
Abstract
Purpose
This study evaluates clinical and laboratory parameters, as well as extravasation and hematoma size on CTA as potential predictors of conventional angiogram (CA) results.
Methods
This is a retrospective study of 380 adult patients presenting with pelvic trauma over a 9-year period. Of these patients, 91 were found to have active arterial extravasation on initial CTA. Statistical analysis between the two groups +CA versus −CA was performed to determine whether clinical and laboratory parameters, as well as extravasation size and hematoma size could predict CA results.
Results
There were no significant differences in all clinical and laboratory data, including hemodynamic instability (defined as systolic blood pressure < 90 mmHg) on presentation (22.2% vs. 21.4%), except for Glasgow Coma Scale (p = 0.015) when comparing the two groups. Extravasation size and hematoma size as continuous or categorical variables were not predictive of subsequent positive CA. Secondary analysis demonstrated no association between select parameters (i.e., hematocrit, systolic blood pressure, and lactate) and subsequent positive CA while controlling for extravasation size or hematoma size.
Conclusion
Clinical and laboratory parameters in blunt pelvic trauma with arterial hemorrhage were not significantly associated with subsequent conventional angiography results, once accounting for degree of hemorrhage. The area of the foci of active extravasation and hematoma size in the axial plane were not significantly associated with the need for embolization. We conclude from these findings that catheter angiography should be considered in patients with blunt pelvic trauma found to have active arterial extravasation, regardless of size of bleed or the patient’s clinical or laboratory values.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Computed tomography angiography (CTA) has become the first-line modality for evaluating hemodynamically stable patients sustaining high-energy trauma with suspicion for pelvic fracture and associated bleeding. Despite the high sensitivity and specificity of pelvic CTA in diagnosing arterial bleeding [1], CTA findings do not always correlate with subsequent positive conventional angiography (CA) [2,3,4,5,6], leading to delays in appropriate care and potentially fatal outcomes. Previous studies have identified possible clinical and laboratory parameters in predicting bleeding and mortality after high-energy trauma [7,8,9]. Furthermore, studies have found that volume of pelvic hematoma on CT is a strong predictor of major arterial injury requiring angioembolization in trauma victims with pelvic fractures [10]. This study evaluates clinical and laboratory parameters, as well as degree of extravasation and hematoma size on CTA as potential predictors of CA results and the need for angioembolization.
Materials and methods
This study was conducted at an urban, level I trauma center, and major referral center with over 2,000 trauma admissions and more than 140,000 emergency department visits annually. This retrospective study was approved by the Institutional Review Board (IRB), is HIPAA-compliant, and informed consent was waived. All adult patients (between the ages of 18 and 65) presenting with pelvic trauma over a 9-year period and sustained pelvic trauma by admission CT imaging were identified. Patients with traumatic brain injury or arriving to the endovascular suite more than 7 h after presentation were excluded from data analysis (Fig. 1). Review of electronic medical record (EMR) was performed, and admission clinical and laboratory parameters were recorded: heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), oxygen saturation (SpO2), respiratory rate (RR), Glasgow Coma Scale (GCS), hemoglobin (Hgb), hematocrit (Hct), lactate, pH, bicarbonate, blood urea nitrogen (BUN), and creatinine (Cr). Extravasation and hematoma size on CTA were also collected.

Flow diagram of the study population
Multiphasic computed tomography
All patients received a single intravenous bolus of 100 mL of iohexol (350 mg of iodine per milliliter, Optiray; Mallinckrodt Imaging, Hazelwood, Mo). Per institutional protocol, patients with suspected pelvic injury underwent pelvic CTA, which included images from the iliac crests to the greater trochanters, beginning 23 s after the start of the contrast material injection. CT scanning of the chest, abdomen, and pelvis was then completed after pelvic CTA acquisition. Given severity of the injuries detected on portal venous phase images, 5-min delayed phase images of the abdomen and pelvis were acquired. Scanning delays from the time of injection were 30 s for chest CT, 70 s for abdominopelvic CT, and 5 min for delayed phase CT. No oral contrast material was administered per department protocol.
Image analysis
Two radiologists, including one resident level (blind) and abdominal fellowship-trained, board-certified body attending (blind) retrospectively reviewed all CT images in consensus at a picture archiving and communication system workstation. Areas of active arterial hemorrhage identified were expected to increase in size and remain of higher attenuation than the aorta on both portal venous phase and delayed phase images. Extravasation size was determined by measuring the largest anterior-posterior (AP) and transverse (TV) dimensions during portal venous phase images on axial view, and the values were used to calculate the area of an ellipse (π × AP/2 × TV/2). Size of extravasation was then categorized as small, medium, and large corresponding to lower, middle, and upper terciles of the cohort. Hematoma size was determined and categorized in a similar fashion.
The rationale for measuring in the portal venous phase is because of limitations in measuring extravasation size: we assumed that contrast blush measured in arterial phase would be too small to be of significance and in delayed-phase imaging; contrast has dissipated and therefore cannot be measured.
A representative case is included as Fig. 2.

Representative example: 22-year-old healthy female presenting as a pedestrian struck by motor vehicle traveling approximately 35–40 mph. a Axial CT in portal venous phase demonstrating region of extravasation (black arrow). b Selective angiography demonstrating active extravasation from a small branch of the internal iliac artery
Statistical analysis
Admission clinical and laboratory parameters were obtained from the Electronic Medical Records (EMR). Obtained parameters included heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), oxygen saturation (SpO2), respiratory rate (RR), Glasgow Coma Scale (GCS), hemoglobin (Hgb), hematocrit (Hct), lactate, pH, bicarbonate, blood urea nitrogen (BUN), and creatinine (Cr).
The proportion of patients presenting with hemodynamic instability, defined as a SBP < 90 was also determined.
The aim of the primary analysis was to evaluate the association between positive CA and extravasation or hematoma size while controlling for clinical parameters previously reported to be associated with the need for angioembolic interventions such as hematocrit, systolic blood pressure, and lactate. Analysis was performed with the extravasation and hematoma sizes as continuous variables and as categorical variables where extravasation and hematoma sizes were divided into terciles.
Secondary analyses were done to identify additional clinical parameters, which are associated with +CA using Student’s t test for continuous variables and Fisher’s exact test for categorical variables. Exploratory analysis was performed to evaluate the association of clinical parameters with extravasation size as a categorical variable, which was done based on ANOVA or Kruskal-Wallis test.
All statistical analyses were performed using R, version 3.6.3 and all p values < 0.05 were considered significant.
Results
Patient population
A total of 380 patients sustaining pelvic trauma were enrolled, of which 354 received a CTA. Ninety-one patients were found to have active extravasation on CTA. Patients with traumatic brain injury or arriving more than 7 h after presentation were excluded. Seventy-three patients subsequently underwent pelvic CA. Of these patients, there were 30 female and 43 male patients included in this study. Patients were divided into two groups: 45 patients with extravasation on conventional angiogram (+CA) and 28 patients with no extravasation on conventional angiogram (−CA). The mean age between both groups was 51.1 and 54.4 respectively.
Mechanism of injury for the patients ultimately undergoing CA included GSW (n = 1), motor vehicle collision (n = 20), pedestrian struck (n = 28), motorcycle/moped accident (n = 8), fall (n = 10), and other crush injury (n = 6).
In the current cohort, the sensitivity and specificity for detecting contrast extravasation on CTA when using CA as the gold standard confirmatory test were 100% (95%CI: 92.13–100%) and 90.38% (95%CI: 86.39–93.51%) respectively. The positive predictive value was 61.64% (95%CI: 53.05–69.56%). The negative predictive value was 100%.
Clinical/laboratory parameters
Statistical analysis of clinical and laboratory parameters are described in Table 1. Differences in HR, SBP, DBP, SpO2, RR, HGB, HCT, lactate, pH, bicarbonate, BUN, and Cr were not significant. In addition, the proportion of patients that were hemodynamically unstable on presentation was not significant (22.2% vs. 21.4%). GCS was lower in the positive group (p = 0.015).
Extravasation size and hematoma size
The categorical terciles designated as small, medium, and large were demonstrated to be significantly different for both extravasation size and hematoma size (data not included).
Statistical analysis of extravasation size and hematoma size are described in Table 2.
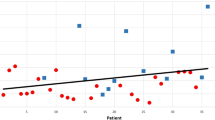
There was no significant difference between extravasation size or hematoma size associated with positive CA when comparing small versus medium, medium versus large, or small versus large. Logistic regression using extravasation size or hematoma size as a continuous variable was not significant.
Logistic regression with the covariates HCT, SBP, and lactate demonstrated no statistically significant differences using extravasation or hematoma size as either a continuous or categorical variable for predicting positivity at subsequent CA.
ANOVA and Kruskal-Wallis tests in all patients with extravasation on initial CTA determined no significant difference in all variables and is described in Table 3 except for SpO2 (p = 0.015) and post hoc analysis demonstrated significance between small versus large (p = 0.0326), medium versus large (p = 0.007), but not small versus medium (p = 0.653) (Table 3).
Hospital course and outcomes
The average time to CTA was 1 h and 29 min in the +CA group versus 1 h and 27 min in the −CA group (p = 0.473). The average time to CA was 3 h and 23 min in the +CA group versus 3 h and 26 min in the −CA group (p = 0.451).
Of the 45 + CA, 11 patients expired during hospitalization. Five of these patients expired on day of admission, and 3 of these patients expired during surgical exploration in addition to angiography.
Of the 28 −CA patients, 2 patients expired during hospitalization. One of these patients expired on day of admission and this patient was intra-op.
Length of hospitalization and intensive care unit stay, as well as patient disposition on discharge are summarized in Table 4.
Discussion
Current evidence suggests contrast-enhanced CT is the most sensitive and specific test to identify the source of arterial bleeding in the pelvis when the clinical condition of the patient permits [1,2,3,4,5,6]. The Society of Interventional Radiology position statement reports indications for CA with possible embolization therapy in the presence of a vascular injury or contrast agent extravasation on contrast-enhanced CT in association with other findings of vascular injury on imaging [11]. Some studies report that when active contrast agent extravasation is demonstrated on CTA of the pelvis, there is a higher likelihood of active arterial hemorrhage demonstrated at the time of CA, with sensitivity ranging from 80 to 90% and specificity ranging from 85 to 98% [12, 13]. In our cohort of pelvic trauma patients, sensitivity and specificity was 100% and 90.38% respectively, and negative predictive value was 100%. However, CTA findings do not always correlate with subsequent findings at CA. For example, the PPV in Jeurn’s study was 22.7% [14], and the study concluded that “contrast extravasation is common, but many patients will not require angioembolization”. The PPV in the current study is 61.64%, which alone warrants further evaluation with CA if there is extravasation identified on CTA. This difference could potentially be explained by differences in institutional protocol, scanning technique, and/or threshold for scanning patients.
It is taught in Trauma Surgery that clinical parameters and laboratory values, specifically initial hematocrit do not accurately reflect estimated blood loss in patients suffering severe trauma and hemorrhage [15]. Several studies have attempted to challenge that teaching and report that the rate of fluid shift from the interstitial space into the vasculature is relatively quick, contrary to historical teaching [15]. Additional studies have suggested that other clinical and laboratory parameters, such as lactate [7] and systolic blood pressure [8, 9], are useful for predicting need for angioembolization in pelvic trauma patients. Our study essentially demonstrated no statistically significant variables (aside from GCS) associated with subsequent positive CA following a positive CTA. Furthermore, multivariate logistic regression for CTA extravasation size with Hct, SBP, and lactate as covariates demonstrated no statistically significant results. A possible explanation for these findings is related to inability to control for factors taking place between the inciting event and presentation to hospital.
Several studies have utilized variations of the GCS to predict mortality in adult severe trauma patients with head injury and also hypovolemic shock, noting two recent studies by Wu et al. [16] and Chu et al. [17], in which the groups utilize a novel scale derived by multiplying the reverse Shock Index defined as the ratio of SBP to HR by GCS. However, a major limitation of utilizing GCS is the fact that direct injury to the central nervous system produces its own set of physiologic changes and in extremes can result in neurogenic shock. For this reason, all patients from our cohort with traumatic brain injury were excluded. Although our data is significant for oxygen saturation as a variable associated with differences in extravasation size, these results are limited as documentation of the quantity of oxygen requirements is poorly documented.
Lactate was not significant when accounting for extravasation or hematoma size (OR 1.085–1.101, p = 0.306–0.386) in the current study. A recent study by Fukuma et al. [7] found that lactate collected at the scene of incident was significantly associated with an increased probability for immediate intervention, whether endovascular or surgical. It is possible that if our cohort had lactate collected from the scene of the incident, it would also be associated with increased probability for subsequent CA requiring embolization in patients with extravasation on initial CTA.
There have been at least two notable studies suggesting the importance of pelvic hemorrhage volumes in predicting therapeutic endovascular requirements. A study by Blackmore et al. in 2006 found that subjects with large pelvic hemorrhage volumes (> 500 mL) were more likely to have pelvic arterial injury than patients with smaller pelvic hemorrhage volumes [18]. In this study, area of hemorrhage on single axial images was calculated and subsequently multiplied by the CT scan slice thickness and summed to determine total volume. A more recent study by Dreizin et al. [10] used a logistic regression model incorporating semiautomated hematoma volume segmentation to estimate a cutoff volume of 433 mL for predicting major arterial injury requiring angioembolization with a positive predictive value of 87–100%.
We attempted to recreate these findings in a setting that would simulate a real-time trauma using quick and simple measurements that any radiologist at a workstation would be able to perform. Using simple logistic regression, we did not find that extravasation size or hematoma size could reliably predict angioembolization requirement. Another study by Anderson et al. was suggestive of similar findings, although the primary objective in that study was to differentiate arterial and venous hemorrhage [19]. Although the simplicity of measuring the area of extravasation in a single plane may underestimate the degree of hemorrhage, we did not believe it to be a substantial underestimation given the largest measurement in a single axial dimension was 1.2 cm. Hematoma would be less reliable as the largest measured axial dimension was 17 cm. It would be interesting to perform a multivariate logistic regression with the covariates we examined and hematoma volume acquired through semiautomated volume segmentation analysis. It would also be interesting to see if there are any significant differences in clinical or laboratory parameters in patients with hematoma volume below versus above the cutoff determined by Dreizin’s group.
There are several limitations to the current study including the retrospective nature of the study and the relatively small sample size. The one variable that did show statistical significance was GCS, which has inherent limitations as described above. Even with the limitations, we believe that these are areas that warrant further investigation in future studies given the inherent instability of trauma patients and the desire to minimize unnecessary procedures and expedite their transfer to ICU level of care.
Availability of data and material
Not applicable
References
Mohseni S, Talving P, Kobayashi L, Lam L, Inaba K, Branco BC, Oliver M, Demetriades D (2011) The diagnostic accuracy of 64-slice computed tomography in detecting clinically significant arterial bleeding after pelvic fractures. Am Surg 77(9):1176–1182
Papakostidis C, Kanakaris N, Dimitriou R, Giannoudis PV (2012) The role of arterial embolization in controlling pelvic fracture haemorrhage: a systematic review of the literature. Eur J Radiol 81:897–904
Agolini SF, Shah K, Jaffe J, Newcomb J, Rhodes M, Reed JF 3rd. (1997) Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma 43:395–399
Pereira SJ, O’Brien DP, Luchette FA et al (2000) Dynamic helical computed tomography scan accurately detects hemorrhage in patients with pelvic fracture. Surgery. 128:678–685
Brasel KJ, Pham K, Yang H, Chirstensen R, Weigelt JA (2007) Significance of contrast extravasation in patients with pelvic fracture. J Trauma 62:1149–1152
Verbeek DO, Zijlstra IA, van der Leij C, Ponsen KJ, van Delden OM, Goslings JC (2014) Management of pelvic ring fracture patients with a pelvic “blush” on early computed tomography. J Trauma Acute Care Surg 76:374–379
Fukuma H, Nakada T, Shimada T, Shimazui T, Aizimu T, Nakao S, Watanabe H, Mizushima Y, Matsuoka T (2019) Prehospital lactate improves prediction of the need for immediate interventions for hemorrhage after trauma. Sci Rep 9:13755
Bozeman MC, Cannon RM, Trombold JM, Smith JW, Franklin GA, Miller FB, Richardson JD, Harbrecht BG (2012) Use of computed tomography findings and contrast extravasation in predicting the need for embolization with pelvic fractures. Am Surg 78:825–830
Kuo LW, Yang SJ, Fu CY, Liao CH, Wang SY, Wu SC (2016) Relative hypotension increases the probability of the need for angioembolisation in pelvic fracture patients without contrast extravasation on computed tomography scan. Injury 47:37–42
Dreizin D, Bodanapally U, Boscak A, et al. CT prediction model for major arterial injury after blunt pelvic ring disruption. Radiology. 2018, 287, 1061, 1069.
Padia SA, Ingraham CR, Moriarty JM, Wilkins LR, Bream PR Jr, Tam AL, Patel S, McIntyre L, Wolinsky PR, Hanks SE (2020) Society of Interventional Radiology position statement on endovascular intervention for trauma. JVIR. 31(3):363–369
Shanmuganathan K, Mirvis SE, Sover ER (1993) Value of contrast-enhanced CT in detecting active hemorrhage in patients with blunt abdominal or pelvic trauma. AJR Am J Roentgenol 161:65–69
Cook RE, Keating JF, Gillespie I (2002) The role of angiography in the management of haemorrhage from major fractures of the pelvis. J Bone Joint Surg (Br) 84:178–182
Jeurn JS, Milia D, Codner P et al (2017) Clinical significance of computed tomography contrast extravasation in blunt trauma patients with a pelvic fracture. J Trauma Acute Care Surg 82(1):138–140
Ryan ML, Thorson CM, Otero CA, Vu T, Schulman CI, Livingstone AS, Proctor KG (2012) Initial hematocrit in trauma: a paradigm shift. J Trauma Acute Care Surg 72(1):54–59
Wu SC, Rau CS, Kuo SCH, Chien PC, Hsiao YH, Hsieh CH (2018) The reverse shock index multiplied by Glasgow Coma Scale score (rSIG) and prediction of mortality outcome in adult trauma patients: a cross-sectional analysis based on registered trauma data. Int J Environ Res Public Health 15:2346
Chu WT, Liao CH, Lin CY et al (2020) Reverse shock index multiplied by Glasgow Coma Scale (rSIG) predicts mortality in severe trauma patients with head injury. Nat Sci Rep 10:2095
Blackmore CC, Cummings P, Jurkovich GJ, Linnau KF, Hoffer EK, Rivara FP (2006) Predicting major hemorrhage in patients with pelvic fracture. J Trauma 61(2):346–352
Anderson SW, Soto JA, Lucey BC, Burke PA, Hirsch EF, Rhea JT (2008) Blunt trauma: feasibility and clinical utility of pelvic CT angiography performed with 64-detector row CT. Radiology 246(2):410–419
Author information
Authors and Affiliations
Contributions
Not applicable
Corresponding author
Ethics declarations
Conflict of interest/Competing interests
The authors declare that they have no conflicts of interest.
Code availability
Not applicable
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
HonShideler, C., Bernal-Fernandez, M., Hsu, M. et al. Clinical and laboratory parameters in blunt pelvic trauma not associated with subsequent positive conventional angiography in patients with positive CTA. Emerg Radiol 28, 557–563 (2021). https://doi.org/10.1007/s10140-020-01888-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-020-01888-w