
Abstract
This study aimed to evaluate the effects of high-power therapeutic ultrasound in the treatment of abdominal localized adiposity in an isolated manner, with the use of neutral gel comparing ultrasonic application with 5% lipolytic active caffeine gel (phonophoresis). A total of 90 healthy women aged between 18 and 40 years were randomized and divided into two groups. The volunteers underwent anamnesis evaluation, perimetry, bioimpedance, ultrasound examination, and blood tests (complete lipidogram, creatinine, and vitamin D) before and after the end of the 10-session ultrasound protocol (3 MHz, 2 W/cm2, and 30w). Comparisons between groups and pre-post evaluation were performed by a two-way repeated-measures analysis of variance. Values of p < 0.05 indicated statistical significance. The results demonstrated a significant reduction in both groups, for the perimetry (p < 0.001) and measurements of adipose tissue thickness (p < 0.001). The examinations exhibited a significant alteration only of the complete lipidogram, but without significance (p > 0.05). When comparing the groups, no statistically significant difference was identified in any of the analyzed parameters. The high-power ultrasonic therapy is efficient in reducing localized adiposity, regardless of whether it is applied with neutral gel or 5% caffeine gel.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It has been established that the impact of adipose tissue on metabolism, as well as its distribution, is closely linked to health risk factors, with abdominal fat being one of the main problems contributing to the development of hypertension, dyslipidemia, metabolic syndrome, heart disease, and certain types of cancer [1, 2].
Overweight, which is defined as the existence of a greater amount of adipose tissue than the healthy ideal, has recently reached epidemic proportions globally and in all socioeconomic spheres, with more than one billion adults exhibiting this condition or obesity. According to the World Health Organization, this increase has been observed in all ages [3].
Localized lipodystrophy presents as an irregular subcutaneous connective tissue. In this case, adipocytes are increased in regions with tissue irregularity and a wavy appearance [4]. With the objective of reducing and attenuating localized lipodystrophy, several non-surgical and minimally invasive techniques and procedures have been developed, in an attempt to reproduce the effectiveness of liposuction [5].
Ultrasound is one of the main techniques used in lipodystrophy treatment, because it emits high-frequency sound vibrations that produce a micro-massage in the tissue, also known as cavitation, resulting in increased adipocyte cell metabolism [6]. The use of ultrasound in the treatment of localized lipodystrophy is associated with its physiological effects, among which are ion displacement, increased membrane permeability, improved reabsorption of liquids, and improvement in blood and lymphatic irrigation [7].
The use of ultrasound as a therapeutic modality began in the 1930s, being its property of heating tissues (thermal effect), considerably increasing the local metabolism, its main biological effect, mainly to accelerate the recovery of musculoskeletal lesions. Since then, therapeutic ultrasound technology has been improved, with different frequencies and various therapeutic applications ranging from uterine fibroid treatments to the permeation of active drugs and to the use for localized fat treatment, where the equipment is specific to generate microbubbles or cavitation, with positive and safe effects on adipose tissue. Faced with such a development of this resource, numerous researches have been published every year and new guidelines that support the safely clinical practice of ultrasonic therapy have been presented, indicating that this is a trend and possibly will lead to new clinical applications for ultrasound [8].
In order to improve dermatological physiotherapeutic treatments, the industry has developed high-powered ultrasonic frequencies of 3 MHz and three-pole heads, that is, with three transducers acting simultaneously, using an effective radiation area (ERA) of 15 cm2. This format allows for the treatment of larger areas within a shorter application time and enables improved distribution of the acoustic and electrical energies by the tissues, reaching the three-dimensional cells below the moving head. Another peculiarity of such equipment is that it can reach intensities of up to 3 W/cm2, generating a working power of up to 45 W that is practically quadruple the power of the previous equipment in the dermato functional area, operating at powers of 10 and 14 W [9].
Various studies have reported that ultrasound therapy for localized fat reduction is efficient when using the asset permeation property, by means of a technique known as phonophoresis, with a frequency of 3 MHz for greater absorption of subcutaneous tissue. Intensities between 0.8 and 1.0 W/cm2 are selected to achieve the thermal effect [10]. This technique uses a gel coupling medium consisting of active drugs, with caffeine being the most researched and referenced active in the literature, as it is efficient in reducing localized adiposity [11].
The main hypothesis of the study was to demonstrate that there is a higher reduction in adipose tissue in the group of patients treated with 5% caffeine gel than in the group treated with the neutral gel, since the lipolytic action of high-power ultrasound would be optimized for the active used. The null hypothesis was that there would be no significant difference between the treated groups and both would present a reduction in adipose tissue in a similar way, as the high-power therapeutic ultrasound, with the parameters used, has an excellent interaction with the treated tissue, being able to reduce the adiposity regardless of the conductive gel.
Although numerous published studies are available involving ultrasound therapy in the treatment of localized adiposity, no studies have been found that address high-power ultrasonic therapy in isolation. All of the reviewed studies exhibited a reduction of measures in areas with increased adiposity, with the use of ultrasonography in the form of phonophoresis, aimed at treatment by absorption with lipolytic actions that makes it impossible to analyze only the effect of ultrasound therapy on such pathology. In this study, the objective was to compare ultrasonic therapy isolated with phonophoresis, that is, to compare the effects of high-power ultrasound when applied with neutral conductive gel versus 5% caffeine gel, which is a highly lipolytic agent. This was carried out to verify whether there was a statistically significant difference in relation to the reduction of lipodystrophy located in 90 women aged between 18 and 40 years.
Materials and methods
A randomized, double-blind clinical trial was conducted, and because it was a study with human beings, it passed the approval of the Research Ethics Committee (CEP) of the Federal Technological University of Paraná (UTFPR) via Plataforma Brasil, Protocol No. 1956753 of March 9, 2017, in accordance with resolution 466/2012 of the National Health Council. The research volunteers also signed a document of free and informed consent. Figure 1 summarizes the procedures used in the methodology of this research work.

Flowchart of the procedures used in the methodology of this research work
Participants
A total of 90 healthy female volunteers, aged 18-40, participated in the study. After the complete evaluation, the volunteers who did not present any exclusion factor were randomly organized in the two groups of the research, labeled group A (gel batch E948) and group B (gel batch E949), as shown in Fig. 1.
The groups had batch numbering established by Buona Vita Company—CIA-BV, which collaborated with the research, taking care of the supply, organization, and randomization of the gels used in the research. As the double-blind clinical trial, the gels came with two numbers of differentiated batches, which were only revealed after the conclusion of the statistical analysis. Group A (gel batch E948) was with 5% caffeine gel, experimental group, and group B (gel batch E949) the neutral gel group, the control group. It is noteworthy that both gels had the same texture and were colorless.
Physical assessment
The patients were submitted to a physical therapy evaluation consisting of anamnesis, physical examination, perimetry, bioimpedance, and photographic records. The volunteers also underwent blood tests to verify their lipid profile (complete lipidogram), as well as urinalysis to determine renal functioning (creatinine) and also vitamin D test. Moreover, they underwent an ultrasound examination of the adipose tissue to determine its thickness. These procedures were performed before and after the treatment, in order to verify whether or not there was a decrease in abdominal localized adiposity following the proposed protocol. The blood tests were also repeated in order to observe any alteration of the lipid profile levels and renal functioning after the accomplishment of the proposed treatment protocol.
Perimetry
The perimetry was performed with an inextensible metric tape of 150 cm (ARKTUS, model 90178090, Santa Tereza do Oeste, Paraná, Brazil) and was carried out at the locations illustrated in Fig. 2a. The abdominal region was divided into four parts: belly button, 5 cm above the belly button, 10 cm above the belly button, and 5 cm below the belly button. The perimetry values were recorded by the same professional pre- and post-intervention, and data were recorded on an assessment sheet.

a Research perimetry scheme. b Regions in which ultrasound examinations were performed to measure thickness of adipose tissue: LEIF (left lateral infra-abdominal), CEIF (Central infra-abdominal), LDIF (right lateral infra-abdominal), LESP (left supra-abdominal region), CESP (supra-abdominal central), and LDSP (right supra-abdominal)
Bioimpedance
Bioimpedance was performed using the digital scale (Omron Healthcare Brasil, model HBF-214, São Paulo, SP, Brazil) that provided information regarding the weight, fat percentage, lean mass percentage, visceral mass, and basal metabolic rate of each volunteer. These data were recorded in the file of each volunteer, and measured before and after the treatment protocol.
Photographic records
The photographic records were created by a single trained examiner, in a well-lit environment, heated and with a non-reflective background. The volunteers were photographed in the orthostatic position on a marked base on the ground in the frontal, posterior plane, and profile, with arms along the body and raised, using a digital camera (Canon Power Shot SX160 IS, 16.0 megapixels, Tokyo, Japan), with a resolution of 1600 × 1500 pixels [11]. A professional tripod (Canon, model Weifeng WT6734, Canon Brazil, São Paulo, Brazil) was used to maintain the same positioning, and marks were placed on the floor for both the tripod and volunteers. The patients were instructed to wear the same clothing for the pre- and post-intervention.
Abdominal ultrasound examination
The volunteers also underwent an ultrasound examination of the adipose tissue, mainly to verify the thickness of the tissue. These imaging tests were performed using the Acuson X300 Siemens Diagnostic Ultrasound Device (Siemens Healthcare, model Acuson X300, Berlim, Germany), with a set of linear transducers, VF13-5, and the convex CH5-2 (Siemens Healthcare, model Acuson X300, Berlim, Germany), which were used to observe and measure the thickness of the adipose tissue of the research volunteers, before and after the proposed treatment protocol. The examination was performed with the patient in the supine position, and the quadrants of the abdominal region that were measured and marked with dermatographic pencil. For all volunteers, six regions with an area of 5 cm2 were examined, with three regions below the umbilical region (infra-umbilical region: left lateral infra-abdominal (LEIF), central infra-abdominal (CEIF), and right lateral infra-abdominal (LDIF)) and three regions above the umbilical line: left supra-abdominal region (LESP), supra-abdominal central (CESP), and right supra-abdominal (LDSP), as illustrated in Fig. 2b.
Laboratory blood tests
The volunteers also underwent blood tests to check their lipid profiles by means of a complete lipidogram: total cholesterol, high density lipoproteins (HDL), low-density lipoproteins (LDL), and triglycerides; renal function test (through creatinine) and also vitamin D test both were performed at the Laboratory of Clinical Analysis of Hospital São Vicente (VICENLAB). This laboratory was hired to perform clinical analysis and for blood tests, it uses standard clinical analysis protocols for biological material tests, respecting all international safety standards and those established by the Municipal Health Department of Curitiba and by the Brazilian Health Regulatory Agency (ANVISA), linked to the Brazilian Ministry of Health. Blood collection was performed after a 12-h fast, following the norms of the collection of biological materials, and this procedure occurred before and after the intervention, at no cost to the volunteers. Treatment was initiated only after blood tests and for post-treatment examination; volunteers were advised to do so immediately after the end of the proposed treatment sessions on the same day or at the latest on the day after protocol termination the research.
Intervention
Following the complete evaluation, the volunteers who did not present exclusion factors were randomized into research groups, labeled as group A (gel batch E948) and group B (gel batch E949).
The groups had batch numbering established by the company Buona Vita-CIA-BV, which collaborated with the research, overseeing the supply, organization, and randomization of the gels used in the study. Because of the double-blind clinical trial, the gels came with two numbers of differentiated lots, which were only revealed following conclusion of the statistical analysis. Group A (gel batch E948) was the gel group with 5% caffeine (experimental group), while group B (gel batch E949) was the neutral gel group (control group). It is worth noting that both gels had the same texture and were colorless, both brand Buona Vita, manufactured by Buona Vita Cosmetics—CIA-BV, Curitiba, Paraná, Brazil.
The treatment protocol consisted of 10 consultations, performed at a frequency of three times per week, where application of the high-power ultrasound, namely Ultrasound Avatar Cuatro—KLD® (KLD, Amparo, São Paulo, Brazil), was performed. The equipment was used in every abdominal region of each volunteer, respecting the application time, which varied for each patient, according to Eq. 1 [12]:
This equation takes into account the size of the treated area in relation to the ERA, which is 15 cm2 in Avatar Cuatro. The intensity applied during the service was equal for all volunteers in both groups: 2.0 W/cm2, generating a working power of 30 W in the continuous wave emission mode.
Statistical analysis
The results were described in terms of means and standard deviations (SDs). Comparisons between groups and evaluation moments (pre and post) were performed by a two-way repeated-measures analysis of variance (groups as one factor and pre- and post-evaluations as repeated measures) [13]. No significant interaction between groups and evaluation moments on the dependent variable was observed. The normality condition was assessed by the Kolmogorov-Smirnov test. Values of p < 0.05 indicated statistical significance. Data were analyzed using the IBM SPSS Statistics v.20.0 software (IBM, model IBM SPSS Statistics v.20.0, Armonk, NY: IBM Corp).
Results
Following the statistical analysis, the compositions of the conductive gels used in the research were revealed: group A with batch E948 was the gel containing 5% caffeine (experimental group) and group B with batch E949 was the neutral gel (control group). During the selection of the patients, two volunteers were excluded from the sample: one did not meet the inclusion criteria and the other gave up when discovering the frequency of the proposed treatment. Throughout the research, the experimental group lost two volunteers by withdrawal and the control group lost three: two owing to withdrawal and one because of pregnancy, as identified in the physical evaluation phase and examinations. Following statistical analysis, it was verified that both groups exhibited significant reductions against the evaluation parameters that measured the abdominal fat distribution (p < 0.05), but when analysis was conducted comparing the groups with one another, there was no statistically significant alteration in any of these parameters.
Table 1 lists the values of the abdominal perimetry, represented by the values of its mean and SD. There was a significant (p < 0.001) reduction in the measurements in both groups, but when compared with one another (experimental versus control), no significant correlation was observed (p > 0.05).
Table 2 lists the results of the measurements of adipose tissue in the abdominal region, as performed by ultrasonography. A significant reduction was evident when comparing the pre- and post-intervention results (p < 0.001), but no statistical significance was identified when comparing the two groups (experimental versus control), as opposed to in the study (p > 0.05).
The research demonstrated very similar behavior between the two groups regarding high-power ultrasonic therapy in the reduction of localized lipodystrophy. In both the perimetry variables and the measurement variables of the adipose tissue thickness through ultrasonography, both groups exhibited significant reductions in measurements in the treated area, as illustrated in Figs. 3 and 4.

Evolution of pre- and post-intervention group of perimetry values for E948 (experimental) and E949 (control) for each region evaluated. a Abdominal measurement 1 (10 cm above belly button). b Abdominal measurement 2 (5 cm above belly button). c Abdominal measurement 3 (belly button). d Abdominal measurement 4 (5 cm below belly button)

Variables of pre- and post-intervention ultrasonography examination of groups E948 (experimental) and E949 (control). The graphs above separately illustrate each region evaluated in the exam. a LEIF. b LESP. c CEIF. d CESP. e LDIF. f LDSP
Figure 5 illustrates the pre- and post-intervention ultrasonography measurements in a 31-year-old volunteer, in terms of the same pre-intervention revaluation quadrants mentioned previously. At the end of each examination session, the equipment generated six images that were subtitled according to the regions examined, and these images were saved in the equipment individually as well as in a PDF report format. The comparison of the measurements was conducted manually, by means of each report generated. The values of the measurements generated before and after the intervention were transferred to an Excel spreadsheet to perform statistical analysis at a later stage. This procedure was performed for each of the research volunteers.


Ultrasound pre- and post images in 31-year-old volunteers, with measurement D1 highlighted to evidence findings for a, b LEIF, c, d CEIF, e, f LDIF, g, h LESP, i, j CESP, k, l LDSP regions
Regarding the evaluated blood markers, no statistical significance was observed when comparing the pre- and post-intervention results within each isolated group. This was also the case when comparing the two groups with one another. Although p < 0.05 was not provided, it was observed that, within the control group (E949), a significant alteration occurred in the total lipidogram levels, and these findings are illustrated in Fig. 6.

Variables of pre- and post-laboratory examinations of groups E948 (experimental) and E949 (control). The graphs indicate the evolution of the blood markers of the research: graph A: total cholesterol values and graph B: LDL values
Discussion
Ultrasound is one of the physiotherapeutic resources that stand out the most in research on the treatment of localized adiposity, always providing satisfactory results [6, 14,15,16]. However, the substantial majority of recently published researches involve the application of ultrasound in a combined manner, that is, aimed at the permeation of lipolytics active principles (phonophoresis) for the treatment of localized adiposity [7, 10, 17].
The parameter values used in this research protocol were those indicated by the manufacturer and differed from current published studies. This is because, in this research, we used higher-intensity parameters and high-power therapeutic ultrasound, with the intention of analyzing the action of ultrasonically isolated therapy compared to phonophoresis in the improvement of localized adiposity, as well as attempting to establish an efficient protocol to treat such dysfunctions. Several published studies that have focused on the reduction of adiposity have been able to prove that a reduction in measurements occurs with the use of ultrasound in a combined manner (phonophoresis), using active principles such as 5% caffeine and tiratricol, among others [7, 10, 17]. These studies have all cited using low-power ultrasonic equipment of 10 and 14 W, always operating at low-intensity dosages.
The results of the decrease in the adipose tissue thickness of the studied samples were significant (p < 0.05), and therefore in agreement with publications that have affirmed that therapeutic ultrasound is effective in the treatment of lipodystrophy [4, 15, 18]. Clinical trials performed with rats suggested that ultrasound applications stimulate fat mobilization by means of a local increase in norepinephrine secretion under the conditions of effective frequency and intensity, thereby proving lipolysis by ultrasonic therapy [19].
It is worth mentioning that the measurements obtained by the perimetry matched those obtained by the ultrasound examination, evidencing a reduction in the treated adipose tissue and these findings are in agreement with research that used the same resources to measure subcutaneous tissue [20, 21].
It is known that cosmetology has been used extensively in aesthetics, exhibiting satisfactory results when associated with phonophoresis [10]; however, owing to the high cost involved, it is less accessible. Determining the optimal intensity and waveform for treating adipose tissue with neutral gel can reduce the costs of treatment involving ultrasonic therapy, as gels with active drugs have a high cost and generally make these treatments very expensive.
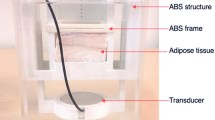
Another important factor that should be highlighted is the modification of the configurations of the ultrasound equipment destined for this area, which is currently equipped with differentiated transducers, generating up to three times more power than that widely contemplated in published studies. A hypothesis that guides this study is that by generating additional energy, this high-power equipment generates potentiated physiological responses in biological tissues, with cavitation being more responsible for modifying adipose tissue and independent of the gel. In a study carried out to evaluate the existence and the cavitation pattern with high-frequency therapeutic ultrasound and with 14 W of output power, it was proved the existence of this phenomenon detected by a synchrotron X-ray ABI [22]. Moreover, this excess energy may eventually modify and alter the composition of the active-containing gels, as the thermal effects are significantly more pronounced than those of the widely studied low-power equipment [23].
It is noteworthy that with the increasing demand of individuals with some level of overweight, the biomedical engineering industry has been developing increasingly specific ultrasound equipment to reduce adipose tissue accurately and safely. Focused therapeutic ultrasound, for example, has demonstrated good efficiency in the reduction of localized adiposity of the abdominal region, with a study demonstrating reductions of up to 25% of the treated area by means of magnetic resonance imaging, and it is also a device that works with high powers using neutral gel as the coupling medium [24].
An experimental, randomized, and controlled study was conducted with 12 albino rabbits of the same weight, and who underwent a hypercaloric diet to increase adipose tissue. A session of ultracavitation (high-potency ultrasound of the liposonic brand) was applied in the ventral region, with neutral gel, 30 W power, and continuous wave emission mode. Only the application time varied among the groups of rabbits, with group 1 being the control group (no intervention), group 2 receiving 3 min of intervention, and group 3 receiving 7 min of intervention. The results exhibited a significant reduction in the number of adipocytes measured after histological analysis of the treated tissue, while preserving the integrity of adjacent tissues [15]. In the present study, histological analysis was not conducted because it was a research involving human beings, but the findings of the ultrasound examination are in agreement with the findings of this research, demonstrating a significant reduction in the adipose tissue thickness. Moreover, as in the cited study, 30 W of power was used in the continuous mode for the treatment of volunteers, and the equipment also used 3 MHz ultrasound.
Conclusions
In this research, the treatment protocol implemented, using high-power ultrasound, exhibited a significant statistical difference in the reduction of the adipose tissue of the volunteers treated in both groups, namely the experimental group (E948 gel batch with 5% caffeine) and control group (E949 batch of neutral gel), and it was possible to verify both the perimetry and measurements of the abdominal ultrasonography as in the photographic records.
No statistical significance was observed when comparing the groups with one another, for any of the variables measured in the study. That is, both groups exhibited reduced abdominal localized adiposity, and no group indicated a superior result, which suggests that, in terms of high-power ultrasonic therapy, the gel formulation is indifferent. According to the results obtained from the research, it can be concluded that high-power therapeutic ultrasound is effective in the reduction of localized adiposity, regardless of whether it is applied with neutral gel or gel with lipolytic drugs, thereby contributing to the treatment of this important dysfunctional impact on women’s self-esteem.
References
Goodpaster BH, Krishnaswami S, Harris TB, Katsiaras A, Kritchevsky SB, Simonsick EM, Nevitt M, Holvoet P, Newman AB (2005) Obesity regional body fat distributions and the metabolic syndrome in older men and woman. Arch Intern Med 165:777–783
Lima WA, Glaner MF (2006) Main factors of risk related to the cardiovascular diseases. Rev Bras Cineantropom Desenvolvimento Humano 8:96–104
Caballero B (2007) The global epidemic of obesity: an overview. Epidemiol Rev 29:1–5
Borges F (2010) Modalidades terapêuticas nas disfunções estéticas, 2nd edn. Editora Phorte, São Paulo
Niwa A, Shono M, Mônaco P, Prado G, Osário N (2010) Experience in the use of focused ultrasound in the treatment of localized fat. Surg Cosmet Dermatol 2:323–325
Coleman KM, Coleman WP, Benchetrit A (2009) Non-invasive, external ultrasonic lipolysis. Semin Cut Med Surg 28:263–267
Pires-de-Campos MS, Leonardi GR, Chorilli M, Spadari-Bratfisch RC, Polacow ML, Grassi-Kassisse DM (2008) The effect of topical caffeine on the morphology of swine hypodermis as measured by ultrasound. J Cosmet Dermatol 7:232–237
Miller DL, Smith NB, Bailey MR, Czarnota GJ, Hynynen K, Makin IR, Bioeffects Committee of the American Institute of Ultrasound in Medicine (2012) Overview of therapeutic ultrasound applications and safety considerations. J Ultrasound Med 31:623–634
Sant'ana EMC (2010) Fundamentação teórica para terapia combinada heccus® - ultrassom e corrente aussie no tratamento da lipodistrofia ginóide e da gordura localizada. Rev Bras de Ciência & Estética 1
Hoppe S, Marin M, Simões N, Simionato G (2010) Phonophoresis in the reduction of the abdominal adiposity. Rev Bras Terap e Saúde 1:13–26
Mendonça AG, Rodrigues RD, Corradi DP, Cruz LB, Meyer PF, Antunes MJ et al (2008) Protocolo de avaliação fisioterapêutica em adiposidade localizada. Fisioterapia Brasil 2008:26–31
Hoogland R (1986) Ultrasound therapy. Holanda-delf, Enrof Nomius
Brunner E, Dumhof S, Langer F, Brunner E (2002) Nonparametric analysis of longitudinal data in factorial experiments, 1st edn. Wiley, New York
Savoia A, Forenza AM, Vannini F, Alberto F, Marino MPD, Baldi A (2010) Noninvasive body contouring by low frequency ultrasound: a clinical study. Open Recons Cosmet Surg 3:11–16
Meyer PF, Carvalho MGF, Andrade LL, Souza RN, Delgado AM et al (2012) Ultra-cavitation effect in adipose tissue of rabbits. Fisioterapia Brasil 13:106–111
Moreno-Moraga J, Valero-Altés T, Riquelme AM, Isarria-Marcosy MI, de la Torre JR (2007) Body contouring by non-invasive transdermal focused ultrasound. Lasers Surg Med 39:315–327
Polacow ML, Pires de Campos MS, Leonardi GR, Ribeiro MC, Montebello MI (2004) Effect of ultrasound on cutaneous permeation of tiratricol: histological analysis. Braz J Phys Ther 8:53–60
Guirro ECO, Guirro RRJ (2002) Fisioterapia dermato-funcional: fundamentos - recursos - patologias, 3a edn. Ed Manole, São Paulo
Miwa H, Kino M, Han LK, Takaoka K, Tsujita T, Furuhata H, Sugiyama M, Seno H, Morita Y, Kimura Y, Okuda H (2002) Effect of ultrasound application on fat mobilization. Pathophysiology 9:13
Leahy S, Toomey C, McCreesh K, O'Neill C, Jakeman P (2012) Ultrasound measurement of subcutaneous adipose tissue thickness accurately predicts total and segmental body fat of young adults. Ultrasound Med Biol 38:28–34
Wagner DR (2013) Ultrasound as tool to assess body fat. J Obes 2013:280713
Izadifar Z, Belev G, Babyn P, Chapman D (2015) Application of analyzer based X-ray imaging technique for detection of ultrasound induced cavitation bubbles from a physical therapy unit. Biomed Eng Online 14:91
Milanese C, Cavedon V, Piscitelli F, Zancanaro C (2014) Effect of low-intensity, low-frequency ultrasound treatment on anthropometry, subcutaneous adipose tissue, and body composition of young normal weight females. J Cosmet Dermatol 13:202–207
Chang SL, Huang YL, Lee MC, Chang CH, Chung WH, Wu EH, Hu S (2014) Combination therapy of focused ultrasound and radio-frequency for noninvasive body contouring in Asians with MRI photographic documentation. Lasers Med Sci 29:165–172
Funding
Financial support was received from the Brazilian Coordination for the Improvement of Higher Education Personnel (CAPES), the National Council for Scientific and Technological Development (CNPq, No. 306508/2015-0), the Brazilian Study and Project Funding Agency (FINEP, No. 2613/2009), the Araucária Foundation (No. 05/2011-10404), and the Brazilian Ministry of Health (No. 2210/2008).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was approved by the Research Ethics Committee (CEP) of the Federal University of Technology—Paraná (UTFPR) via Plataforma Brasil, Protocol No. 1956753 of March 9, 2017, in accordance with resolution 466/2012 of the National Health Council.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
da Silva Siqueira, K., Maia, J.M. High-power therapeutic ultrasound for treatment of abdominal localized adiposity—double-blind randomized clinical trial. Lasers Med Sci 35, 927–938 (2020). https://doi.org/10.1007/s10103-019-02895-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-019-02895-1