
Abstract
Low-level laser therapy (LLLT)-induced photobiomodulation (PBM) stimulates bone tissue regeneration by inducing osteoblast differentiation and mitochondrial activation. However, the role of reactive oxygen species (ROS) in this process remains controversial. The aim of this systematic review was to collect and analyze the available literature on the cellular and molecular effects of LLLT on osteoblasts and the role of ROS in this process. A search was conducted in PubMed, ScienceDirect, Scopus, and Web of Science. Studies published in English over the past 15 years were selected. Fourteen articles were included with moderate (n = 9) and low risk of bias (n = 5). Thirteen studies reported the use of diode lasers with wavelengths (λ) between 635 and 980 nm. One study used an Nd:YAG laser (λ1064 nm). The most commonly used λ values were 808 and 635 nm. The energy densities ranged from 0.378 to 78.75 J/cm2, and irradiation times from 1.5 to 300 s. Most studies found increases in proliferation, ATP synthesis, mitochondrial activity, and osteoblastic differentiation related to moderate and dose-dependent increases in intracellular ROS levels. Only two studies reported no significant changes. The data presented heterogeneity owing to the variety of LLLT protocols. Although several studies have shown a positive role of ROS in the induction of proliferation, migration, and differentiation of different cell types, further research is required to determine the specific role of ROS in the osteoblastic cell response and the molecular mechanisms involved in triggering previously reported cellular events.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Laser therapy has been widely used in dentistry to overcome the difficulties and limitations of conventional treatments owing to its broad biomedical utility [1]. Low-level laser therapy (LLLT) has shown anti-inflammatory, analgesic, and biostimulant effects, increasing the regenerative potential of some tissues such as bone by modulating cellular metabolic processes [2]. The effects of photobiomodulation (PBM) are attributed to light absorption by the internal photoreceptors of the electron transport chain in the mitochondria, which induces intracellular mitochondrial activation leading to an increase in ATP production [3]. Studies on PBM in osteoblasts [4, 5] have shown increased mineralization, cell proliferation and migration [6], changes in the cytoskeleton, increased expression of differentiation genes such as runt-related transcription factor 2 (RUNX-2), and modulation of reactive oxygen species (ROS) production [7].
ROS play an important role in numerous cellular functions such as cell signaling, regulation of cell cycle progression, enzyme activation, and nucleic acid and protein synthesis [8]. LLLT promotes oxygen metabolism, thereby increasing ROS production [9]. However, the specific role of ROS in osteoblast PBM remains controversial. Although it has been shown that PBM induces a modest and dose-dependent increase of ROS production in normal cell lines, it seems that it could reduce ROS levels in cells previously exposed to oxidative stress [10]. However, some studies have shown that a decrease in mitochondrial stress is associated with osteoblastic differentiation [7].
In vitro studies have attempted to elucidate the role of ROS in the response of osteoblasts to PBM. However, the results obtained were heterogeneous [6, 7, 11, 12]. The biostimulatory effects of the laser depend on different parameters such as energy and power density, wavelength, output power, distance, frequency, and time of irradiation. Therefore, the heterogeneity of the effects is likely related to the variability in the irradiation parameters used [13].
Rigorously designed in vitro studies are essential as a first step in the proper setup of in vivo studies, as they bring investigators closer to establishing properly supported standards for the development of future clinical care guidelines. However, individual analyses of in vitro studies do not provide sufficient evidence to guide the development of reliable clinical protocols yet, making it necessary to provide an overview of the available scientific evidence regarding osteoblast PBM and the possible role of ROS in the induction of these effects. Therefore, this systematic review aimed to compile and analyze the literature published during the last 15 years regarding the cellular response and molecular basis of osteoblastic cells to low-level laser irradiation, as well as the role of ROS in this process.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. The guidelines were formulated according to the population, intervention, comparison, and results strategy. The following research question was raised: What is the role of ROS in the cellular response and molecular basis of osteoblastic cells to low-level laser irradiation? This review was registered in the Prospective International Registry of Systematic Reviews database (PROSPERO CRD42021246303).
Eligibility criteria
The inclusion criteria were (1) in vitro studies evaluating the effects of LLLT on osteoblast cells, (2) in vitro studies investigating the effects of LLLT on osteoblastic differentiation from stem cells, and (3) studies that reported at least one of the following parameters: cell viability, proliferation, differentiation, mitochondrial activity, and ROS production. The exclusion criteria were (1) in vitro studies reporting PBM using LEDs, (2) review articles, and (3) letters to the editor or brief comments.
Outcomes of interest
The outcomes of interest for this review were those that reported effects on osteoblasts treated with LLLT as the following: (i) cell viability, (ii) cell proliferation, (iii) ATP production, (iv) ROS production, (v) effect of photosensitizers in photodynamic therapy, and (vi) osteoblast differentiation from mesenchymal stem cells treated with LLLT.
Data sources and search strategy
To identify relevant articles, electronic/manual searches of the PubMed, Science Direct, Scopus, and Web of Science databases were performed. The algorithms that were used are listed in Table 1. Studies published in English over the past 15 years were selected. To find unpublished data, a database listing unpublished studies (OpenGray) was searched. Additionally, the authors of the included studies were contacted to obtain missing data that were considered important for the study findings.
Study appraisal and synthesis methods
To assess whether the studies met the inclusion criteria, two authors (J. G. and L. E.) reviewed the titles and abstracts of the articles. Subsequently, the abstracts were reevaluated independently by two other authors (P.B. and M.G.) to reach a consensus according to the inclusion criteria. In case of disagreements, an assessment was performed by a third reviewer (L. E.). The full texts of the articles were reviewed by two authors (J. G. and L. E.), and a consensus was reached by the four reviewers (J. G., L. E., P. B., and M. G.) for the final inclusion of the articles in the study. All disagreements were resolved by the authors. The reference lists of the selected articles were reviewed, and the full texts of potentially relevant studies were examined. A protocol for data extraction was defined, and the data related to the research questions were extracted and recorded in duplicate by two authors (J. G., L. E.) using custom-designed data extraction forms, considering the following aspects:(1) citation: study location and year of publication; (2) type of study; (3) type of intervention; (4) results; and (5) authors’ conclusions. The collected information was then categorized according to the intervention applied.
Risk of bias and quality of included studies
The methodological quality of the included studies was determined using a tool to assess the risk of bias, adapted by de Almeida et al. [14] from the methodology used by Cericato et al. [15] with some modifications. The considered parameters are listed in Table 2. A score was assigned to each study, and the studies were classified according to their quality: low quality (0–6 points), moderate quality (7–9 points), or high quality (10–12 points).
Data analysis
Common variables were identified for the collection and consolidation of data extracted from full-text articles. A descriptive summary of the variables considered was made, which included (1) type of laser, (2) application mode (pulsed or continuous), (3) wavelength, (4) power, (5) power density, (6) energy density, (7) irradiation distance, (8) irradiation time, (9) number of exposures, and (10) scattering control strategies.
Results
Search results
Of 109 potentially relevant articles identified in the database searches, 33 corresponded to duplicate records, 61 were excluded due to title and/or abstract, and 15 were obtained for full-text analysis (Fig. 1). Finally, 14 articles were included in the systematic review (Table 3).

PRISMA diagram that represents the flow of information through the phases of the systematic review
Risk of bias and quality assessment
The quality assessment of the articles is presented in Table 4. Five studies [16–20] had a low risk of bias (35.7%), and nine [7, 21–28] had a moderate risk of bias (64.3%) according to previously established parameters.
Data analysis and treatment effects
The results of the included studies are shown in Table 5. Differences in the irradiation protocols (type of laser, number of applications, power, distance, and irradiation time) showed heterogeneity in the data. Therefore, it was not possible to perform a comparative analysis among the studies and only individual analyses were performed for each study.
Description of studies and experimental models
Cells models
The most used cell model was the murine osteoblast precursor line MC3T3-E1 [16, 17, 20, 24]. Two studies used human osteoblast-like cells derived from osteosarcoma Saos-2 [7, 27] and MG63 [23]. Three studies used human osteoblasts [19, 22, 26] and one study analyzed osteoblast-like cells derived from mouse bone marrow OFCOL II [21].
To assess the effects on osteoblastic differentiation, three studies used irradiated stem cells from dental pulp (DPSCs) [25], human periodontal ligament (hPDLSCs) [28], and bone marrow stroma (BMSCs) [18].
Irradiation protocols
For the studies included in this review, diode lasers with wavelengths (λ) ranging from 635 to 980 nm were implemented. Only one study used an Nd:YAG laser (λ = 1064 nm) [27]. The most commonly used wavelengths are 808 nm [7, 17, 18, 28] and 635 nm [7, 16, 26]. One study used two lasers of different wavelengths [7]. The energy densities used in the selected studies ranged from 0.378 to 78.75 J/cm2. The reported irradiation times ranged from 1.5 to 300 s (Table 3).
Significant variations were observed in the irradiation protocol used. Some authors have included photosensitizing substances, such as methylene blue (MB) [22], 5-aminolevulinic acid (5-ALA) [16], and indocyanine green (ICG) [19]. Moreover, other substances have also been tested, such as melatonin [17] and vitamin D [28]. Additionally, some studies have reported the control of laser radiation scattering with dark sheets [18, 19, 21, 26, 28], staining among wells [22], or the use of lenses to magnify the irradiation area [22]. Likewise, great variability was reported in irradiation distances, ranging from 1 to 20 cm (Table 3).
Test methods
Eleven of the 14 articles reported the evaluation of cell viability. The most commonly used test was MTT test (3-(3,4-dimethylthiazol-2-yl)-2,5-diphenyltetrazoliumbromide) [16, 17, 19, 21–23, 26, 28].
In four studies [20–22, 27], to evaluate metabolic activity, a direct relationship was made between the results of viability tests and the behavior of mitochondrial activity and ATP production in osteoblast cells. Pires et al. [21] used a mitochondrial function assay with fluorescent staining of the mitochondria in living cells. Additionally, cell proliferation was evaluated using resazurin technique [19, 26], cell count [24, 28], immunocytochemistry, enzyme-linked immunosorbent assay (ELISA), and 5-Bromo-2-deoxyuridine [20]. To evaluate cell migration, Kunimatsu et al. [20] and Tsuka et al. [27] used cell invasion and migration assays. ROS production was evaluated in three reviewed articles [7, 16, 24]; two quantified ROS levels using the dichlorofluorescein diacetate technique [7, 24], and one detected oxidative stress using a fluorogenic probe [16].
In five studies [7, 16, 17, 20, 23], intracellular signaling pathways in osteoblasts activated by low-level laser irradiation were evaluated. Western blot analysis was performed in three studies to evaluate the activation of the pErk pathway [23], expression of Akt and its phosphorylation (p-Akt) [7], and activation of the p38 MAPK pathway [17]. Son et al. [17] used a pharmacological approach with a p38 MAPK inhibitor to confirm that the induction of differentiation and mineralization occurred through the p38 MAPK pathway. Kunimatsu et al. [20] quantified the total protein concentration using a bicinchoninic acid (BCA) assay to evaluate the concentration of proteins involved in the MAPK and ERK signaling pathways. Kushibiki et al. [16] determined the activation of the AP-1 pathway using a dual indicator, the green fluorescent protein GFP/luciferase.
To evaluate the effects of photobiomodulation on osteoblastic differentiation, five articles reported the use of reverse transcription-polymerase chain reaction to evaluate gene expression of RUNX-2 [7, 25, 28], osterix (OSX) [25], alkaline phosphatase (ALP) [7, 19, 26, 28], bone gamma-carboxyglutamate protein (BGLAP) [19, 26], collagen type I alpha 1 chain [19, 26, 28], and secreted protein acidic and cysteine-rich [28]. Amaroli et al. [18] performed Western blot analysis to detect the synthesis of RUNX-2, OSX, and transforming growth factor beta-1 proteins. Five studies [17–19, 26, 28] evaluated the enzymatic activity of ALP. The study by Cavalcanti et al, was excluded because it did not evaluate osteoblastic differentiation [29].
Regarding the evaluation of extracellular matrix m ineralization, six studies [16–19, 26, 28] detected calcium deposits using the Alizarin Red S colorimetric assay, Ballini et al. [25] used von Kossa staining, and Tani et al. [7] used fluorescence analysis of mineralized bone-like nodule structure formation. The BCA assay and methylxylene blue (MXB) staining method to measure calcium nodule formation were used by a single author [16]. Kushibiki et al. [16] performed an ELISA to quantify osteocalcin (OC) and bone morphogenetic protein 2 (BMP-2) proteins. Amaroli et al. [18] used immunostaining to detect and localize RUNX-2 and OSX proteins in cells.
Effect of laser photobiomodulation on cell response
Cell viability, proliferation, and migration
Migliario et al. showed that laser stimulation increased the proliferation of MC3T3-E1 cells at 5 J/cm2 but decreased proliferation at 50 J/cm2. This suggests that higher energy densities may have an inhibitory effect on the proliferation of this cell type. By simultaneously treating cells with N-acetylcysteine (NAC), a recognized antioxidant agent, laser-induced cell proliferation was inhibited [24].
Pires et al. [21] reported an increase in the proliferation of OFCOL II cells irradiated with a Ga-Al-As laser, which may be the result of the positive photobiomodulation effect of an 830 nm laser. As an effect related to cell proliferation, the results of two studies have suggested that laser PBM improves osteoblast cell migration [20, 27]. Tsuka et al. [27] reported that Nd:YAG laser irradiation using an energy density of 10.34 J/cm2 promoted wound closure in osteoblast cell culture compared to that in the untreated control. Similarly, Kunimatsu et al. [20] showed an increase in the confluence of wounds made in MC3T3-E1 cells irradiated with a 910 nm laser, using an energy density of 2.85 J/cm2, 10 h after scraping. Thus, cell migration tended to increase over time in the irradiated cells compared to that in the control group. In the same study, DNA synthesis was significantly increased by PBM with a near-infrared diode laser (NIR) with energy densities of 2.85, 5.7, or 17.1 J/cm2, which is related to an increase in MC3T3-E1 cell division.
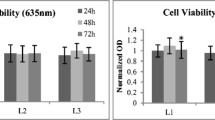
Additionally, Ates et al. [26] evaluated the effects of PBM with 635- and 809-nm diode lasers in human osteoblasts; the energy doses studied had a transitory effect on viability and proliferation; although a slight increase in cell viability (p > 0.05) was observed in all groups at 24 h, the effect was not maintained for 48 or 72 h. In another study [19], the same authors studied the effects of the application of ICG as a photosensitizer before PBM with an 808-nm diode laser. The results showed that cell viability at 24 h increased significantly when ICG was applied, and an energy density of 2 J/cm2 was used in comparison with the control group. However, the photosensitized groups treated with 1 and 2 J/cm2 for 72 h had significantly decreased viability compared with the control group [19].
Two studies reported that cell viability was not affected by photobiomodulation [7, 17]. Additionally, Xu et al. [22] observed that it was compromised only when the laser was combined with methylene blue.
Kushibiki et al. [16] evaluated the effect of 635-nm diode laser treatment on the viability of rat mesenchymal stromal cells (MSCs) and MC3T3-E1 cells. The laser applied for 0, 34, 67, or 102 s at energy densities of 0, 1, 2, or 3 J/cm2 did not induce a significant reduction in the viability of the 2 cell types evaluated after 3 days of irradiation. Huang et al. [23] determined that 920-nm diode laser treatment, using energy densities of 5 or 10 J/cm2, increased the proliferative capacity and decreased the expression of inflammatory mediators in MG63 cells infected with lipopolysaccharide.
Induction of osteoblast differentiation
Ates et al. [26] demonstrated that PBM treatment of human osteoblasts did not affect ALP production compared to that in the control group. However, a decrease in calcium deposits was observed in all experimental groups on day 14 after irradiation, except in the group treated with a 635 nm laser and an energy density of 1 J/cm2. Similarly, a significant decrease in BGLAP was observed with an energy density of 0.5 J/cm2 and, to a lesser extent, at irradiations of 1 and 2 J/cm2. The only doses that significantly increased COL1A expression were the 635 nm–2 J/cm2 and 809 nm–1 J/cm2 groups. Subsequently, Ates et al. [19] showed that laser irradiation combined with ICG induced a significant increase in ALP activity in osteoblast cells at 7 days, an activity that decreased after 14 days. In general, mineralization was lower on day 7 and higher on day 14 (p < 0.01). COLIA was upregulated in ICG-and laser-treated cells on day 14. Alike, Son et al. [17] observed that 808 nm laser irradiation of MC3T3-E1 cells combined with the application of 50 μM melatonin markedly increased OSX expression at 48 and 72 h. Similarly, when cells were treated with 50 µM melatonin and laser irradiated, ALP activity increased significantly and continued to increase until day 14. Additionally, laser PBM combined with melatonin treatment induced an increase in mineralized nodules compared with other cell cultures on day 7, which increased significantly on day 14 [17].
Kushibiki et al. showed an increase in the formation of calcium nodules and mineralization depending on the laser dose applied to MSCs and MC3T3-E1 cells. Moreover, the increase in the levels of BMP2 and other markers of osteoblastic differentiation in these cells was evident after laser treatment [16] (Table 5). Although the doses of laser-induced differentiation in both types of cells, it was slower in MSC cells than in MC3T3-E1 cells. The findings of this study showed that low doses of PBM induced differentiation in osteoblast precursor cells and primary mesenchymal cells [16]. Similar results were reported by Tani et al. [7] for Saos-2 and human mesenchymal stem cells (hMSCs) after the application of lasers and LEDs. The analysis indicated that the 635 nm laser induced an increase in the expression of osteogenic markers, such as RUNX-2 and ALP, and the formation of mineralized nodules in both cell lines. Additionally, in cells treated with an 808-nm laser, there was an increase in the formation of calcified nodules and an increase in RUNX2 expression, but not in ALP, both in osteoblasts and hMSCs [7].
Amaroli et al. [18] showed an increase in RUNX2 and OSX protein synthesis in BMSCs from day 5 after irradiation with an 808-nm diode laser (64 J/cm2). Additionally, after 10 days of treatment, there was a marked accumulation of RUNX2 and OSX in the nuclear and perinuclear regions, which correlated with their function as regulators of gene expression for bone formation. Moreover, a significant increase in ALP activity and the formation of calcium deposits was observed 15 days after laser treatment. These results showed that 808-nm diode laser irradiation promoted the differentiation of BMSCs toward the osteoblastic lineage [18].
Ballini et al. [25], using DPSCs, determined that treatment with a 980-nm diode laser at 3 J/cm2 produced an increase in ALP activity by days 5 and 10 post-irradiation and an increase in the formation of calcified nodules after 30 days of irradiation. A reduction in RUNX2 expression was observed 3 and 6 h after PBM, simultaneously with an accumulation of cells in the G2 phase of the cell cycle. However, RUNX2 and OSX expression increased 12 h and 1 week after treatment with LLLT. These results suggest that LLLT stimulates osteoblast differentiation in vitro, leading to an increase in bone formation [25].
Effects of LLLT on metabolic activity and ATP production in osteoblast cells
Xu et al. [22] demonstrated that PDT alone or combined with MB (Table 3), applied to normal human osteoblasts, did not produce immediate adverse effects on cellular metabolic activity, nor was there any induction of apoptosis 24 h after PDT. However, after this period, the mitochondrial activity of osteoblasts treated with lasers at 20 and 40 mW/cm2 combined with MB was reduced by approximately 34% and was significantly lower than that of the other treatments. Kunimatsu et al. [20] found that irradiation with a 910-nm diode laser and energy densities 2.85, 5.7, and 17.1 J/cm2 in MC3T3-E1 significantly increased ATP synthesis compared to the control group. Similar results were reported by Tsuka et al. [27], studying the effects of PBM on Saos-2 with pulsed Nd:YAG laser for 60 s at 0.3 W. Pires et al. [21] reported that in OFCOL II cells irradiated with an 830 nm laser, mitochondria perinuclear clustering formed during the first 48 h post-irradiation. After 72 h of PBM, alterations were observed in the mitochondria, which went from a filamentous to a granular appearance, and their cytoplasmic distribution was evident in comparison to the control cells [21].
Effects of LLLT on ROS production and activation of intracellular signaling pathways in osteoblast cells
Kushibiki et al. [16] observed an increase in intracellular ROS formation in MC3T3 cells, mainly at an energy density of 3 J/cm2, significantly induced AP-1-dependent transcription, as well as an increase in the activity of AP-1 components (FosB, c-Fos, c-Jun, JunD, Fra-1, Fra-2). Conversely, Migliario et al. [24] found that laser treatment at different fluences and during different times in MC3T3 induced a significant increase in ROS production depending on the dose and observed an increase in ROS with the highest energy densities (39.37 and 78.75 J/cm2). However, this effect was inhibited when cells were treated with 1 mM NAC [24]. Furthermore, Kunimatsu et al. [20] demonstrated activation of the MAPK pathway through the phosphorylation of ERK1/2 in MC3T3-E1 cells by irradiation with a diode NIR laser (Table 3). Huang et al. [23] suggested a highly proliferative state in MG63 cell cultures irradiated with a low-level laser, as well as an increase in phosphorylated ERK1/2.
Tani et al. [7] observed a slight but significant increase in ROS induced by a red laser using an energy density of 0.4 J/cm2 Saos-2. Additionally, the results showed the expression of Akt and its activated phosphorylated form, p-Akt, in cultured and irradiated cells. Son et al. [17] demonstrated that in MC3T3-E1 cells, PBM potentiated the effects of melatonin to stimulate phosphorylated MAPK p38 and ATF2, a specific target protein of MAPK p38, and phosphorylated PRKD1, compared to untreated control cells. Additionally, the authors confirmed that combined therapy (laser and melatonin) induced differentiation and mineralization through MAPK p38 activation.
Discussion
Quality of evidence, limitations, and possible biases in the review
The findings of this review correspond to the results obtained from in vitro trials. Therefore, caution should be exercised in their interpretation and when extrapolating their results to a clinical setting.
According to the bias assessment, the studies had a low or moderate risk of bias (Table 4). In general, these studies met the minimum criteria for conducting an in vitro study of cellular responses. However, more details are required in the description of the methodology used in the laser irradiation protocols. Additionally, the evaluation of the selected studies was performed by adapting a tool previously used in another review, since no guidelines have been established for the evaluation of the quality of in vitro studies, and even less so for studies on PBM.
Likewise, differences in the proposed methodologies make it difficult to compare the data obtained and standardize possible protocols that could be applied in vivo. It was also evident that there was no standardization or report of the minimum application parameters that should be mentioned in the articles.
The performance of in vitro assays is essential and represents a first step toward the standardization of various therapies, such as LLLT. However, it is necessary to consider that in vivo conditions could modify the effects of LLLT, since bone composition and structure would interact directly with laser irradiation and influence the therapy results [30].
Agreements and disagreements with other studies or reviews
Effect of LLLT on cell proliferation and differentiation
PBM plays an important role in accelerating the regeneration and repair of various tissues. A possible mechanism involved in this process is the induction of cell differentiation. LLLT can promote the production of several growth factors, osteogenic gene expression, differentiation from stem cells, and osteoblast proliferation and activity [31, 32]. The selected studies in the present review correlated increased expression of RUNX2, OSX, BGLAP, and COL1A genes; OPN and OC synthesis; and ALP activity with increased osteoblast differentiation. These effects may be due to ROS generation, which stimulates transcription through AP-1 activation [33]. This factor is involved in several cellular events including differentiation, proliferation, survival, and apoptosis [34]. This confirmed the findings of Kushibiki et al. [16], in which an increase in the expression of bone markers was observed, promoting osteoblastic differentiation.
Regarding the induction of cell proliferation and differentiation through photobiomodulation, previous studies have demonstrated the induction of cell proliferation due to activation of cytochrome C oxidase. This enzyme participates in electron transfer, which regulates mitochondrial membrane potential and enables ATP synthesis [28]. Son et al. showed that 808-nm diode laser irradiation significantly promoted the differentiation and mineralization of MC3T3-E1 cells and had an enhancing effect on melatonin when cells were irradiated in repeated doses with an energy density 1.2 J/cm2 to 3.6 J/ cm2 [17]. Amaroli et al. [18] used a laser with the same wavelength, but with an energy density of 64 J/cm2 delivered at various doses from day 0 to day 15, increasing the transcription of osteoblastic differentiation markers in bone marrow-derived cells [18]. In a study by Abdelgawad et al. [28], the use of an 808-nm diode laser and the application of vitamin D3 significantly stimulated the differentiation and proliferation of hPDLSCs and precursor cells when cell cultures were irradiated at a fluence of 2 J/cm2 [28]. Notably, the three studies mentioned above obtained significant results in promoting differentiation and proliferation, and increased mineralization in osteoblast precursor cells, even though the application parameters were different. The power density, irradiation time, and laser application distance likely influenced the results obtained despite using the same wavelength but with varying energy densities.
Regarding the use of photosensitizing substances, Son et al. [17] and Abdelgawad et al. [28] used melatonin and vitamin D3, respectively, to generate an anabolic effect on cells, obtaining satisfactory results in laser irradiation groups. Similarly, significant effects were obtained by Amaroli et al. [18] and Tani et al. [7], who used lasers with the same wavelength, but without using additional substances [7, 18]. Thus, such substances should not be considered a determining factor in the results obtained when PBM is employed to promote differentiation, proliferation, and mineralization of osteoblast precursor cells.
Regarding the wavelength used to carry out the irradiation, Tani et al. irradiated cell cultures with three different wavelengths: two 635 nm and 808 nm lasers, and 405 nm blue-violet LED, using an energy density of 0.38 J/cm2 [7]. It was concluded that the 635 nm red laser showed a more significant potential in increasing bone regeneration. However, when comparing the results obtained between the 635 nm and 808 nm lasers (even when the energy density, power density, and exposure time were the same), it is important to consider that the application distances and penetration depth were different, which may have influenced the variability of the results.
In addition to the effect of PBM on the proliferation and differentiation of various cell types, an increase in cellular migration was also found [20, 27], similar to that reported by Tschon et al. [35], who showed that PBM with a 915 nm laser promoted wound healing mainly through stimulation of cell migration and collagen deposition by osteoblasts.
Implications of ROS production
ROS are natural byproducts of oxygen metabolism and act as the final acceptor of the electron transport chain. These molecules are chemically active and play fundamental roles in cell signaling, cell cycle regulation, enzyme activation, and nucleic acid and protein synthesis [9]. Similarly, they function as activators of transcription factors, which induce the positive regulation of several stimulating and protective genes that may be related to cell proliferation, migration, and differentiation. Previous studies have shown that ROS can activate the MAPK [36, 37] and Akt pathways [38], which participate in multiple cellular processes [37–39]. Specifically, the MAPK family, including ERK1/2 and p38 MAPK, has been shown to play a role in osteoblast proliferation and differentiation, as reported in several studies included in this review [40, 41]. Similarly, the MAPK/ERK pathway has been linked to cell proliferation and migration [41]. According to this fact, the results of the present review showed that LLLT using fluences 2.85 and 10.34 J/cm2 promoted wound closure, dependent on irradiation time [20, 27]. Huang et al. [23] reported an increase in phosphorylated ERK 1/2 in MG63 cells, suggesting a state of proliferative activity. Additionally, Migliario et al. [24] demonstrated the role of ROS in cell proliferation since it was inhibited under all experimental conditions when the cells were treated with an antioxidant (NAC). Tani et al. [7] suggested that the Akt-mediated signaling pathway is involved in osteoblastic responses induced by 635 nm laser irradiation, possibly through the positive modulation of ROS levels.
ROS act as secondary messengers with signaling functions at non-cytotoxic levels in many physiological systems [42]. However, excessive ROS formation can occasionally occur, causing damage to the lipid and protein components of cells [43]. Nevertheless, depending on the laser wavelength, energy density, power, exposure time, and other factors, defense mechanisms can be activated to control excessive ROS production [44]. To date, in vitro studies have shown contradictory results regarding the effect of PBM on the ROS balance. Although PBM induces a modest dose-dependent increase in ROS production in normal cell lines, it appears that it could reduce ROS levels in cells previously exposed to oxidative stress. However, it is not yet possible to conclude whether these PBM effects are reproducible in various cell types and to what extent different wavelengths can differentially modulate ROS production [10].
Implications for practice
Considering the possible limitations of this systematic review and the heterogeneity of methodologies and reported results, the analysis showed that LLLT could increase the regenerative potential of some tissues, such as bone, by regulating cellular metabolic processes, due to its anti-inflammatory and biostimulant effects. The production of ROS and its effect on metabolic activity could constitute a central point of analysis for the foundation of the cellular effects of lasers.
Implications for future research
The results of the reviewed studies were heterogeneous, which made it difficult to conclude the appropriate protocols used to obtain more efficient results regarding cell viability, proliferation, and differentiation. The quality of the evidence was mostly moderate (64.3%) with a low bias (35.7%). Although several studies have shown a positive role of ROS in the induction of proliferation, migration, and differentiation of different cell types, further research is required to determine the specific role of ROS in the osteoblastic cell response and the molecular mechanisms involved in triggering previously reported cellular events. Additionally, more research, such as in vivo studies, is required to determine the most suitable irradiation protocols to achieve the expected effects at the cellular and tissue levels.
Conclusions
Data were limited, with heterogeneity in comparisons due to variations in LLLT protocols. The quality of the evidence was weak because the reports had a moderate risk of bias. The wavelength most commonly used for PBM of osteoblast precursor cells is 808 nm. Generally, studies have reported an increase in cell proliferation, ATP synthesis, mitochondrial activity, osteoblast differentiation, and cellular events related to the increase in intracellular ROS in LLLT-treated cells. Activation of AP-1-dependent transcription and signaling pathways, such as Akt-mediated signaling, was observed, suggesting a high proliferative state in irradiated cells. Additional research is necessary to determine the role of ROS in the osteoblast cell response to LLLT.
References
Scheinin A, Kantola S (1969) Laser-induced effects on tooth structure I. Crater Production With A CO2-Laser. Acta Odontol Scan 27(2):173–179
Spanemberg JC, Figueiredo MA, Cherubini K, Salum FG (2016) Low-level laser therapy: a review of its applications in the management of oral mucosal disorders. Altern Ther Health Med 22(6):24–31
Ahrabi B, Tavirani MR, Khoramgah MS, Noroozian M, Darabi S, Khoshsirat S et al (2019) The effect of photobiomodulation therapy on the differentiation, proliferation, and migration of the mesenchymal stem cell: a review. J Lasers Med Sci 10(Suppl 1):96
Deana AM, de Souza AM, Teixeira VP, Mesquita-Ferrari RA, Bussadori SK, Fernandes KPS (2018) The impact of photobiomodulation on osteoblast-like cell: a review. Lasers Med Sci 33(5):1147–1158
Incerti Parenti S, Tschon M, Sartori M, Visani A, Aroni E, Fini M et al (2020) Evidence from systematic reviews on photobiomodulation of human bone and stromal cells: Where do we stand? Arch Biochem Biophys 685:108333
Jawad MM, Husein A, Azlina A, Alam MK, Hassan R, Shaari R (2013) Effect of 940 nm low-level laser therapy on osteogenesis in vitro. J Biomed Opt 18(12):128001
Tani A, Chellini F, Giannelli M, Nosi D, Zecchi-Orlandini S, Sassoli C (2018) Red (635 nm), Near-Infrared (808 nm) and Violet-Blue (405 nm) Photobiomodulation potentiality on human osteoblasts and mesenchymal stromal cells: a morphological and molecular in vitro study. Int J Mol Sci 19:7–1946
Sharma P, Jha AB, Dubey RS, Pessarakli MJ (2012) Reactive oxygen species, oxidative damage, and antioxidative defense mechanism in plants under stressful conditions. J Bot 2012:1–26
Chung H, Dai T, Sharma SK, Huang Y-Y, Carroll JD, Hamblin MR (2012) The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng 40(2):516–533
Rupel K, Zupin L, Colliva A, Kamada A, Poropat A, Ottaviani G et al (2018) Photobiomodulation at multiple wavelengths differentially modulates oxidative stress in vitro and in vivo. Oxid Med Cell Longev 2018:6510159
Altan AB, Bicakci AA, Avunduk MC, Esen H (2015) The effect of dosage on the efficiency of LLLT in new bone formation at the expanded suture in rats. Lasers Med Sci 30(1):255–262
Aras MH, Bozdag Z, Demir T, Oksayan R, Yanik S, Sokucu O (2015) Effects of low-level laser therapy on changes in inflammation and in the activity of osteoblasts in the expanded premaxillary suture in an ovariectomized rat model. Photomed Laser Surg 33(3):136–144
Kalhori KAM, Vahdatinia F, Jamalpour MR, Vescovi P, Fornaini C, Merigo E et al (2019) Photobiomodulation in Oral Medicine. Photobiomodul Photomed Laser Surg 37(12):837–861
de Almeida VL, de Andrade Gois VL, Andrade RN, Cesar CP, de Albuquerque-Junior RL, de Mello RS et al (2016) Efficiency of low-level laser therapy within induced dental movement: a systematic review and meta-analysis. J Photochem Photobiol B 158:258–266
Cericato GO, Bittencourt MA, Paranhos LR (2015) Validity of the assessment method of skeletal maturation by cervical vertebrae: a systematic review and meta-analysis. Dentomaxillofacial Radiol 44(4):20140270
Kushibiki T, Tu Y, Abu-Yousif AO, Hasan T (2015) Photodynamic activation as a molecular switch to promote osteoblast cell differentiation via AP-1 activation. Sci Rep 5:13114
Son JH, Park BS, Kim IR, Sung IY, Cho YC, Kim JS et al (2017) A novel combination treatment to stimulate bone healing and regeneration under hypoxic conditions: photobiomodulation and melatonin. Lasers Med Sci 32(3):533–541
Amaroli A, Agas D, Laus F, Cuteri V, Hanna R, Sabbieti MG et al (2018) The effects of photobiomodulation of 808 nm diode laser therapy at higher fluence on the in vitro osteogenic differentiation of bone marrow stromal cells. Front Physiol 9:123
Ateş GB, Ak A, Garipcan B, Gülsoy M (2018) Indocyanine green-mediated photobiomodulation on human osteoblast cells. Lasers Med Sci 33(7):1591–1599
Kunimatsu R, Gunji H, Tsuka Y, Yoshimi Y, Awada T, Sumi K et al (2018) Effects of high-frequency near-infrared diode laser irradiation on the proliferation and migration of mouse calvarial osteoblasts. Lasers Med Sci 33(5):959–966
Pires Oliveira DAA, De Oliveira RF, Zangaro RA, Soares CP (2008) Evaluation of low-level laser therapy of osteoblastic cells. Photomed Laser Surg 26(4):401–404
Xu Y, Young MJ, Battaglino RA, Morse LR, Fontana CR, Pagonis TC et al (2009) Endodontic antimicrobial photodynamic therapy: safety assessment in mammalian cell cultures. J Endod 35(11):1567–1572
Huang TH, Lu YC, Kao CT (2012) Low-level diode laser therapy reduces lipopolysaccharide (LPS)-induced bone cell inflammation. Lasers Med Sci 27(3):621–627
Migliario M, Pittarella P, Fanuli M, Rizzi M, Renò F (2014) Laser-induced osteoblast proliferation is mediated by ROS production. Lasers Med Sci 29(4):1463–1467
Ballini A, Mastrangelo F, Gastaldi G, Tettamanti L, Bukvic N, Cantore S et al (2015) Osteogenic differentiation and gene expression of dental pulp stem cells under low-level laser irradiation: A good promise for tissue engineering. J Biol Regul Homeost Agents 29(4):813–822
Ateş GB, Can AA, Gülsoy MJ (2017) Investigation of photobiomodulation potentiality by 635 and 809 nm lasers on human osteoblasts. Lasers Med Sci 32(3):591–599
Tsuka Y, Kunimatsu R, Gunji H, Nakajima K, Kimura A, Hiraki T et al (2019) Effects of Nd:YAG low-level laser irradiation on cultured human osteoblasts migration and ATP production: in vitro study. Lasers Med Sci 34(1):55–60
Abdelgawad LM, Abdelaziz AM, Sabry D, Abdelgwad MJ (2020) Influence of photobiomodulation and vitamin D on osteoblastic differentiation of human periodontal ligament stem cells and bone-like tissue formation through enzymatic activity and gene expression. BioMol Concepts 11(1):172–181
Cavalcanti M, Maria DA, de Isla N, Leal ECP, Joensen J, Bjordal JM et al (2015) Evaluation of the proliferative effects induced by low-level laser therapy in bone marrow stem cell culture. Photomed Laser Surg 33(12):610–616
Amaroli A, Colombo E, Zekiy A, Aicardi S, Benedicenti S, De Angelis N (2020) Interaction between laser light and osteoblasts: photobiomodulation as a trend in the management of socket bone preservation—a review. Biology (Basel) 9(11):409
Fávaro-Pípi E, Ribeiro DA, Ribeiro JU, Bossini P, Oliveira P, Parizotto NA et al (2011) Low-level laser therapy induces differential expression of osteogenic genes during bone repair in rats. Photomed Laser Surg 29(5):311–317
Wu Y-h, Wang J, Gong D-x, Gu H-y, Hu S-s, Zhang HJ (2012) Effects of low-level laser irradiation on mesenchymal stem cell proliferation: a microarray analysis. Lasers Med Sci 27(2):509–519
Dhar A, Young MR, Colburn NH (2002) The role of AP-1, NF-κB and ROS/NOS in skin carcinogenesis: the JB6 model is predictive. Mol Cell Biochem 234(1):185–193
Gazon H, Barbeau B, Mesnard JM, Peloponese JM (2018) Hijacking of the AP-1 signaling pathway during development of ATL. Front Microbiol 8:2686
Tschon M, Incerti-Parenti S, Cepollaro S, Checchi L, Fini M (2015) Photobiomodulation with low-level diode laser promotes osteoblast migration in an in vitro micro wound model. J Biomed Opt 20(7):78002
Son Y, Cheong YK, Kim NH, Chung HT, Kang DG, Pae HO (2011) Mitogen-activated protein kinases and reactive oxygen species: how can ROS activate MAPK pathways? J Signal Transduct 2011:792639
Zhang J, Xing D, Gao XJ (2008) Low-power laser irradiation activates Src tyrosine kinase through reactive oxygen species-mediated signaling pathway. J Cell Physiol 217(2):518–528
Zhang L, Xing D, Gao X, Wu SJ (2009) Low-power laser irradiation promotes cell proliferation by activating PI3K/Akt pathway. J Cell Physiol 219(3):553–562
AlGhamdi KM, Kumar A, Moussa NA (2012) Low-level laser therapy: a useful technique for enhancing the proliferation of various cultured cells. Lasers Med Sci 27(1):237–249
Arakaki N, Yamashita A, Niimi S, Yamazaki TJ (2013) Involvement of reactive oxygen species in osteoblastic differentiation of MC3T3-E1 cells accompanied by mitochondrial morphological dynamics. Biomed Res 34(3):161–166
Sun Y, Liu W-Z, Liu T, Feng X, Yang N, Zhou HF (2015) Signaling pathway of MAPK/ERK in cell proliferation, differentiation, migration, senescence and apoptosis. J Recept Signal Transduct Res 35(6):600–604
Kumar Rajendran N, George BP, Chandran R, Tynga IM, Houreld N, Abrahamse H (2019) The influence of light on reactive oxygen species and NF-кB in disease progression. Antioxidants (Basel) 8(12):640
Zhang B, Xie QY, Quan Y, Pan XM, Liao DF (2015) Reactive oxygen species induce cell death via Akt signaling in rat osteoblast-like cell line ROS 17/2.8. Toxicol Ind Health 31(12):1236–1242
Jha N, Ryu JJ, Choi EH (2017) Generation and role of reactive oxygen and nitrogen species induced by plasma, lasers, chemical agents, and other systems in dentistry. Oxid Med Cell Longev 2017:7542540
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Garzón, J., Baldion, P.A., Grajales, M. et al. Response of osteoblastic cells to low-level laser treatment: a systematic review. Lasers Med Sci 37, 3031–3049 (2022). https://doi.org/10.1007/s10103-022-03587-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-022-03587-z