
Abstract
Background
We have established a risk-scoring system, termed the “eCura system,” for the risk stratification of lymph node metastasis in patients who have received noncurative endoscopic submucosal dissection (ESD) for early gastric cancer (EGC). We aimed to clarify whether this system contributes to the selection of patients requiring radical surgery after ESD.
Methods
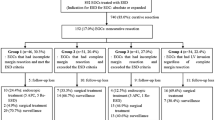
Between 2000 and 2011, 1,969 patients with noncurative ESD for EGC were included in this multicenter study. Depending on the treatment strategy after ESD, we had patients with no additional treatment (n = 905) and those with radical surgery after ESD (n = 1,064). After the application of the eCura system to these patients, cancer recurrence and cancer-specific mortality in each risk category of the system were compared between the two patient groups.
Results
Multivariate Cox analysis revealed that in the high-risk category, cancer recurrence was significantly higher (hazard ratio = 3.13, p = 0.024) and cancer-specific mortality tended to be higher (hazard ratio = 2.66, p = 0.063) in patients with no additional treatment than in those with radical surgery after ESD, whereas no significant differences were observed in the intermediate-risk and low-risk categories. In addition, cancer-specific survival in the low-risk category was high in both patient groups (99.6 and 99.7%). A limitation of this study is that it included a small number of cases with undifferentiated-type EGC (292 cases).
Conclusions
The eCura system is a useful aid for selecting the appropriate treatment strategy after noncurative ESD for EGC. However, caution is needed when applying this system to patients with undifferentiated-type EGC.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Previous reports have stated that 10.3–29.3% of early gastric cancers (EGCs) that were treated with endoscopic resection do not meet the current curative criteria [1,2,3,4,5,6,7,8]; this phenomenon is termed “noncurative resection.” According to the current treatment guidelines [9,10,11], gastrectomy with lymph node dissection is recommended for all such patients because of the potential risk of lymph node metastasis (LNM). However, only 5–10% of these patients develop LNM [3, 4, 7, 8, 12,13,14,15], and the merits of radical surgery for such patients remain unclear. Previous studies have revealed that cancer-specific survival (CSS) does not significantly differ between patients who are followed up but receive no additional treatment and those who undergo radical surgery after noncurative endoscopic submucosal dissection (ESD) [7, 14, 16]. However, these findings were only described in single-institution studies or studies with a relatively small number of patients.
We recently conducted a large-scale multicenter retrospective cohort study of patients who did not meet the current curative criteria for ESD in EGC and demonstrated that CSS in patients who underwent radical surgery after ESD was significantly higher in those patients than in patients who were followed up but received no additional treatment after ESD, although both CSS values were high (98.7 vs 97.5% for 5-year CSS), and the discrepancy was rather small [17]. Furthermore, to stratify these patients, we developed a seven-point risk-scoring system (the eCura system), with three risk categories based on five clinicopathological factors that predicted LNM in patients undergoing radical surgery after noncurative ESD [18]. This system was internally validated through a survival analysis performed in another set of patients who were followed up but received no additional treatment after ESD for EGC [18]. However, because this system did not directly compare the prognoses of patients with radical surgery after ESD to the prognoses of those with no additional treatment after ESD, it remains unclear whether this system contributes to the selection of patients requiring radical surgery after noncurative ESD. In this study, we hypothesized that the contribution of radical surgery after noncurative ESD to cancer-specific mortality and cancer recurrence differs among the three risk categories of the eCura system. To confirm this hypothesis, we performed a comparative study between patients with radical surgery and those with no additional treatment after noncurative ESD for EGC.
Methods
This retrospective cohort study involved patients who underwent noncurative ESD for EGC at 19 institutions in Japan; all institutions were members of the Establishment of Accommodation of Early Stomach Cancer Treatment (EAST) study group [17]. This study protocol was approved by the institutional review boards of each center before the recruitment of patients. Written informed consent was obtained from each patient before ESD. All authors had access to the study data and reviewed and approved the final version of the manuscript.
Study participants
Details regarding the study design and characteristics of the study participants have been published elsewhere [17]. Briefly, the original study population consisted of 1,969 patients from a multicenter retrospective study who did not meet the current curative criteria for ESD in EGC [17]. All the included patients, except for those who died, were followed up for ≥3 years [17]. Although the guidelines [9, 10] state that radical surgery is indicated for any patient who does not meet the current curative criteria for ESD in EGC, we had two patient groups: those who underwent radical surgery after ESD, and those who were followed up but received no additional treatment after ESD [17].
eCura system and comparison of the two patient groups
The eCura system consists of five clinicopathological factors, which are scored as follows: 1 point each for tumor size >30 mm, positive vertical margin, venous invasion, and SM2 (depth of tumor invasion into the submucosa was ≥500 µm from the muscularis mucosa), and 3 points for lymphatic invasion [18]. The total risk score, which ranged from 0 to 7 points, was then categorized as either low risk (0–1 point), intermediate risk (2–4 points), and high risk (5–7 points) [18]. In this study, the eCura system was applied to both patients with no additional treatment and those with radical surgery after ESD, and the cancer-specific mortality and cancer recurrence in each risk category were compared between the two patient groups.
Tumor histopathology was evaluated according to the Japanese classification of gastric carcinoma, third English edition [19]. In this study, lymphatic and venous invasions were examined basically using hematoxylin–eosin staining, and in cases with pathologically difficult judgement, pathologists decided to add immunohistochemical staining.
Follow-ups and definition of cancer recurrence
According to the guidelines [9], patients with radical surgery after ESD were usually followed up using annual esophagogastroduodenoscopy (EGD) and computed tomography (CT). Patients with no additional treatment underwent scheduled surveillance using EGD and CT (usually at follow-up intervals of 6–12 months) in addition to CT before follow-up. In this study, cancer recurrence was defined as radiologically or pathologically proven cancer relapse in the lymph nodes and/or other organs after a series of treatments for EGC (i.e., ESD and radical surgical resection in patients with radical surgery, and only ESD in those with no additional treatment).
Statistical analysis
The Shapiro–Wilk test was used to investigate the normal distribution of continuous variables, and non-normally distributed continuous variables are expressed here as the median with the interquartile range. The Mann–Whitney U test was used to compare the two groups. Categorical variables are expressed as number (percentage). Comparisons among categorical variables were performed using the chi-square test, or, if appropriate, Fisher’s exact test.
CSS and cancer recurrence were estimated using the Kaplan–Meier method, and the differences in CSS and cancer recurrence between patients with no additional treatment and those with radical surgery after ESD in each risk category were assessed using the log-rank test. Furthermore, Cox proportional hazards regression analysis was used to assess the performance of the scoring system for predicting cancer-specific mortality and cancer recurrence, and the hazard ratios (HRs) were calculated.
Data were analyzed using the SPSS version 23.0 for Windows software (IBM Corp., Armonk, NY, USA). A p value of < 0.05 was considered statistically significant. Data processing and statistical analyses were conducted by an independent statistician (TN).
Results
The enrolled patients comprised 905 patients with no additional treatment and 1,064 patients with radical surgery after ESD for EGC. Among the patients with no additional treatment, 549, 248, and 108 patients were assigned to the low-, intermediate-, and high-risk categories of the eCura system, respectively. Moreover, 386, 455, and 223 patients with radical surgery after ESD were assigned to the three risk categories. The detailed characteristics of patients with no additional treatment and those with radical surgery after ESD in each risk category are shown in Table 1.
Cancer-specific mortality and cancer recurrence in patients with no additional treatment and in those with radical surgery after ESD
In the low-risk category, CSS in patients with no additional treatment and in those with radical surgery after ESD was high (99.6 vs. 99.7% for 5-year CSS), but was not significantly different for the two groups (p = 0.46; Fig. 1a and Table 2). In the intermediate-risk and high-risk categories, CSS in patients with no additional treatment was significantly lower than in patients with radical surgery (p = 0.003 and p = 0.007, respectively; Fig. 1b, c). Multivariate Cox proportional hazard regression analysis revealed that in the high-risk category, cancer-specific mortality in patients with no additional treatment tended to be higher than that in patients with radical surgery {HR [95% confidence interval (CI)] = 2.66 (0.95–7.48); p = 0.063}. However, no significant differences of this kind were noted in the low- and intermediate-risk categories (Table 3).

Comparison of cancer-specific survival between patients with no additional treatment and those with radical surgery after ESD for EGC, categorized according to the risk categories of the eCura system. a Low-risk patients. b Intermediate-risk patients. c High-risk patients. In the low-risk category, cancer-specific survival in patients with no additional treatment and in those with radical surgery after ESD was high, but was not significantly different between the groups (p = 0.46), whereas cancer-specific survival in patients with no additional treatment was significantly lower than in patients with radical surgery in the intermediate-risk and high-risk categories (p = 0.003 and p = 0.007, respectively). ESD endoscopic submucosal dissection, EGC early gastric cancer
Regarding cancer recurrence, the Kaplan–Meier method and log-rank test revealed similar results for CSS (Fig. 2a–c). Multivariate Cox analysis demonstrated that in the high-risk category, cancer recurrence in patients with no additional treatment was significantly higher than in patients with radical surgery [3.13 (1.16–8.46); p = 0.024]. However, no such significant differences in cancer recurrence were noted for the low- and intermediate-risk categories (Table 3).

Comparison of cancer recurrence between patients with no additional treatment and those with radical surgery after ESD for EGC, according to the risk categories of the eCura system. a Low-risk patients. b Intermediate-risk patients. c High-risk patients. In the low-risk category, cancer recurrence did not significantly differ between patients with no additional treatment and those with radical surgery after ESD (p = 0.88), whereas cancer recurrence in patients with no additional treatment was significantly lower than that in patients with radical surgery in the intermediate-risk and high-risk categories (p < 0.001 and p = 0.002, respectively). ESD endoscopic submucosal dissection, EGC early gastric cancer
Discussion
In this comparative study between patients with no additional treatment and those with radical surgery after ESD, we clarified that the contribution of radical surgery after noncurative ESD for EGC to prognosis and cancer recurrence was different for each risk category in the eCura system.
According to the guidelines [9,10,11], radical surgery is recommended for all patients after ESD that does not meet the current curative criteria for EGC. However, no significant difference in CSS has been observed between patients with no additional treatment and those with radical surgery after ESD in any previous study [7, 14, 16]. Although our previous study revealed a statistically significant difference between the patient groups, this discrepancy was rather small [17]. We had performed the risk stratification of such patients using the eCura system [18]. In the present study, we directly compared patients with no additional treatment to those with radical surgery after ESD. Results indicated that in the low-risk category, CSS in patients with no additional treatment and in those with radical surgery after noncurative ESD for EGC was extremely high and was similar for both groups (99.6 vs 99.7% for 5-year CSS). In addition, multivariate Cox analysis revealed that there were no significant differences in cancer recurrence and cancer-specific mortality between the groups. Thus, radical surgery after noncurative ESD may lead to only a limited improvement in the prognosis among those in the low-risk category. Meanwhile, compared with surgery for EGC, ESD for EGC is reported to be associated with a better quality of life, owing to the preservation of the entire stomach and the maintenance of physiologic gastric motility [20]. Moreover, the disadvantage of radical surgery after noncurative ESD was the rate of adverse events associated with surgery and operative mortality (e.g., 2.3% for total gastrectomy in a Japanese web-based nationwide registry [21], and 10 and 4% for gastrectomy with D2 and D1 lymphadenectomy, respectively, in a Dutch trial [22]). Although stomach preservation may provoke cancer recurrence worries [23], these findings and the results of the present study support our suggestion that follow-up with no additional treatment is an acceptable option for patients in the low-risk category of the eCura system.
By contrast, in the high-risk category, cancer recurrence was significantly higher and cancer-specific mortality tended to be higher in patients with no additional treatment than in those with radical surgery. These results suggest that radical surgery after ESD is effective for improving the prognoses of patients in the high-risk category. Meanwhile, in the intermediate-risk category, multivariate Cox analysis revealed no significant differences in cancer recurrence and cancer-specific mortality between patients with no additional treatment and those with radical surgery after ESD. However, we cannot ignore the higher HR among patients with no additional treatment in this risk category (1.66 for cancer-specific mortality and 2.00 for cancer recurrence). Thus, from our data, it is difficult to conclusively determine a treatment strategy after ESD for patients in the intermediate risk category. However, these data not only aid clinical decision-making after ESD but also provide an opportunity to discuss risks with patients; this could lead to better treatment acceptance and compliance.
When follow-up with no additional treatment is selected after noncurative ESD, the follow-up schedule is an important issue. However, there are no data regarding an appropriate follow-up schedule in patients who are followed up with no additional treatment after noncurative ESD. In addition, our previous study revealed that cancer recurrence limited to regional LNM in CT could be detected in only 21.4% of patients with cancer recurrence who were followed up with no additional treatment after noncurative ESD (usually at a follow-up interval of 6–12 months), and cancer recurrence was found in distant LNM or organs in 78.6% of them [17]. Thus, the detection of cancer recurrence at a stage that is eligible for curative treatment by salvage surgery may be difficult in the majority of such patients. Clinicians should provide this information for patients when those patients desire follow-up with no additional treatment after noncurative ESD for EGC. Meanwhile, previous studies have examined CT at a follow-up interval of 6–12 months in patients with no additional treatment after noncurative ESD [4, 7, 14, 16, 24]. Although further study is needed to establish an appropriate follow-up interval in such patients, scheduled surveillance at intervals of at least 6 months by CT may be needed.
The present study has two strengths. First, we used the largest cohort of patients so far. The number of enrolled patients in the present study was more than three times that of the largest study (n = 569 patients) conducted until now [7]. Second, we compared patients with no additional treatment to those with radical surgery after ESD in each risk category of the eCura system by multivariate analysis, and we revealed the role of radical surgery after noncurative ESD for EGC.
However, this study has several limitations. First, this study employed a retrospective design, which has a potential for bias. Second, the number of cases was small, with relatively few patients in the low-risk category. Still, this study sample is the largest reported so far, with extremely high CSS and low cancer recurrence in the low-risk category, which led to a small number of cases for both treatment strategies after ESD. However, based on these results, we can conclude that follow-up with no additional treatment is an acceptable option for patients in the low-risk category. Third, this study did not include all patients with EGCs because some patients underwent surgery as the first treatment strategy, leading to selection bias. In particular, patients with undifferentiated-type EGC comprised only 14.8% of the patients included in this study, which differs from the prevalence of undifferentiated-type EGC reported in previous studies of surgery for EGC (35.9–40.4%) [3, 25, 26]. This indicates that many patients with undifferentiated-type EGC underwent surgery as the first treatment. Thus, caution in the use of this scoring system is needed for patients with undifferentiated-type EGC, and we recommend that the application of the eCura system should be limited to differentiated-type EGC. Fourth, the use of immunohistochemical staining, in addition to hematoxylin–eosin staining, for assessing lymphatic and venous invasions varied from case to case in this study. Lastly, the eCura system, which was the result of LNM analysis in patients with noncurative EGC, was established in the same cohort. Therefore, although the present study yielded significant results for a comparison of cancer recurrence and cancer-specific mortality between patients with no additional treatment and those with radical surgery after ESD for each risk category, this study is the internal validation of the eCura system.
In conclusion, we revealed that in the high-risk category of the eCura system, radical surgery after noncurative ESD for EGC is effective at reducing cancer recurrence. By contrast, in the low-risk category of the eCura system, this treatment method may lead to only a limited improvement in the prognosis because both treatment methods achieve extremely low cancer recurrence and cancer-specific mortality. These results may provide clinicians and patients with important information that can aid decision-making after noncurative ESD. However, the next step—the external validation of this system—is now warranted.
Abbreviations
- EGCs:
-
Early gastric cancers
- LNM:
-
Lymph node metastasis
- CSS:
-
Cancer-specific survival
- ESD:
-
Endoscopic submucosal dissection
- EAST:
-
Establishment of accommodation of early stomach cancer treatment
- SM2:
-
Tumor invasion into submucosa ≥500 µm from the muscularis mucosa
- EGD:
-
Esophagogastroduodenoscopy
- CT:
-
Computed tomography
- HRs:
-
Hazard ratios
- CI:
-
Confidence interval
References
Yamanouchi K, Ogata S, Sakata Y, Tsuruoka N, Shimoda R, Nakayama A, et al. Effect of additional surgery after non-curative endoscopic submucosal dissection for early gastric cancer. Endosc Int Open. 2016;4:E24–9.
Hoteya S, Iizuka T, Kikuchi D, Ogawa O, Mitani T, Matsui A, et al. Clinicopathological outcomes of patients with early gastric cancer after noncurative endoscopic submucosal dissection. Digestion. 2016;93:53–8.
Youn HG, An JY, Choi MG, Noh JH, Sohn TS, Kim S. Recurrence after curative resection of early gastric cancer. Ann Surg Oncol. 2010;17:448–54.
Kim ER, Lee H, Min BH, Lee JH, Rhee PL, Kim JJ, et al. Effect of rescue surgery after non-curative endoscopic resection of early gastric cancer. Br J Surg. 2015;102:1394–401.
Ohnita K, Isomoto H, Shikuwa S, Yajima H, Minami H, Matsushima K, et al. Early and long-term outcomes of endoscopic submucosal dissection for early gastric cancer in a large patient series. Exp Ther Med. 2014;7:594–8.
Tanabe S, Hirabayashi S, Oda I, Ono H, Nashimoto A, Isobe Y, et al. Gastric cancer treated by endoscopic submucosal dissection or endoscopic mucosal resection in Japan from 2004 through 2006: JGCA nationwide registry conducted in 2013. Gastric Cancer. 2017;. doi:10.1007/s10120-017-0699-4.
Suzuki H, Oda I, Abe S, Sekiguchi M, Nonaka S, Yoshinaga S, et al. Clinical outcomes of early gastric cancer patients after non-curative endoscopic submucosal dissection in a large consecutive patient series. Gastric Cancer. 2017;20:679–89. doi:10.1007/s10120-016-0651-z.
Sunagawa H, Kinoshita T, Kaito A, Shibasaki H, Kaneko K, Ochiai A, et al. Additional surgery for non-curative resection after endoscopic submucosal dissection for gastric cancer: a retrospective analysis of 200 cases. Surg Today. 2017;47:202–9.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017;20:1–19.
Ono H, Yao K, Fujishiro M, Oda I, Nimura S, Yahagi N, et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer. Dig Endosc. 2016;28:3–15.
Pimentel-Nunes P, Dinis-Ribeiro M, Ponchon T, Repici A, Vieth M, De Ceglie A, et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2015;47:829–54.
Ryu KW, Choi IJ, Doh YW, Kook MC, Kim CG, Park HJ, et al. Surgical indication for non-curative endoscopic resection in early gastric cancer. Ann Surg Oncol. 2007;14:3428–34.
Son SY, Park JY, Ryu KW, Eom BW, Yoon HM, Cho SJ, et al. The risk factors for lymph node metastasis in early gastric cancer patients who underwent endoscopic resection: is the minimal lymph node dissection applicable? A retrospective study. Surg Endosc. 2013;27:3247–53.
Yang HJ, Kim SG, Lim JH, Choi J, Im JP, Kim JS, et al. Predictors of lymph node metastasis in patients with non-curative endoscopic resection of early gastric cancer. Surg Endosc. 2015;29:1145–55.
Itoh H, Oohata Y, Nakamura K, Nagata T, Mibu R, Nakayama F. Complete ten-year post-gastrectomy follow-up of early gastric cancer. Am J Surg. 1989;158:14–6.
Toya Y, Endo M, Nakamura S, Akasaka R, Kosaka T, Yanai S, et al. Clinical outcomes of non-curative endoscopic submucosal dissection with negative resected margins for gastric cancer. Gastrointest Endosc. 2017;85:1218–24. doi:10.1016/j.gie.2016.11.018.
Hatta W, Gotoda T, Oyama T, Kawata N, Takahashi A, Yoshifuku Y, et al. Is radical surgery necessary in all patients who do not meet the curative criteria for endoscopic submucosal dissection in early gastric cancer? A multi-center retrospective study in Japan. J Gastroenterol. 2017;52:175–84.
Hatta W, Gotoda T, Oyama T, Kawata N, Takahashi A, Yoshifuku Y, et al. A scoring system to stratify curability after endoscopic submucosal dissection for early gastric cancer: “eCura system”. Am J Gastroenterol. 2017;112:874–81.
Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14:101–12.
Higuchi N, Nakamura K, Ihara E, Akahoshi K, Akiho H, Sumida Y, et al. Preserved gastric motility in patients with early gastric cancer after endoscopic submucosal dissection. J Gastroenterol Hepatol. 2013;28:494–8.
Kikuchi H, Miyata H, Konno H, Kamiya K, Tomotaki A, Gotoh M, et al. Development and external validation of preoperative risk models for operative morbidities after total gastrectomy using a Japanese web-based nationwide registry. Gastric Cancer. 2017;. doi:10.1007/s10120-017-0706-9.
Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010;11:439–49.
Choi JH, Kim ES, Lee YJ, Cho KB, Park KS, Jang BK, et al. Comparison of quality of life and worry of cancer recurrence between endoscopic and surgical treatment for early gastric cancer. Gastrointest Endosc. 2015;82:299–307.
Kang MS, Hong SJ, Kim DY, Han JP, Choi MH, Kim HK, et al. Long-term outcome after endoscopic submucosal dissection for early gastric cancer: focusing on a group beyond the expanded indication. J Dig Dis. 2015;16:7–13.
Sano T, Sasako M, Kinoshita T, Maruyama K. Recurrence of early gastric cancer. Follow-up of 1475 patients and review of the Japanese literature. Cancer. 1993;72:3174–8.
Ikeda Y, Saku M, Kishihara F, Maehara Y. Effective follow-up for recurrence or a second primary cancer in patients with early gastric cancer. Br J Surg. 2005;92:235–9.
Acknowledgements
We thank Hiroyuki Ono (Shizuoka Cancer Center), Koki Nakamura (Hiroshima City Hospital), Naohiko Harada (National Hospital Organization Kyushu Medical Center), Yasumasa Hara (Toyama Prefectural Central Hospital), and Ryo Shimoda (Saga Medical School) for the enrollment of patients and data collection; and we also thank Tomoyuki Koike (Tohoku University Graduate School of Medicine) for insightful comments.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Human rights statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent or a substitute for it was obtained from all patients before they were included in the study.
Rights and permissions
About this article

Cite this article
Hatta, W., Gotoda, T., Oyama, T. et al. Is the eCura system useful for selecting patients who require radical surgery after noncurative endoscopic submucosal dissection for early gastric cancer? A comparative study. Gastric Cancer 21, 481–489 (2018). https://doi.org/10.1007/s10120-017-0769-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-017-0769-7