
Abstract
Exposure to high altitude above 3000 m leads to two outcomes—acclimation or high-altitude maladies. To reach a particular outcome, the plasma proteome is modified differentially, either in context of an acclimation response or mal-acclimation response leading to disease. This ensures that hypoxia-responsive plasma protein trends reflect acclimation in acclimated individuals when compared with their levels prior to acclimation. Such protein trends could be used to assess acclimation in an individual and any significant deviation from this trend may indicate non-acclimation, thereby preventing high-altitude illnesses before they manifest. In this study, we investigate and statistically evaluate the trendlines of various hypoxia-responsive plasma protein levels, reported significantly perturbed in our previous studies, in individuals (male; n = 20) exposed to 3520 m at high-altitude day 1 (HAD1), HAD4, and HAD7L and to 4420 m at HAD7H, HAD30, and HAD120. We observe that thioredoxin (Trx), glutathione peroxidase 3 (GPx-3), and apolipoprotein AI (Apo-AI) are statistically robust markers to assess acclimation across the exposure duration while sulfotransferase 1A1 (ST1A1) is a capable negative control whose levels increase only in cases of HAPE. We also observe exposure day-specific and resident altitude-specific proteins capable of accurately assessing acclimation when compared with baseline levels or the lower altitude zone.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
High-altitude acclimation, although essential for safe ascent till below the death zone (> 7500 m), has received insufficient scientific scrutiny to comprehend the trends of various proteins of diagnostic value in the proteome during chronic exposure to high-altitude conditions. High-altitude acclimation fundamentally depends on two factors: duration and altitude of exposure. Although it has received scarce scientific scrutiny, it’s the most crucial aspect to high-altitude exploration. Acclimation status assessment at altitude has never been given thorough objective analysis. In the general populace, acclimation assessment is based on an individual deciding whether one should ascend higher within a stipulated time (Karinen et al. 2008). In the Armed forces, acclimation assessment is based on finishing physical tasks at the end of a fixed exposure duration before ascending further (Deshwal et al. 2012; Syed et al. 2010). The current acclimation process (for Indian Army) requires at least 10 days of continuous high-altitude exposure with incremental ascents every 5th day incorporating both factors, duration and altitude. The acclimatization process at its core aims to make individuals tolerant to the ambient hypobaric hypoxia. However, all preliminary diagnostic foci for assessment of acclimatization are limited to subjective physical symptoms. Poor acclimation causes high-altitude maladies like acute mountain sickness (AMS) and high-altitude pulmonary edema (HAPE) (Ren et al. 2010). Even though these diseases themselves have received wide scientific interest, the process of objectively assessing acclimation has not evolved much. During ascent, if a person is suspected to have AMS, he/she is asked to fill a Lake Louise questionnaire, marking themselves for symptoms like nausea, fatigue, and headache. Even in case of more severe HAPE, initial diagnosis is limited to benign parameters like difficulty in breathing, excess frothy sputum, and tiredness. Thus, there is definitive treatment only when the disorder shows peak physiological manifestation. There is no preventive care possible as there are no known markers to distinguish an acclimatized individual from one who has not been able to acclimatize (mal-acclimatized) during the same exposure tenure. In context of high-altitude expeditions, a mal-acclimatized individual is at risk of developing multiple high-altitude illnesses which can be prevented by timely descent to a lower altitude. However, since there are no objective methods of assessing acclimation status, in most cases, it is too late for timely descent. A tool for assessing acclimation can prevent such life-threatening scenarios.
Previously, using SD rats, we provided a proof-of-concept shortened acclimation protocol and the lung and plasma proteins that are involved in the process (Paul et al. 2018). Here we show specific plasma protein trendlines indicative of acclimation during high-altitude exposures ranging from day 1 at 3520 m to day 120 at 4420 m. Plasma levels of thioredoxin (Trx), glutathione peroxidase 3 (GPx-3), and apolipoprotein A1 (Apo-AI) along with HAPE indicator (Ahmad et al. 2015) sulfotransferase 1A1 (ST1A1) very accurately reflect acclimation over the aforementioned altitude range and duration. Exposure day-specific and exposure altitude-specific proteins have also been presented. A proof-of-concept diagnostic tool with a statistically relevant biomarker protein panel is presented. This shall help assess acclimation status from the first day of exposure at high altitudes and possibly prevent high-altitude illnesses to a large extent in the future.
Materials and methods
Ethics statement
All study protocols were cross-checked and approved by the institutional ethics committee (IEC/DIPAS/B2/1) in accordance with the Helsinki declaration. Informed written consent was obtained prior to the study from all participants.
Collection of blood samples and extraction of plasma
Two separate regimental groups consisting of male Indian Army troops (Group 1 had mean age 24 years, mean weight 62 ± 3 kg; while Group 2 had mean age 30 years, mean weight 67 ± 0.67 kg) were defined for blood sampling. Exclusion criteria for both the groups were smoking, lung disease/defects, cardiac disease/defects, hypertension, obesity, previous exposure to altitudes 1500 m above sea-level, and presence of any infectious/non-infectious disease during the study. In each group, first, samples were taken in normoxic conditions (Baseline) with further sampling done at various intervals of high-altitude exposure from the 1st day of exposure till the 120th day. Samples from Group 1 (n = 20) were taken at Baseline1 (BL1; 216 m above sea level), then at High-Altitude exposure day 1(HAD1), HAD4, and HAD7L (3520 m above sea level). Due to operational requirements, Group 1 descended after HAD7. Samples from Group 2 (n = 20) were taken at Baseline2 (BL2; 332 m above sea level), HAD7H, HAD30, and HAD120 (4420 m above sea level). Samples from Group 2 could not be collected for HAD1 and HAD4 due to extraordinary circumstances faced by Group 2 during that time. The altitude of sample collection during high-altitude stay for the two groups signify a high-altitude zone (Group 1; 3520 m) and very high-altitude zone (Group 2; 4420 m). All individuals were in supine position during blood collection. The sample collected was then centrifuged at 3500 rpm for 15 min to separate plasma layer. The plasma was collected in fresh tubes and protease inhibitor cocktail (P8340, Sigma, USA) was added to each sample. Finally, plasma tubes were stored at − 80 °C till further use.
ELISA tests
ELISA was performed as per the manufacturers’ instructions for detection of the following proteins in the collected plasma samples: thioredoxin (Trx; kit details: E-EL-H1727, Elabscience, USA), thioredoxin reductase (TR; kit details: ab192150, Abcam, USA), phenol sulfotransferase (ST1A1; kit details: SEB268Hu, Cloud-Clone Corp., USA), calmodulin (CAM; kit details: E-EL-H0625, Elabscience, USA), glutathione peroxidase 3 (GPx-3; kit details: SEC992Hu, Cloud-Clone Corp., USA), hemopexin (Hpx; kit details: ab108859, Abcam, USA), apolipoprotein A1 (Apo-AI; kit details: ab108804, Abcam, USA), and haptoglobin (Hp; kit details: ab108856, Abcam, USA).
Statistical analyses
Graphpad Prism (version 7) was used to tabulate data and perform statistical analyses of the data. One-way ANOVA followed by Tukey’s multiple-comparison test comparing the stated proteins’ ability to assess acclimatization status across 1, 4, 7, 30, and 120 days at 3520 m and 4420 m. ROC analysis was performed with significance at p < 0.001 using AUC values, sensitivity, and specificity for same proteins to decide whether acclimated or non-acclimated. An AUC ≥ 0.8 only was considered for further analysis.
Results
Groups undergoing acclimation
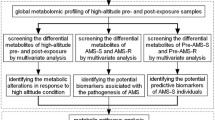
The Indian Army conducts a staged ascent protocol (Deshwal et al. 2012) to help its troops acclimate to high altitude. Group 1 and Group 2 (n = 20 each), two separate regimental groups consisting of male Indian Army troops, were exposed to 3520 m and 4420 m, respectively (Fig. 1). Group 1 plasma samples were collected at baseline (BL1; 216 m), high-altitude day 1 (HAD1), HAD4, and HAD7L. Group 2 plasma samples were collected at BL2 (332 m), HAD7H, HAD30 and HAD120. All members in both groups fully acclimated as per the Indian Army’s standard protocol and no cases of high-altitude illnesses were observed.

Study design. Two groups (n = 20 each) of male Indian Army troops were exposed to 3520 m for 7 days (Group 1) and 4420 m for 120 days (Group 2). In Group 1 at 3520 m, blood samples were collected from all volunteers on days 1, 4, and 7. In Group 2 at 4420 m, blood samples were collected at days 7, 30, and 120. All subjects acclimated as per Indian Army’s standard acclimation protocol. No cases of altitude illness were observed. Specific blood plasma proteins were assayed using ELISA. Their median with range was plotted and after performing statistical analysis utilizing ROC curve for each protein, significant proteins were listed for each group and exposure days. These proteins could further be used to make a diagnostic tool capable of diagnosing acclimation status in humans exposed to high-altitude. Trx: Thioredoxin; GPx3: glutathione peroxidase; ApoA1: apolipoprotein A1; CAM: calmodulin; ST1A1: sulfotransferase 1A1; Hpx; hemopexin; Hp: haptoglobin and TR: thioredoxin reductase
Plasma proteins assayed
Our previous investigations had provided us a list of plasma proteins that was consistently and significantly perturbed during high-altitude or hypobaric hypoxia exposures (Paul et al. 2018; Ahmad et al. 2011, 2013, 2014, 2015, 2016; Padhy et al. 2013; Tyagi et al. 2014). We assayed the plasma protein levels of thioredoxin (Trx), thioredoxin reductase (TR), sulfotransferase 1A1 (ST1A1), calmodulin (CAM), glutathione peroxidase 3 (GPx-3), hemopexin (Hpx), apolipoprotein A1 (Apo-AI), and haptoglobin (Hp) using ELISA across both groups and plotted their trendlines. The proteins were chosen based on their regular significant appearance in different datasets in context of hypobaric hypoxia as well as either high relevance in hypoxia signaling (Trx, GPx-3) or novel functional insight (ST1A1, Apo AI). The proteins chosen had three common features. They were present in the plasma proteome in at least moderate amounts; they were recurrent in multiple proteome investigations focused on high-altitude and hypobaric hypoxia in context of high-altitude illnesses. Finally, all proteins had statistical significance in previous studies. These proteins were then assessed on their ability to indicate acclimation in an individual using standard statistical protocols. All aforementioned proteins were plotted as median with range (Fig. 2) to assess their plasma concentrations in both groups. We observed that perturbations were present not just across days of exposure but also in case of changes in altitude. The trendline formed by these perturbations may be indicators of altitude acclimation.

Plasma concentration of proteins in Group 1 and Group 2 at various sampling intervals. Concentration (y-axis) of assayed plasma proteins is plotted against baseline 1 (BL1; 216 m), high-altitude exposure day 1 (HAD1), HAD4, and HAD7L (same as) (at 3520 m) for Group 1 and BL2 (332 m), HAD7H, HAD30, and HAD120 (at 4420 m) for Group 2. The trendlines formed by the median values are investigated further as indicators of acclimation
ROC analysis of assayed plasma proteins
The protein concentrations were then subjected to statistical analysis consisting of ROC curve analysis (Supplementary figures Figs. S1–S12). Proteins with AUC values between 0.8 and 1 (good to excellent) with p values < 0.001 were further considered to plot trendlines in context of acclimation status. In context of this study, sensitivity of a protein is defined as its ability to positively indicate acclimation in an individual while specificity is defined as its ability to correctly identify the poorly acclimated individuals for a particular day and altitude zone.
Group 1 ROC analysis
It was observed that Trx and GPx-3 levels form the most accurate measures when testing an individual for an acclimating protein signature during stay at high-altitude zone (3520 m) for 7 days for all three intervals measured (HAD1, HAD4, HAD7L) against BL1 (Group 1) (Table 1). The sensitivity and specificity for Trx were 85% and 80% (BL1 vs HAD1); 90% and 80% (BL1 vs HAD4); 100% and 80% (HAD7L) (Table 1). For GPx-3, sensitivity and specificity were 80% and 85% (BL1 vs HAD1); 80% and 90% (BL1 vs HAD4); 85% and 85% (BL1 vs HAD7L) (Table 1). Other proteins whose trends can be used as signatures in this group for particular days of exposure are TR and Hp for HAD1; ST1A1, CAM, and Hpx for HAD4; and CAM, Hpx, and Hp for HAD7L (Table 1).
Group 2 ROC analysis
In Group 2 ROC analysis, the different intervals of measurement were HAD7H, HAD30, and HAD120 against BL2. Trx with AUC values of 0.8525 (p = 0.000138) in HAD7H; 0.97 (p < 0.0001) in HAD30; 0.9275 (p < 0.0001) in HAD120 and Apo-AI with AUC values of 0.865 (p < 0.0001) in HAD7H; 0.8825 (p < 0.0001) in HAD30; 0.835 (p = 0.000292) in HAD120 (Table 1) stand out as the most accurate set of proteins to check for acclimatization post 7 days at very high-altitude zone (4420 m). Trx showed 85% sensitivity and 80% specificity; 100% sensitivity and 75% specificity; and 90% sensitivity and 90% specificity (Table 1) while Apo-AI showed 90% sensitivity and 85% specificity; 90% sensitivity and 85% specificity; and 85% sensitivity and 75% specificity for HAD7H, HAD30, and HAD120, respectively (Table 1). Other proteins with accurate diagnostic ability but for given days are TR and CAM for HAD7H; CAM and GPx-3 for HAD30; and ST1A1 and Hpx for HAD120 (Table 1).
HAD1 vs subsequent high-altitude exposure days
The HAD1 group is a unique time point during high-altitude exposure as the subject has not acclimated and maximum incidence of illnesses like acute mountain sickness is reported (Smedley and Grocott 2013). But in this study, we are identifying HAD1 as pre-acclimated based on the hindsight that all individuals in both groups acclimated.
The ROC curve was plotted for HAD1 vs all subsequent days (HAD4 to HAD120) for all proteins. It was to investigate whether acclimation occurring across the temporal scale at different altitudes can be assessed by a protein signature. We observed that altitude itself played a definitive role along with the duration of stay. For Group 1 (till HAD7L), we observed TR to be accurate in terms of distinguishing between pre-acclimated and acclimated. TR had AUC 0.81 (p value = 0.000802) with 85% sensitivity and 70% specificity (Table 1) at HAD4 and AUC 0.8125 (p value = 0.000727) with 85% sensitivity and 75% specificity at HAD7L (Table 1). No effect of altitude variation was observed in TR’s accuracy as in Group 2 HAD7H, it had similar AUC 0.8125 (p value = 0.000727) with 80% sensitivity and 75% specificity (Table 1). For Group 2 (from HAD7H till HAD120), GPx-3, Apo-AI, and Trx were observed to be highly capable of the same (Table 1).
Other proteins which had good/excellent AUC values for certain days include ST1A1 for HAD4; Hpx and Hp for HAD7L; CAM and Hpx for HAD7H; ST1A1, CAM, and Hp for HAD30; and ST1A1 and Hp for HAD120 (Table 1). A notable mention must be made of ST1A1 in accurately differentiating between HAD1 and HAD4 samples. This corroborates its ability to distinguish between controls and HAPE patients, as previously observed (Ahmad et al. 2015).
Assessing effects of altitude variation
Based on the comparison of various days of high-altitude exposure against HAD1, we observed a distinction in marker proteins as per the change in altitude. Between Group 1 and Group 2, HAD7 is the common timepoint of sample collection but in two different altitude zones (high- vs very high-altitude zones). Thus, this timepoint can have proteins that can be indicative of just altitude-dependent systemic response without the duration of exposure being a factor upon moving to a higher altitude in an acclimated individual. GPx-3, Apo-AI, Hp, TR, CAM, and Trx provide exceptional accuracy with regard to increasing altitude acclimation (Table 1). We observed that among these proteins, differences in fold change values are significant at the two altitudes for Trx, CAM, Apo-AI, and Hp (Fig. 3a). The fold change values are direct comparisons of ratio of protein level at their respective baseline values (either BL1 or BL2) vs HAD7 (either HAD7L or HAD7H). Thus, this particular pattern of proteins can be useful when acclimation response needs to be checked at very high-altitude zone upon ascending from a high-altitude zone. A similar trend in protein fold change values (as shown in Fig. 3a) can be used as an indication that the individual is acclimated to very high-altitude zone.

Fold change differences of proteins between high- and very high-altitude zones and protein concentration trendlines depicting acclimation across temporal scale. (a) Fold change values were calculated for HAD7L vs BL1 (Group 1) and HAD7H vs BL2 (Group 2) with baseline being normalized to 1 in both cases. Fold change values were then plotted for all proteins comparing their respective fold change values between HAD7L (at 3520 m) and HAD7H (at 4420 m). Significance is shown using star over the bars. Trx (thioredoxin), TR (thioredoxin reductase), CAM (calmodulin), GPx3 (glutathione peroxidase 3), Apo A1 (apolipoprotein A1), and Hp (haptoglobin). ***p value≤0.0001. (b) Trendlines were plotted for fold change values (y-axis) vs Group 1 sampling intervals (x-axis). Fold change values were calculated by normalizing against BL1 (baseline). Trx and GPx3 were observed to be the most accurate in terms of determining acclimation status in high-altitude zone till HAD7 as per their AUC values. Thus, their trendline was plotted to provide an objective indicator of acclimation at high-altitude zone. (c) Trendlines were plotted for fold change values (y-axis) vs Group 2 sampling intervals (x-axis). Fold change values were calculated by normalizing against BL2 (baseline). Trx and Apo A1 were observed to be the most accurate in terms of determining acclimation status in very high-altitude zone till HAD120 as per their AUC values. Thus, their trendline was plotted to provide an objective indicator of acclimation at high-altitude zone. (d) Trendlines were plotted for fold change values (y-axis) against HAD1 for all subsequent exposure days across Groups 1 and 2 (x-axis). Trx, TR, GPx3, and Apo A1 were observed to provide maximal accuracy as per their AUC values in distinguishing between pre-acclimated (HAD1) and acclimated (HAD4–HAD120). Fold change values were calculated by normalizing against HAD1. Thus, their trendline was plotted to provide an objective indicator of acclimation at both high- and very high-altitude zones when baseline readings are unavailable
Trendlines depicting acclimation in selected plasma proteins
We have clearly established statistically significant proteins with their median values (and range). But the entire point of this investigation was to create a plasma protein signature that defines acclimation to altitude. Two proteins, Trx and GPx-3, were observed to represent an acclimating response in Group-1 (3520 m) till HAD7L with significant accuracy based on their AUC values along with sensitivity and specificity (Table 1). Thus, their trendline was plotted based on fold change values (calculated from median) in respective groups with baseline (both BL1 and BL2) normalized to 1 (Fig. 3b). It was observed that Trx levels remain unchanged while GPx-3 levels rise significantly at HAD4 before declining close to baseline levels at HAD7L. In case of longer duration of high-altitude exposure at very high-altitude zone (observed in Group 2; 4420 m), Trx and Apo-AI, were observed to provide the best accuracy to determine acclimation (Fig. 3c). According to AUC values of HAD1 vs HAD4 and HAD7L (Table 1), TR shows the best accuracy in distinguishing between pre-acclimated and acclimated. Also, when comparing HAD1 vs HAD7H, TR has similar AUC. The trendline of TR (Fig. 3d) shows continuous increase through HAD1 till HAD7L before a sharp decline at HAD7H.
As per the AUC values of Apo-AI, Trx, and GPx-3, they were highly accurate in distinguishing pre-acclimated (HAD1) from acclimated at HAD7, HAD30, and HAD120. Their trendline was plotted to indicate the levels of these proteins during long-term exposure to a very high-altitude zone (Fig. 3d).
Discussion
We observed that TR, GPx-3, Apo-AI, and Trx, with a negative control as HAPE-discriminating SULT1A1, form a suitable panel of proteins to assess acclimation during Stage I and Stage II of Indian Army acclimation protocol till HAD120. High-altitude acclimation till date has been an empirical subjective process where stratification of individuals into acclimated or non-acclimated categories depended on absence of any discomfort to the climber. Indian Army has an empirical method of assessment which designates an individual as acclimated to a given altitude based on his performance of certain physical tasks (walk, run, and climb at altitude) (Deshwal et al. 2012) which although not perfect still is better than no assessment at all. However, this lack of an objective method of acclimation assessment put the climbers at great risk since they might ascend to more remote altitudes before they knew that their lives are at stake due to poor acclimation leading to increased risk of high-altitude illnesses. Thus, we have endeavored to find an objective method of altitude acclimation. In this study, we have proposed certain proteins whose trendlines based on ROC analysis were observed to be accurate in determining the acclimation status of individuals exposed to altitudes.
A hypothetical device and its intended use based on our findings are also proposed: a biomarker panel with separate coated wells and attached capillaries will have antibodies of Trx, Apo-AI, GPx-3, and ST1A1 coated separately in respective wells. To monitor the reaction, a colored enzyme-reagent pair may be used. As the individual is performing staged ascent to a high-altitude area, he/she will have to take 3 to 4 separate strips with them to measure on the first day (either just before ascent or on the first day of ascent) followed by a second measure on either first day of ascent (if first measure was just before ascent) or on the fourth day of ascent and third measure on the seventh day of ascent. In case there is Stage II acclimation to a higher altitude zone, the final measurement may be taken at either the 30th or 120th days of ascent. There is minimal chance of any false results as inter-individual variations are prevented and cut-off values are not required.
Trx, GPx-3, and TR are part of the thioredoxin-glutaredoxin system. The thioredoxin-glutaredoxin system has been known since 1989 as a central antioxidant system that is pivotal in redox homeostasis (Holmgren 1989; Björnstedt et al. 1994). Thioredoxin (Trx) is essential to survival and loss-of-function mutations lead to embryonic lethality (Haendeler et al. 2002). Thioredoxin reductase (TR) is essential for keeping thioredoxin in reduced state (Arnér and Holmgren 2000). GPx-3, apart from its role as an antioxidant, has also been observed in multiple hypoxia studies to be differentially expressed (Kumral et al. 2005; Nakanishi et al. 1995). Apo-AI in a previous investigation was observed to increase in HAPE patients as compared with normoxic controls (Ahmad et al. 2011). In this study too, trends show an increase at and after 7 days of exposure. But the quantum of change in acclimated and HAPE patients as compared with normoxic controls is vast. In this study, the fold change increase of Apo-AI is about 2-fold whereas for HAPE cases, the plasma levels of Apo-AI rise more than 7-fold. This indicates that increases in plasma Apo-AI levels more than 3-fold may be considered an early sign of illness, especially HAPE, during high-altitude exposures.
We also prove that measuring baseline levels of proteins may be skipped altogether in favor of HAD1 protein levels as it also provided accurate trends in assessing acclimation. In biological sciences, controls are essential to any experiment. In case of hypoxia, normoxic controls have been considered the norm. However, in case of acclimation to high-altitude hypoxia, the proteins and their trends are significantly accurate even when comparing the 1st day of exposure (HAD1) with the subsequent days (HAD4-HAD120). We observed that TR, GPx-3, Apo-AI, and Trx form a suitable panel of proteins to assess acclimation during Stage I and Stage II till HAD120.
A protein of particular interest, especially for longer stays at higher altitudes, is the calcium messenger, Cam. Its levels are highly accurate in indicating acclimation at HAD7 (both HAD7L and HAD7H), HAD30, and HAD120 till altitude of 4420 m (very high-altitude zone). A future direction of investigation regarding long-term acclimation to altitude and eventually adaptation may be the study of calcium associated/regulated signaling proteins and events. Calcium signaling events have already been implicated in important research domains like cancer signaling, neuronal health, inflammation, infectious diseases, muscle hypertrophy, obesity, diabetes, oxidative stress, and cardiac conditions (Arruda and Hotamisligil 2015; Bezprozvanny 2009; Bezprozvanny and Hayden 2004; Bhosale et al. 2015; Boyle et al. 2014; Climent et al. 2014; Demuro et al. 2010; Lewis 2001; Lourido and Moreno 2015; Nikolskaia et al. 2006). We hypothesize that acclimation to hypoxia, particularly hypobaric hypoxia, during chronic and severe exposures may be associated with calcium signaling which may cause a shift in the metabolic state of the cell. This aspect could be further dealt with using in vitro and animal models in future studies. Based on the relevance and commonality of calcium signaling events in the other domains stated above, we may evolve our understanding towards the most basic response of an organism to adapt to its environment metabolically.
Study limitations
This study has two limitations. The relatively small sample size may not provide the most accurate of trends concerning the proteins of interest. Also, due to small sample size, cut-off values depicting significant departures from the established trendline, indicative of non-acclimatization could not be established. However, the overall accuracy of the proteins in assessing acclimation is proven by the good and excellent AUC values which bypass the restrictions of small sample sizes. The second limitation of this study is the absence of any cases of diseased individuals. As no individual in the sample suffered from any high-altitude illness due to non-acclimation, we cannot state kind (positive or negative) and quantum of deviation from the protein trends observed in acclimation. However, we have tried to correlate studies detailing high-altitude illnesses with proteins in this study, e.g., ST1A1 and Apo-AI, to overcome this lacuna and provide insight into distinguishing acclimated from non-acclimated.
Conclusion
The present study, we believe is a major culmination of the various investigations into proteome-based altitude acclimation markers. This study shall provide a feasible and robust method to objectively identify acclimated individuals and those with susceptibility to high-altitude illness, particularly HAPE. Also, a conceptual framework for a diagnostic tool has been established.
Data and materials availability
Correspondence and requests for materials should be addressed to yasminchem@gmail.com.
References
Ahmad Y, Shukla D, Garg I, Sharma NK, Saxena S, Malhotra VK, Bhargava K (2011) Identification of haptoglobin and apolipoprotein AI as biomarkers for high altitude pulmonary edema. Funct Integr Genomics 11(3):407–417
Ahmad Y, Sharma NK, Garg I, Ahmad MF, Sharma M, Bhargava K (2013) An insight into the changes in human plasma proteome on adaptation to hypobaric hypoxia. PLoS One 8(7):e67548
Ahmad Y, Sharma NK, Ahmad MF, Sharma M, Garg I, Bhargava K (2014) Proteomic identification of novel differentiation plasma protein markers in hypobaric hypoxia-induced rat model. PLoS One 9(5):e98027
Ahmad Y, Sharma NK, Ahmad MF, Sharma M, Garg I, Srivastava M, Bhargava K (2015) The proteome of hypobaric induced hypoxic lung: insights from temporal proteomic profiling for biomarker discovery. Sci Rep 5:10681
Ahmad Y, Mishra S, Arya A, Paul S, Sharma M, Prasad J, Bhargava K (2016) Revisiting cobalt chloride preconditioning to prevent hypobaric hypoxia-induced damage: identification of global proteomic alteration and key networks. Funct Integr Genomics 16(3):281–295
Arnér ES, Holmgren A (2000) Physiological functions of thioredoxin and thioredoxin reductase. Eur J Biochem 267(20):6102–6109
Arruda AP, Hotamisligil GS (2015) Calcium homeostasis and organelle function in the pathogenesis of obesity and diabetes. Cell Metab 22(3):381–397
Bezprozvanny I (2009) Calcium signaling and neurodegenerative diseases. Trends Mol Med 15(3):89–100
Bezprozvanny I, Hayden MR (2004) Deranged neuronal calcium signaling and Huntington disease. Biochem Biophys Res Commun 322(4):1310–1317
Bhosale G et al (2015) Calcium signaling as a mediator of cell energy demand and a trigger to cell death. Ann N Y Acad Sci 1350(1):107–116
Björnstedt M et al (1994) The thioredoxin and glutaredoxin systems are efficient electron donors to human plasma glutathione peroxidase. J Biol Chem 269(47):29382–29384
Boyle KE, Hwang H, Janssen RC, DeVente JM, Barbour LA, Hernandez TL, Mandarino LJ, Lappas M, Friedman JE (2014) Gestational diabetes is characterized by reduced mitochondrial protein expression and altered calcium signaling proteins in skeletal muscle. PLoS One 9(9):e106872
Climent B, Moreno L, Martínez P, Contreras C, Sánchez A, Pérez-Vizcaíno F, García-Sacristán A, Rivera L, Prieto D (2014) Upregulation of SK3 and IK1 channels contributes to the enhanced endothelial calcium signaling and the preserved coronary relaxation in obese Zucker rats. PLoS One 9(10):e109432
Demuro A, Parker I, Stutzmann GE (2010) Calcium signaling and amyloid toxicity in Alzheimer disease. J Biol Chem 285(17):12463–12468
Deshwal R, Iqbal M, Basnet S (2012) Nifedipine for the treatment of high altitude pulmonary edema. Wilderness Environ Med 23(1):7–10
Haendeler J, Hoffmann J, Tischler V, Berk BC, Zeiher AM, Dimmeler S (2002) Redox regulatory and anti-apoptotic functions of thioredoxin depend on S-nitrosylation at cysteine 69. Nat Cell Biol 4(10):743–749
Holmgren A (1989) Thioredoxin and glutaredoxin systems. J Biol Chem 264(24):13963–13966
Karinen H, Peltonen J, Tikkanen H (2008) Prevalence of acute mountain sickness among Finnish trekkers on Mount Kilimanjaro, Tanzania: an observational study. High Alt Med Biol 9(4):301–306
Kumral A, Gonenc S, Acikgoz O, Sonmez A, Genc K, Yilmaz O, Gokmen N, Duman N, Ozkan H (2005) Erythropoietin increases glutathione peroxidase enzyme activity and decreases lipid peroxidation levels in hypoxic-ischemic brain injury in neonatal rats. Neonatology 87(1):15–18
Lewis RS (2001) Calcium signaling mechanisms in T lymphocytes. Annu Rev Immunol 19(1):497–521
Lourido S, Moreno SN (2015) The calcium signaling toolkit of the Apicomplexan parasites toxoplasma gondii and Plasmodium spp. Cell Calcium 57(3):186–193
Nakanishi K, Tajima F, Nakamura A, Yagura S, Ookawara T, Yamashita H, Suzuki K, Taniguchi N, Ohno H (1995) Effects of hypobaric hypoxia on antioxidant enzymes in rats. J Physiol 489(3):869–876
Nikolskaia OV, de A. Lima APC, Kim YV, Lonsdale-Eccles JD, Fukuma T, Scharfstein J, Grab DJ (2006) Blood-brain barrier traversal by African trypanosomes requires calcium signaling induced by parasite cysteine protease. J Clin Invest 116(10):2739–2747
Padhy G, Sethy NK, Ganju L, Bhargava K (2013) Abundance of plasma antioxidant proteins confers tolerance to acute hypobaric hypoxia exposure. High Alt Med Biol 14(3):289–297
Paul S, Gangwar A, Bhargava K, Ahmad Y (2018) STAT3-RXR-Nrf2 activates systemic redox and energy homeostasis upon steep decline in pO2 gradient. Redox Biol 14:423–438
Ren Y, Fu Z, Shen W, Jiang P, He Y, Peng S, Wu Z, Cui B (2010) Incidence of high altitude illnesses among unacclimatized persons who acutely ascended to Tibet. High Alt Med Biol 11(1):39–42
Smedley T, Grocott MP (2013) Acute high-altitude illness: a clinically orientated review. Br J Pain 7(2):85–94
Syed V, Sharma S, Singh R (2010) Determinants of acclimatisation in high altitude. Med J Armed Forces India 66(3):261–265
Tyagi T, Ahmad S, Gupta N, Sahu A, Ahmad Y, Nair V, Chatterjee T, Bajaj N, Sengupta S, Ganju L, Singh SB, Ashraf MZ (2014) Altered expression of platelet proteins and calpain activity mediate hypoxia-induced prothrombotic phenotype. Blood 123(8):1250–1260
Acknowledgments
The authors also thank Dr. Aditya Arya for his inputs in designing Figure 1.
Funding
The study was carried out under Project DIP-263 funded by DRDO. Subhojit Paul is a recipient of CSIR fellowship. Anamika Gangwar is a recipient of DST-INSPIRE fellowship.
Author information
Authors and Affiliations
Contributions
Y.A. conceptualized the study. K.B. provided the plasma samples. S.P. and A.G. carried out the experiments. S.P, A.G, Y.A, and P.K analyzed and interpreted the data. N.K provided us the weight and age of each volunteer in both the groups. S.P. and A.G. wrote the manuscript. Y.A. critically evaluated and drafted the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 2327 kb)
Rights and permissions
About this article

Cite this article
Paul, S., Gangwar, A., Bhargava, K. et al. Plasma protein(s)–based conceptual diagnostic tool for assessing high-altitude acclimation in humans. Funct Integr Genomics 20, 191–200 (2020). https://doi.org/10.1007/s10142-019-00712-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10142-019-00712-0