
Abstract
Purpose
Temporary ileostomy is sometimes created after colorectal surgery and may cause renal impairment. However, the impact of ileostomy on renal function during adjuvant chemotherapy for colorectal cancer (CRC) remains unknown. The aim of the present study was to examine the effects of ileostomy on renal function during adjuvant chemotherapy.
Methods
We examined 184 patients who received adjuvant CAPOX therapy (capecitabine and oxaliplatin) for CRC with or without ileostomy between January 2011 and December 2020 at the University of Tokyo Hospital. Clinicopathological factors, including renal function, were retrospectively reviewed in association with temporary ileostomy. Factors associated with reductions in the estimated glomerular filtration rate (eGFR) during CAPOX therapy were analyzed.
Results
Eighteen patients (10%) underwent temporary ileostomy. The maximum decrease in eGFR during CAPOX therapy was significantly higher in patients with than in those without ileostomy (− 16.1 vs. − 5.6 mL/min/1.73m2, p = 0.003). A multivariate analysis identified ileostomy as one of factors independently associated with reductions in eGFR during CAPOX therapy (p = 0.003). The cumulative number of readmission due to dehydration was also higher in patients with ileostomy (33% vs. 1%, p < 0.001).
Conclusions
Ileostomy significantly reduced eGFR during adjuvant CAPOX therapy. Therefore, renal function needs to be monitored during CAPOX therapy, particularly in patients with ileostomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is the fourth most commonly diagnosed and third most deadly cancer worldwide [1, 2], and radical surgery is the mainstay of treatment for patients with resectable CRC. Based on the significant efficacy of 5-fluorouracil and oxaliplatin for reducing the postoperative recurrence of CRC after curative resection [3,4,5], a growing number of CRC patients are likely to receive oxaliplatin-based adjuvant chemotherapy after radical colorectal surgery to prevent recurrence [6,7,8,9]. However, CAPOX therapy, a standard adjuvant regimen consisting of capecitabine and oxaliplatin, frequently causes digestive toxicities, such as vomiting and diarrhea, which may result in renal impairment [10].
Anastomotic leakage remains a severe complication after colorectal surgery, with considerable morbidity and adverse oncological outcomes [11, 12]. Previous studies showed that stoma creation reduced the risk of reoperation and sepsis in colorectal surgery [13, 14]; therefore, a covering stoma is often constructed to protect an anastomosis. Stomas are often accompanied by several morbidities, such as wound infection, prolapse, parastomal hernia, skin irritation, and a high output [13,14,15]. Ileostomy is now more frequently selected, because overall stoma-related comorbidities are less frequent than in colostomy patients [13,14,15,16].
One of the most common complications of ileostomy is dehydration. A high stoma output results in the depletion of salt and water, and is also a common cause of readmission [17,18,19]. Therefore, patients with ileostomy may be susceptible to chemotherapy-induced dehydration. However, limited information is currently available on the relationship between ileostomy and renal dysfunction induced by CAPOX therapy.
The aim of the present study was to clarify changes in the renal function of CRC patients with ileostomy during the sequence of surgery and adjuvant CAPOX, and investigate whether temporary ileostomy is a risk factor for renal dysfunction caused by CAPOX therapy.
Materials and methods
Patients
We investigated consecutive patients who received CAPOX therapy for CRC in the adjuvant setting between January 2011 and December 2020 at the University of Tokyo Hospital. Patients who received adjuvant chemotherapy at other hospitals, those who underwent stoma closure in the middle of chemotherapeutic cycles, patients who experienced the recurrence of CRC within 6 months after radical resection, and those without available data on renal function before, during, or after CAPOX were excluded.
For comparison of postoperative change in renal function, we also investigated consecutive patients who underwent ileostomy creation and were followed without adjuvant chemotherapy during the same study period. Patients who underwent stoma closure within a month, and those who were followed up for less than 6 months after radical resection were excluded. Patients who experienced the recurrence of CRC within 6 months after radical resection, and those without available data on renal function were excluded as well.
From the patients collected as mentioned above, those without available data on renal function 1 year after index surgery were further excluded in the long-term analysis.
The present study was approved by the Ethics Committees of the University of Tokyo (No. 3252-[13]).
Stoma creation
Most patients with colon cancer underwent colectomy with an anastomosis, whereas a double-barreled stoma was created in patients after the resection of the tumor-bearing segment under specific conditions, such as bowel obstruction, severe hypoalbuminemia, and/or preoperative high-dose steroid use [20, 21]. Some patients with rectal cancer who underwent anterior resection and a stapled anastomosis were also subjected to stoma creation at the surgeon’s discretion in consideration of the conditions mentioned above and other factors, such as tumor height from the anal verge and preoperative chemoradiotherapy [16]. We created a diverting stoma in all rectal cancer patients undergoing intersphincteric resection. The terminal ileum 40 cm proximal to the ileocecal valve was generally selected as a diverting stoma site in patients with rectal cancer; however, colostomy was constructed for selected patients when they were considered to have a reduced chance of stoma reversal based on additional factors, including age and anorectal function [16]. When patients with a stoma showed a high output, we prescribed probiotics and/or antidiarrheal agents.
In patients with a diverting stoma, we performed stoma closure essentially after the completion of adjuvant chemotherapy.
Chemotherapy
CAPOX therapy consisted of the intravenous infusion of oxaliplatin at 130 mg/m2 and the oral administration of capecitabine at a dose of 1000 mg/m2 twice daily for 2 weeks. The treatment course was repeated every 3 weeks [10]. The initial dose intensities of CAPOX were reduced for some patients at the discretion of the attending doctor in consideration of the age of patients, the Eastern Cooperative Oncology Group performance status, and comorbidities.
Basically, the first cycle of CAPOX was administrated in hospital, and subsequent cycles of CAPOX at outpatient clinic. When patients exhibited severe dehydration, patients were readmitted and treated with intravenous fluid replacement.
Data extraction
We retrieved the following data: sex, age, height, weight, body mass index, comorbidities, such as diabetes, hypertension, cardiac, pulmonary, renal, and hepatic diseases, use of steroids, the primary location and cancer stage at diagnosis according to the American Joint Committee on Cancer staging manual [22], a history of preoperative chemoradiotherapy, relative dose intensities of chemotherapeutic drugs, total cycles of CAPOX, reasons for discontinuation of CAPOX, total number of readmission, and reasons for readmission.
Measurement of eGFR
As an index of renal function, we examined the estimated glomerular filtration rate (eGFR). eGFR was calculated using the Japanese Society of Nephrology formula as follows: eGFR (mL/min/1.73m2) = 194 × serum creatinine−1.094 × age−0.287 (× 0.739 if female) [23].
In the analysis of changes in eGFR of patients during CAPOX therapy, we divided patients into two groups according to ileostomy, namely, the ‘Ileostomy’ and ‘Non-ileostomy’ groups. Patients with colostomy were classified into the Non-ileostomy group. We measured eGFR at the following timepoints: before the first cycle of CAPOX as baseline (usually at the first outpatient visit after discharge), before each subsequent course of CAPOX, within 3 months after the last course of CAPOX, and 1 year after index surgery. eGFR was additionally measured when patients exhibited symptoms suggestive of dehydration. We also reviewed the lowest eGFR value during all CAPOX cycles. According to the RIFLE criteria for acute kidney injury [24], we defined > 25% reduction in eGFR from the baseline as clinically important renal impairment.
In patients with temporary ileostomy who did not receive adjuvant chemotherapy, we retrieved eGFR at the first outpatient visit after discharge as baseline. In addition, we extracted the lowest eGFR value before stoma closure.
Statistical analyses
Statistical analyses were performed using JMP Pro 15.0.0 (SAS institute, Cary, NC, USA). All variables were summarized as medians (range), means ± standard deviations, or numbers (percentages). Quantitative variables were compared using the Mann–Whitney U test. Categorical variables were compared using Fisher’s exact test. Univariate and multivariate regression analyses were performed to identify risk factors for reductions in eGFR during CAPOX therapy. Variables with a p value less than 0.05 in the univariate analysis were subjected to a multivariate analysis. All reported p values were two-sided, and results were considered to be significant if the p value was less than 0.05.
Results
Among 187 patients who received adjuvant CAPOX therapy, 184 were included in the present study. Eighteen patients (10%) underwent ileostomy (Fig. 1).

Study flow diagram for analyses
Table 1 summarizes the details of patients divided according to ileostomy. There were significantly more male patients in the Ileostomy group (78% vs. 52%, p = 0.047). Patients with hypertension were only present in the non-ileostomy group (0% vs. 30%, p = 0.004). All patients in the Ileostomy group underwent surgery for rectal cancer (p < 0.001), and, thus, significantly more patients received preoperative chemoradiotherapy (39%) in the Ileostomy group than in the Non-ileostomy group (7%, p < 0.001). Other background characteristics were similar between the two groups.
Table 2 shows the outcomes of adjuvant CAPOX therapy. CAPOX was discontinued due to dehydration more frequently in the Ileostomy group than the Non-ileostomy group (11% vs. 0%, p = 0.009). In addition, there were more patients readmitted for dehydration (33% vs. 1%, p < 0.001) and allergy (6% vs. 0%, p = 0.002) in the Ileostomy group. No significant differences were observed in other parameters between the two groups.
Mean eGFR at baseline was 77.7 in the Ileostomy group and 78.5 in the Non-ileostomy group (p = 0.95). Figure 2 shows changes in eGFR in the Ileostomy and Non-ileostomy groups. The minimum eGFR in both groups during CAPOX was significantly lower than the baseline (p = 0.008, p = 0.002) and recovered after CAPOX. eGFR 1 year after index surgery was similar to the level before CAPOX in both groups.

eGFR values in patients with or without ileostomy during sequential treatments of surgery and adjuvant CAPOX. eGFR estimated glomerular filtration rate; *: p < 0.05 vs. eGFR before CAPOX; †: the lowest eGFR during CAPOX therapy
The changes observed in eGFR over the treatment course of CAPOX were compared between the Ileostomy and Non-ileostomy groups. As shown in Fig. 3, the magnitude of the maximum reduction in eGFR was significantly larger in the Ileostomy group than in the Non-ileostomy group during CAPOX therapy (− 16.1 vs. − 5.6 mL/min/1.73m2, p = 0.003). However, no intergroup difference was noted in changes in eGFR at the end of CAPOX therapy from baseline (Fig. 3).

Comparison of reductions in eGFR between Ileostomy and Non-ileostomy groups. eGFR estimated glomerular filtration rate; †: the maximum reduction in eGFR during CAPOX therapy
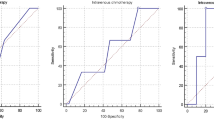
Figure 4 shows the timepoint at which eGFR decreased the most during CAPOX therapy. The maximum reduction in eGFR was frequently observed in the first cycle of CAPOX in 83 patients (45%), and during the latter four cycles of CAPOX in 46 patients (25%). When confined to the Ileostomy group (18 patients), more patients (33%, six patients) showed the lowest eGFR during the latter four cycles (Fig. 4 inset).

Timepoint at which the maximum reduction in eGFR occurred during CAPOX therapy. Results for the Ileostomy group alone were shown in the inset
We analyzed clinicopathological factors to identify risk factors for reductions in eGFR during CAPOX therapy. As shown in Table 3, the univariate analysis demonstrated that the decline in eGFR during CAPOX therapy correlated with ileostomy (p < 0.001), eGFR before CAPOX (p = 0.006), rectal tumor (p = 0.014), and preoperative CRT (p = 0.010). Among these variables, ileostomy and eGFR before CAPOX were independently associated with reductions in eGFR during CAPOX therapy in the multivariate analysis (p = 0.003 and p = 0.005, respectively, Table 3).
Finally, we compared postoperative changes in eGFR in ileostomy patients classified according to the implementation of adjuvant CAPOX. Compared to 178 patients with ileostomy who did not receive adjuvant chemotherapy (Supplementary Figure 1), patients in the Ileostomy group were diagnosed at more advanced stage (p < 0.001, Supplementary Table 1). The magnitude of the maximum reduction in eGFR was larger in the Ileostomy group than in ileostomy patients without adjuvant chemotherapy (− 16.1 vs. − 8.3, p = 0.018, Supplementary Table 2). The accumulated number of readmission due to dehydration was also higher in the Ileostomy group than in ileostomy patients without CAPOX (33% vs. 3%, p = 0.004, Supplementary Table 2).
Discussion
Previous studies reported that ileostomy formation caused renal impairment in 0.8–20% of treated patients [17,18,19, 25]. The decline in eGFR associated with ileostomy ranged between 4.4 and 6.0 mL/min/1.73m2 [26,27,28]. However, changes in eGFR during adjuvant CAPOX therapy remain unclear. The present study is the first to investigate declines in eGFR during CAPOX therapy in patients with diverting ileostomy.
We showed that eGFR in patients with ileostomy decreased by up to 16.1 mL/min/1.73m2 during CAPOX (Fig. 3), and that patients with ileostomy were readmitted more frequently than patients without ileostomy during CAPOX therapy (Table 1). Moreover, ileostomy formation was identified as an independent risk factor for renal dysfunction during CAPOX (Table 2). CAPOX therapy often induces dehydration through digestive toxicities, including diarrhea. A clinical trial previously demonstrated that 3% of patients developed grade 3/4 dehydration during CAPOX therapy [10]. In addition, ileostomy patients were more susceptible to dehydration due to the high-volume output of intestinal fluids from ileostomy and/or fluid malabsorption in the colon [29,30,31]. On the other hand, we demonstrated that ileostomy alone did not cause a considerable decline in eGFR and frequent readmission by the comparative analyses between ileostomy patients with and without CAPOX (Supplementary Table 2). Therefore, significant declines in renal function may be attributed to complications caused by both ileostomy and chemotherapy in the patients examined in the present study.
During CAPOX therapy, the first cycle was the most frequent timepoint at which the maximum reduction in eGFR was observed (Fig. 4). Regarding the prevention of renal dysfunction after ileostomy formation, previous studies underscored the importance of the early management of fluids and electrolytes after surgery [25, 32]. Due to the decline in eGFR induced by CAPOX, early management may be of similar importance, particularly in ileostomy patients receiving CAPOX therapy. In our hospital, we implemented early intervention if patients exhibited symptoms of dehydration. This might contribute to preventing further decreases in eGFR after the first cycle of CAPOX.
In addition, temporary ileostomy closure before adjuvant CAPOX may be an alternative way to reduce the potential risk of renal impairment. Several studies showed that delay in adjuvant chemotherapy was associated with worse survival [33, 34]. Clinical guidelines recommend that adjuvant chemotherapy should be initiated within 8 weeks after radical resection [6, 7, 35]. On the other hand, patients are usually readmitted to undergo elective stoma closure after hospitalization for CRC surgery due to the rules of the health insurance system in Japan. Yaegashi et al. proposed early stoma closure in selected patients as renal impairment observed after ileostomy did not improve after stoma closure [27]. Therefore, early stoma closure before the implementation of adjuvant chemotherapy is a practical option for selective patients who did not develop postoperative complications after radical resection.
The lowest eGFR was noted in 25% of patients showed after four cycles of CAPOX, and ileostomy patients showed declines in eGFR in the latter half cycle more frequently than those without ileostomy (Fig. 4). The IDEA collaboration demonstrated that adjuvant CAPOX therapy for 3 months was not inferior to that for 6 months in low-risk stage III CRC patients with a depth of T1–3 and N1 lymph node metastasis [36, 37]. Therefore, we recommend 3 months of CAPOX therapy for patients with the above risk factors for CAPOX-induced declines in eGFR.
The present study has several limitations. It was a retrospective study conducted at a single hospital with a small patient cohort. There were differences in several baseline characteristics between the groups. For example, ileostomy was created in only rectal cancer patients. However, we consider that the renal function during adjuvant chemotherapy after surgery is basically independent of primary tumor location. Moreover, this study may have included a selection bias; adjuvant CAPOX may not have been selected for elderly patients or those with background comorbidities, including renal dysfunction. In addition, we did not measure the daily ileostomy output after discharge. Furthermore, the relationship between renal impairment induced by CAPOX and long-term renal function or survival was not investigated. We could not compare long-term changes in eGFR in ileostomy patients followed without CAPOX as most of these patients received stoma closure within a few months.
Conclusions
Ileostomy is a risk factor for renal impairment during CAPOX therapy. Future studies with a larger patient cohort are needed to confirm the present results. Renal function needs to be carefully monitored during CAPOX therapy, particularly in patients with ileostomy.
Data availability
The data sets during and/or analyzed during the current study available from the corresponding author on reasonable request.
References
Bray F, Ferlay J, Soerjomataram I et al (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6):394–424
Rawla P, Sunkara T, Barsouk A (2019) Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol 14(2):89–103
Laurie JA, Moertel CG, Fleming TR et al (1989) Surgical adjuvant therapy of largebowel carcinoma : an evaluation of levamisole and the combination of levamisole and fluorouracil. The North Central Cancer Treatment Group and the Mayo Clinic. J Clin Oncol 7(10):1447–1456
Moertel CG, Fleming TR, Macdonald JS et al (1990) Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med 322:352–358
Moertel CG, Fleming TR, Macdonald JS et al (1995) Fluorouracil plus levamisole as effective adjuvant therapy after resection of stage III colon carcinoma : a final report. Ann Intern Med 122:321–326
National Comprehensive Cancer Network (2022) Clinical Practice Guidelines in Oncology. Colon Cancer, version 1.2022. https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 5 Apr 2022.
National Comprehensive Cancer Network (2022) Clinical practice guidelines in oncology. Rectal Cancer, version 1.2022. https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 5 Apr 2022.
Nozawa H, Kawai K, Sasaki K et al (2021) Women are predisposed to early dose-limiting toxicities during adjuvant CAPOX for colorectal cancer. Int J Clin Pract 75(11):e14863
Osumi H, Shinozaki E, Suenaga M et al (2017) Change in clinical outcomes during the transition of adjuvant chemotherapy for stage III colorectal cancer. PLoS ONE 12(5):e0176745
Schmoll HJ, Cartwright T, Tabernero J et al (2007) Phase III trial of capecitabine plus oxaliplatin as adjuvanttherapy for stage III colon cancer: a planned safetyanalysis in 1864 patients. J Clin Oncol 25(1):102–109
Mirnezami A, Mirnezami R, Chandrakumaran K et al (2011) Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg 253(5):890–899
Ashburn JH, Stocchi L, Kiran RP et al (2013) Consequences of anastomotic leak after restorative proctectomy for cancer: effect on long-term function and quality of life. Dis Colon Rectum 56(3):275–280
Rondelli F, Reboldi P, Rulli A et al (2009) Loop ileostomy versus loop colostomy for fecal diversion after colorectal or coloanal anastomosis: a meta-analysis. Int J Colorectal Dis 24(5):479–488
Tilney HS, Parvinder SS, Lovegrove RE et al (2007) Comparison of outcomes following ileostomy versus colostomy for defunctioning colorectal anastomoses. World J Surg 31(5):1142–1151
Chudner A, Gachabayov M, Dyatlov A et al (2019) The influence of diverting loop ileostomy vs. colostomy on postoperative morbidity in restorative anterior resection for rectal cancer: a systematic review and meta-analysis. Langenbecks Arch Surg 404(2):129–139
Fukui R, Nozawa H, Hirata Y et al (2021) Low preoperative maximum squeezing pressure evaluatedby anorectal manometry is a risk factor for non-reversal of divertingstoma. Langenbecks Arch Surg 406(1):131–139
Gessler B, Haglind E, Angenete E (2012) Loop ileostomies in colorectal cancer patients–morbidity and risk factors for nonreversal. J Surg Res 178(2):708–714
Feinberg SM, McLeod RS, Cohen Z (1987) Complications of loop ileostomy. Am J Surg 153(1):102–107
Justiniano CF, Temple LK, Swanger AA et al (2018) Readmissions with dehydration after Ileostomy creation: rethinking risk factor. Dis Colon Rectum 61(11):1297–1305
Konishi T, Watanabe T, Kishimoto J et al (2006) Risk factors for anastomotic leakage after surgery for colorectal cancer: results of prospective surveillance. J Am Coll Surg 202(3):439–444
Suding P, Jensen E, Abramson MA et al (2008) Definitive risk factors for anastomotic leaks in elective open colorectal resection. Arch Surg 143(9):907–911
Amin MB, Edge S, Greene F et al (2017) AJCC cancer staging manual, 8th edn. Springer, NewYork (NY)
Matsuo S, Imai E, Horio M et al (2009) Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 53(6):982–992
Bellomo R, Ronco C, Kellum JA et al (2004) Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care 8(4):R204-212
Beck-Kaltenbach N, Voigt K, Rumstadt B (2011) Renal impairment caused by temporary loop ileostomy. Int J Colorectal Dis 26(5):623–626
Gessler B, Haglind E, Angenete E (2014) A temporary loop ileostomy affects renal function. Int J Colorectal Dis 29(9):1131–1135
Yaegashi M, Otsuka K, Kimura T et al (2020) Early renal dysfunction after temporary ileostomy construction. Surg Today 50(3):703–710
Fielding A, Woods R, Moosvi SR et al (2020) Renal impairment after ileostomy formation: a frequent event with long-term consequences. Colorectal Dis 22(3):269–278
Paquette IM, Solan P, Rafferty JF et al (2013) Readmission for dehydration or renal failure after ileostomy creation. Dis Colon Rectum 56(8):974–979
Shabbir J, Britton DC (2010) Stoma complications: a literature overview. Colorectal Dis 12(10):958–964
Messaris E, Sehgal R, Deiling S et al (2012) Dehydration is the most common indication for readmission after diverting ileostomy creation. Dis Colon Rectum 55(2):175–180
Migdanis A, Koukoulis G, Mamaloudis I et al (2018) Administration of an oral hydration solution prevents electrolyte and fluid disturbances and reduces readmissions in patients with a diverting ileostomy after colorectal surgery: a prospective, randomized, controlled trial. Dis Colon Rectum 61(7):840–846
Biagi JJ, Raphael MJ, Mackillop WJ et al (2011) Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: a systematic review and meta-analysis. JAMA 305(22):2335–2342
Sun Z, Adam MA, Kim J et al (2016) Determining the optimal timing for initiation of adjuvant chemotherapy after resection for stage II and III colon cancer. Dis Colon Rectum 59(2):87–93
Hashiguchi Y, Muro K, Saito Y et al (2020) Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol 25(1):1–42
Grothey A, Sobrero AF, Shields AF et al (2018) Duration of adjuvant chemotherapy for stage III colon cancer. N Eng J Med 378(13):1177–1188
Andre T, Meyerhardt J, Iveson T et al (2020) Effect of duration of adjuvant chemotherapy for patients with stage III colon cancer (IDEA collaboration): final results from a prospective, pooled analysis of six randomised, phase 3 trials. Lancet Oncol 21(12):1620–1629
Author information
Authors and Affiliations
Contributions
KO, HN and SI developed the study design and concept, retrieved the data of patients and carried out the analysis. KO, HN, KS, KM, SE and SI participated in writing and revising the manuscript critically. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was approved by the Ethics Committees of the University of Tokyo (No. 3252-(13)).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
About this article

Cite this article
Okamoto, K., Nozawa, H., Sasaki, K. et al. Diverting ileostomy is a risk factor for renal impairment during CAPOX therapy. Int J Clin Oncol 27, 1616–1623 (2022). https://doi.org/10.1007/s10147-022-02217-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-022-02217-6