
Abstract
Lumbar spinal stenosis (LSS) is one of the most common indications for surgery in the USA. The addition of instrumented fusion to decompression for the treatment of LSS has become common, but recent randomized controlled trials (RCTs) have produced percieved conflicting results with unclear clinical implications. This review seeks clarity through an analysis of available RCTs. We performed a search of the PubMed database for RCTs that directly addressed decompression vs. decompression and fusion for the surgical treatment of LSS. RCTs were screened and reviewed to compare content such as patient selection, pathology, radiographic criteria, and operative technique. Five RCTs resulted from our search and were included in our analysis. Two studies yielded class I data while three yielded class III data due to study design related issues. Heterogeneity between these studies is emphasized with regard to patient selection, LSS definition, spondylolisthesis, instability, and surgical technique. Efforts to decipher which patients will truly benefit from instrumented fusion for the surgical treatment of LSS are still ongoing. Surgeon judgment will remain a crucial component for surgical decision making until future trials provide clarity. Instrumented fusion should be tailored to the individual patient rather than incorporated as a routine practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Symptomatic relief by decompressing mass effect is a central premise in spinal neurosurgery, which is thought to relieve vascular compromise and improve neurologic function [8, 19, 22]. This concept forms the basis for decompressive laminectomy in patients suffering from symptomatic lumbar spinal stenosis (LSS), the most common indication for surgery in the USA [1, 20].
While the concept of decompression is intuitively appealing, providing data to support this concept has been challenging. Two randomized controlled trials (RCTs) have compared the effectiveness of non-operative management to that of surgical decompression. Malmivaara et al. randomized 94 patients with symptomatic LSS to decompressive laminectomy or non-operative management and showed that the surgery improved leg and back pain, though the difference between arms dwindled with time [17, 27]. A second study by Weinstein et al. randomized 289 patients to surgery or non-operative management. Interpretation of this study is limited by the significant proportion of patient who crossed over from the non-surgical to the surgical arm. The as-treated analysis suggests that surgical decompression affords faster and greater pain relief [28]. While these results are imperfect, they are generally consistent with the experience of spine practitioners. As such, it is generally accepted that decompressive laminectomy should be considered in patients suffering from symptomatic LSS who have failed non-operative management.
As more decompressive laminectomies have been performed, the complexity of the procedure has also increased [13]. More and more, lumbar decompression is accompanied by instrumented fusion, with the rational of stabilizing micro-instability unappreciated radiographically [14], or laminectomy-induced instability [29]. The practice of augmenting decompression with instrumented fusion remains a controversial subject [21], especially given differential risk profiles and reimbursement for these procedures [4, 7, 11, 23]. This controversy culminated with two high quality RCTs that were co-published in New England Journal of Medicine (NEJM) in April 2016 [7, 9].
Here, we performed a comprehensive search of the literature to identify pertinent RCTs that would inform this controversial matter. We reviewed pertinent information from these studies with the goal of laying a foundation for resolving the controversy.
Materials and methods
We performed a search of the PubMed database for literature published from 1966 to July 2018.
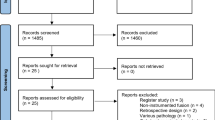
Our initial search used the heading “lumbar laminectomy stenosis fusion” and yielded 479 articles including 21 filtered RCTs. The titles and abstracts of each of these 479 references were reviewed and those not providing prospective randomized data that included either direct comparison or insight into decompression vs. decompression and fusion specifically for the surgical treatment of LSS were not included. The excluded trials compared various specialized fusion techniques, non-instrumented surgical variations, or involved non-operative treatment. The resulted studies included the 2016 NEJM co-published spinal laminectomy versus instrumented pedicle screw (SLIP) trial [10] and the Swedish Spinal Stenosis Study (SSSS) [6] along with two additional studies (Grob et al. and Fischgrund et al.) [5, 12].
We knew of an additional study (Bridwell et. al) [2] that had been referenced in SSSS as evidence for the perceived modern mandatory view toward fusion in the setting of spondylolisthesis. This trial had not resulted with the above search criteria. When the search was modified to “spinal stenosis fusion,” it yielded 2464 articles of which 166 were prospective clinical trials. The title and abstracts of each of these clinical trials were reviewed as described above. The Bridwell et al. study resulted, but no additional trial met our criteria beyond the initial results.
Further Pubmed searches for “lumbar laminectomy instrumentation,” “laminectomy instrumentation,” “laminectomy instrumentation stenosis,” “instrumentation lumbar stenosis,” “lumbar fusion outcome instrumentation,” and “Fusion lumbar stenosis” did not provide additional studies meeting our criteria.
Each trial was reviewed with regards to patient selection, randomization, inclusion/exclusion criteria, radiographic criteria, results, and outcome measures.
Results
We identified 5 studies in our search. Two studies yielded class I data while three yielded class III data due to study design related issues. Differences in patient selection, radiographic criteria, and findings are provided in Table 1.
The two studies that provided class I data were reported by Ghogawala et al. and Försth et al. in the SLIP and SSSS trials, respectively.
Ghogawala et al. in the SLIP trial included patients with symptomatic LSS secondary to single level grade I lumbar spondylolisthesis, defined radiographically as 3–14 mm of slippage. Patients were excluded for evidence of gross instability (defined as > 3 mm movement on flexion/extension films). Disc herniation and prior surgery were also excluded. Fifty-seven patients were randomized to decompressive laminectomy and partial medial facetectomy or laminectomy augmented with instrumented fusion. The primary outcome measure was the change in the SF-36 physical-component summary score at 2 years after surgery. The study was powered to detect 7.5 points difference in this scale. In the final analysis, the fusion group showed a greater improvement in the SF-36 physical-component summary score than did those in the laminectomy-alone group (15.2 vs. 9.5, P = 0.046). Oswestry disability index (ODI) score improvement was considered as a secondary outcome. While ODI improvement differed between arms (26 points in the fusion group and 18 points in the decompression group), this difference did not reach statistical significance (P = 0.06).
Försth et al. in SSSS included patients with 1–2 levels of symptomatic LSS with or without spondylolisthesis. Lumbar stenosis was defined as a cross sectional area < 75 mm2 of the thecal sac on magnetic resonance imaging. Spondylolisthesis was defined as > 3 mm of slippage. Patients with a Cobb angle > 20, spondylolysis, prior surgery, or herniated disc were excluded. The primary outcome was ODI at 2 years after surgery. The study was powered to detect 12 points difference in this scale. The study found no significant differences in ODI improvement between the instrumented-fusion group and decompression-alone group. The improvement was 16 points in the fusion group and 20 points in the decompression only group.
There were three older RCTs that are pertinent but suffer from methodological/design deficiencies and limited sample size.
The study by Bridwell et al. did not specify specific radiographic criteria for inclusion or exclusion. Forty-four patients with symptomatic LSS without evidence of instability (defined as > 3 mm movement on flexion/extension films) were randomized to 3 groups: group 1 decompression only (with facet preservation), group 2 decompression and posterolateral fusion without instrumentation, and group 3 decompression and instrumented fusion. Three independent observers evaluated post-operative radiographs for radiographic parameters and grading of the fusion mass using the Lenke classification system [16]. Patients were asked to grade their functional status post-operatively on a 3-point scale (worse, same, and better). No power calculation was performed. The primary outcome measure was not clearly defined. The authors reported that group 3 (laminectomy augmented with instrumented fusion) experienced statistically significant decreases in spondylolisthesis progression, as well as a higher proportion of solid fusion mass and improved ambulation.
Grob et al. included patients with symptomatic LSS defined as midsagittal diameter of < 11 mm on X-ray. Patients with evidence of instability, defined by > 5 mm of spondylolisthesis or lateral offset > 5 mm, were excluded. Forty-five patients were randomized into 3 groups: group 1 decompression only, group 2 with non-instrumented fusion at the most stenotic segment, and group 3 with non-instrumented fusion at all involved segments. The primary outcome measure was not clearly specified. No power calculation was performed. The author reports no statistically significant difference between the 3 groups.
Fischgrund et al. studied patients with symptomatic LSS with a single level of spondylolisthesis identified on X-ray. Sixty-eight patients were randomized to instrumented or non-instrumented fusion. The primary outcome measure was not clearly specified. No power calculation was performed. Successful arthrodesis occurred in 83% of the instrumented spines versus 45% of the non-instrumented ones (P < 0.05). Back and lower limb pain improved in both groups post-operatively, but no differences were noted between the two groups.
Discussion
Synthesizing the available RCT literature on the efficacy of instrumented fusion in addition to decompressive surgery for the surgical treatment of LSS is challenging given the significant heterogeneity in study design, definitions of surgical techniques, outcome measures, and patient populations. For instance, decompressions in SLIP and Grob et al. consisted of complete laminectomy with partial medial facetectomy while Bridwell et al. performed laminectomies without facetectomy. In SSSS, decompression was performed with or without facetectomy based on the discretion of the surgeon. This type of variation undoubtedly contributed to the reported results.
Despite the various limitations inherent in the LSS RCT studies, it is possible to construct a conceptual framework based on insights derived from these studies. The Bridwell study and the SLIP study suggest that a subset of LSS patients benefit from upfront decompression/fusion. Such benefit was not observed in the patients enrolled in the Grob et al., Fischgrund et al., and the SSSS study. A reasonable synthesis of these results is that many LSS patients do not derive significant benefit from fusion at the time of decompression. As such, routine incorporation of fusion in all lumbar decompression patients would be unjustified, and instrumented fusion should be tailored to the individual patient rather than incorporated as a routine practice.
The question, thus, becomes one of identifying LSS patients who would mostly likely benefit from an upfront decompression/fusion. Since SLIP study reported significant improvement in outcome in the fusion/decompression arm, it is reasonable to hypothesize that patients suffering from single level LSS with grade I spondylolisthesis (the inclusion criteria for SLIP) may be more likely to benefit from upfront decompression/fusion. It is important to note that even in this population, only select patients benefitted from upfront decompression/fusion relative to stand-alone decompression. The importance of patient selection for decompression/fusion in this context cannot be over-emphasized. While the complications rate did not differ significantly between the fusion and non-fusion arms in the various RCTs, the studies were not designed to detect a difference in complications. Larger series do report severe complications in patients who underwent spinal fusions, especially in the elderly [4]. Furthermore, the RCTs reviewed here enroll patients up to 4 years, but clinical relapse and the need for re-operation may manifest well beyond the study period, where processes such as adjacent segment disease may be greater than 35% at 10-year follow-up [9].
While the measure of re-operation was not a primary or secondary outcome in SLIP, a great deal of attention has been devoted to this topic. In SLIP, 34% of the decompression only patients required re-operation while 14% of the decompression and fusion patients required such re-operation. The proportion of patients requiring surgery in the decompression only arm in SLIP is more than double than those reported in SSSS (where the re-operation rate did not differ in the two arms) and those previously reported [28]. The inability to blind the surgeon to the intervention prohibits exclusion of unconscious bias that may affect how a surgical procedure is performed. The impossibility of such blinding highlights a fundamental challenge inherent in surgical RCTs. The argument is that the durability of an initial fusion may provide longer benefit, prevent re-operation, and as such may be more cost-effective long term [11]. Further study is needed to substantiate this hypothesis.
There are several key issues identified in our review that should guide future research in surgical intervention for LSS. First, there is general consensus that spinal fusion is needed in patients who suffer symptoms related to spinal instability [25]. However, there is little agreement on clinical and radiographic criteria for assessing instability. While flexion/extension X-rays are often done for this assessment, the diagnostic accuracy of these studies remain variable [3, 26]. Similarly, while face angle/edema may predict instability [15, 24], there is further variability in terms of how such information is used to guide surgical decision making. Equally important to consider is that the available RCTs have yet to factor into how spinal alignment (e.g., sagittal balance, loss of lordosis… etc.) may impact outcome or spinal stability. Additionally, the current imaging tools for spine neurosurgery are focused on delineation of anatomy while pain is fundamentally a physiologic response. It is not inconceivable that the same anatomy can yield differing physiologic responses. Finally, surgical techniques for decompression and fusion continue to evolve at rapid pace. For instance, many surgeons are now performing decompression by undercutting the lamina rather than total removal of the lamina [18]. It is essential that the research keeps pace with this rapid evolution in order to maintain clinical applicability.
Until future studies address the issues summarized above, surgical judgment will remain the main driving force in determining whether instrumented fusion should be performed to augment decompressive laminectomy in the setting of symptomatic LSS. From a surgeon’s perspective, the decision of whether to offer fusion ultimately rests on whether pre-existing instability contributed to the patient’s symptoms and whether instability is likely to result after the decompression. This is a complex decision requiring incorporation of multiple facets of clinical presentation (did the patient present with neurogenic claudication, back pain, radiculopathy, or other symptoms), radiographic assessment (spinal alignment, flexion/extension imaging, facet anatomy… etc.), additional testing (spinal epidural injection, discogram… etc.), and the intended procedure (lamina sparing decompression, extent of facet removed… etc.). Additionally, review in a multi-disciplinary board involving multiple spine surgeons may allow integration of distinct perspectives in optimizing surgical decisions. Finally, it is essential for the surgeon to understand the patient’s expectation and preferences. For instance, would a patient prefer an upfront fusion relative in favor of a 20% reduction in the risk for needing a surgery in the future? In the end, the foundation of individualizing the decision of whether to fuse will lay on a careful discussion with patients about the surgical options and the limitations of our current data in the context of the surgeon’s skill sets.
References
Amundsen T, Weber H, Lilleås F, Nordal HJ, Abdelnoor M, Magnaes B (1995) Lumbar spinal stenosis. Clinical and radiologic features. Spine (Phila Pa 1976) 20:1178–1186
Bridwell K, Sedgewick T, O'Brien M, Lenke L, Baldus C (1993) The role of fusion and instrumentation in the treatment of degenerative spondylolisthesis with spinal stenosis. J Spinal Disord 6:461–472
Cabraja M, Mohamed E, Koeppen D, Kroppenstedt S (2012) The analysis of segmental mobility with different lumbar radiographs in symptomatic patients with a spondylolisthesis. Eur Spine J 21:256–261
Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG (2010) Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 303:1259
Fischgrund JS, Mackay M, Herkowitz HN, Brower R, Montgomery DM, Kurz LT (1997) 1997 Volvo award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine (Phila pa 1976) 22:2807–2812
Försth P, Ólafsson G, Carlsson T, Frost A, Borgström F, Fritzell P, Öhagen P, Michaëlsson K, Sandén B (2016) A randomized, controlled trial of fusion surgery for lumbar spinal stenosis. N Engl J Med 374:1413–1423
Fritzell P, Hägg O, Wessberg P, Nordwall A, Swedish Lumbar Spine Study Group (2002) Chronic low back pain and fusion: a comparison of three surgical techniques: a prospective multicenter randomized study from the Swedish lumbar spine study group. Spine (Phila Pa 1976) 27:1131–1141
Genevay S, Atlas SJ (2010) Lumbar spinal stenosis. Best Pract Res Clin Rheumatol 24:253–265
Ghiselli G, Wang JC, Bhatia NN, Hsu WK, Dawson EG (2004) Adjacent segment degeneration in the lumbar spine. J Bone Jt Surg-Ser A 86:1497–1503
Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge SN, Coumans J-VCE, Harrington JF, Amin-Hanjani S, Schwartz JS, Sonntag VKH, Barker FG, Benzel EC (2016) Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. N Engl J Med 374:1424–1434
Glassman SD, Polly DW, Dimar JR, Carreon LY (2012) The cost effectiveness of single-level instrumented posterolateral lumbar fusion at 5 years after surgery. Spine (Phila Pa 1976) 37:769–774
Grob D, Humke T, Dvorak J (1993) Significance of simultaneous fusion and surgical decompression in lumbar spinal stenosis. Orthopade 22:243–249
Kepler CK, Vaccaro AR, Hilibrand AS, Anderson DG, Rihn JA, Albert TJ, Radcliff KE (2014) National trends in the use of fusion techniques to treat degenerative spondylolisthesis. Spine (Phila Pa 1976) 39:1584–1589
Landi A, Gregori F, Marotta N, Donnarumma P, Delfini R (2015) Hidden spondylolisthesis: unrecognized cause of low back pain? Prospective study about the use of dynamic projections in standing and recumbent position for the individuation of lumbar instability. Neuroradiology 57:583–588
Lattig F, Fekete TF, Grob D, Kleinstück FS, Jeszenszky D, Mannion AF (2012) Lumbar facet joint effusion in MRI: a sign of instability in degenerative spondylolisthesis? Eur Spine J 21:276–281
Lenke LG, Bridwell KH, Bullis D, Betz RR, Baldus C, Schoenecker PL (1992) Results of in situ fusion for isthmic spondylolisthesis. J Spinal Disord 5:433–442
Malmivaara A, Slätis P, Heliövaara M, Sainio P, Kinnunen H, Kankare J, Dalin-Hirvonen N, Seitsalo S, Herno A, Kortekangas P, Niinimäki T, Rönty H, Tallroth K, Turunen V, Knekt P, Härkänen T, Hurri H, Finnish Lumbar Spinal Research Group (2007) Surgical or nonoperative treatment for lumbar spinal stenosis? Spine (Phila Pa 1976) 32:1–8
Mobbs R, Phan K (2017) Minimally invasive unilateral laminectomy for bilateral decompression. JBJS Essent Surg Tech 7:e9
Olmarker K, Rydevik B, Hansson T, Holm S (1990) Compression-induced changes of the nutritional supply to the porcine cauda equina. J Spinal Disord 3:25–29
Otani K, Kikuchi S, Yabuki S, Igarashi T, Nikaido T, Watanabe K, Konno S (2013) Lumbar spinal stenosis has a negative impact on quality of life compared with other comorbidities: an epidemiological cross-sectional study of 1862 community-dwelling individuals. ScientificWorldJournal 2013:590652
Pearson AM (2016) Fusion in degenerative spondylolisthesis: how to reconcile conflicting evidence. J Spine Surg 2:143–145
Porter RW, Ward D (1992) Cauda equina dysfunction. The significance of two-level pathology. Spine (Phila Pa 1976) 17:9–15
Rihn JA, Patel R, Makda J, Hong J, Anderson DG, Vaccaro AR, Hilibrand AS, Albert TJ (2009) Complications associated with single-level transforaminal lumbar interbody fusion. Spine J 9:623–629
Schinnerer KA, Katz LD, Grauer JN (2008) MR findings of exaggerated fluid in facet joints predicts instability. J Spinal Disord Tech 21:468–472
Schroeder GD, Kepler CK, Kurd MF, Vaccaro AR, Hsu WK, Patel AA, Savage JW (2015) Rationale for the surgical treatment of lumbar degenerative spondylolisthesis. Spine (Phila Pa 1976) 40:E1161–E1166
Shaffer WO, Spratt KF, Weinstein J, Lehmann TR, Goel V (1990) 1990 Volvo Award in clinical sciences. The consistency and accuracy of roentgenograms for measuring sagittal translation in the lumbar vertebral motion segment An experimental model. Spine (Phila Pa 1976) 15:741–750
Slätis P, Malmivaara A, Heliövaara M, Sainio P, Herno A, Kankare J, Seitsalo S, Tallroth K, Turunen V, Knekt P, Hurri H (2011) Long-term results of surgery for lumbar spinal stenosis: a randomised controlled trial. Eur Spine J 20:1174–1181
Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood E, Hanscom B, Herkowitz H, Cammisa F, Albert T, Boden SD, Hilibrand A, Goldberg H, Berven S, An H, Investigators S (2008) V Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 358:794–810
Yadhati A, Kurra S, Tallarico RA, Lavelle WF (2017) Lumbar vertebral body and pars fractures following laminectomy. J Surg Case Rep 2017:rjx007
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Not required/applicable
Informed consent
Not required/applicable
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Leschke, J.M., Chen, C.C. Supplementing decompression with instrumented fusion for symptomatic lumbar spinal stenosis—a critical appraisal of available randomized controlled trials. Neurosurg Rev 44, 643–648 (2021). https://doi.org/10.1007/s10143-020-01270-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-020-01270-x