
Abstract
The objective of this study was to analyze the effects of ceramic material thickness and resin cement shade on the color matching of ceramic veneers at the gray tooth structures. Seventy-two artificial maxillary right central incisor teeth (C2 shade) were prepared according to veneer tooth preparation in practice. Ceramic materials (LT, A2 shade, IPS e.max Press) were selected to fabricate the 0.50- and 0.75-mm thick veneers at the body region. The ceramic veneer specimens were bonded to the artificial teeth by the 6 shades of resin cements (Variolink Veneer: shades of HV+3, LV-2, LV-3; and RelyXTM Veneer: shades of WO, TR, A3). A clinical spectrophotometer (Crystaleye, Olympus) was used to measure the color parameters. The color differences (ΔE values) of ceramic veneers and A2 shade tab (Vitapan Classical, Vita) and C* ab values were calculated. The results of three-way ANOVA indicated that the ΔE values of ceramic veneer and A2 shade tab were significantly different in the thickness of ceramic materials, shades of resin cements, and measuring regions (p < 0.001). There were significant differences in 0.50-mm-thick ceramic veneers that exhibited higher ΔE values compared with veneers that were 0.75-mm thick. Tukey’s HSD test showed that the average ΔE values in body region were significantly smaller than that in cervical and incisal regions. The color matching of ceramic veneers was significantly influenced not only by the ceramic thickness and the resin cement shades but also the tooth regions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The popularity of porcelain veneers has been attributed to their superior optical property, increased translucency, and improved esthetics [1]. As a conservative technique, patients and clinician prefer these restorations due to minimal tooth reduction compared to other full coverage restorations [2].
The preparations of ceramic veneers are mostly limited to the enamel layer, in order to obtain a durable bonding interface and achieve greater clinical longevity [3]. Accordingly, the thickness of ceramic materials was restricted by the amount of tooth reduction. Ideally, a thin translucent ceramic bonded to a non-discolored tooth provides an esthetically pleasing ceramic veneer restoration [4]. If a ceramic veneer was placed on a gray underlying tooth structure, it might result in discoloration and shadowing of the veneer restorations [5, 6]. Therefore, clinicians should take care to achieve a good color matching for ceramic veneers due to the material’s limited thickness and high translucency [7].
Color matching in dentistry has traditionally been performed with shade guides according to the color of healthy adjacent natural tooth [8]. Because the desirable color of ceramic veneers and the color of underlying tooth structure cannot always be chosen by the clinicians, the shades and thickness of ceramic materials and the shades of resin cements become important variables in manipulating the final color of ceramic veneers [7, 9]. In practice, the corresponding try-in pastes in the resin cement system can be used to evaluate the color matching of veneers and predict the final esthetic effects of veneers [10]. When the resultant color of the ceramic veneers does not match the expected color, the different shades of resin cements could be expected to modify the final color of ceramic veneer to achieve the good color matching [5, 7, 9, 11].
The purpose of this study was to analyze the effect of the thickness of ceramic materials and resin cement shades on the color matching of ceramic veneers at the gray tooth structures. The null hypothesis was that the final color of ceramic veneers would not be affected by ceramic thickness and resin cement shades.
Materials and methods
One heat-pressed glass-ceramic material and six shades of resin cements were evaluated in this study. The flowchart of experimental design is in Fig. 1.

Flowchart of experiment design
Fabrication of ceramic veneers
Seventy-two artificial maxillary right central incisor teeth (C2 shade, Yamahachi, Yamahachi Dental Mfg. Co., Japan) were used to simulate the natural discolored teeth. The root section of artificial tooth was fabricated with self-curing acrylic resin (Shanghai Medical Equipment Co., LTD., China) to position the artificial tooth in standard maxillary model (Nisshin Corporation, Japan). These artificial teeth were prepared using a veneer teeth preparatory kit (NTI-Set 1752, NTI-Kahla GmbH, Germany) according to the clinical procedure. The tooth reductions were achieved to 0.3, 0.5, and 0.7 mm at the cervical, body, and incisal regions, respectively. Preparation depth was evaluated by relining a silicone index (Silagum putty soft, DMG, Hamburg, Germany) of uncut tooth structure. The incisal finish line of artificial tooth was prepared for a window design and the cervical margin was placed at the crown part of the cemento-enamel junction about 1.0 mm.
The ceramic veneer samples were of the same morphology and curve on the buccal surface using the method of impression duplicating wax patterns. The buccal surface morphology of the artificial teeth and root was duplicated with impression materials (Honigum and Silagum, DMG, Hamburg, Germany) (Impression I). After the teeth preparation, the molten wax was put into impression I, and the prepared artificial tooth was inserted into the impression. The artificial tooth and duplicating wax pattern were taken out together after the wax solidified. The wax patterns were checked with the loupe (Shanghai optical instrument factory, China) and repaired when the edges were defective. The wax patterns were then imbedded and pressed with ceramic ingots (IPS e.Max, LT, A2 shade, Ivoclar, Vivadent, Liechtenstein) according to the manufacturer’s instructions. The ceramic veneer samples were the specimens of the 0.50-mm-thick group.
A ceramic veneer sample of the 0.50-mm-thick group was selected and fixed on the prepared resin abutment tooth with 0.25-mm-thick double-faced adhesive tape. The edges of ceramic veneer and resin abutment were sealed with the wax. Then, the buccal surface impression of the combination ceramic veneer with resin teeth and the root section was taken with impression materials (Honigum and Silagum, DMG, Hamburg, Germany) (Impression II). The wax patterns of 0.75-mm-thick group were fabricated using Impression II and imbedded and pressed using the above methods.
The ceramic veneer specimen was adjusted to seat on its corresponding artificial teeth. All ceramic specimens were cleaned using the ultrasonic in distilled water for 10 min. The buccal surfaces of ceramic veneers were glazed with colorless glaze liquid (Ivoclar Vivadent, Liechtenstein) according to the manufacturer’s instructions. The thickness of ceramic veneers in the cervical, body, and incisal area was measured by the thickness gauge with accuracy 0.01 mm (Weihai measuring implement factory co., LTD, China).
The bonding of ceramic veneer
Thirty-six ceramic veneer samples in each thickness category were randomly divided into six groups (n = 6) according to the color parameters of ceramic veneers before cementation. Six resin cement shades were selected from two resin cement systems, corresponding to shades LV-3, LV-2, HV+3 (Variolink Veneer, Ivoclar Vivadent, Liechtenstein) and WO, TR, A3 (RelyX™ Veneer, 3M ESPE, USA). The bonding process of each resin cement system was undertaken according to the manufacturer’s instructions. The resin cement was placed on the bonding surface of the ceramic veneers and gently pressed onto the resin artificial teeth. A light-polymerizing unit (Mini LED™, Satelec, France) was used to cure for 5 s. The excess resin cements were removed and then curing continued for 40 s. The bonded specimens were stored in physiological saline for 24 h at 37 °C to ensure complete polymerization.
Color measurement
The right maxillary lateral incisor and left maxillary central incisor in the maxillary standard model (Nisshin Corporation, Japan) were replaced by resin artificial teeth (A2 shade, Yamahachi, Yamahachi dental Mfg., co. Japan). To simulate the clinical situation, the maxillary standard model with ceramic veneer samples was mounted in a black inspection box (Crystaleye, Olympus, Japan) that simulates the dark background of the oral cavity. A dental spectrophotometer (Crystaleye, Olympus, Japan) was used to measure the color parameters of specimens in the cervical, body, and incisal regions: (1) the prepared resin artificial teeth, (2) the ceramic veneer specimens before the bonding treatment, and (3) the ceramic veneer specimens after cementation.
Calculation of color difference
The color differences were calculated using the following formula: ΔE* = [(L*1 − L*A2)2 + (a*1 − a*A2)2 + (b*1 − b*A2)2]1/2; the chroma of the ceramic veneer specimens were calculated by the following formula: C*ab = (a*2 + b*2)1/2.
In order to determine the color effect of resin cement on the ceramic veneers, the ∆E value of 3.3 was considered the clinically unacceptable threshold in this study [12–14].
Statistical analysis
The three-way ANOVA was used to analyze the main effect of the thickness of ceramic materials, the shade of resin cements, and the measuring regions on the color differences (ΔE values) of ceramic veneers and A2 shade tab (Vita Classical Shade Guide, Vita Zahnfabrik, Germany). Tukey’s HSD test was used to evaluate within-group effects of the cement shades and the color measuring regions on the ΔE values at each ceramic thickness (α = 0.05).
Results
The average thickness of ceramic veneers in 0.50-mm-thick group is 0.34, 0.51, and 0.73 mm in cervical, body, and incisal region, respectively (Table 1). The thickness of the 0.75-mm-thick specimens was about more than 0.20 mm in three regions compared with 0.50-mm-thick group. The L*, a*, and b* values of the seventy-two prepared artificial teeth were smaller standard deviations and 95% confidence intervals in Table 2. The color parameters of the shade guide for the A2 shade tab in the Crystaleye software (Crystaleye Application Ver. 1.4, Olympus, Japan) are as follows: cervical L*71.9, a*1.4, b*18.5; body L*72.7, a*1.0, b*18.8; incisal L*68.2, a*0.3, b*14.5.
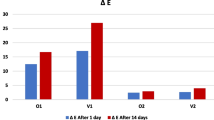
Distributions of the L* and C*ab values of 0.50- and 0.75-mm-thick specimens are presented in Figs. 2, 3. The color parameters of ceramic veneers cemented with LV-3, LV-2 or TR shade resin cements have similar distribution of L* and C*ab values. The color parameters of ceramic veneers cemented with WO shade resin cement were located in the high L* value or low C*ab value region. The L* and C*ab values of the ceramic veneers cemented by HV+3 shade resin cement were close to the values of A2 shade tab in body region. The ΔE values between ceramic veneers and A2 shade tab are presented in Table 3. These values ranged from 1.9 to 6.5 for the 0.5 mm-thick ceramic veneer specimens and from 1.0 to 5.9 for the 0.75-mm-thick specimens. The highest ΔE value was observed in the cervical regions of 0.50-mm-thick cemented with LV-3 shade, whereas the 0.75-mm-thick ceramic veneers cemented with the WO shade exhibited the lowest ΔE value in the body regions.

The distribution of L* and C*ab of 0.50-mm-thick ceramic specimens in the cervical, body, and incisal regions

The distribution of L* and C*ab of 0.75-mm-thick ceramic specimens in the cervical, body, and incisal regions
The results of three-way ANOVA showed that the ΔE values were influenced by ceramic thickness, shade of resin cements, and measuring regions, as well as the interaction terms of these three variables (p < 0.001). The results of Tukey’s HSD test showed that the mean ΔE value in body region was significantly smaller than that in cervical and incisal regions (Table 3).
Discussion
The null hypothesis that the final color of ceramic veneers would not be affected by ceramic thickness and resin cement shades was rejected. The results of the present study indicate that the color differences between ceramic veneers and A2 shade tab are influenced by the ceramic thickness and shades of resin cements.
Most of previous studies in vitro have evaluated the effect of ceramic thickness and cement shade on the resulting color of veneer restoration, in which disc-shaped specimens were fabricated to represent the middle third region of veneer restorations [6, 7, 15, 16]. Although the disc-shaped specimens were very convenient for the sample fabrication and color measurement, the shape of specimens was obviously different from the veneer restorations in practices. The overall resulting color of veneer restorations included the optical properties of the cervical, body, and incisal regions [17]. Therefore, the test should be done on restorations to simulate the geometry of a tooth and the surface texture [18]. In this study, the ceramic veneer specimens were fabricated to the same surface shape and uniform thickness (Table 1).
The color parameters of ceramic veneer specimens were influenced by ceramic thickness and resin cement shades in different veneer regions. In the incisal region, the ceramic veneers presented more brightness and higher chroma than the A2 shade tab, except that LV-3 shade produced lower L* values. In the cervical and body region, the ceramic veneers presented lower brighter values than the A2 shade tab, regardless of resin cement shades, whereas the chroma yielded different changes due to the different shades of resin cement. The C*ab values of ceramic veneers bonded by the WO shades obviously decrease. It was noted that the distributions of L*–C*ab of 0.50- and 0.75-mm-thick group had similar tendency in Figs. 2 and 3.
The color differences of ceramic veneers and A2 shade tab were changed by using the different shades of resin cement (Table 3). For the LV-3 and LV-2 cement shades, the color differences were above the clinically unacceptable threshold (ΔE > 3.3), regardless of ceramic thickness and veneer regions. Similarly, ceramic veneers cemented with the TR or A3 shade cements produced ΔE values greater than 3.3, except in the body region. These showed that the color of the gray abutment tooth controlled the final color outcome of the restoration, when ceramic veneers bonded by these shades of resin cement [2, 11]. The matching colors (ΔE < 3.3) were obtained from the 0.50-mm-thick ceramic with HV+3 shade resin cement and 0.75-mm-thick ceramic with HV+3 or WO shade of resin cement. The results were probably due to the fact that these cements contained some opacity components [16]. Previous studies showed that the WO shade or white opaque cements resulted in a significant color change of ceramic veneer specimens [7, 11, 19]. Therefore, the WO and HV+3 cement shades seem to be more effective in masking discolored abutment teeth [19–21].
The effect of resin cement shades on the final color of ceramic veneers was influenced by the thickness of ceramic materials [16]. Although some previous studies reported that the cement shade had little effect on the final color of crowns, the thickness of ceramic specimens ranged from 1.0 to 2.0 mm in these studies [5, 21–23]. However, thickness of veneer restorations ranges usually from 0.5 to 1.0 mm in the clinical application [7, 20]. Ceramic materials showed more translucency with decreasing thickness [11, 19, 23]. Transparent ceramic veneer allowed more light to enter and increased scattering, indicating that the underlying color can have a significant impact on the final color [11, 24]. In the present study, there were significant differences between the 0.50-mm-thick ceramic veneers that exhibited higher ΔE values when compared with 0.75-mm-thick veneers. This was in agreement with previous investigators who reported that the 0.5-mm-thick ceramics showed higher ΔE values between the shade tab and the ceramic veneers than did ceramics that were 1.0 mm in thickness [20].
The color matching of ceramic veneers with A2 shade tab was also influenced by the measuring regions of ceramic veneer. The mean ΔE values in the body region were significantly smaller than the cervical or incisal region (Table 3). The optical properties of tooth were change in different regions along the tooth axis of the labial surface of the central incisors [25]. The color parameters of tooth in the incisal were easily affected by the dark environment at the oral cavity because the incisal site is most often translucent. The ΔE values in the incisal region might be the result of the difference in translucency between ceramic materials and A2 shade tab. In the cervical region, the color parameters of underlying tooth showed that the magnitude of L* was lower in the cervical area and that C*ab values were the highest in the cervical area [26]. In addition, the ceramic thickness was the thinnest in the cervical site. Therefore, the color of darker abutment tooth might influence the esthetic and color outcome of the final veneers in the cervical region [11, 20].
The limitations of this study were that only A2 shade heat-pressed glass–ceramic materials and C2 shade discolored teeth were investigated. In addition, the composite resin teeth were used to stimulate the discolored abutment tooth. However, the optical properties of the resin artificial teeth differ from those of a natural tooth. The influence of different ceramic materials and different abutment tooth color should be considered in future researches.
Conclusions
Within the limitation of this in vitro study, the following conclusions were drawn:
-
1.
The color matching of ceramic veneers was significantly influenced by the ceramic thickness, the resin cement shades, and the tooth regions. Clinicians should pay more attention to the color matching of ceramic veneers in the cervical and incisal regions.
-
2.
The WO and HV+3 shades of resin cements can effectively shield the influence of gray shade of abutment on veneer restorations.
References
Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. Porcelain veneers: a review of the literature. J Dent. 2000;28:163–77.
Dozic A, Tsagkari M, Khashayar G, Aboushelib M. Color management of porcelain veneers: influence of dentin and resin cement colors. Quintessence Int. 2010;41:567–73.
Layton DM, Clarke M, Walton TR. A systematic review and meta-analysis of the survival of feldspathic porcelain veneers over 5 and 10 years. Int J Prosthodont. 2012;25:590–603.
Barghi N, McAlister E. Porcelain for veneers. J Esthet Dent. 1998;10:191–7.
Chaiyabutr Y, Kois JC, Lebeau D, Nunokawa G. Effect of abutment tooth color, cement color, and ceramic thickness on the resulting optical color of a CAD/CAM glass-ceramic lithium disilicate-reinforced crown. J Prosthet Dent. 2011;105:83–90.
Azer SS, Rosenstiel SF, Seghi RR, Johnston WM. Effect of substrate shades on the color of ceramic laminate veneers. J Prosthet Dent. 2011;106:179–83.
Turgut S, Bagis B. Effect of resin cement and ceramic thickness on final color of laminate veneers: an in vitro study. J Prosthet Dent. 2013;109:179–86.
Hassel AJ, Koke U, Schmitter M, Beck J, Rammelsberg P. Clinical effect of different shade guide systems on the tooth shades of ceramic-veneered restorations. Int J Prosthodont. 2005;18:422–6.
Niu E, Agustin M, Douglas RD. Color match of machinable lithium disilicate ceramics: effects of cement color and thickness. J Prosthet Dent. 2013;111:42–50.
Xu B, Chen X, Li R, Wang Y, Li Q. Agreement of try-in pastes and the corresponding luting composites on the final color of ceramic veneers. J Prosthodont. 2014;23:308–12.
Kurklu D, Azer SS, Yilmaz B, Johnston WM. Porcelain thickness and cement shade effects on the colour and translucency of porcelain veneering materials. J Dent. 2013;41:1043–50.
Ruyter IE, Nilner K, Moller B. Color stability of dental composite resin materials for crown and bridge veneers. Dent Mater. 1987;3:246–51.
Corciolani G, Vichi A, Louca C, Ferrari M. Color match of two different ceramic systems to selected shades of one shade guide. J Prosthet Dent. 2011;105:171–6.
Douglas RD, Steinhauer TJ, Wee AG. Intraoral determination of the tolerance of dentists for perceptibility and acceptability of shade mismatch. J Prosthet Dent. 2007;97:200–8.
Turgut S, Bagis B. Colour stability of laminate veneers: an in vitro study. J Dent. 2011;39:e57–64.
Xing W, Jiang T, Ma X, Liang S, Wang Z, Sa Y, Wang Y. Evaluation of the esthetic effect of resin cements and try-in pastes on ceromer veneers. J Dent. 2010;38:e87–94.
Alghazzawi TF, Lemons J, Liu PR, Essig ME, Janowski GM. Evaluation of the optical properties of CAD-CAM generated yttria-stabilized zirconia and glass-ceramic laminate veneers. J Prosthet Dent. 2012;107:300–8.
Wang H, Xiong F, Zhenhua L. Influence of varied surface texture of dentin porcelain on optical properties of porcelain specimens. J Prosthet Dent. 2011;105:242–8.
Turgut S, Bagis B, Turkaslan SS, Bagis YH. Effect of ultraviolet aging on translucency of resin-cemented ceramic veneers: an in vitro study. J Prosthodont. 2014;23:39–44.
Turgut S, Bagis B, Ayaz EA. Achieving the desired colour in discoloured teeth, using leucite-based cad-cam laminate systems. J Dent. 2014;42:68–74.
Chang J, Da Silva JD, Sakai M, Kristiansen J, Ishikawa-Nagai S. The optical effect of composite luting cement on all ceramic crowns. J Dent. 2009;37:937–43.
Kilinc E, Antonson SA, Hardigan PC, Kesercioglu A. Resin cement color stability and its influence on the final shade of all-ceramics. J Dent. 2011;39:e30–6.
Vichi A, Ferrari M, Davidson CL. Influence of ceramic and cement thickness on the masking of various types of opaque posts. J Prosthet Dent. 2000;83:412–7.
Stevenson B, Ibbetson R. The effect of the substructure on the colour of samples/restorations veneered with ceramic: a literature review. J Dent. 2010;38:361–8.
Joiner A. Tooth colour: a review of the literature. J Dent. 2004;32:3–12.
Hasegawa A, Ikeda I, Kawaguchi S. Color and translucency of in vivo natural central incisors. J Prosthet Dent. 2000;83:418–23.
Acknowledgements
The authors thank Dr Shao-Pu Zhang for his help in the preparation of the manuscript. The authors appreciate the technical supports provided by Chang-Jun Guan and Da-Hai Li. Our study was partly funded by Health and Family Planning Commission of Dalian Municipality (No: WSJ/KJC-2014-JL-77).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Xing, W., Chen, X., Ren, D. et al. The effect of ceramic thickness and resin cement shades on the color matching of ceramic veneers in discolored teeth. Odontology 105, 460–466 (2017). https://doi.org/10.1007/s10266-016-0287-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-016-0287-9