
Abstract
Knee trauma is a common presenting symptom in the emergency setting. Avulsive knee injuries are important to diagnose timely and accurately to avoid unnecessary patient morbidity. Many of these avulsive knee injuries have characteristic appearances on imaging. This article presents a comprehensive review of some of the most common types with real cases used for imaging correlation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Knee trauma is a common presentation in emergency departments across the country with myriad etiologies and clinical implications. The complex tendinous and ligamentous attachments of the knee lend themselves to specific patterns of injury after trauma. Prompt recognition of these specific radiographic findings is crucial to avoid potentially significant morbidity that can accompany knee injury.
Acute avulsion fractures at the knee represent a subset of these traumatic injuries and include the well-known Segond, reverse Segond fractures, arcuate ligament, and cruciate ligament avulsions. Characteristic fractures may also be seen at the insertion of the arcuate ligament complex, iliotibial band, biceps femoris, semimembranosus, and patellar and quadriceps tendons.
Chronic repetitive injuries include Sinding-Larsen-Johansson syndrome and Osgood-Schlatter disease. These correlate to chronic repetitive micro-avulsion injuries. Similarly, periosteal sleeve avulsions occur in the pediatric population whereby the periosteum and/or a fragment of patellar articular cartilage is stripped from the upper or lower patellar pole.
Radiography is the usual first-line imaging modality with often subtle fracture morphology.
CT can confirm equivocal osseous findings in the majority of cases, especially in non-osteopenic bone, and can provide indirect signs of non-avulsive ligament tears. MRI provides additive value in assessing subtle fractures in osteopenic bone and the extent of secondary internal derangement.
General radiographic features of acute avulsive fractures of the knee often involve small bony fragments with irregular or sharply defined non-sclerotic, non-corticated margin(s). The fragment is often found in close proximity to a known tendinous or ligamentous attachment site, most commonly occurring at the epiphyses, apophyses, or bony protuberances. Associated features include soft tissue swelling, joint effusions, and malalignment.
Avulsion fractures about the knee should be considered the “tip of the iceberg,” usually denoting the presence of significant internal knee derangement for which MRI is ultimately indicated.
Posterior cruciate ligament (PCL) avulsion fracture (Figs. 1 and 2)
“Direct” sign of PCL avulsion fracture: Osseous fragment displaced from the PCL attachment is not often seen but pathognomonic when present.

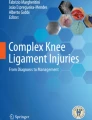
Cross-table AP and lateral radiographs of the right knee demonstrate a displaced cortical fragment originating from a donor site on the posterior tibial plateau at the location of the PCL insertion (red arrows). A suprapatellar lipohemarthrosis is also observed (green arrow). Isolated PCL disruption most commonly involves the tibial insertion and is associated with reverse Segond fracture. Vectors of injury include a direct blow to the anterior flexed knee in the setting of a dashboard impaction during an MVA for instance or with severe hyperextension

Sagittal bone windows CT (left) of the left knee in a different patient shows the utility of CT in the detection of minimally distracted PCL avulsions (red arrow). The lateral radiograph (not shown) was equivocal for fracture lucency. Sagittal proton density MRI image (right) demonstrates thickening, redundancy, and increased signal within the PCL (green arrow), which is attached to a mildly displaced bone fragment (blue arrow) from the posterior tibial plateau. Repair with reimplantation and fixation is warranted due to increased risk of premature osteoarthrosis and instability
Pearls
“Indirect” signs of PCL tear/avulsion fracture on radiographs and CT include: [1, 2]
-
1)
Reverse Segond fracture (deep meniscofemoral MCL fiber avulsion)
-
2)
Fracture isolated to the posterior tibial plateau
-
3)
Posterior sagging of the tibia relative to the femur on cross-table lateral view
-
4)
Anterior impaction fractures (with edema on MRI) of the femoral condyles and tibial plateau (hyperextension) or anterior tibial plateau (posterior displacement only).
Anterior cruciate ligament (ACL) avulsion fracture (Figs. 3 and 4)
Pearls
Radiographic and CT signs of ACL tear/avulsion fractures include: [8, 9]
-
1)
Deepened lateral femoral condylar notch greater than or equal to 1.5–2.0 mm
-
2)
Greater than or equal to 7 mm anterior tibial translation (100% PPV)
-
3)
Arcuate and Segond avulsion fractures (Segond fractures have essentially 100% PPV for ACL tear)
-
4)
On CT a PCL angle less than 105o (normal 113–114°) results in “buckling” of the PCL due to anterior tibial translation
-
5)
On CT the ACL does not parallel the Blumensaat line (roof of intercondylar notch)

Lateral and AP radiographs of the right knee show a fragment situated anteriorly and medially within the intercondylar notch adjacent to the site of distal ACL attachment (anterior tibial spine). ACL avulsions are more common in children, occurring during forced flexion-internal rotation of the tibia. In adults, the mechanism of injury is usually forced hyperextension and associated secondary internal injuries are common (see next section). Follow-up MRI is important to assess the integrity of the ACL, degree of distraction, and secondary injuries thereby impacting surgical management. Associated avulsions include Segond and Arcuate fractures (see next section)

Sagittal PD WI and coronal fat-saturated T2 WI demonstrate avulsion fragment at the tibial insertion of the ACL (blue arrow) and adjacent marrow edema (red arrow). The Meyers/McKeever classification denotes four stages of progressively severe avulsion injury. Type I corresponds to a minimally displaced fragment, allowing for conservative treatment and rehabilitation. Type II fractures include a component of anterior fragment elevation, while types III (above) and IV involve complete separation of the fragment with added rotation or comminution being present in type IV. Arthroscopic reimplantation of the fragment is warranted in type II injuries to ensure union with internal fixation necessitated by type III and IV fractures
Segond avulsion fracture (Figs. 5 and 6)
Pearl
Do not assume a Segond fracture is old (i.e., from the initial ACL tear) in a patient with prior ACL reconstruction, especially in the presence of an effusion and recent trauma. Compare with prior studies! [10]

AP radiograph (left) and corresponding coronal bone windows CT (right) demonstrate small avulsion fragment adjacent to the lateral tibial plateau consistent with a Segond fracture (red arrows). This occurs at the insertion of the middle third of the lateral meniscocapsular ligament. Recent research has pointed to an avulsion of the “anterolateral ligament” as the etiology of the Segond fracture. Close inspection of the anterior tibial spine (ACL insertion) and fibular head (arcuate ligament and biceps femoris tendon insertions) should be performed on all radiographs to assess for secondary fractures incited by the initial rotatory varus stress injury. MRI is indicated in all cases to evaluate for internal derangement given the near 100% incidence of ACL tear and meniscal injuries

Coronal fat saturated T2 WI (right) shows florid edema in the soft tissue lateral to the joint line but only subtle disruption of the dark lateral tibial cortical margin (green arrow). The avulsed fragment is minimally displaced by the inserting lateral meniscocapsular ligament. Iliotibial band tears can be associated. Without radiographic correlation, Segond fractures can be difficult to diagnose on MRI in the presence of marked edema
Reverse Segond avulsion fracture (Figs. 7 and 8)

AP view shows a reverse Segond fracture (red arrow), seen as a bony fragment adjacent to the medial margin of the medial tibial plateau at the attachment site of the meniscotibial fibers of the deep MCL. Mechanism of injury is valgus stress with external rotation. There is a high association with PCL tears, so MRI is warranted [3]

Coronal fat-saturated T2 WI shows subcortical edema and a small reverse Segond avulsion fracture at the medial plateau deep capsular MCL insertion (red arrow). Note a contralateral bone bruise at the site of impaction injury involving the lateral femoral condyle (yellow arrow)
Arcuate ligament avulsion fracture and the posterolateral corner (PLC; Fig. 9)
PLC structures include the biceps femoris (BF) tendons (long + short), arcuate ligament, fabellofibular ligament, lateral collateral ligament (LCL), oblique popliteal ligament, and popliteofibular ligament. The arcuate, fabellofibular, and popliteofibular ligaments insert on the posterosuperior fibular styloid and LCL/BF anterolaterally. The “arcuate sign” is a thin sliver of bone at the posterosuperior portion of the fibular styloid process. LCL/biceps femoris avulsions tend to cause larger anterolateral fibular head avulsion fragments. [5]

Oblique view showing avulsion fragment representing the fibular styloid at attachment of the arcuate ligament complex (blue arrow), which forms the posterolateral joint capsule and is one of many of the posterolateral corner (PLC) supporting structures
Pearl
High association with ACL injury, so MRI is always warranted. Bone marrow edema of the posterior lateral tibial plateau on MRI should raise suspicion for PLC injury.
Iliotibial band avulsion fracture (Figs. 10 and 11) [6]

Mildly rotated AP radiograph of the right knee demonstrates an ossific fragment marginating the lateral tibial plateau (green arrow). A comminuted displaced distal femoral metaphyseal fracture is partially visualized

Axial CT image confirms the fragment to originate from the anterolateral tibial cortex at the level of Gerdy’s tubercle at the insertion of the iliotibial band. The iliotibial band, the distal component of the tensor fascia lata, constitutes a major stabilizing support structure for the anterolateral knee and avulsion fractures at this level are uncommonly seen in isolation (Segond fracture is the most frequent secondary fracture). Varus force to a flexed, internally rotated knee is the typical mechanism of injury
Quadriceps tendon avulsion fracture (Fig. 12) [6]

Lateral view (right) demonstrates proximally retracted avulsion fragment arising from the superior patellar pole at the quadriceps tendon insertion (blue arrow) with patella baja deformity. Avulsion fractures are uncommon at this level, usually seen in conjunction with sudden extreme contraction of the quadriceps during flexion as occurs in abrupt athletic deceleration. Injury more commonly occurs at the myotendinous junction of the distal quadriceps (gout, diabetes, collagen vascular disease, and hyperparathyroidism are predisposing conditions in this regard)
Patellar tendon avulsion fracture (Fig. 13)

Cross-table lateral view (left) demonstrates distally retracted avulsion fragment arising from the inferior patellar pole at the proximal patellar tendon insertion (red arrow) with patella alta deformity. The patellar tendon shadow is thickened and there is a knee effusion. The mechanism of injury typically involves eccentric contraction of the quadriceps apparatus while the foot is planted and the knee in flexion. Predisposing conditions also include diabetes, chronic renal failure, lupus and other collagen vascular diseases [1, 2]
Medial patellofemoral retinaculum avulsion fracture (Fig. 14)

Medial patellar retinacular avulsion is typically seen in conjunction with transient lateral patellar dislocation. Though often radiographically occult, small crescentic avulsion fragments may be seen marginating the medial patellar cortex on sunrise views or cross-sectional CT images (yellow arrows). Predisposing factors include dysplastic patellae with flattening of the articular surface or hypoplastic femoral trochlear grooves. The usual force vector is internal rotation applied to the flexed knee while the foot is planted [4]
Osgood-Schlatter disease (Figs. 15 and 16)

Secondary to chronic repetitive microtrauma at the unfused patellar tibial tubercle insertion in adolescent patients, Osgood-Schlatter disease manifests radiographically with regional swelling, fragmentation and hypertrophy of the tibial tubercle ossification center and blurring of the inferior margin of the retropatellar fat pad (blue arrow). Findings are bilateral in up to 50% of patients. Treatment is usually conservative with rest or immobilization, pain control and (if warranted) limited local steroid injections [2]

MRI can be beneficial in cases of early or radiographically inapparent Osgood-Schlatter disease, demonstrating patellar tendon distal swelling, fluid filled deep infrapatellar bursa, marrow edema and fragmentation at the tibial tubercle as well as thickening of the overlying cartilage as seen in these fat-saturated sagittal and axial PD images (blue arrows)
Sinding-Larson-Johansson syndrome (Figs. 17 and 18)

Representing the sequela of chronic repetitive microtrauma to the proximal patellar osseous insertion, SLJ syndrome is the pediatric correlate of jumper’s knee, characterized radiographically by the presence of small dystrophic calcific fragments marginating the inferior patellar pole and regional swelling of the patellar tendon (blue arrow). Over time, there may be elongation and secondary spurring/remodeling of the inferior patella. Early cases are usually radiographically occult. Relevant history of overuse and repetitive microtrauma is key in distinguishing from patellar sleeve avulsion injury, as previously discussed. Management is conservative and non-operative with rest, pain control and gradual quadriceps stretching exercises [2]

Especially useful in early or radiographically occult cases, MRI demonstrates thickening of the proximal patellar tendon with increased T2 signal (blue arrows) as seen on these coronal fat saturated T2 and sagittal PD images. Edema is also typically seen in the adjacent inferior patella often in conjunction with small low T1 low T2 dystrophic calcific foci marginating the cortex. There are overlapping imaging features with “Jumper’s Knee,” although the osseous findings in SLJ tend to be far more pronounced and age of onset is usually younger
Conclusion
Though often subtle, easily overlooked and innocuous in their radiographic appearance, avulsion fractures at the knee represent a gamut of potential musculoskeletal injuries that are often harbingers of more extensive internal derangement for which MRI is ultimately indicated. As such, it is incumbent upon the interpreting radiologist to not only have a thorough understanding of their pathophysiology and imaging features, but also of their potential prognostic implications. Timely orthopedic referral and early cross-sectional imaging evaluation may best avoid delayed diagnosis and decrease the incidence of secondary post-traumatic osteoarthrosis.
References
Gottsegen C, Eyer B, White E et al (2008) Avulsion fractures of the knee: imaging findings and clinical significance. Radiographics 28:1755–1770. https://doi.org/10.1148/rg.286085503
Stevens M, El-Khoury G, Kathol M et al (1999) Imaging features of avulsion injuries. Radiographics 19:655–672. https://doi.org/10.1148/radiographics.19.3.g99ma05655
Capps G, Hayes C (1994) Easily missed injuries around the knee. Radiographics 14:1191–1210. https://doi.org/10.1148/radiographics.14.6.7855335
Delzell P, Schils J, Recht M (1996) Subtle fractures about the knee: innocuous-appearing yet indicative of significant internal derangement. AJR 167:699–703
Huang G, Yu J, Munshi M et al (2003) Avulsion fracture of the head of the fibula (the “arcuate” sign); MR imaging findings predictive of injuries to the posterolateral ligaments and posterior cruciate ligament. AJR 180:381–387
Bencardino J, Rosenberg Z, Brown R et al (2000) Traumatic musculoskeletal injuries of the knee: diagnosis with MR imaging. Radiographics 20:S103–S120. https://doi.org/10.1148/radiographics.20.suppl_1.g00oc16s103
Vinson E, Major N, Helms C (2008) The posterolateral corner of the knee. AJR 190:449–458
Chang MJ, Chang CB, Choi JY, Je MS, Kim KT (2014) Can magnetic resonance imaging findings predict the degree of knee joint laxity in patients undergoing anterior cruciate ligament reconstruction? BMC Musculoskelet Disord 15(214). https://doi.org/10.1186/1471-2474-15-214
Ng WHA, Griffith JF, Hung EHY, Paunipagar B, Law BKY, Yung PSH (2011) Imaging of the anterior cruciate ligament. World J Orthop 2:75–84. https://doi.org/10.5312/wjo.v2.i8.75
Shaikh H, Herbst E, Rahnemai-Azar AA, Bottene Villa Albers M, Naendrup JH, Musahl V, Fu FH (2017) The Segond fracture is an avulsion of the anterolateral complex. Am J Sports Med 45(10):2247–2252. https://doi.org/10.1177/0363546517704845
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Beckett, R., Le, P., Rheinboldt, M. et al. Avulsion fractures of the knee: a review of the pathophysiology, radiographic, and cross-sectional imaging features. Emerg Radiol 26, 683–689 (2019). https://doi.org/10.1007/s10140-019-01711-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-019-01711-1