
Abstract
Bypass revascularization helps prevent complications in Moyamoya Disease (MMD). To systematically review complications associated with combined direct and indirect (CB) bypass in MMD and analyze differences between the adult and pediatric populations. A systematic literature review was conducted per PRISMA guidelines. PUBMED, Cochrane Library, Web of Science, and CINAHL, were queried from January 1980 to March 2022. Complications were defined as any event in the immediate post-surgical period of a minimum 3 months follow-up. Exclusion criteria included lack of surgical complication reports, non-English articles, and CB unspecified or reported separately. 18 final studies were included of 1580 procured. 1151 patients (per study range = 10—150, mean = 63.9) were analyzed. 9 (50.0%) studies included pediatric patients. There were 32 total hemorrhagic, 74 total ischemic and 16 total seizure complications, resulting in a rate of 0.04 (95% CI 0.03, 0.06), 0.7 (95% CI 0.04, 0.10) and 0.03 (95% CI 0.02, 0.05), respectively. The rate of hemorrhagic complications in the pediatric showed no significant difference from the adult subgroup (0.03 (95% CI 0.01—0.08) vs. 0.06 (95% CI 0.04—0.10, p = 0.19), such as the rate of ischemic complications (0.12 (95% CI 0.07—0.23) vs. 0.09 (95% CI 0.05—0.14, p = 0.40). Ischemia is the most common complication in CB for MMD. Pediatric patients had similar hemorrhagic and ischemic complication rates compared to adults.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Moyamoya disease (MMD) is an idiopathic, progressive, and rare cerebrovascular disease with a relatively high incidence in East Asian populations [20, 30], characterized by chronic progressive stenosis at the apices of the intracranial internal carotid arteries (ICA) [1, 30]. In response to the reduction in cerebral blood flow due to ICA stenosis, there is a compensatory development of structurally fragile collateral vasculature, which appears on a cerebral angiogram like a "puff of smoke," translating in Japanese to its name, “moyamoya.” Moyamoya carries a high risk of ischemic and hemorrhagic stroke, at approximately 5% [4, 8, 25, 30]. Bypass revascularization surgery is often performed to reduce the risk of strokes.
Bypass revascularization strategies consist of direct (DB), indirect (IB), or combined direct and indirect (CB) approaches, which describe whether the anastomosed artery is connected directly to the vessel or laid directly on the brain for indirect angiogenesis. The results of CB have been previously summarized in the literature regarding patients' clinical features, surgical techniques, and outcomes [31]. However, no consensus exists regarding the frequency of complications following combined revascularization surgery. A comprehensive report on the rate of complications associated with CB would be valuable to counsel patients preoperatively and help guide future treatment guidelines. Herein, the present study aims to conduct a systematic review and meta-analysis of the literature to assess the complications of CB techniques in MMD treatment.
Methods
Literature search
A systematic literature review on CB for MMD was conducted per the PRISMA guidelines. The search string used to query the databases was: ("moyamoya" OR "moya-moya" OR "moya moya") AND ("combined" OR "direct" OR "indirect" OR "bypass" OR "revascularization"). The search terms were queried using PUBMED, Cochrane Library, Web of Science, and CINAHL from January 1, 1980, to March 1, 2022. The quality of each study was assessed with the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework, and the risk of bias was assessed with the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool [32].
Inclusion and exclusion criteria
Literature in the English language that presented a CB to the present day was considered. We included only clinical case series that presented combined bypass complications for MMD with a minimum of a three-month follow-up. Articles in which complications could not be individually analyzed were excluded. Letters to the editor and commentaries were also excluded from the initial review. Studies involving only DB or IB were excluded. Patients with Moyamoya syndrome were excluded from the study. Studies were reviewed thoroughly, and data obtained included author and year of publication, the treatment option, number of patients, outcome, complications, and follow-up period. The age of cutoff for adults was defined per individual study protocol, but most commonly, 16 years of age.
The assessment of complications encompassed ischemic, hemorrhagic, and seizure events. This evaluation was shaped by the limited number of studies reporting complications, as well as considerations pertaining to the inherent characteristics of the techniques analyzed. Ischemic events such as transient ischemic attacks (TIAs) and minor strokes were considered as ischemic complication, while hemorrhagic complication encompassed events such as intracranial hemorrhages and hematomas.
Study selection
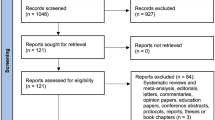
The search strategy revealed a total of 1580 articles. The detailed selection process is depicted in Supplemental Fig. 1. After the critical review of all the articles, studies were finally included in this systematic review. Reference lists of the articles were manually searched to ensure all the potential studies were included. Two independent reviewers (S.B. and D.O.) performed the data analysis and extraction, with disagreements settled by a senior author (R.B.)

Hemorrhagic Complications – All Patient Cohorts. Thirty-two total hemorrhagic complications occurred in 1151 patients. The overall weighted rate of hemorrhagic events (I.2 = 24%) was 0.04 (95% CI 0.03, 0.06)
Statistical analysis
Statistical analyses included data aggregation and exploratory and multivariate analyses using R, version 4.0.1 (R Foundation for Statistical Computing). Significance was defined as p < 0.05. A Fisher scoring algorithm was used to generate a meta-analysis of relevant studies. The rate of complications was calculated as the number of complications experienced per the total number of patients. For the analysis of rates, an inverse variance methodology was used. Heterogeneity across studies was evaluated using Cochran's Q test, I2 test, and τ2 test. An I2 value greater than 50% indicated high statistical heterogeneity, for which a random-effects model was used. A random-effects model was used for all analyses due to heterogeneity and all comparisons that utilized meta-regression. Chi-squared tests were used to test for differences between cohorts. A meta-regression analysis was used to test for significant differences between pooled meta-analyses of rates.
Results
Literature review
A total of 1580 studies were procured. Of these, 377 were removed as duplicates. The titles of 1167 studies were screened manually and by automated tools, and 1080 articles were excluded. Eighty-seven reports were available for an abstract/full-text review. Sixty-nine articles were excluded per our exclusion criteria, with 18 final studies included (Supplemental Fig. 1).
Baseline characteristics
A total of 1151 patients (per study range = 10—150, mean = 63.9) who underwent combined revascularization were analyzed in our study (Table 1). 9 (50.0%) studies included pediatric patients. Hemorrhagic, ischemic, and seizure complications were reported in all 18 articles. With respect to GRADE quality of evidence, 3 (16.7%) had low quality, 10 (55.6%) had medium quality, and 5 (27.8%) had a high quality of evidence. All studies were rated as having a medium risk of bias with respect to ROBINS-I evaluation.
Angiographic
The most common techniques in the population were STA-MCA (superficial temporal artery to the middle cerebral artery) + EDMS (encephalo-duro-myo-synangiosis), present in 5 (27.8%) studies; STA-MCA + EDAS (encephalo-duro-arterio-synangiosis), present in 4 (22.2%) studies; STA-MCA + EMS (encephalo-myo-synangiosis), present in 3 (16.7%) studies, STA-MCA + EDMAPS (encephalo-duro-myo-arterio-pericranial-synangiosis) present in 2 (11.1%) studies, STA-MCA + EDMAS (encephalo-duro-myo-arterio-synangiosis) present in 1 (5.5%) study, STA-MCA + EDGS (encephalo-duro-galeo-synangiosis) present in 1 (5.5%) study, and STA-MCA + EDS (encephalo-duro-synangiosis) present in 1 (5.5%) study and STA-MCA + TPFF (pedicled temporoparietal fascial flap) present in 1 (5.5%) study.
Complications
Thirty-two total hemorrhagic complications occurred in 1151 patients (Fig. 1). A common-effects model was used to evaluate the overall weighted rate of hemorrhagic events (I2 = 24%), resulting in a rate of 0.04 (95% CI 0.03, 0.06). Seventy-four total ischemic complications occurred in 1151 patients (Fig. 2). A random-effects model was used to evaluate the overall weighted rate of ischemic events (I2 = 64%), resulting in a rate of 0.07 (95% CI 0.04, 0.10). Sixteen total seizure complications occurred in 1151 patients (Fig. 3). A common-effects model was used to evaluate the overall weighted rate of seizure events (I2 = 11%), resulting in a rate of 0.03 (95% CI 0.02, 0.05).

Ischemic Complications – All Patient Cohorts.Seventy-four total ischemic complications occurred in 1151 patients. The overall weighted rate of hemorrhagic events (I.2 = 64%) was 0.07 (95% CI 0.04, 0.10)

Seizure Complications – All Patient Cohorts. Sixteen total seizure complications occurred in 1151 patients. The overall weighted rate of seizure events (I.2 = 11%) was 0.03 (95% CI 0.02, 0.05)
Pediatric versus adult comparison
10 (55.6%) studies reported on the adult population alone in 431 patients, 5 (27.8%) studies reported on the pediatric population in 229 total patients, and 4 (22.2%) studies reported on a mixed population of adults and pediatrics in 491 patients. Of the 14 studies that reported on purely adult or pediatric studies or separated the two within the article, a meta-regression was conducted to evaluate for subgroup differences in instances where the Fisher scoring algorithm was able to converge (hemorrhagic and ischemic complications). The rate of hemorrhagic complications in the pediatric subgroup was found to be not significantly different when compared to the adult subgroup (0.03 (95% CI 0.01—0.08) vs. 0.06 (95% CI 0.04—0.10, p = 0.19) (Fig. 4). The rate of ischemic complications in the pediatric subgroup was also found not to be significantly different from the adult subgroup (0.12 (95% CI 0.07—0.23) vs. 0.09 (95% CI 0.05—0.14, p = 0.40) (Fig. 5). Muscle use in the indirect component of the combined bypass was utilized in 11 (61.1%) of studies or 755 (65.5%) of 1151 patients.

Hemorrhage Complications – Pediatrics vs Adult Meta Regression. Data analysis above show that there was no significant difference on the rate of hemorrhagic complications between pediatric vs adult subgroups (0.03 (95% CI 0.01—0.08) vs. 0.06 (95% CI 0.04—0.10, p = 0.19)

Ischemic Complications – Pediatrics vs Adult Meta Regression. There was no statistically significant difference between pediatric vs adult subgroups (0.12 (95% CI 0.07—0.23) vs. 0.09 (95% CI 0.05—0.14, p = 0.40)
Discussion
Since the 1970s, STA-MCA anastomosis has been used in MMD patients [18]. Successful anastomosis between the donor and recipient arteries can improve blood flow immediately after surgery [5]. Bypass surgery contributes to improving neurological and neurocognitive status as well as secondary stroke prevention in MMD patients. To the author's knowledge, no consensus or unified review exists on the frequency of complications following approaches for MMD. Herein, ischemic events were the most ubiquitous complication experienced among adult and pediatric populations, followed by hemorrhagic and seizure events. In the adult group, most CB cases utilized an STA-MCA with EDMS technique, while the pediatric population routinely underwent an STA-MCA with EMS.
A prior study by Choi et al. demonstrated that adults with MMD treated conservatively tend to have hemorrhagic manifestations, while younger children tend to have ischemic presentations [6]. Another study found the hemorrhage rate in non-surgically treated adults with MMD as high as 17.9% [13], with the recurrent hemorrhage rates of around 16.9% [21]. The non-surgically treated pediatric population was seen to have infarct rates of up to 21%, and almost 52% had frequent transient ischemic attacks [6]. Our findings indicate a lower rate of complications with CB relative to these reported rates without complication, suggesting that CB is an effective therapy against MMD progression. In a comprehensive pooled analysis comparing CB, DB, and IB techniques, Nguyen et al. found no discernible distinctions between CB and either of the other two methods, except in specific instances, with early hemorrhagic events exhibiting a preference for CB, while late ischemic events were inclined towards DB [24]. Furthermore, a CB may be necessary for pediatric patients as it could enhance treatment longevity through its direct and indirect combined methods of vascularization. However, the incidence of complications, as shown in the present study, is limited due to the relatively small number of studies reporting on this metric. Thus, future studies should aim to include more patients and more extended follow-up periods to enhance our understanding of this practice.
Interestingly, the present study observed that pediatric patients experienced ischemic complications at the same rate as adults. This is in light of the different anatomy of pediatric patients and the overall smaller caliber vessel size. The data on the pediatric population of MMD is much sparser than the adult population. Revascularization surgery for pediatrics depends on factors such as patient age, presenting symptoms, and institutional practices. Factors dissuading the use of DB in pediatric MMD treatment include smaller-caliber recipient and donor vessels, longer operative times, potential for poor scalp wound healing, and risks associated with temporary clamping. Ravindran et al. 2019, a meta-analysis of 29 studies, found that stroke rates for IB, DB indirect, direct, and CB were 9, 4.5, and 6%, respectively [28]. Fung et al. 2005 found that the perioperative stroke rate for pediatric MMD treatment was 4%, with no difference in stroke incidence between IB and DB cohorts [12]. In a long-term follow-up study of 23 pediatric patients who underwent CB [26], only three postoperative strokes were observed: 2 cases of hyperperfusion and 1 case of minor perioperative stroke. These studies suggest that although CB procedures may be superior to non-combined procedures, the risk of ischemic events is still significantly high in the pediatric population.
CB has been shown to be effective in improving blood flow to the brain in children with MMD. In one study, children who underwent CB had significantly improved blood flow to the brain compared to those who did not undergo surgery. Furthermore, most children who underwent CB experienced an improvement in their symptoms and a reduction in the number of recurrent strokes. However, it is essential to note that CB is a complex and potentially uncertain procedure. It is typically only recommended for children with severe MMD who are at high risk of recurrent strokes or other complications. As with any surgical procedure, risks are involved, including the potential for complications such as infection, bleeding, and brain damage. Therefore, the decision to undergo CB should be made in consultation with a team of experienced healthcare providers.
Out of 18 included studies, roughly 84% originated from Asian countries, while only 16% originated from Europe and USA. Notably, this may be due to the higher prevalence in East Asian countries, like Japan and Korea [14], compared to the USA [33]. This significantly lower prevalence and incidence may directly affect the standard of care between these two regions. Interestingly, literature was mainly sourced from 4 countries performing STA-MCA procedures for treating MMD: USA, Germany, Japan, Korea, and China; STA-MCA + EDMS was the most common procedure recorded in the present study and was only reported from Japan and China. These countries also reported cases of STA-MCA with EDAS, a technique also reported in the USA. The use of STA-MCA + EDMS in both the US and Asian countries may be due to more favorable long-term outcomes when compared with STA-MCA + EMS [11, 16]. Overall, the combination of Japan, China, and Korea had the broadest range of surgical treatments for MMD: STA-MCA with EDAS, EDMS, EMS, EDAMS, EDMAPA, EDGS, and EDS. Compared to the USA or Germany, this wide variability is likely due to the higher prevalence of MMD in Asian countries, lending to an increase in surgical options and better outcomes [1].
Limitations
Our study has limitations inherent to a meta-analysis, including selection bias, heterogeneity of included studies, and publication bias. The inclusion criteria for the present study had a minimum of 3 months of follow-up; however, three studies did not define the full range of long-term follow-up. This includes two studies that stated at least six months and 1 study that stated at least 12 months in their methods, which limits the understanding of the study's entire follow-up period. The age of what defined an adult in the included articles varied between studies. Furthermore, our study has limitations as it exclusively concentrated on analyzing ischemic, hemorrhagic, and seizure complications, without addressing other potential complications like those related to wound healing.
Conclusion
Ischemic events are the most common complication in CB for MMD. Compared to the adult population, pediatric patients had a non-significant difference in the rate of either ischemic or hemorrhagic complications. Understanding the overall and age-specific complication rates may help counsel patients and potentially guide the clinical management of these patients. More extensive studies will help confirm and expand knowledge of the differences between adult and pediatric moyamoya.
Data availability
Not applicable.
References
Acker G, Fekonja L, Vajkoczy P (2018) Surgical management of moyamoya disease. Stroke 49(2):476–482. https://doi.org/10.5853/jos.2015.01627
Amin-hanjani S, Singh A, Rifai H, Thulborn KR et al (2013) Combined direct and indirect bypass for moyamoya. Neurosurgery 73(6):962–968. https://doi.org/10.1227/neu.0000000000000139
Chen Z, Zhang L, Qu J, Wu Y et al (2018) Clinical analysis of combined revascularization in treating ischemic moyamoya disease in adults. Neurochirurgie 64(1):49–52. https://doi.org/10.1016/j.neuchi.2017.08.005
Cho WS, Chung YS, Kim JE et al (2015) The natural clinical course of hemodynamically stable adult moyamoya disease. J Neurosurg 122(1):82–89. https://doi.org/10.3171/2014.9.jns132281
Cho WS, Kim JE, Kim CH, Ban SP, Kang HS, Son YJ et al (2014) Long-term outcomes after combined revascularization surgery in adult moyamoya disease. Stroke 45(10):3025–3031. https://doi.org/10.1161/strokeaha.114.005624
Choi JU, Kim DS, Kim EY, Lee KC (1997) Natural history of moyamoya disease: Comparison of activity of daily living in surgery and non surgery groups. Clin Neurol Neurosurg 99(2):11–18. https://doi.org/10.1016/s0303-8467(97)00033-4
Czabanka M, Peña-Tapia P, Scharf J, Schubert GA, Münch E, Horn P et al (2011) Characterization of direct and indirect cerebral revascularization for the treatment of European patients with moyamoya disease. Cerebrovasc Dis 32(4):361–369. https://doi.org/10.1159/000330351
Demartini Z Jr, Teixeira BC, Koppe GL, Gatto LAM, Roman A, Munhoz RP (2022) Moyamoya disease and syndrome: A review. Radiol Bras 55(1):31–37. https://doi.org/10.1590/0100-3984.2021.0010
Deng X, Gao F, Zhang D, Zhang Y, Wang R, Wang S, Cao Y, Zhao Y, Pan Y, Ye X, Liu X, Zhang Q, Wang J, Yang Z, Zhao M, Zhao J (2018) Effects of different surgical modalities on the clinical outcome of patients with moyamoya disease: A prospective cohort study. J Neurosurg 128(5):1327–1337. https://doi.org/10.3171/2016.12.jns162626
Fujimura M, Tominaga T (2012) Lessons learned from moyamoya disease: Outcome of direct/indirect revascularization surgery for 150 affected hemispheres. Neurol Med Chir (Tokyo) 52(5):327–332. https://doi.org/10.2176/nmc.52.327
Fujita K, Tamaki N, Matsumoto S (1986) Surgical treatment of moyamoya disease in children: Which is more effective procedure, EDAS or EMS? Childs Nerv Syst 2(3):134–138. https://doi.org/10.1007/bf00270841
Fung LW, Thompson D, Ganesan V (2005) Revascularisation surgery for paediatric moyamoya: A review of the literature. Childs Nerv Syst 21(5):358–364. https://doi.org/10.1007/s00381-004-1118-9
Gross BA, Du R (2013) The natural history of moyamoya in a North American adult cohort. J Clin Neurosci 20(1):44–48. https://doi.org/10.1016/j.jocn.2012.08.002
Hertza J, Loughan A, Perna R, Davis AS, Segraves K, Tiberi NL (2014) Moyamoya disease: A review of the literature. Appl Neuropsychol Adult 21(1):21–27. https://doi.org/10.1080/09084282.2012.721147
Houkin K, Kamiyama H, Takahashi A, Kuroda S et al (1997) Combined revascularization surgery for childhood moyamoya disease: STA-MCA and encephalo-duro-arterio-myo-synangiosis. Childs Nerv Syst 13(1):24–29. https://doi.org/10.1007/s003810050034
Isono M, Ishii K, Kamida T, Inoue R, Fujiki M, Kobayashi H (2002) Long-term outcomes of pediatric moyamoya disease treated by encephalo-duro-arterio-synangiosis. Pediatr Neurosurg 36(1):14–21. https://doi.org/10.1159/000048343
Jiang H, Ni W, Xu B, Lei Y, Tian Y, Xu F, Gu Y, Mao Y (2014) Outcome in adult patients with hemorrhagic moyamoya disease after combined extracranial-intracranial bypass. J Neurosurg 121(5):1048–1055. https://doi.org/10.3171/2014.7.jns132434
Karasawa J, Kikuchi H, Furuse S, Kawamura J, Sakaki T (1978) Treatment of moyamoya disease with STA-MCA anastomosis. J Neurosurg 49(5):679–688. https://doi.org/10.3171/jns.1978.49.5.0679
Karasawa J, Touho H, Ohnishi H, Miyamoto S, Kikuchi H (1992) Long-term follow-up study after extracranial-intracranial bypass surgery for anterior circulation ischemia in childhood moyamoya disease. J Neurosurg 77(1):84–89. https://doi.org/10.3171/jns.1992.77.1.0084
Kim JS (2016) Moyamoya disease: Epidemiology, clinical features, and diagnosis. J Stroke 18(1):2–11. https://doi.org/10.5853/jos.2015.01627
Kim KM, Kim JE, Cho WS, Kang HS, Son YJ, Han MH, Oh CW (2017) Natural history and risk factor of recurrent hemorrhage in hemorrhagic adult moyamoya disease. Neurosurgery 81(2):289–296. https://doi.org/10.1093/neuros/nyw179
Kim SH, Lee H, Yoo M, Jin S et al (2019) Angiographic and clinical outcomes of non-patent anastomosis after bypass surgery in adult moyamoya disease. Acta Neurochir (Wien) 161(2):379–384. https://doi.org/10.1007/s00701-018-3733-3
Kuroda S, Nakayama N, Yamamoto S, Kashiwazaki D et al (2020) Late (5–20 years) outcomes after STA-MCA anastomosis and encephalo-duro-myo-arterio-pericranial synangiosis in patients with moyamoya disease. J Neurosurg 134(3):909–916. https://doi.org/10.3171/2019.12.jns192938
Nguyen VN, Motiwala M, Elarjani T et al (2022) Direct, indirect, and combined extracranial-to-intracranial bypass for adult moyamoya disease: An updated systematic review and meta-analysis. Stroke 53(12):3572–3582. https://doi.org/10.1161/STROKEAHA.122.039584
Patel NN, Mangano FT, Klimo P Jr (2010) Indirect revascularization techniques for treating moyamoya disease. Neurosurg Clin N Am 21(3):553–563. https://doi.org/10.1016/j.nec.2010.03.008
Rashad S, Fujimura M, Niizuma K, Endo H et al (2016) Long-term follow-up of pediatric moyamoya disease treated by combined direct–indirect revascularization surgery: Single institute experience with surgical and perioperative management. Neurosurg Rev 39(4):615–623. https://doi.org/10.1007/s10143-016-0734-7
Ravina K, Kim PE, Rennert RC, Wolfswinkel EM et al (2019) Lessons learned from the initial experience with pedicled temporoparietal fascial flap for combined revascularization in moyamoya angiopathy: A case series. World Neurosurg 132:259–273. https://doi.org/10.1016/j.wneu.2019.08.182
Ravindran K, Wellons JC, Dewan MC (2019) Surgical outcomes for pediatric moyamoya: A systematic review and meta-analysis. J Neurosurg Pediatr 13:1–10. https://doi.org/10.3171/2019.6.peds19241
Sakamoto T, Kawaguchi M, Kurehara K, Kitaguchi K, Furuya H, Karasawa J (1997) Risk factors for neurologic deterioration after revascularization surgery in patients with moyamoya disease. Anesth Analg 85(5):1060–1065. https://doi.org/10.1097/00000539-199711000-00018
Smith ER, Scott RM (2010) Moyamoya: Epidemiology, presentation, and diagnosis. Neurosurg Clin N Am 21(3):543–551. https://doi.org/10.1016/j.nec.2010.03.007
Starke RM, Komotar RJ, Hickman ZL, Paz YE, Pugliese AG, Otten ML, Garrett MC, Elkind MSV, Marshall RS, Festa JR, Meyers PM, Connolly ES Jr (2009) Clinical features, surgical treatment, and long-term outcome in adult patients with moyamoya disease. Clin Article J Neurosurg 111(5):936–942. https://doi.org/10.3171/2009.3.jns08837
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M et al (2016) ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:4919. https://doi.org/10.1136/bmj.i4919
Uchino K, Johnston SC, Becker KJ, Tirschwell DL (2005) Moyamoya disease in Washington State and California. Neurology 65(6):956–958. https://doi.org/10.1212/01.wnl.0000176066.33797.82
Xu B, Song DL, Mao Y, Gu YX, Xu H, Liao YJ, Liu CH, Zhou LF (2012) Superficial temporal artery-middle cerebral artery bypass combined with encephalo-duro-myo-synangiosis in treating moyamoya disease: Surgical techniques, indications and midterm follow-up results. Chin Med J (Engl) 125(24):4398–4405
Zhao J, Liu H, Zou Y, Zhang W et al (2018) Clinical and angiographic outcomes after combined direct and indirect bypass in adult patients with moyamoya disease: A retrospective study of 76 procedures. Exp Ther Med 15(4):3570–3576. https://doi.org/10.3892/etm.2018.5850
Zhao Y, Yu S, Lu J, Yu L, Li J, Zhang Y, Zhang D, Wang R, Zhao Y (2018) Direct bypass surgery vs. combined bypass surgery for hemorrhagic moyamoya disease: A comparison of angiographic outcomes. Front Neurol 9:1121. https://doi.org/10.3389/2Ffneur.2018.01121
Acknowledgements
No financial funding or support was received for this project. No additional financial disclosures.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Albert M. Isaacs, Anthony E. Bishay, Dillan Amaral, Jhon E. Bocanegra-Becerra, Livia V. Abreu, Michael Dewan, Sávio Batista and Stefan Koester. The first draft of the manuscript was written by Anthony E. Bishay, Dan Zimelewicz Oberman, Raphael Bertani, Sávio Batista and Stefan Koester, and all authors commented on previous versions of the manuscript. Supervision was coordinated by Eberval Gadelha Figueiredo. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Prior presentation
No portion of this data has been presented before.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Batista, S., Koester, S., Bishay, A.E. et al. Complications associated with combined direct and indirect bypass in Moyamoya Disease: A meta-analysis. Neurosurg Rev 47, 58 (2024). https://doi.org/10.1007/s10143-024-02285-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10143-024-02285-4