
Abstract
Age-related hearing loss (ARHL) is a devastating public health issue. To successfully address ARHL using existing and future treatments, it is imperative to detect the earliest signs of age-related auditory decline and understand the mechanisms driving it. Here, we explore early signs of age-related auditory decline by characterizing cochlear function in 199 ears aged 10–65 years, all of which had clinically defined normal hearing (i.e., behavioral thresholds ≤ 25 dB HL from .25 to 8 kHz bilaterally) and no history of noise exposure. We characterized cochlear function by measuring behavioral thresholds in two paradigms (traditional audiometric thresholds from .25 to 8 kHz and Békésy tracking thresholds from .125 to 20 kHz) and distortion product otoacoustic emission (DPOAE) growth functions at f2 = 2, 4, and 8 kHz. Behavioral thresholds through a standard clinical frequency range (up to 8 kHz) showed statistically, but not clinically, significant declines across increasing decades of life. In contrast, DPOAE growth measured in the same frequency range showed clear declines as early 30 years of age, particularly across moderate stimulus levels (L2 = 25–45 dB SPL). These substantial declines in DPOAE growth were not fully explained by differences in behavioral thresholds measured in the same frequency region. Additionally, high-frequency Békésy tracking thresholds above ~11.2 kHz showed frank declines with increasing age. Collectively, these results suggest that early age-related cochlear decline (1) begins as early as the third or fourth decade of life, (2) is greatest in the cochlear base but apparent through the length of the cochlear partition, (3) cannot be detected fully by traditional clinical measures, and (4) is likely due to a complex mix of etiologies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
INTRODUCTION
The number of adults in the USA with age-related hearing loss (ARHL) — approximately 30 million (Lin et al. 2011; Blackwell et al. 2014; Hoffman et al. 2017) — makes ARHL a public health emergency. A primary site of age-related auditory decline is the cochlea. As such, new gene and cell therapies for treatment of hearing loss primarily target the cochlea and offer hope for preservation and restoration of cochlear function (Müller and Barr-Gillespie 2015; Crowson et al. 2017; Cunningham and Tucci 2017; Shibata et al. 2020). However, the efficacy of these therapies will be limited by the extent to which age-related cochlear decline can be successfully detected and differentially diagnosed in its earliest stages (Oshima et al. 2010). This early and differential diagnosis is challenging, and sensitive clinical protocols for this purpose are lacking.
A significant complication is the heterogeneity of ARHL, which can result from multiple etiologies. Considerable debate has ensued over which pathologies are most prevalent in aging ears. Schuknecht (1964) identified four primary cochlear pathologies contributing to ARHL: sensory (damage or loss of sensory hair cells), neural (damage or loss of spiral ganglion neurons), metabolic (decline of cochlear electrochemistry), and cochlear conductive (decline in mechanical function within the cochlear partition). Schuknecht later emphasized the influence of metabolic and neural dysfunction — rather than sensory cell dysfunction — in the aging ear (Schuknecht and Gacek 1993). This idea was supported by evidence that quiet-raised animals demonstrated metabolic decline and atrophy of the stria vascularis with age, sometimes in the absence of significant outer hair cell loss (Gratton et al. 1997; Spicer and Schulte 2002; Mills and Schmiedt 2004). However, recent work using advanced histological techniques has called this into question, suggesting that sensory cell loss is also prominent in aged ears (Wu et al. 2020).
Non-invasive, early detection of age-related auditory decline is also challenging. Studies in humans have demonstrated that several pathologies contributing to ARHL, such as metabolic or sensory decline, are associated with specific configurations of the behavioral audiogram (Schuknecht 1964; Dubno et al. 2013). Unfortunately, using audiogram patterns to distinguish between cochlear pathologies is not possible until age-related decline is evident in behavioral thresholds, which are notoriously insensitive to subtle changes in the auditory system. For example, behavioral thresholds can remain completely unaffected even after a significant decline in the cochlear synaptic population (Kujawa and Liberman 2009). Additionally, measures of outer hair cell function such as otoacoustic emissions (OAEs) — low-level sounds that arise from outer hair cells (OHCs) in the cochlea and can be recorded non-invasively in the ear canal (Kemp 1978) — show frank declines earlier in life than behavioral thresholds (Poling et al. 2014; Hunter et al. 2020).
Here, we assessed the influence of early aging on a specific OAE response: distortion product (DP)OAE growth functions. DPOAEs are produced when the ear is stimulated simultaneously with two tones at frequencies f1 and f2 (f2 > f1); growth functions measure DPOAEs across a range of stimulation levels. DPOAE growth functions are thought to assess the growth of distortion associated with the non-linear interaction of cochlear mechanical activity due to the two stimulus tones. DPOAE growth functions have an approximate relationship with measures of basilar membrane displacement amplitude at low levels (Withnell and Yates 1998). However, the relationship between BM and DPOAE growth is complex; while BM displacement is measured at a single cochlear location, DPOAE growth is affected by the increase in amplitude at each place within the generation region, as well as the spread of excitation along the cochlear partition as the non-linear region expands (Kim et al. 1980; Martin et al. 2009, 2011). Previous work has extracted certain characteristics of the DPOAE growth functions, including threshold and slope (as a function of stimulus level), to predict behavioral thresholds (Kummer et al. 1998; Gorga et al. 2003), characterize cochlear aging (Ortmann and Abdala 2016; Abdala et al. 2018), and differentiate between cochlear pathologies (Gates et al. 2002; Ueberfuhr et al. 2016).
We examined age-related changes in DPOAE growth patterns in 199 individuals between 10 and 65 years of age. Participants were selected to have behavioral thresholds (≤ 25 dB HL from 0.25 to 8 kHz) and no self-reported history of noise exposure to explore signs of auditory aging in otherwise clinically unremarkable individuals. Our primary objectives were to determine if age-related auditory decline was present in ears without hearing loss and, if so, to characterize the impact of that aging on DPOAE growth. Our secondary objective was to use characteristics of DPOAE growth functions to examine potential underlying cochlear pathology.
METHODS
Participants
Data presented here are from a subset of participants from a larger study that investigated age-related changes in auditory function (Hearing Assessment Reformulation Project [HARP]). Data from 199 individuals (139 F, 60 M; age range 10–65 years) were included as part of this analysis out of 401 participants in the original data set. To be included in this analysis, participants from the original data set had to have (1) audiometric thresholds ≤ 25 dB HL at 0.25, 0.5, 1, 2, 3, 4, 6, and 8 kHz bilaterally; (2) no self-reported history of significant noise exposure or otologic disease/surgery; (3) an unremarkable otoscopic examination and normal immittance results; and (4) DPOAE growth function(s) that met noise floor and signal-to-noise ratio criteria for at least one f2 test frequency (discussed later). Apart from traditional audiometric thresholds, which were measured bilaterally, all other measures were collected in a single “test ear” of each participant. The test ear was defined as the ear with better audiometric thresholds from 0.25 to 8 kHz, or a randomly selected ear if thresholds between ears were equivalent. All procedures were conducted in accordance with the guidelines of Northwestern University’s Institutional Review Board.
For the purposes of this analysis, participants who met the inclusion criteria were separated into five categorical age groups: 10–19 years, 20–29 years, 30–39 years, 40–49 years, and 50 + years. These age groups were selected to examine changes in peripheral auditory function across each decade of life and to attempt to roughly equalize group sizes, particularly across the older age groups. Only three participants above the age of 59 (aged 61, 65, and 65, respectively) met the inclusion criteria and therefore were included in the 50 + age group. The distribution of participant ages within a categorical age group tended to be relatively uniform. However, the youngest group (10–19 years) skewed slightly towards the upper end, and the second youngest group (20–29 years) skewed slightly towards the lower end. Figure 1 shows these distributions. The race and ethnicity of participants in the original data set reflected the population of Cook County, IL, at the time of data collection. Because our analysis includes only a subset of the original participants, our sample includes more female, White, and not Hispanic or Latino individuals than the population of Cook County. Demographic and age grouping information from participants in our sample is shown in Table 1.

Age (in years) distributions of participants within a categorical age group tended to be relatively uniform, though the two youngest groups (10–19 years, 20–20 years) tended to skew slightly left and right, respectively
The primary measures of interest for this analysis included (1) audiometric thresholds measured through 8 kHz; (2) Békésy tracking thresholds measured through 20 kHz; and (3) DPOAE growth functions measured with discrete tones at f2 frequencies 2, 4, and 8 kHz. Tracking threshold data and other DPOAE data (specifically, DPOAE-grams recorded using a different measurement protocol) from a subset of the original 401 participants have previously been reported (see Lee et al. 2012 and Poling et al. 2014, respectively). Tracking thresholds reported previously by Lee et al. (2012) are reported again because this analysis uses a different subset of participants (based on the inclusion criteria described above). Differences between the subset of participants in this study and previously published data are primarily a result of the audiometric threshold criterion used for this analysis. Audiometric threshold and DPOAE growth function data have not previously been reported.
Instrumentation, Calibration, and Procedure
Audiometric thresholds were obtained from 0.25 to 8 kHz in 5-dB steps bilaterally using the modified Hughson-Westlake procedure (Hughson and Westlake 1944) and a commercial clinical audiometer (Interacoustics AA220) calibrated to ANSI S3.6–1996 specifications. Békésy tracking thresholds were obtained between 0.125 and 20 kHz in 2-dB steps using a custom-modified Békésy tracking program described in Lee et al. (2012). All measurements were made in a double-walled sound-treated booth.
Detailed instrumentation and calibration descriptions for both Békésy tracking and DPOAE measurements are available in Lee et al. (2012) and Poling et al. (2014), respectively, and are summarized here. Stimuli used for both Békésy tracking and DPOAE measurements were calibrated using a depth compensation procedure to reduce the effects of standing waves in the ear canal (Souza et al. 2014). For Békésy tracking measurements, signal generation and threshold logging were done using custom-written software on an Apple Macintosh computer, and digital-to-analog and analog-to-digital conversion was done with a MOTU 828 MkII audio interface (44.1 kHz, 24 bits). For DPOAE measurements, signal generation and data collection were done using custom software on a PC (EMAV; Neely and Liu 1993); D/A and A/D conversion was done with an Echo Layla 3G audio interface (44.1 kHz, 24 bits) connected to a PC. For both Békésy tracking measures and DPOAE recordings, signals were routed through a custom-built headphone amplifier to custom MB Quart 13.01HX tweeters and delivered to the ear using an ER10B + probe assembly (Etymōtic Research, Elk Grove Village, IL) sealed in the ear canal with a foam tip.
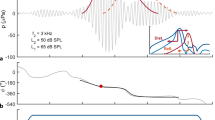
DPOAE growth functions were measured using discrete tone stimuli at three f2 frequencies: 2, 4, and 8 kHz with an f2/f1 ratio of 1.30, 1.23, and 1.22 at these three frequencies, respectively. These f2/f1 ratios were chosen to reduce the effects of interstimulus suppression (Withnell and Yates 1998) and to reduce the interference between the two DPOAE components. L1 was fixed at 60 dB SPL while L2 varied in level from 0 to 60 dB SPL in 2-dB steps. The specific strategy of holding L1 constant and varying L2 was adopted from Withnell and Yates (1998), as DPOAE growth curves measured using this paradigm most closely approximate basilar membrane displacement measured at the characteristic frequency, at least at low levels (< 40 dB SPL).
DPOAE Analysis
DPOAEs were averaged in the time domain over at least eight sets of measurements to improve the signal-to-noise (SNR) ratio. DPOAE (2f1-f2) amplitudes were estimated using a fast Fourier transform (FFT). Noise floors at a given f2/L2 combination were estimated using frequency bins adjacent to the 2f1-f2 DPOAE. Because DPOAE growth functions were measured using discrete tone stimuli, DPOAE components were not separated prior to analysis. This limitation will be further considered in “Discussion”; however, it was expected that the distortion (short-latency) component of the DPOAE would dominate the response in most ears, regardless of age, at least at stimulus levels above ~ 30 dB SPL (e.g., Mauermann and Kollmeier 2004). For an individual DPOAE growth function to be included in this analysis, data were required to meet noise floor (NF) and SNR criteria at a given f2 frequency. Specifically, a growth function was required to have an absolute NF level < 0 dB SPL at a minimum of 21 out of 31 L2 levels (21-point rule) and an SNR (DPOAE to NF level) ≥ 3 dB SPL at a minimum of 15 out of 31 L2 levels (15-point rule). These criteria ensured that DPOAE growth functions with many aberrant points were not included in analysis, while still allowing us to characterize growth function behavior at low L2 levels.
In order to maximize the number of growth functions included in our analysis, individual data points that did not meet the above criteria (SNR ≥ 3 dB SPL and NF < 0 dB SPL) were considered for a procedure to estimate the missing value. Here, we refer to this procedure as interpolation. A data point qualified for interpolation when the DPOAE data from two surrounding L2 levels at the same f2 frequency (L2 + 2 dB SPL and L2 − 2 dB SPL, respectively) met the NF and SNR criteria described above. When this criterion was met, the DPOAE level was interpolated by averaging the DPOAE level at the two surrounding L2 levels. DPOAE data that did not meet the criterion for interpolation remained unchanged. Data points (NF and/or OAE level) were interpolated for 192 participants; however, only 0.4 % of the total data points (across all participants) were interpolated and all but five participants had fewer than 10 interpolated points out of 31 total data points. As expected, over half (~ 61 %) of all interpolated data points were at L2 levels < 25 dB SPL. The number of points interpolated was essentially equal for all three f2 frequencies. After interpolation, a final cleaning procedure discarded the entire growth function of a participant at a given f2 frequency if either the 15- and/or 21-point rules were not met. This cleaning procedure left a total of 568 growth functions (188, 195, and 185 from f2 = 2, 4, and 8 kHz, respectively) from the 199 participants for analysis.
DPOAE Growth Function Characterization and Analysis
DPOAE growth functions were characterized using the segmented package (v. 1.2) (Muggeo 2003, 2017) in the R statistical system (v. 4.0.2) (R Core Team 2020), which fits regression models with continuous piecewise relationships. Specifically, we used a three-segment linear fit to characterize growth functions. We selected the piecewise linear fit for quantifying growth function data because it is easily interpretable and allows for the quantification and comparison of different aspects of the functions across age groups and frequencies. Specifically, the fit provides estimates of the function slope across each of the three linear segments and provides an estimate of breakpoints, or L2 level(s) at which there is a change in the slope of the growth function, as schematized in Fig. 2. This allowed us to characterize cochlear response growth across three ranges of input levels (L2): low level (L2 = ~ 0–25 dB SPL), moderate level (L2 = ~ 25–45 dB SPL), and high level (L2 = ~ 45–60 dB SPL). This fitting procedure also allowed us to explore if the boundaries representing these three level ranges varied between age groups.

Schematic of the slopes and breakpoints of the DPOAE growth function estimated by the three-segment piecewise linear fitting
Two fitting procedures — both utilizing the linear piecewise fitting — were used to characterize DPOAE growth functions. The first procedure fit a piecewise linear function to the aggregate DPOAE growth function data within a given age group at a given f2 frequency. This fit allowed for group-level comparisons and general characterization of growth functions across age groups. DPOAE levels were converted from dB SPL to pascals before the data were fit. Data were subset by age group and f2 frequency, respectively, and fit using the segmented function with a linear model. The simple linear regression model predicted DPOAE level (Pa) by L2 level (dB SPL). The segmented function allows the user to specify up to two initial breakpoint values from which to begin breakpoint estimation. Because our average DPOAE growth data did not visually indicate major differences in breakpoint values between age groups or across frequencies, starting values of L2 = 25 and L2 = 45 were chosen for all fits. We further specified that the segmented function implement a bootstrap restarting algorithm (Wood 2001) with 50 bootstrap samples (as recommended by the author of the segmented package for the estimation of two breakpoints) and case resampling (i.e., replacement). Estimated regression slopes, breakpoints, and standard error values for each fit were extracted for analysis.
The second procedure fit a piecewise linear function to individual DPOAE growth functions from each participant at each frequency. These individual fits allowed for greater examination of growth function differences within age groups. Additionally, exploring data at the individual level allowed us to take the first steps towards understanding the potential clinical utility of DPOAE growth functions. The second fit procedure followed the same general steps as the first with the exception of also subsetting data by each participant (in addition to age group and f2 frequency) prior to the fitting. Estimated regression slopes, breakpoints, and standard error values were extracted for analysis.
RESULTS
Behavioral Thresholds
Traditional Audiometric Thresholds (0.25–8 kHz)
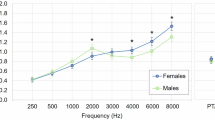
Average audiometric thresholds from 0.25 to 8 kHz of each age group are shown in panel A of Fig. 3. The inset figure shows the same average audiometric thresholds with a smaller y axis for easier visualization of group differences. Only thresholds from the test ear of each participant were included. Our inclusion criteria dictated that participants have audiometric thresholds ≤ 25 dB HL at all test frequencies from 0.25 to 8 kHz bilaterally to be included in this analysis. Thus, all participants, regardless of their age, would be clinically classified as having normal hearing (Olusanya et al. 2019).

Average behavioral thresholds tended to decline with increasing age, particularly at frequencies > 8 kHz. All error bars indicate + / − 1 standard deviation from the mean. Thresholds are jittered at each test frequency for easier visualization. A Average audiometric thresholds measured using a modified Hughson-Westlake procedure from .25 to 8 kHz decline with age, though these declines are not clinically significant. The dotted line indicates 25 dB HL, which indicates both our inclusion criteria for this analysis and a standard cutoff for defining normal hearing over the .25–8 kHz frequency range. Inset shows the same thresholds with a condensed y axis for better visualization of age group differences. B Average behavioral thresholds measured using a modified Békésy tracking technique also decline with age, particularly at frequencies > 10 kHz. Inset shows the same thresholds with a linear x axis for better visualization of age group differences in the high frequencies. Note that 105 dB SPL represents the maximum output limitations of the equipment and is equivalent to “no response”
Even so, audiometric thresholds differed between age groups within the clinically normal range. A two-way ANOVA (frequency × age group) indicated a significant main effect of frequency (F(7, 2511) = 10.28, p < 0.001) and a significant main effect of age group (F(4, 8047) = 57.64, p < 0.001). There was not a significant interaction between frequency and age group (F(28, 1171) = 1.20, p = 0.22). Post hoc pairwise multiple comparisons using a Bonferroni correction indicated significant differences in audiometric thresholds between the youngest group (10–19 years) and the three oldest groups (30–39 years, 40–49 years, and 50 + years) and the second youngest group (20–29 years) and the same three oldest groups. Additionally, there were significant differences in thresholds between the 30–39-year group and the two oldest age groups. The effect size of threshold differences between age groups were estimated using Cohen’s d and ranged from small (d = − 0.29) between the youngest group (10–19 years) and 30–39-year group to large (d = − 0.84) between the youngest group and 50 + year group.
Despite these statistical differences, the average threshold differences between age groups were within the range of test–retest reliability of clinical behavioral audiometry (± 5–10 dB) (Studebaker 1967). Specifically, differences in average threshold between the youngest (10–19 years) and 30–39-year group were ≤ 5 dB at all test frequencies. The most extreme average threshold difference was 8.75 dB at 6 kHz between the youngest (10–19 years) and oldest group (50 + years). The largest threshold differences between age groups at the DPOAE f2 frequencies of interest (2 kHz, 4 kHz, and 8 kHz) were 3 dB, 7 dB, and 6.5 dB, respectively.
Békésy Tracking Thresholds (0.125–20 kHz)
Average Békésy tracking thresholds from 0.125 to 20 kHz of each age group are shown in panel B of Fig. 3; the inset of this figure shows the same data with a linear x axis for better visualization of high-frequency differences between age groups. These data are a subset of tracking thresholds previously published in Lee et al. (2012). They are included here because they are a different subset of participants, as some participants in Lee et al. (2012) did not meet our audiometric inclusion criteria (thresholds ≤ 25 dB HL from 0.25 to 8 kHz). Note that 105 dB SPL represents the maximum output limitations of the equipment and is equivalent to “no response.” Missing data were discarded prior to analysis.
To reduce the number of group comparisons, and therefore to increase statistical power, we collapsed tracking threshold data across five frequency ranges: low (0.125–0.75 kHz), mid (1–3 kHz), high (4–10 kHz), extended high (11.2–15 kHz), and ultra-high (16–20 kHz). The Kruskal–Wallis H test was used to assess for differences in tracking thresholds between age groups within each frequency grouping. Results indicated no significant differences between age groups in the low (0.125–0.75 kHz) (H(4) = 0.94, p = 0.92) and mid (1–3 kHz) (H(4) = 1.98, p = 0.74) frequency ranges. There were statistically significant differences between age groups in the high, extended-high, and ultra-high-frequency ranges (H(4) = 47.57, p < 0.001; H(4) = 98.93, p < 0.001; and H(4) = 99.75, p < 0.001, respectively). As such, post hoc Mann–Whitney tests with Bonferroni correction (to account for the number of comparisons) were performed to determine age group differences in the high, extended high, and ultra-high-frequency ranges. Table 2 shows all post hoc test results; a summary is provided here. Briefly, differences in tracking thresholds between age groups increased with frequency. For example, in the high and extended-high-frequency ranges (4–10 kHz and 11.2–15 kHz, respectively), tracking thresholds of the two youngest groups were statistically significantly better than those of the two oldest groups. Results in the ultra-high frequencies (16–20 kHz) followed a similar pattern. However, differences between age groups were more prominent, with significant differences in thresholds emerging even between the two youngest groups. Specifically, the ultra-high-frequency thresholds of the youngest group (10–19 years, M = 69.35) were statistically significantly better than the ultra-high-frequency thresholds of all other age groups, including the 20–29-year group (M = 105), U = 982, p = 0.001. The median threshold and interquartile range (IQR) in this frequency range of the two oldest age groups (40–49 years, 50 + years) were 105 and 0, respectively, indicating that most participants in these age groups did not have a measurable threshold within this frequency range (note that 105 dB SPL corresponds to no response).
Though differences in tracking thresholds between age groups at higher frequencies (> ~ 11.2 kHz) are notable, differences at standard clinical test frequencies (< 8 kHz) were similar to audiometric threshold results. Differences in tracking thresholds between age groups within the standard clinical frequency range were even smaller than differences in audiometric thresholds, likely because of methodological differences between behavioral threshold measurement procedures. First, stimuli for the two procedures were calibrated using different methods, as specified in “Methods.” Additionally, audiometric thresholds were measured with a 5-dB step size, whereas tracking thresholds were measured with a 2-dB step size. Average tracking thresholds of all five age groups fell within a normative range (based on norms established by our laboratory) through 11.2 kHz. Additionally, differences in tracking thresholds between age groups within this frequency range were modest. The largest threshold differences between age groups at the DPOAE f2 frequencies of interest (2 kHz, 4 kHz, and 8 kHz) were 1 dB, 5 dB, and 10.8 dB, respectively.
DPOAE Growth Functions
Average DPOAE growth functions and noise floors of each of the five age groups at f2 = 2, 4, and 8 kHz are displayed in Fig. 4. While average DPOAE levels are similar across age groups at L2 levels below ~ 25 dB SPL, differences between age groups emerge at higher L2 levels. Specifically, the slope of the average DPOAE growth functions between L2 levels of ~ 25–45 dB SPL appears to systematically decline with increasing age. This effect is most apparent when f2 = 8 kHz. Additionally, the average DPOAE growth functions of all age groups display non-monotonic behavior at 2 kHz and 4 kHz, as evidenced by a characteristic bend in the function above an L2 level of ~ 50 dB SPL. In contrast, only the average DPOAE growth functions of the youngest two age groups (10–19 years, 20–29 years) display this non-monotonic behavior at 8 kHz. The DPOAE growth functions of the remaining age groups (30 + years) appear to show monotonic behavior at this frequency.

Average distortion product otoacoustic emission (DPOAE) growth functions decline considerably with increasing age at all three frequencies tested: f2 = 2 kHz (left), 4 kHz (middle), and 8 kHz (right). Average noise floor levels are similar between age groups and are shown at the bottom of each panel. Average DPOAE and noise floor levels are plotted as a function of L2. Error bars indicate + / − 1 standard error of the mean
Individual DPOAE growth functions across each age group and f2 frequency are displayed in Fig. 5. There is notable variability between individual DPOAE growth functions within each age group, particularly as frequency increases. However, the tendency for DPOAE growth to decline with age is still apparent. Variability in DPOAE growth is greatest for the two youngest age groups. Note that our inclusion criteria required that most — not all — points along an individual growth function meet noise floor (21 of 31 points) and SNR (15 of 31 points) criteria. Thus, it was possible for a growth function to be included in the analysis even with several aberrant points.

Distortion product otoacoustic emission (DPOAE) growth functions from individual participants (thin lines) show considerable variability across all age groups at all three frequencies tested: f2 = 2 kHz (top row), 4 kHz (middle row), and 8 kHz (bottom row). However, the general tendency for DPOAE growth to decline with increasing age is still apparent. Average DPOAE growth functions for each age group and frequency combination are overlaid with thick lines. Individual (thin, gray lines) and average (thick, gray lines) noise floors are similar between all age groups
Group Level Three-Segment Linear Fitting
To characterize group-level differences between our five age groups, aggregate DPOAE growth function data from each age group at each f2 frequency were fit with a three-segment continuous piecewise function. This fitting procedure provides estimates of the slopes of each of the three linear segments of the function and of the two breakpoints, or L2 levels that correspond to a point of change between the segments. Figure 6 shows the resulting fitted values plotted against the average measured DPOAE growth functions from each age group. The fitted functions closely match the average measured data (in Pa) for all age groups.

Fitted DPOAE growth functions (solid, colored lines) closely match average measured DPOAE growth functions (gray, dashed lines) from each age group at each f2 frequency. DPOAE growth functions were fit using a three-segment piecewise linear function, which provided estimates of the slope of three linear segments of the function as well as two breakpoints that corresponded to slope changepoints between segments
Estimated breakpoints and associated 95 % confidence intervals were extracted from each fitted function and are shown in Fig. 7. The estimated breakpoints and associated 95 % confidence intervals suggest that both Break 1 and Break 2 are similar across all age groups within a given f2 frequency, though variability increases with frequency and age. For example, at f2 = 2 kHz, the estimated Break 1 and Break 2 values are similar between age groups. In the youngest group (10–19 years), Break 1 and Break 2 are L2 = 32.91 dB SPL and 54.83 dB SPL, respectively. This is similar to the oldest group (50 + years), in which breakpoint estimates are L2 = 28.95 dB SPL and 52.00 dB SPL. However, the confidence interval widens with increasing age for both Break 1 and Break 2 estimates at this test frequency, suggesting increased variability, particularly for the two oldest age groups. Additionally, the confidence interval around Break 1 and Break 2 widens for all age groups as f2 frequency increases. For example, the confidence interval around the youngest age group (10–19 years) Break 1 estimate at f2 = 2 kHz spans less than 5 dB SPL; in contrast, the confidence interval around the Break 1 estimate of the same age group at f2 = 8 kHz is almost 9 dB SPL. The confidence interval around the Break 1 estimate for the oldest age group (50 + years) spans ~ 8.5 dB at f2 = 2 kHz and increases to over 20 dB at f2 = 8 kHz.

Estimated breakpoints from the average fitted DPOAE level growth functions are similar across all age groups at each f2 frequency, as all 95 % confidence intervals overlap (indicated by error bars). However, the variability in estimated breakpoint values increases with frequency and age
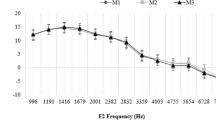
Estimated slope values were also extracted from each fitted function. Slope 2 shows clear and systematic declines with increasing age at all f2 frequencies, as shown in Fig. 8. The estimated 95 % confidence intervals around Slope 2 of the three oldest age groups (30–39 years, 40–49 years, and 50 + years) do not overlap with those of the youngest two age groups at 2 kHz and at 4 kHz. This suggests a consistent difference in Slope 2 between the youngest and oldest age groups at these two frequencies. At f2 = 8 kHz, even the confidence intervals of the two youngest age groups (10–19 years, 20–29 years) are non-overlapping, with further declines in Slope 2 with increasing age. In contrast, Slopes 1 and 3 were similar across all age groups at a given f2 frequency, though there is variability across all frequencies and age groups. Because there were no systematic trends, Slope 1 and Slope 3 estimates and associated standard errors at each f2 frequency for each age group are shown in Table 3. Remarkably, relative to the youngest age group, the percentage decline in Slope 2 reaches 40–60 % by age 30–39 years. These declines are exaggerated with increasing age, with the percentage decline reaching 65–75 % across all f2 frequencies by age 40 + .

Estimated Slope 2 values from the average fitted DPOAE level growth functions decline with increasing age at each f2 frequency. The 95 % confidence intervals (indicated by error bars) of the three oldest age groups (30–39, 40–49, and 50 + years, respectively) do not overlap with the confidence interval around the youngest age group (10–19 years), suggesting a systematic and consistent difference in Slope 2 between age groups. Slope 2 declines by 40–60 % (relative to the youngest group) by age 30–39 years. In contrast, Slopes 1 and 3 were similar across all age groups (shown in Table 3)
Taken together, these results suggest that the general configuration of DPOAE growth functions is similar across all age groups, with the exception of Slope 2, which systematically declines with age. The first breakpoint (Break 1) occurs roughly between L2 = 25–35 dB SPL across all frequencies and age groups, suggesting that Slope 1 represents DPOAE growth at low L2 levels, including at threshold (where the measured DPOAE rises ≥ 3 dB above the noise floor). Though we did not directly estimate the threshold of the DPOAE growth functions, we would expect differences in threshold to manifest as a difference between age groups in Slope 1 and/or Break 1. The second breakpoint (Break 2) occurs roughly between L2 = 40–55 dB SPL and defines the upper boundary of Slope 2. Because Break 2 is also similar between age groups at each frequency, this further indicates that DPOAE growth functions flatten with increasing age without a shift in the entire function.
Individual Three-Segment Linear Fittings
For an outcome measure such as DPOAE growth functions to have clinical utility for diagnosing ARHL, it must be able to detect and differentiate early signs of ARHL within an individual in a monitoring application and between individuals when a contrast against norms is used. To that end, we repeated the same three-segment linear fitting procedure on each participant’s DPOAE growth function(s) and extracted estimated slope (Slope 1, Slope 2, Slope 3) and breakpoint (Break 1, Break 2) values from each participant. Ultimately, this procedure was beneficial for several reasons. First, it allowed us to glean the efficacy of using a three-segment linear fit to characterize growth functions at the individual level. Second, it allowed us to characterize the individual variability in DPOAE growth. Third, it allowed us to make statistical comparisons of slopes and breakpoints across age groups.
Of the 568 total growth functions included in the analysis after data cleaning, only two were unable to be fit using the segmented function with the selected fitting parameters. One of these growth functions was from a participant in the youngest age group (10–19 years) at 8 kHz; the other growth function was from a participant in the 30–39-year age group at 2 kHz. This left 566 growth functions for analysis (187, 195, and 184 at f2 = 2, 4, and 8 kHz, respectively). Despite the aforementioned variability in measured growth functions, the fitted functions closely matched the measured data across all age groups and frequencies. Fitted functions generally fell into one of three subjectively defined categories: (1) the fitted function closely matched the measured data and had the same general configuration as the average data, with or without measured data that was smooth (Fig. 9, panels A and B); (2) the fitted function closely matched the measured data but did not have the same configuration as the average data (Fig. 9, panel C); and (3) at least a portion of the fitted function deviated from the measured data and did not have the same configuration as the average data (Fig. 9, panel D). Visual inspection of fitted vs. measured growth function data from each participant indicated that the vast majority of fitted functions (> 90 %) both closely matched the measured data and had the same general configuration as the average data. The remaining 10 % of fitted growth functions were split equally between categories 2 and 3. There were no noticeable differences in the quality of fit or configuration of the growth functions across age groups or frequencies. No fitted functions were removed prior to analysis, primarily because deviations from fit were small, and because deviations in configuration encapsulate the normal variability of measured DPOAE growth functions between individuals.

Fitted individual DPOAE growth functions (dotted lines) generally matched the measured data (solid lines) closely across all age groups and frequencies. Fitted growth functions generally fell into one of three subjectively defined categories; exemplars from each of these categories are shown here. (A) The fitted function closely matches the measured data and follows the average configuration pattern (category 1). (B) The fitted function closely matches the measured data and follows the average configuration pattern (category 1), even when the measured data are not smooth. (C) The fitted function closely matches the measured data but does not follow the average configuration pattern (category 2). (D) The fitted function deviates from the measured data across a portion of the function (category 3). Over 90 % of the 566 fitted functions fell into category 1, indicating that most fitted functions closely matched the measured data
The breakpoint values were extracted from the individual fits. Figure 10 shows violin plots of the estimated breakpoint values from each participant. Results followed the same trends as the average data, in that neither Break 1 nor Break 2 was different between age groups. Specifically, both breakpoints were not significantly different between age groups at any f2 frequency, as assessed using a Kruskal–Wallis H test. Results indicated no significant differences in the value of Break 1 between age groups at f2 = 2 kHz (H(4) = 1.54, p = 0.82), 4 kHz (H(4) = 3.42, p = 0.49), or 8 kHz (H(4) = 2.16, p = 0.71). Results further indicated no significant differences in the value of Break 2 between age groups at f2 = 2 kHz (H(4) = 5.74, p = 0.22), 4 kHz (H(4) = 4.26, p = 0.37), or 8 kHz (H(4) = 7.64, p = 0.11). However, the breakpoint data from individual fits highlight the variability in DPOAE growth between individuals. The interquartile range (IQR) of each breakpoint value at each f2 frequency spanned a relatively small range (~ 6.58–10.14 dB SPL). However, every age group had outliers.

Estimated Break 1 (top panels) and Break 2 (bottom panels) values from the fitted DPOAE growth functions of individual participants are similar across age groups at each f2 frequency, consistent with results from the average fitted data (shown in Fig. 7). There were no statistically significant differences in Break 1 or Break 2 between age groups at any f2 frequency. These data further highlight the variability in DPOAE growth between individuals across all age groups. Dots represent outlying values as defined by 1.5 times the interquartile range
Slope values from individual fits were also extracted and are shown in Fig. 11. Again, Kruskal–Wallis H tests were used to assess for differences in slopes between age groups at each f2 frequency. As expected based on results from the average data, results indicated significant differences in the value of Slope 2 between age groups at all three f2 frequencies: 2 kHz (H(4) = 17.48, p = 0.002), 4 kHz (H(4) = 22.60, p < 0.001), and 8 kHz (H(4) = 19.07, p = 0.001).

*p < 0.05; **p < 0.01; ***p < 0.001. Estimated Slope 1 (top panels), Slope 2 (middle panels), and Slope 3 (bottom panels) values from individual participants in each age group at each f2 frequency highlight both the variability in individual DPOAE growth functions and the consistent declines in Slope 2 with age. Like the average fitted estimates of Slope 2 (shown in Fig. 8), Slope 2 values from the individual fitted data consistently decline with age at all three f2 frequencies. These declines were statistically significant, specifically between the youngest groups (10–19 and 20–29 years) and the two oldest groups (40–49 and 50 + years). In contrast to the average fitted estimates of Slopes 1 and 3 (Table 3), which showed no meaningful differences between age groups, there were several statistically significant differences in Slope 1 and 3 values between age groups in the fitted data from individual participants. These statistically significant differences also tended to be between the two youngest (10–19 and 20–29 years) and two oldest (40–49 and 50 + years) age groups. However, the differences in Slopes 1 and 3 were not as consistent as the differences in Slope 2 and highlight the variability in individual DPOAE growth. Dots represent outlying values as defined by 1.5 times the interquartile range
Post hoc Mann–Whitney tests with Bonferroni corrections to account for the number of comparisons were performed to examine age group differences at each f2 frequency. Results with adjusted p-values are shown in Table 4. In summary, the youngest age group (10–19 years) had statistically significantly larger Slope 2 values than the two oldest age groups (40–49 years, 50 + years) at all three f2 frequencies. Additionally, the 20–29-year age group had statistically significantly larger Slope 2 values than the two oldest age groups at 4 kHz and 8 kHz. Effect sizes of Slope 2 differences were estimated using Cohen’s d. Effect sizes of the difference between the youngest (10–19 years) and 40–49-year age group ranged from small (d = 0.44) at 4 kHz, to medium (d = 0.67 and d = 0.75) at 2 kHz and 8 kHz, respectively. Effect sizes of the differences between the youngest (10–19 years) and oldest (50 + years) age groups ranged from small (d = 0.42) at 4 kHz to medium (d = 0.71) and large (d = 0.80) at 8 kHz.
Slopes 1 and 3 were also compared between age groups using the same methodology. Specifically, Kruskal–Wallis H tests were used to assess for group differences across each f2 frequency. In contrast to the results from the averaged fitting data, results suggested statistically significant differences in Slope 1 values between age groups at all three frequencies: 2 kHz (H(4) = 12.99, p = 0.01), 4 kHz (H(4) = 17.17, p = 0.002), and 8 kHz (H(4) = 20.78, p < 0.001). Results further suggested statistically significant differences in Slope 3 values between age groups at 4 kHz (H(4) = 21.26, p < 0.001) and 8 kHz (H(4) = 12.30, p = 0.02), but not at 2 kHz.
Post hoc Mann–Whitney tests with Bonferroni corrections were performed, as appropriate, to determine differences in Slopes 1 and 3 between each age group at each frequency. In short, the youngest age group tended to have higher Slope 1 values than the oldest age group (50 + years), particularly as frequency increased. This was inconsistent with findings from the average fitting, which suggested no differences in Slope 1 between age groups. However, differences between age groups were not as consistent as they were for Slope 2. More specifically, at 2 kHz, post hoc testing suggested that there were no statistically significant differences in Slope 1 values between any age group. This null result may be due to the weakly significant global effect at 2 kHz coupled with the use of a conservative p-value correction. At 4 kHz, post hoc testing revealed that the Slope 1 values of the youngest age group (10–19 years, M = 0.10 μPa/dB SPL) were statistically significantly larger than those of the oldest age group (50 + years, M = 0.03 μPa/dB SPL) only (U = 853, p = 0.007). The effect size of this difference, assessed using Cohen’s d, was medium (d = 0.50). At 8 kHz, post hoc testing suggested that the Slope 1 values of the youngest age group (10–19 years, M = 0.13 μPa/dB SPL) were statistically significantly larger than Slope 1 values from the 40–49-year age group (M = 0.02 μPa/dB SPL), U = 870, p = 0.001, and the 50 + year age group (M = 0.02 μPa/dB SPL), U = 677, p = 0.01. The effect sizes of these differences were small (d = 0.21) and negligible (d < 0.20), respectively.
Additionally, the youngest two age groups (10–19 years, 20–29 years) tended to have smaller Slope 3 values than the two oldest age groups (40–49 years, 50 + years). Though these findings are inconsistent with the results from the average fitting, it is not unexpected given that the average DPOAE growth data highlight a “flattening” of growth in the older age groups above ~ 40 dB SPL. At 4 kHz, the only statistically significant differences in the Slope 3 value were between the two youngest age groups (10–19 years, M = − 0.45; 20–29 years, M = − 0.61) and 40–49-year age group (M = − 0.16); the younger groups have a smaller Slope 3 than the older (U = 379, p = 0.04 and U = 560, p = 0.001, respectively). At 8 kHz, only the 20–29-year age group (M = − 0.36) had a statistically significantly lower Slope 3 than the oldest age group (50 + years, M = − 0.05), U = 432, p = 0.02.
In summary, the declines in Slope 2 with increasing age were consistent between the average and individual fitted data. Specifically, Slope 2 showed systematic declines with increasing age in both cases (shown in Figs. 8 and 11, respectively). The decline was apparent across all tested frequencies and increased both with age and with f2 frequency. In contrast, the average fitted estimates of Slope 1 and Slope 3 (shown in Table 3) indicated no meaningful differences between age groups, whereas there were several statistically significant differences in Slopes 1 and 3 in the individual fitted estimates. These statistically significant differences also tended to be between the youngest (10–19 and/or 20–29 years) and oldest (40–49 and/or 50 + years) age groups. However, the differences in Slopes 1 and 3 were not as consistent or systematic as the differences in Slope 2. Given that the statistically significant differences appear only at some frequencies between some age groups, and only in the individual (and not average) fitted data, these differences may primarily reflect the variability in individual DPOAE growth functions and fitting procedures.
Behavioral Thresholds and DPOAE Growth
We also explored the relationship between behavioral thresholds and DPOAE growth. Specifically, we explored the relationship between behavioral thresholds and Slope 2 of the DPOAE growth functions. Pearson’s correlations between behavioral tracking threshold and Slope 2 of the individual DPOAE growth functions at each f2 test frequency ranged from very weak at 2 kHz (r(184) = 0.02, p = 0.83) and 4 kHz (r(188) = − 0.19, p = 0.01) to weak at 8 kHz (r(179) = − 0.26, p = 0.000). These correlations are displayed in Fig. 12 in panels A (2 kHz), B (4 kHz), and C (8 kHz), respectively.

The correlations between Slope 2 of the individual DPOAE growth functions and behavioral tracking threshold from each participant at the same f2 frequency ranged from very weak at 2 kHz (panel A) and 4 kHz (panel B) to weak at 8 kHz (panel C). This suggests that behavioral thresholds do not fully explain declines in Slope 2 that occur with age
Additionally, we questioned if the same declines in DPOAE growth would be apparent if a stricter definition of “normal” hearing were used. Therefore, we also examined average DPOAE growth functions after modifying our inclusion criteria to include only participants with audiometric thresholds ≤ 15 dB HL from 0.25 to 8 kHz. We selected 15 dB HL because it is a more stringent, but less commonly used cutoff for defining “normal” vs. “impaired” hearing. This reduced our number of participants from 199 to 130 (34, 60, 13, 15, and 8 participants from the youngest to oldest age groups, respectively). However, declines in average DPOAE growth were still apparent, particularly at 8 kHz (Fig. 13).

Average distortion product otoacoustic emission (DPOAE) growth functions still decline considerably with increasing age at all three frequencies tested, f2 = 2 kHz (left), 4 kHz (middle), and 8 kHz (right), even when stricter audiometric threshold inclusion criteria are used (audiometric thresholds ≤ 15 dB HL from .25 to 8 kHz). This suggests that behavioral thresholds ≤ 8 kHz may be insufficient for detecting subtle age-related auditory change, even if more stringent criteria for “normal” hearing were to be adopted. Average noise floor levels are similar between age groups and are shown at the bottom of each panel. Average DPOAE and noise floor levels are plotted as a function of L2. Error bars indicate + / − 1 standard error of the mean
DISCUSSION
We examined DPOAE growth in individuals aged 10–65 years with clinically normal hearing. Results showed considerable declines in DPOAE growth, but modest differences in behavioral thresholds with age at frequencies ≤ 8 kHz. Additionally, behavioral thresholds at frequencies ≥ 10 kHz declined significantly with age.
Behavioral Thresholds
Our inclusion criteria allowed us to explore signs of auditory aging that occur before behavioral thresholds are severely affected, and the extent to which standard definitions of “normal” hearing detect these signs. Even “normal” ears showed subtle declines in behavioral thresholds with age at frequencies ≤ 8 kHz. However, these declines were not clinically significant, reaffirming that behavioral thresholds ≤ 8 kHz and a 25 dB HL cutoff to define “normal” are poor markers of cochlear health (Gatlin and Dhar 2021). In contrast, behavioral thresholds above ~ 10 kHz decline substantially with age. This suggests that a decline in sensory cell function and/or sensory cell loss is present in the cochlear base early in life and extensive by age 40 + (Hamernik et al. 1989; Lee et al. 2012).
However, it is possible that small changes to thresholds — even within the clinically normal range — are fully or partially driving changes in DPOAEs. Parsing out the effect of sensitivity from age-related changes to DPOAEs is challenging. While studies have shown DPOAE declines with age (e.g., Lonsbury-Martin et al. 1991; Gates et al. 2002; Ueberfuhr et al. 2016), few have strictly controlled for sensitivity using stringent inclusion criteria and/or statistical techniques (e.g., Stover and Norton 1993; Uchida et al. 2008; Ortmann and Abdala 2016). For several reasons, threshold differences at frequencies ≤ 8 kHz may not be fully driving the declines in DPOAE growth seen here. First, differences in DPOAE growth are apparent even at 2 kHz, where the largest behavioral tracking threshold differences between age groups are negligible (1–3 dB). Second, substantial declines in DPOAE growth are apparent in the 30–39-year age group at all f2 frequencies, despite differences in behavioral tracking thresholds (re youngest group) being < 1 dB at 2 and 4 kHz, and < 3 dB at 8 kHz. Third, DPOAE declines occur in the mid-level region of the growth function (L2 = ~ 25–45 dB SPL), suggesting that it is not a threshold phenomenon. We expected changes in sensitivity to manifest as differences in either Slope 1 or Break 1; however, there were no considerable differences between age groups for either. Fourth, correlations between behavioral tracking thresholds ≤ 8 kHz and Slope 2 of DPOAE growth functions were weak (Fig. 12). Fifth, notable declines in DPOAE growth remain even with a stricter definition of “normal” hearing. Thus, even with stricter cutoffs, behavioral thresholds ≤ 8 kHz may be insufficient in detecting early age-related cochlear decline. However, more work is needed to explicitly define the relationship between behavioral thresholds and DPOAE growth.
DPOAE Growth Functions
Our data show that DPOAE growth is non-linear when L2 ≤ 25 dB SPL and more linear from ~ 25 to 45 dB SPL across all age groups. Other studies suggest that cochlear response patterns (e.g., Cooper and Rhode 1992; Nuttall and Dolan 1996; Ruggero et al. 1997) and DPOAE growth (e.g., Dorn et al. 2001; Ortmann and Abdala 2016) are approximately linear below ~ 40 dB SPL. This difference in growth function morphology may be due, in part, to differences in measurement paradigms. Because we used a fixed L1/varied L2 DPOAE measurement paradigm with an f2/f1 ratio ≤ 1.3, level differences between the primary tones were large (up to 60 dB SPL) at low L2 levels, and the compression noted below ~ 25 dB SPL may have arisen from the suppressive effects of L1 on L2 and/or the f2 place. This differs from the commonly used “scissors” paradigm (Dorn et al. 2001), where differences between primary tones are smaller (< 40 dB SPL). It also differs slightly from the fixed L1/varied L2 paradigm used in guinea pigs by Withnell and Yates (1998), where an f2/f1 ratio of 1.6 was chosen to minimize suppressive effects and level differences between primaries were smaller. Indeed, when they used an f2/f1 ratio of 1.2 and a higher L1, their DPOAE growth functions more closely resemble ours, with linear growth from ~ 20 to 40 dB SPL and a compression threshold resembling our Break 2. Additional differences between our data and basilar membrane growth data at low stimulus levels may be explained by the fact that we are measuring growth of the 2f1-f2 distortion product rather than BM gain. DPOAE and BM growth may be differentially influenced by various factors, including contributions from sources basal to the f2 place (Martin et al. 2009, 2011), and/or the reticular lamina (Dewey et al. 2019; Ren and He 2020). However, the extent to which suppression vs. differences in DPOAE/BM growth are driving this compressive behavior below ~ 25 dB SPL may be complicated to measure and interpret.
What is driving the age-related declines in DPOAE growth, if not sensitivity? The nature of these data only allows us to offer speculations. At least three age-related cochlear pathologies from Schuknecht’s framework are theoretically detectable using DPOAEs: sensory, metabolic, and/or mechanical decline. While we can likely exclude extensive sensory cell loss apical to the 8 kHz place, metabolic and/or mechanical decline may be present in our aged ears. Either may manifest at mid- to high stimulus levels, where a broader array of outer hair cells (OHCs) is activated.
Specifically, a subtle decline in metabolic function and subsequent reduction of the endocochlear potential (EP) could manifest as a premature saturation of the cochlear transduction current at higher stimulus levels. While stark declines in EP induced over a short experimental time course greatly reduce BM gain at low stimulus levels (e.g., Ruggero and Rich 1991), DPOAEs arise from a more distributed cochlear area and may be differentially affected. It is possible that our participants have declines in EP but still have normal behavioral thresholds below 8 kHz, given that even large shifts in EP (up to 70 mV) in the apical region of the gerbil cochlea can lead to small (< 20 dB) shifts in compound action potential (CAP) threshold (Schmiedt et al. 2002). Even in the cochlear base, estimates suggest that a ~ 1 mV decline in EP leads to a ~ 1 dB decline in CAP threshold in cats (Sewell 1984) and gerbils (Schmiedt et al. 2002). This suggests that the EP could decline by ~ 20 mV or more over the course of a life span with behavioral thresholds remaining in the range of clinically normal (up to 25 dB HL). Nevertheless, the relationship between EP and DPOAEs is more complex. Studies that have manipulated the EP and simultaneously recorded changes to the EP and the 2f1-f2 DPOAE have demonstrated that DPOAEs follow a different time course of decline and recovery than the EP itself (Rebillard and Lavigne-Rebillard 1992). However, animals with chronically decreased EP (due to furosemide) exhibit reduced DPOAEs (Schmiedt et al. 2002). Thus, DPOAEs may be sensitive to subtle age-related declines in the EP, even if the timeline and degree of decline between the two is not tightly coupled.
The presence of cochlear mechanical dysfunction in our older participants is also possible. Broadened frequency selectivity (i.e., tuning) occurs with age (Lutman et al. 1991; Dubno and Ahlstrom 2001), and in the absence of clinical hearing loss (Badri et al. 2011). Puzzlingly, broadened tuning could suggest that increasing stimulus level would activate a broader array of OHCs in older than younger ears. Yet DPOAE amplitude and growth appear to decrease with age (e.g., Lonsbury-Martin et al. 1991; Uchida et al. 2008; Ortmann and Abdala 2016). Broadened tuning with reduced DPOAEs in older ears could be explained by phase interference between DPOAE wavelets (e.g., Talmadge et al. 1999; Dhar et al. 2002; Shera 2003), and/or if the number, or function (i.e., fidelity), of OHCs within the activated spatial region contributing to the measured DPOAE change with age. Evidence suggests that OHCs basal to the f2 place may contribute to DPOAEs (Martin et al. 2009, 2011); thus, damaged hair cells in extended high-frequency regions could cause the reduction of DPOAE growth that we see in our older ears (relative to younger ears), particularly at 8 kHz. Suggestive of this, the correlation between behavioral tracking thresholds at 10 kHz (~ 1/4 octave basal to the f2 place) and Slope 2 of DPOAE growth functions at 8 kHz is − 0.31 (p < 0.001). This is slightly higher than correlations between Slope 2 and behavioral tracking thresholds at the f2 frequencies. Additional work is needed to explore potential differences in basal OAE generators between young and aged ears.
Individual DPOAE Growth Functions and Clinical Relevance
A tool with high clinical utility must detect subtle signs of dysfunction within individuals. While we successfully fit individual DPOAE growth functions, there was notable variability between individual participants (Fig. 5). Variability was smallest for the oldest age groups, possibly because we only included older ears with excellent sensitivity. It is tempting to wonder whether young ears with lower-than-average DPOAE growth already exhibit cochlear decline undetectable by current clinical tools, and/or if these ears will be more susceptible to future auditory insults. The latter possibility highlights the need for longitudinal work.
There was also variability in the estimated slope and breakpoint values between individuals, particularly in the oldest age groups. This may be because DPOAE growth function morphology was more variable in older individuals. More work is needed to better understand the factors that contribute to this variability. This includes factors intrinsic to an individual, such as differences in DPOAE component contributions, which were not considered here. While we assumed that the distortion component dominated DPOAE growth above ~ 30 dB SPL, the reflection component may have contributed at lower stimulus levels and may differ systematically with age (Abdala and Dhar 2012). Additionally, differences in cochlear micromechanics between individuals (e.g., number and health of stereocilia and/or OHCs) likely contribute to variability in DPOAE growth, though these are difficult to quantify in humans. Extrinsic factors, including calibration, signal processing, data fitting, and measurement paradigm, may also contribute to variability in DPOAE growth and require further exploration (e.g., Johnson et al. 2006).
CONCLUSION
Our data show age-related declines in DPOAE growth in individuals with clinically normal hearing. This challenges the notion that clinically “normal” hearing means a pristine auditory system and suggests the need for a future where hearing-related monitoring and treatment precede communication difficulties. There may be potential in using DPOAE growth to detect early signs of cochlear aging, particularly if factors contributing to variability in DPOAE growth become better understood.
References
Abdala C, Dhar S (2012) Maturation and aging of the human cochlea: a view through the DPOAE looking glass. J Assoc Res Otolaryngol 13:403–421. https://doi.org/10.1007/s10162-012-0319-2
Abdala C, Ortmann AJ, Shera CA (2018) Reflection- and distortion-source otoacoustic emissions: evidence for increased irregularity in the human cochlea during aging. J Assoc Res Otolaryngol 19:493–510. https://doi.org/10.1007/s10162-018-0680-x
Badri R, Siegel JH, Wright BA (2011) Auditory filter shapes and high-frequency hearing in adults who have impaired speech in noise performance despite clinically normal audiograms. J Acoust Soc Am 129:852–863. https://doi.org/10.1121/1.3523476
Blackwell DL, Lucas JW, Clarke, Tainya C (2014) Summary health statistics for U.S. adults: National Health Interview Survey, 2012. Vital Health Stat 10. https://doi.org/10.1037/e403882008-001
Cooper NP, Rhode WS (1992) Basilar membrane mechanics in the hook region of cat and guinea-pig cochleae: sharp tuning and nonlinearity in the absence of baseline position shifts. Hear Res 63:163–190. https://doi.org/10.1016/0378-5955(92)90083-Y
Crowson MG, Hertzano R, Tucci DL (2017) Emerging therapies for sensorineural hearing loss. Otol Neurotol 38:792–803. https://doi.org/10.1097/MAO.0000000000001427
Cunningham LL, Tucci DL (2017) Hearing loss in adults. N Eng J Med 377:2465–2473. https://doi.org/10.1056/NEJMra1616601
Dewey JB, Applegate BE, Oghalai JS (2019) Amplification and suppression of traveling waves along the mouse organ of Corti: evidence for spatial variation in the longitudinal coupling of outer hair cell-generated forces. J Neurosci 39:1805–1816. https://doi.org/10.1523/JNEUROSCI.2608-18.2019
Dhar S, Talmadge CL, Long GR, Tubis A (2002) Multiple internal reflections in the cochlea and their effect on DPOAE fine structure. J Acoust Soc Am 112:2882–2897. https://doi.org/10.1121/1.1516757
Dorn PA, Konrad-Martin D, Neely ST et al (2001) Distortion product otoacoustic emission input/output functions in normal-hearing and hearing-impaired human ears. J Acoust Soc Am 110:3119–3131. https://doi.org/10.1121/1.1417524
Dubno JR, Ahlstrom JB (2001) Psychophysical suppression measured with bandlimited noise extended below and/or above the signal: effects of age and hearing loss. J Acoust Soc Am 110:1058–1066. https://doi.org/10.1121/1.1381024
Dubno JR, Eckert MA, Lee F-S et al (2013) Classifying human audiometric phenotypes of age-related hearing loss from animal models. J Assoc Res Otolaryngol 14:687–701. https://doi.org/10.1007/s10162-013-0396-x
Gates GA, Mills D, Nam B et al (2002) Effects of age on the distortion product otoacoustic emission growth functions. Hear Res 163:53–60. https://doi.org/10.1016/S0378-5955(01)00377-X
Gatlin AE, Dhar S (2021) History and lingering impact of the arbitrary 25-dB cutoff for normal hearing. Am J Audiol 1–4 https://doi.org/10.1044/2020_AJA-20-00181
Gorga MP, Neely ST, Dorn PA, Hoover BM (2003) Further efforts to predict pure-tone thresholds from distortion product otoacoustic emission input/output functions. J Acoust Soc Am 113:3275. https://doi.org/10.1121/1.1570433
Gratton MA, Schulte BA, Smythe NM (1997) Quantification of the stria vascularis and strial capillary areas in quiet-reared young and aged gerbils. Hear Res 114:1–9. https://doi.org/10.1016/S0378-5955(97)00025-7
Hamernik RP, Patterson JH, Turrentine GA, Ahroon WA (1989) The quantitative relation between sensory cell loss and hearing thresholds. Hear Res 38:199–211. https://doi.org/10.1016/0378-5955(89)90065-8
Hoffman HJ, Dobie RA, Losonczy KG et al (2017) Declining prevalence of hearing loss in US adults aged 20 to 69 years. JAMA Otolaryngol Head Neck Surg 143:274–285. https://doi.org/10.1001/jamaoto.2016.3527
Hughson W, Westlake H (1944) Manual for program outline for rehabilitation of aural casualties both military and civilian. Trans Am Acad Ophthalmol Otolaryngol 48(Suppl):1–15
Hunter LL, Monson BB, Moore DR et al (2020) Extended high frequency hearing and speech perception implications in adults and children. Hear Res 107922 https://doi.org/10.1016/j.heares.2020.107922
Johnson TA, Neely ST, Garner CA, Gorga MP (2006) Influence of primary-level and primary-frequency ratios on human distortion product otoacoustic emissions. J Acoust Soc Am 119:418–428. https://doi.org/10.1121/1.2133714
Kemp DT (1978) Stimulated acoustic emissions from within the human auditory system. J Acoust Soc Am 64:1386–1391. https://doi.org/10.1121/1.382104
Kim DO, Molnar CE, Matthews JW (1980) Cochlear mechanics: nonlinear behavior in two-tone responses as reflected in cochlear-nerve-fiber responses and in ear-canal sound pressure. J Acoust Soc Am 67:1704–1721. https://doi.org/10.1121/1.384297
Kujawa SG, Liberman MC (2009) Adding insult to injury: cochlear nerve degeneration after “temporary” noise-induced hearing loss. J Neurosci 29:14077–14085. https://doi.org/10.1523/JNEUROSCI.2845-09.2009
Kummer P, Janssen T, Arnold W (1998) The level and growth behavior of the 2f1−f2 distortion product otoacoustic emission and its relationship to auditory sensitivity in normal hearing and cochlear hearing loss. J Acoust Soc Am 103:3431–3444. https://doi.org/10.1121/1.423054
Lee J, Dhar S, Abel R et al (2012) Behavioral hearing thresholds between 0.125 and 20 kHz using depth-compensated ear simulator calibration. Ear Hear 33:315–329. https://doi.org/10.1097/AUD.0b013e31823d7917
Lin FR, Niparko JK, Ferrucci L (2011) Hearing loss prevalence in the United States. Arch Intern Med 171:1851–1853. https://doi.org/10.1001/archinternmed.2011.506
Lonsbury-Martin BL, Cutler WM, Martin GK (1991) Evidence for the influence of aging on distortion-product otoacoustic emissions in humans. J Acoust Soc Am 89:1749–1759. https://doi.org/10.1121/1.401009
Lutman ME, Gatehouse S, Worthington AG (1991) Frequency resolution as a function of hearing threshold level and age. J Acoust Soc Am 89:320–328. https://doi.org/10.1121/1.400513
Martin GK, Stagner BB, Chung YS, Lonsbury-Martin BL (2011) Characterizing distortion-product otoacoustic emission components across four species. J Acoust Soc Am 129:3090–3103. https://doi.org/10.1121/1.3560123
Martin GK, Stagner BB, Fahey PF, Lonsbury-Martin BL (2009) Steep and shallow phase gradient distortion product otoacoustic emissions arising basal to the primary tones. J Acoust Soc Am 125:85–92. https://doi.org/10.1121/1.3073734
Mauermann M, Kollmeier B (2004) Distortion product otoacoustic emission (DPOAE) input/output functions and the influence of the second DPOAE source. J Acoust Soc Am 116:2199–2212. https://doi.org/10.1121/1.1791719
Mills DM, Schmiedt RA (2004) Metabolic presbycusis: differential changes in the auditory brainstem and otoacoustic emission responses with chronic furosemide application in the gerbil. J Assoc Res Otolaryngol 5:1–10. https://doi.org/10.1007/s10162-003-4004-3
Muggeo VMR (2003) Estimating regression models with unknown break-points. Stat Med 22:3055–3071. https://doi.org/10.1002/sim.1545
Muggeo VMR (2017) Interval estimation for breakpoint in segmented regression: a smooth score-based approach. Aust NZ J Stat 59:311–322. https://doi.org/10.1080/00949655.2016.1149855
Müller U, Barr-Gillespie PG (2015) New treatment options for hearing loss. Nat Rev Drug Discov 14:346–365. https://doi.org/10.1038/nrd4533
Neely S, Liu Z (1993) EMAV: otoacoustic emission averager. In: Technical memorandum. Omaha, NE: Boys Town National Research Hospital
Nuttall AL, Dolan DF (1996) Steady-state sinusoidal velocity responses of the basilar membrane in guinea pig. J Acoust Soc Am 99:1556–1565. https://doi.org/10.1121/1.414732
Olusanya BO, Davis AC, Hoffman HJ (2019) Hearing loss grades and the international classification of functioning, disability and health. Bull World Health Organ 97:725–728. https://doi.org/10.2471/BLT.19.230367
Ortmann AJ, Abdala C (2016) Changes in the compressive nonlinearity of the cochlea during early aging: estimates from distortion OAE input/output functions. Ear Hear 37:603–614. https://doi.org/10.1097/AUD.0000000000000319
Oshima K, Suchert S, Blevins NH, Heller S (2010) Curing hearing loss: patient expectations, health care practitioners, and basic science. J Commun Disord 43:311–318. https://doi.org/10.1016/j.jcomdis.2010.04.002
Poling GL, Siegel JH, Lee J et al (2014) Characteristics of the 2f1-f2 distortion product otoacoustic emission in a normal hearing population. J Acoust Soc Am 135:287–299. https://doi.org/10.1121/1.4845415
R Core Team (2020) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/
Rebillard G, Lavigne-Rebillard M (1992) Effect of reversible hypoxia on the compared time courses of endocochlear potential and 2f1-f2 distortion products. Hear Res 62:142–148. https://doi.org/10.1016/0378-5955(92)90179-Q
Ren T, He W (2020) Two-tone distortion in reticular lamina vibration of the living cochlea. Commun Biol 3:35. https://doi.org/10.1038/s42003-020-0762-2
Ruggero MA, Rich NC (1991) Furosemide alters organ of Corti mechanics: evidence for feedback of outer hair cells upon the basilar membrane. J Neurosci 11:1057–1067. https://doi.org/10.1523/JNEUROSCI.11-04-01057.1991
Ruggero MA, Rich NC, Recio A et al (1997) Basilar-membrane responses to tones at the base of the chinchilla cochlea. J Acoust Soc Am 101:2151–2163. https://doi.org/10.1121/1.418265
Schmiedt RA, Lang H, Okamura H, Schulte BA (2002) Effects of furosemide applied chronically to the round window: a model of metabolic presbyacusis. J Neurosci 22:9643–9650. https://doi.org/10.1523/JNEUROSCI.22-21-09643.2002
Schuknecht HF (1964) Further observations on the pathology of presbycusis. Arch Otolaryngol 80:369–382. https://doi.org/10.1001/archotol.1964.00750040381003
Schuknecht HF, Gacek MR (1993) Cochlear pathology in presbycusis. Ann Otol Rhinol Laryngol 102:1–16. https://doi.org/10.1177/00034894931020S101
Sewell WF (1984) The effects of furosemide on the endocochlear potential and auditory-nerve fiber tuning curves in cats. Hear Res 14:305–314. https://doi.org/10.1016/0378-5955(84)90057-1
Shera CA (2003) Wave interference in the generation of reflection- and distortion-source emissions. Biophysics of the Cochlea: from Molecules to Models 439–453. https://doi.org/10.1142/5219
Shibata SB, West MB, Du X et al (2020) Gene therapy for hair cell regeneration: review and new data. Hear Res 107981. https://doi.org/10.1016/j.heares.2020.107981
Souza NN, Dhar S, Neely ST, Siegel JH (2014) Comparison of nine methods to estimate ear-canal stimulus levels. J Acoust Soc Am 136:1768–1787. https://doi.org/10.1121/1.4894787
Spicer SS, Schulte BA (2002) Spiral ligament pathology in quiet-aged gerbils. Hear Res 172:172–185. https://doi.org/10.1016/S0378-5955(02)00581-6
Stover L, Norton SJ (1993) The effects of aging on otoacoustic emissions. J Acoust Soc Am 94:2670–2681. https://doi.org/10.1121/1.407351
Studebaker GA (1967) Intertest variability and the air-bone gap. J Speech Hear Disord 32:82–86. https://doi.org/10.1044/jshd.3201.82
Talmadge CL, Long GR, Tubis A, Dhar S (1999) Experimental confirmation of the two-source interference model for the fine structure of distortion product otoacoustic emissions. J Acoust Soc Am 105:275–292. https://doi.org/10.1121/1.424584
Uchida Y, Ando F, Shimokata H et al (2008) The effects of aging on distortion-product otoacoustic emissions in adults with normal hearing. Ear Hear 29:176–184. https://doi.org/10.1097/AUD.0b013e3181634eb8
Ueberfuhr MA, Fehlberg H, Goodman SS, Withnell RH (2016) A DPOAE assessment of outer hair cell integrity in ears with age-related hearing loss. Hear Res 332:137–150. https://doi.org/10.1016/j.heares.2015.11.006
Withnell RH, Yates GK (1998) Onset of basilar membrane non-linearity reflected in cubic distortion tone input-output functions. Hear Res 123:87–96. https://doi.org/10.1016/S0378-5955(98)00100-2
Wood SN (2001) Minimizing model fitting objectives that contain spurious local minima by bootstrap restarting. Biometrics 57:240–244. https://doi.org/10.1111/j.0006-341X.2001.00240.x
Wu P, O’Malley JT, de Gruttola V, Liberman MC (2020) Age-related hearing loss is dominated by damage to inner ear sensory cells, not the cellular battery that powers them. J Neurosci 40:6357–6366. https://doi.org/10.1523/JNEUROSCI.0937-20.2020
Acknowledgements
The authors wish to thank Rebekah Abel, Gayla Poling, Jungmee Lee, and Steve Zecker for their instrumental roles in the design and execution of the original project.
Funding
This research was supported by NIH/NIDCD Grant R01 DC008420.
Author information
Authors and Affiliations
Contributions
CCG analyzed the data and co-wrote the manuscript with SD. JS and SD designed the original study. JS critically reviewed and edited the manuscript.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Glavin, C.C., Siegel, J. & Dhar, S. Distortion Product Otoacoustic Emission (DPOAE) Growth in Aging Ears with Clinically Normal Behavioral Thresholds. JARO 22, 659–680 (2021). https://doi.org/10.1007/s10162-021-00805-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10162-021-00805-3