a systematic review and meta-analysis. PLoS One. 2020;15(4):e230914. https://doi.org/10.1371/journal.pone.0230914.
Rashidian N, Alseidi A, Kirks RC. Cancers metastatic to the liver. Surg Clin North Am. 2020;100(3):551–63. https://doi.org/10.1016/j.suc.2020.02.005.
Saito Y, Morine Y, Shimada M. Mechanism of impairment on liver regeneration in elderly patients: role of hepatic stellate cell function. Hepatol Res. 2017;47(6):505–13. https://doi.org/10.1111/hepr.12872.
Treska V. Methods to increase future liver remnant volume in patients with primarily unresectable colorectal liver metastases: current state and future perspectives. Anticancer Res. 2016;36(5):2065–71.
Ko FC. Preoperative frailty evaluation: a promising risk-stratification tool in older adults undergoing general surgery. Clin Ther. 2019;41(3):387–99. https://doi.org/10.1016/j.clinthera.2019.01.014.
Costa G, Massa G, ERASO (Elderly Risk Assessment for Surgical Outcome) Collaborative Study Group. Frailty and emergency surgery in the elderly: protocol of a prospective, multicenter study in Italy for evaluating perioperative outcome (the FRAILESEL study). Updates Surg. 2018;70(1):97–104. https://doi.org/10.1007/s13304-018-0511-y.
Engstrand J, Nilsson H, Strömberg C, Jonas E, Freedman J. Colorectal cancer liver metastases—a population-based study on incidence, management and survival. BMC Cancer. 2018;18(1):78. https://doi.org/10.1186/s12885-017-3925-x.
Treska V, Skalicky T, Ferda J, Finek J, Liska V. Colorectal liver metastases surgery—the present and the perspectives. Rozhl Chir. 2014;93(12):568–71.
McNally SJ, Parks RW. Surgery for colorectal liver metastases. Dig Surg. 2013;30(4–6):337–47. https://doi.org/10.1159/000351442.
Drescher HK, Weiskirchen S, Weiskirchen R. Current status in testing for nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH). Cells. 2019;8(8):845. https://doi.org/10.3390/cells8080845.
Lang H, Baumgart J, Mittler J. Associating liver partition and portal vein ligation for staged hepatectomy in the treatment of colorectal liver metastases: current scenario. Dig Surg. 2018;35(4):294–302. https://doi.org/10.1159/000488097.
Mizuguchi T, Kawamoto M, Meguro M, Okita K, Ota S, Ishii M, et al. Impact of aging on morbidity and mortality after liver resection: a systematic review and meta-analysis. Surg Today. 2015;45(3):259–70. https://doi.org/10.1007/s00595-014-0863-y.
Stättner S. Contemporary liver surgery. Eur Surg. 2018;50:79–80. https://doi.org/10.1007/s10353-018-0533-1.
Zarzavadjian Le Bian A, Tabchouri N, Bennamoun M, Louvet C, Tubbax C, Sarran A, et al. After laparoscopic liver resection for colorectal liver metastases, age does not influence morbi-mortality. Surg Endosc. 2019;33(11):3704–10. https://doi.org/10.1007/s00464-019-06663-8.
Leal JN, Sadot E, Gonen M, Lichtman S, Kingham TP, Allen PJ, et al. Operative morbidity and survival following hepatectomy for colorectal liver metastasis in octogenarians: a contemporary case matched series. HPB (Oxford). 2017;19(2):162–9. https://doi.org/10.1016/j.hpb.2016.09.009.
Mise Y, Kopetz S, Mehran RJ, Aloia TA, Conrad C, Brudvik KW, et al. Is complete liver resection without resection of synchronous lung metastases justified? Ann Surg Oncol. 2015;22(5):1585–92. https://doi.org/10.1245/s10434-014-4207-3.
Kumari S, Semira Ch, Lee M, Lee B, Wong R, Nott L, et al. Resection of colorectal cancer liver metastases in older patients. ANZ J Surg. 2020;90(5):796–801. https://doi.org/10.1111/ans.15750.
Albertsmeier M, Engel A, Guba MO, Stintzing S, Schiergens TS, Schubert-Fritschle G, et al. Synchronous colorectal liver metastases: focus on the elderly. An effectiveness study from routine care. Langenbecks Arch Surg. 2017;402(8):1223–32. https://doi.org/10.1007/s00423-017-1611-8.
Kulik U, Framke T, Grosshennig A, Ceylan A, Bektas H, Klempnauer J, et al. Liver resection of colorectal liver metastases in elderly patients. World J Surg. 2011;35(9):2063–72. https://doi.org/10.1007/s00268-011-1180-x.
Angelsen JH, Viste A, Løes IM, Eide GE, Hoem D, Sorbye H, et al. Predictive factors for time to recurrence, treatment and post-recurrence survival in patients with initially resected colorectal liver metastases. World J Surg Oncol. 2015;13:328. https://doi.org/10.1186/s12957-015-0738-8.
Orcutt ST, Artinyan A, Li LT, et al. Postoperative mortality and need for transitional care following liver resection for metastatic disease in elderly patients: a population-level analysis of 4026 patients. HPB (Oxford). 2012;14:863–70. https://doi.org/10.1111/j.1477-2574.2012.00577.x.
Author contribution
V. Treska: conceptualization, methodology, writing, supervision; T. Skalicky: methodology, formal analysis; V. Liska: methodology, writing; J. Fichtl: methodology, resources; J. Bruha: resources.
Funding
The study was supported by Research Project PROGRES, P 36, Charles University in Prague
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
V. Treska, T. Skalicky, V. Liska, J. Fichtl and J. Bruha declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Treska, V., Skalicky, T., Liska, V. et al. Liver resections for colorectal liver metastases in elderly patients. Eur Surg 53, 66–74 (2021). https://doi.org/10.1007/s10353-020-00685-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10353-020-00685-6