
Abstract
Background
Anemia greatly affects the development of renal and cardiovascular outcomes in chronic kidney disease (CKD) patients. However, the impact based on CKD stage remains unclear.
Methods
We prospectively followed 2,602 Japanese CKD patients under the care of nephrologists. CKD was defined according to cause, estimated glomerular filtration rate <60 mL/min, and/or proteinuria. Patient outcomes [primary end-points: cardiovascular events (CVEs), all-cause mortality, and end-stage kidney disease (ESKD) requiring renal replacement therapy] were assessed in association with basal hemoglobin (Hb) levels (<10, 10–12 and ≥12 g/dL), stratified by CKD stages.
Results
During follow-up, 123 patients developed CVEs, 41 died, and 220 progressed to ESKD. For stages G3, G4 and G5, ESKD frequencies were 2.8, 64.4, and 544.8 person-years, while CVEs and death were 25.6, 45.6, and 76.3 person-years, respectively. The combined endpoint rate was significantly higher in patients with Hb <10 versus Hb 10–12 g/dL, but a higher risk for CVEs and death with Hb <10 g/dL was found only in G3 [hazard ratio (HR) 4.49, (95 % confidence interval (95 % CI) 2.06–9.80)]. In contrast, risk for ESKD with Hb <10 g/dL was found only in G4 [HR 3.08 (95 % CI 1.40–6.79)] and G5 [HR 1.43 (95 % CI 1.01–2.05)]. No increased risks with higher Hb levels were found.
Conclusion
The impact of renal anemia of Hb <10 g/dL on clinical outcomes differed by CKD stage, with a significantly high risk for CVEs and all-cause mortality in G3 and progression to ESKD in G4 and G5.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Renal anemia is common in chronic kidney disease (CKD) and is a modifiable risk factor for developing both renal and cardiovascular outcomes [1]. For nephrologists, the main goal of patient management before renal replacement therapy (RRT) is to delay end-stage kidney disease (ESKD) and to reduce cardiovascular events (CVEs) and premature death. Studies revealed that anemia greatly affects cardiovascular outcomes; this is known as cardio-renal-anemia syndrome [2]. Moreover, mortality rates were lower in patients regularly followed up by a nephrologist, likely because of the specialist care before initiating dialysis [3]. In spite of the clinical importance of anemia management before initiating dialysis, only a few studies have assessed the impact of anemia on clinical outcomes, especially regarding premature death and CVEs, when regularly followed by nephrologists [4, 5].
Concerning the management of anemia in CKD patients, recent randomized controlled trials (RCTs) in Western countries have shown that normalization of hemoglobin (Hb) with erythropoiesis-stimulating agents (ESAs) was not beneficial for renal and cardiovascular disease [6–8]. Based on these reports, the guidelines for CKD recommended a target Hb around 10–12 g/dL in both the Kidney Disease Improving Global Outcomes (KDIGO) [9] as well as the Japanese guidelines [10, 11]. However, in contrast to the Western data, non-beneficial effects in patients with higher Hb levels have not been reported in Japanese RCTs for CKD, namely, higher Hb levels with ESAs were associated with improved renal function, cardiac function, and quality of life [12–15]. On the other hand, naturally occurring higher levels of Hb related to lower renal outcomes in both Western and Japanese CKD patients [16, 17]. Additionally, studies without targeted Hb levels demonstrated that even mild anemia was associated with a higher risk for premature death and ESKD in CKD [4, 17]. Moreover, the prevalence of anemia and outcomes were different among CKD stages [5]. However, reports on clinical outcomes in Japanese CKD patients are limited.
These facts raise the need to explore potential links between Hb levels and clinical outcomes in a Japanese CKD regularly followed by nephrologists. We hypothesized that anemia without targeted Hb levels might have different impacts on renal and non-renal outcomes; therefore, we further examined the association of anemia with clinical outcomes according to CKD severity.
Methods
Participants (the Gonryo CKD cohort)
We conducted a prospective observational cohort study entitled “The Gonryo CKD project” on an outpatient basis in 11 hospitals offering nephrology services, including one university hospital in Miyagi Prefecture, located in the northeast area of Japan [18, 19]. The participating hospitals covered almost the entire medical network of the area. Between May 2006 and November 2008, every outpatient from the nephrologists was invited to participate. Thus, 4,015 patients who gave informed consent and were under the regular care of nephrologists were enrolled. Based on the previous publications of the study, certain subjects were excluded for the following reasons: lack of data on serum creatinine levels (n = 145), unknown underlying renal disease (n = 170), no-show (n = 1), estimated glomerular filtration rate (eGFR) >60 mL/min without proteinuria (n = 888), or no urinary testing results (n = 117). Because of additional exclusion of those without Hb data (n = 92), 2,602 patients meeting the CKD criteria were evaluated in the present study (Supplemental Figure 1). The Institutional Review Boards at Tohoku University School of Medicine (Number 2006-10, UMIN000011211) and the respective participating hospitals approved the study protocol.
Patient classification and primary outcomes
Participants were classified according to baseline Hb levels: <10, 10–12 (reference), and ≥12 g/dL. The reference range of 10–12 g/dL reflected the target Hb level in Japanese guidelines [10]. To examine Hb levels ≥12 g/dL, this group was further subdivided into 12–13 and ≥13 g/dL. For analysis according to CKD stages, participants were stratified by baseline eGFR as follows: eGFR ≥60 (G1–2), 60–30 (G3), 30–15 (G4), and <15 mL/min (G5). We defined diabetes patients as those treated for diabetes, not only for diabetic nephropathy of underlying renal disease.
The primary outcomes were CVEs, all-cause death before RRT, or ESKD requiring RRT. CVEs included angina pectoris, acute myocardial infarction (AMI), congestive heart failure, and stroke (cerebral bleeding or infarction). The outcomes were determined from the medical records, death certificates, and interviews with the attending physicians at the time of the annual checkups until the 3-year follow-up. A CVE was defined as a disease of the circulatory system (International Classification of Disease, 10th Revision: I00–I99), and the patients with angina pectoris or AMI included patients diagnosed using coronary angiography; those who received coronary stenting, angioplasty, or a bypass operation; or those who had a definite clinical course of AMI. In cases with congestive heart failure, only those who needed admission for treatment were counted. Diagnosis of stroke was based on the Classification of Cerebrovascular Diseases III published by the National Institute of Neurological Disorders and Stroke [20], and only patients whose conditions were confirmed by using computed tomography or brain magnetic resonance imaging were included. Asymptomatic cerebral infarction or lacunar infarction was not included. Moreover, as the follow-up period of 3 years is not sufficient to adopt initiation of RRT, we also included patients who had a >50 % decline in eGFR over 3 years as a secondary renal endpoint.
Data collection
Patient data were obtained from the medical records at each hospital. Patient characteristics and laboratory data were collected as baseline data; as follow-up data, serum creatinine, eGFR, Hb, and CVE were collected annually from the date of cohort entry until the end of follow-up, i.e., death, initiation of RRT, or 3 years after registration. Blood pressure data were obtained with the patient in the sitting position, using an automatic sphygmomanometer based on the Korotkoff sound technique. We used the urine and blood examination results from each participating hospital as laboratory data. Serum creatinine levels were measured using the enzyme assay method and monitored annually. We estimated the glomerular filtration rate using the formula for the Japanese population (mL/min/1.73 m2) [21]. The presence of urine protein was defined as a positive dipstick test for spot urine, which corresponded to values >30 mg/dL using the urine analyzer in each hospital. Moreover, information on treatments, such as ESAs, iron use, insulin, and antihypertensive medications were obtained from the medical records. ESAs included darbepoetin alfa, continuous erythropoietin receptor activator, and recombinant human erythropoietin. Iron use included intravenous iron and oral iron.
Statistical analysis
Data are shown as mean ± standard deviation unless otherwise specified. A P value <0.05 indicated statistical significance. Differences between groups were analyzed using a t test or one-way analysis of variance (ANOVA); if the ANOVA demonstrated significance, a post hoc test was used. Correlations were calculated using the non-parametric Spearman rank test. In the survival analysis, the renal outcome was progression to ESKD, and the non-renal outcomes were combined CVEs and all-cause mortality. The composite endpoints included CVEs, all-cause mortality, and ESKD. The results of traditional and competing Cox regression analyses were presented as hazard ratios (HR) with 95 % confidence intervals (95 % CIs). The test of interaction was estimated by adding multiplicative interaction terms between Hb levels and eGFR to the relevant Cox model. We calculated the risks for renal and non-renal endpoint, using the competing risk approach. Because the patients who started undergoing RRT were not followed up in this cohort, the occurrence of either ESKD or non-renal outcomes prevents the occurrence of the other. [22]. All data were statistically analyzed using Stata version 12.1 statistical software (Stata Corp LP, College Station, Texas, USA).
Results
Baseline characteristics and association between Hb level and CKD stage
The median eGFR of all patients was 53.4 mL/min (interquartile range 32.6–74.0), and the mean Hb level at baseline was 12.8 ± 2.1 g/dL. Table 1 summarizes the features at baseline among Hb levels. As expected, the frequency of patients receiving care for anemia (treated with ESAs and/or iron use) was higher among patients with lower Hb levels. The percentage of patients with Hb levels lower than the maintenance level of 10 g/dL, in whom only 40.6 % were receiving ESA therapy, was 1.7 % in G1–2, 4.2 % in G3, 20.7 % in G4, and 54.7 % in G5. Hb levels decreased with CKD progression in patients with and without diabetes, and a greater proportion of patients with CKD stages G4 and G5 were receiving care for anemia (Fig. 1).

Hemoglobin levels according to CKD stage in 2,602 patients. Hemoglobin levels decreased in accordance with CKD progression in patients both with and without diabetes, and the patients undergoing ESA and iron treatment increased at the advanced CKD stages. CKD chronic kidney disease, ESA erythropoiesis-stimulating agents
Incidence of primary endpoints among Hb levels by CKD stages
During a median follow-up of 2.38 years (interquartile range 1.69–3.00), 41 patients died, 123 patients developed CVEs, and 220 patients ended follow-up because they developed ESKD. The incidence rate of primary endpoints was higher in patients with Hb levels <10 g/dL for each CKD stage as shown in Fig. 2 and Supplemental Table 1. In addition, the composite endpoint rate was higher in advanced CKD stages, with a higher frequency of ESKD in G4 and G5, while combined CVEs and all-course mortality were observed in all CKD stages. Compared with Hb levels of 10–12 g/dL, Hb levels less than 10 g/dL were associated with a significantly increased risk for the composite endpoint in univariate and multivariate models [HR 3.41 (95 % CI 2.71–4.30) and HR 1.90 (95 % CI 1.47–2.44), respectively] after adjustment for age, sex, smoking, comorbidities (diabetes mellitus and prior cardiovascular disease), systolic blood pressure, body mass index, proteinuria, and eGFR. Further adjustment for treatment with ESA and iron use remained significant [HR 1.65 (95 % CI 1.27–2.14); Table 2].

The incidence rate of primary endpoints. The incidence rate is presented in 1,000 person-years for the composite endpoint, including renal (ESKD, gray) and non-renal outcomes (all-cause mortality and cardiovascular events, black), by hemoglobin levels among CKD stages. The composite endpoint rate was higher in patients with Hb levels <10 g/dL for each CKD stage. The frequency of ESKD was higher in G4 and G5, while non-renal outcomes were observed in all CKD stages. CKD chronic kidney disease, CVEs cardiovascular events, ESKD end-stage kidney disease, Hb hemoglobin
On the other hand, Hb levels ≥12 g/dL were associated with a lower risk in multivariate analysis [HR 0.51 (95 % CI 0.37–0.69); Table 2]. As a sub-analysis, Hb levels ≥13 g/dL did not increase the risk compared with Hb levels of 10–12 g/dL in multivariate analysis [HR 0.47 (95 % CI 0.33–0.69)].
Moreover, the magnitude of the association between Hb levels and the risk of composite outcomes decreased significantly by 7.7 % per every 1 mL/min/1.73 m2 increase in eGFR [HR for interaction term = 1.017 (95 % CI 1.007–1.026), P for interaction = 0.001]. Therefore, we used a stratified analysis by CKD stages to negate the effect of renal function on the relationship between Hb levels and outcomes.
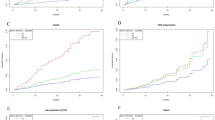
Anemia is a risk for renal and non-renal outcomes in CKD
In G3, the cumulative incidence of non-renal outcomes before ESKD was significantly higher in patients with Hb levels <10 g/dL compared to those with 10–12 g/dL [HR 4.49 (95 % CI 2.06–9.80)] in the multivariate competing risk model adjusted for age, sex, diabetes, history of cardiovascular disease, systolic blood pressure, smoking, proteinuria, and ESA use (Fig. 3). In G4 and G5, the cumulative incidence of non-renal outcomes before ESKD did not differ based on Hb levels, while the incidence of ESKD increased significantly in patients with Hb levels <10 g/dL compared to those with 10–12 g/dL in multivariate models, i.e. HR 3.08 (95 % CI 1.40–6.79) in G4 and HR 1.43 (95 % CI 1.01–2.05) in G5, respectively (Fig. 3). Data for the crude and multivariate competing hazard models are presented in Supplemental Table 2. In addition, we considered that CKD patients, especially those in G3 stage, did not necessarily start RRT during the 3-year follow-up period, despite deterioration of renal function. Therefore, we also examined the secondary renal endpoint included a >50 % decline of eGFR. After 3 years, 72 patients exhibited a decline in eGFR of >50 %; however, in G3, the secondary renal outcome did not increase significantly in patients with Hb levels <10 g/dL compared to those with 10–12 g/dL in the multivariate model [HR 0.86 (95 % CI 0.23–3.26)] adjusted for age, sex, diabetes, history of cardiovascular disease, systolic blood pressure, smoking, proteinuria, and ESA use. In contrast, in G4 and G5, the secondary renal outcome increased significantly in patients with Hb levels <10 g/dL compared to those with 10–12 g/dL in the multivariate model [HR 2.66 (95 % CI 1.47–4.82) and HR 1.44 (95 % CI 1.01–2.05); Supplemental Table 3].

Multivariate competing hazard risks according to CKD stage. Adjusted hazard ratio and 95 % CI for the association of ESKD with CVEs and all-cause mortality according to Hb levels stratified by chronic kidney disease stages. Hb levels of 10–12 g/dL were used as reference. In G3, the incidence for combined CVEs before ESKD was significantly higher with Hb levels <10 g/dL, while in G4 and G5 category, that for ESKD was significantly higher with Hb levels <10 g/dL in competing multivariate models, adjusted for age, sex, diabetes, history of cardiovascular disease, systolic blood pressure, smoking, eGFR, proteinuria, and use of ESA. 95 % CI 95 % confidence interval, CKD chronic kidney disease, CVEs cardio vascular events, eGFR estimated glomerular filtration rate, ESKD end-stage kidney disease, Hb hemoglobin, HR hazard ratio
Discussion
The present study clearly illustrates that Hb levels <10 g/dL are associated with increased risk of all-cause mortality and CVEs in G3 and with progression to ESKD in G4 and G5 in Japanese patients with CKD under the regular care of nephrologists. There were no increased clinical risks in patients with higher Hb levels.
Low Hb level (Hb <10 g/dL) predicted both renal and non-renal outcomes, and this association was affected by CKD stage; to our knowledge, this is the first study showing the impact of anemia on clinical outcomes according to CKD progression. Our results also confirmed that non-renal endpoints were more frequent outcomes than ESKD in G3, but the opposite in G4 and G5, similar to previous reports in Caucasians with CKD [5]. As expected, the frequency of the composite endpoint increased with advanced CKD due to the high incidence of ESKD. On the contrary, non-renal outcomes were observed in all CKD stages. Considering the causality between renal anemia and renal insufficiency, there was an interaction between Hb levels and eGFR. Therefore, it is reasonable that renal function modified the effect of Hb <10 g/dL on the endpoint and that the relationship between Hb levels and outcomes varied across CKD stages. Thus, the outcomes differed among CKD stages; accordingly, competing risks were calculated between renal and non-renal outcomes stratified by CKD stages. No patient with Hb levels >10 g/dL in G1–2 developed ESKD. In G3, Hb levels <10 g/dL predicted the risk for non-renal outcomes. In cardio-renal anemia syndrome [2], hypervolemia appears to be more common due to impaired renal function in CKD, and those with anemia have a higher rate of cardiovascular disease. Previous studies showed that renal dysfunction, combined with anemia, was associated with an increased risk of cardiac function (left ventricular mass index) and mortality after dialysis in Japanese patients with CKD [14, 15, 23].
Hb levels <10 g/dL were also an independent risk for ESKD in advanced CKD stages G4 and G5. Nonetheless, renal anemia is common after G3, and it has been well established that anemia per se is a traditional risk factor for renal outcomes in the CKD population [12, 13, 16, 17, 24]. Our study showed a relationship between Hb levels <10 g/dL and ESKD in G4 and G5, but not in G3 in patients receiving regular nephrology care. This finding was not altered even after including a >50 % decline of eGFR as a secondary renal outcome.
Furthermore, we evaluated whether higher Hb level increased the incidence of outcomes. Indeed, the incidence rate was always lower in patients with higher Hb levels for each CKD stage (Fig. 2, Supplemental Table 1). Moreover, the relative risks of outcomes were not accelerated in our observational cohort with a higher Hb level of Hb >12 g/dL, whose risk for the composite endpoint was significantly lower than those with Hb 10–12 g/dL in crude and multivariate models (Table 2). Even when considering Hb levels ≥13 g/dL, there was no increased incidence of outcomes. This is in contrast to a report that Japanese patients undergoing dialysis had the most favorable survival prognosis at Hb levels between 10 and 11 g/dL, whereas there was an increased risk when Hb ≥11 g/dL [11]. However, the risk related to elevated Hb in dialysis population may be affected by dialysis-induced hemoconcentration. In dialysis patients, Hb levels are usually measured before the dialysis session when the patient is at the highest level of hemodilution; therefore, some patients of high Hb levels are expected to have higher Hb than a physiological level after the dialysis. Moreover, thrombosis of native arteriovenous fistulas, which are the most common vascular access in Japan, should also be considered. RCTs examining patients with CKD receiving ESA treatments also reported negative outcomes in patients with higher targeted Hb levels, ≥13 g/dL [6–8]. Because these major RCTs were performed on a CKD population selected for ESA treatments, a poor hematopoietic response to ESAs was an important risk for all-cause mortality, stroke, and renal outcomes [25]. The Hb level has been shown to be quite stable with ESA treatment [26]; therefore, the prognostic value of anemia on outcomes might be different in subjects undergoing an intervention trial to target Hb compared to that in the general CKD population. This is supported by a study in which mild anemia, defined as Hb levels of 11–13.5 g/dL in men and 11–12 g/dL in women, increased risk of death or ESKD compared to higher Hb levels in a prospective European cohort with CKD stage 3–5 under the care of a nephrologist [4]. Moreover, mild anemia of Hb <13.8 g/dL in diabetic nephropathy associated with the increased risk for ESKD [17].
As indicated in Table 1, the prevalence of anemia was rather high in our cohort. However, the rate of ESA and iron treatments was only 40.6 and 13.4 %, respectively, in patients with Hb levels <10 g/dL. These data were similar to a Japanese cohort with CKD G3–5 in which Hb levels >10 g/dL comprised 61.6 %, of which 55.7 % received ESA therapy [27]. Baseline characteristics in our cohort were collected during 2006–2008, which is prior to publication of the 2009 Japanese guideline for CKD that targeted an increase in Hb levels [10].
There are several limitations to the current study. First, this was an observational study and did not have adequate power to determine target Hb levels or the effects of ESAs or other therapeutics for personalized management of CKD. Second, we did not have the prescribed amount of ESAs; thus, we were unable to calculate the resistance to ESAs, which would be associated with increased outcomes in CKD [8, 25]. In other words, our population included those for whom anemia was not corrected with ESA treatment, which may have affected the outcomes. Third, we did not measure serum factors involved in iron recycling or the hepcidin level, both of which contribute to anemia severity. Fourth, even by using the stratified analysis by CKD stages, an interaction between renal function and Hb levels may affect the relationship between Hb levels and outcomes. Accordingly, the present study did not assess the mechanism of or factors associated with anemia that may have contributed to the increased mortality. These needs to be addressed in future studies.
In conclusion, Hb levels <10 g/dL are a risk for poor clinical outcomes in patients with advanced CKD. However, the impact is different based on the CKD stage, with a significantly higher risk for CVEs and all-cause mortality in stage G3 and progression to ESKD in stages G4 and G5. In addition, Hb levels ≥12 g/dL were associated with lower risk in each CKD stage in a prospective observational cohort of Japanese outpatients with CKD who were receiving regular care. These findings will help to stratify the risk and to control anemia for CKD patients in each stage.
References
Go AS, Yang J, Ackerson LM, Lepper K, Robbins S, Massie BM, et al. Hemoglobin level, chronic kidney disease, and the risks of death and hospitalization in adults with chronic heart failure: the Anemia in Chronic Heart Failure: Outcomes and Resource Utilization (ANCHOR) Study. Circulation. 2006;113:2713–23.
Silverberg DS, Wexler D, Blum M, Tchebiner JZ, Sheps D, Keren G, et al. The effect of correction of anaemia in diabetics and non-diabetics with severe resistant congestive heart failure and chronic renal failure by subcutaneous erythropoietin and intravenous iron. Nephrol Dial Transplant. 2003;18:141–6.
Tseng CL, Kern EF, Miller DR, Tiwari A, Maney M, Rajan M, et al. Survival benefit of nephrologic care in patients with diabetes mellitus and chronic kidney disease. Arch Intern Med. 2008;168:55–62.
De Nicola L, Minutolo R, Chiodini P, Zamboli P, Cianciaruso B, Nappi F, et al. Prevalence and prognosis of mild anemia in non-dialysis chronic kidney disease: a prospective cohort study in outpatient renal clinics. Am J Nephrol. 2010;32:533–40.
De Nicola L, Chiodini P, Zoccali C, Borrelli S, Cianciaruso B, Di Iorio B, et al. Prognosis of CKD patients receiving outpatient nephrology care in Italy. Clin J Am Soc Nephrol. 2011;6:2421–8.
Drüeke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall IC, Tsakiris D, et al. Normalization of hemoglobin level in patients with chronic kidney disease and anemia. N Engl J Med. 2006;355:2071–84.
Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S, Wolfson M, et al. Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med. 2006;355:2085–98.
Pfeffer MA, Burdmann EA, Chen CY, Cooper ME, de Zeeuw D, Eckardt KU, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med. 2009;361:2019–32.
KDIGO Clinical Practice Guideline for Anemia in Chronic. Kidney disease. Kidney Int Suppl. 2012;2:279–335.
Japanese Society of Nephrology. Evidence-based practice guideline for the treatment of CKD. Clin Exp Nephrol. 2009;13:537–66.
Tsubakihara Y, Nishi S, Akiba T, Hirakata H, Iseki K, Kubota M, et al. 2008 Japanese Society for Dialysis Therapy: guidelines for renal anemia in chronic kidney disease. Ther Apher Dial. 2010;14:240–75.
Kuriyama S, Tomonari H, Yoshida H, Hashimoto T, Kawaguchi Y, Sakai O. Reversal of anemia by erythropoietin therapy retards the progression of chronic renal failure, especially in nondiabetic patients. Nephron. 1997;77:176–85.
Tsubakihara Y, Gejyo F, Nishi S, Iino Y, Watanabe Y, Suzuki M, et al. High target hemoglobin with erythropoiesis-stimulating agents has advantages in the renal function of non-dialysis chronic kidney disease patients. Ther Apher Dial. 2012;16:529–40.
Akizawa T, Gejyo F, Nishi S, Iino Y, Watanabe Y, Suzuki M, et al. Positive outcomes of high hemoglobin target in patients with chronic kidney disease not on dialysis: a randomized controlled study. Ther Apher Dial. 2011;15:431–40.
Akaishi M, Hiroe M, Hada Y, Suzuki M, Tsubakihara Y, Akizawa T, KRN321 Study Group. Effect of anemia correction on left ventricular hypertrophy in patients with modestly high hemoglobin level and chronic kidney disease. J Cardiol. 2013;62:249–56.
Iseki K, Ikemiya Y, Iseki C, Takishita S. Haematocrit and the risk of developing end-stage renal disease. Nephrol Dial Transplant. 2003;18:899–905.
Mohanram A, Zhang Z, Shahinfar S, Keane WF, Brenner BM, Toto RD. Anemia and end-stage renal disease in patients with type 2 diabetes and nephropathy. Kidney Int. 2004;66:1131–8.
Nakayama M, Sato T, Sato H, Yamaguchi Y, Obara K, Kurihara I. Different clinical outcomes for cardiovascular events and mortality in chronic kidney disease according to underlying renal disease: the Gonryo study. Clin Exp Nephrol. 2010;14:333–9.
Nakayama M, Sato T, Miyazaki M, Matsushima M, Sato H, Taguma Y, et al. Increased risk of cardiovascular events and mortality among non-diabetic chronic kidney disease patients with hypertensive nephropathy: the Gonryo study. Hypertens Res. 2011;34:1106–10.
Special report from the National Institute of Neurological. Disorders and Stroke. Classification of cerebrovascular diseases III. Stroke. 1990;21:637–76.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18:695–706.
Akizawa T, Saito A, Gejyo F, Suzuki M, Nishizawa Y, Tomino Y, et al. Impacts of recombinant human erythropoietin treatment during predialysis periods on the progression of chronic kidney disease in a large-scale cohort study (Co-JET study). Ther Apher Dial. 2014;18:140–8.
Gouva C, Nikolopoulos P, Ioannidis JP, Siamopoulos KC. Treating anemia early in renal failure patients slows the decline of renal function: a randomized controlled trial. Kidney Int. 2004;66:753–60.
Solomon SD, Uno H, Lewis EF, Eckardt KU, Lin J, Burdmann EA, et al. Erythropoietic response and outcomes in kidney disease and type 2 diabetes. N Engl J Med. 2010;363:1146–55.
Skali H, Lin J, Pfeffer MA, Chen CY, Cooper ME, McMurray JJ, et al. Hemoglobin stability in patients with anemia, CKD, and type 2 diabetes: an analysis of the TREAT (Trial to Reduce Cardiovascular Events With Aranesp Therapy) placebo arm. Am J Kidney Dis. 2013;61:238–46.
Akizawa T, Makino H, Matsuo S, Watanabe T, Imai E, Nitta K, et al. Management of anemia in chronic kidney disease patients: baseline findings from Chronic Kidney Disease Japan Cohort Study. Clin Exp Nephrol. 2011;15:248–57.
Acknowledgments
This study was supported by grants from Astellas Pharm Inc. The authors express special thanks to Ms. Yumi Yamaguchi and Ms. Ayuko Momoi for administrative assistance. Study contributors: Yuji Yamaguchi (Japanese Red Cross Sendai Hospital), Katsuya Obara (Tohoku Kosai Hospital), Isao Kurihara (Tohoku Kosai Miyagino Hospital), Yasumichi Kinoshita and Kazuto Sato (Japanese Red Cross Ishinomaki Hospital), Kazuro Kaise (Sendai Medical Center), Akira Sugiura and Masahiro Miyata (Osaki Citizen Hospital), Kazuhisa Takeuchi (Koujinkai Central Clinic), Kenji Nakayama and Naoki Akiu (Sendai City Hospital) and Tetsuya Otaka (Katta General Hospital). This study was supported by a grant from Astellas Pharm, Inc. and Miyagi Kidney Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s10157-017-1435-4.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Yamamoto, T., Miyazaki, M., Nakayama, M. et al. Impact of hemoglobin levels on renal and non-renal clinical outcomes differs by chronic kidney disease stages: the Gonryo study. Clin Exp Nephrol 20, 595–602 (2016). https://doi.org/10.1007/s10157-015-1190-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-015-1190-3