
Abstract
Diode lasers are widely used in dental laser treatment, but little is known about their thermal effects on different titanium implant surfaces. This is a key issue because already a 10 °C increase over the normal body temperature can induce bone injury and compromise osseo-integration. The present study aimed at evaluating the temperature changes and surface alterations experienced by different titanium surfaces upon irradiation with a λ = 808 nm diode laser with different settings and modalities. Titanium discs with surfaces mimicking different dental implant surfaces including TiUnite and anodized, machined surfaces were laser-irradiated in contact and non-contact mode, and with and without airflow cooling. Settings were 0.5–2.0 W for the continuous wave mode and 10–45 μJ, 20 kHz, 5–20 μs for the pulsed wave mode. The results show that the surface characteristics have a marked influence on temperature changes in response to irradiation. The TiUnite surface, corresponding to the osseous interface of dental implants, was the most susceptible to thermal rise, while the machined surfaces, corresponding to the implant collar, were less affected. In non-contact mode and upon continuous wave emission, the temperature rose above the 50 °C tissue damage threshold. Scanning electron microscopy investigation of surface alterations revealed that laser treatment in contact mode resulted in surface scratches even when no irradiation was performed. These findings indicate that the effects of diode laser irradiation on implant surfaces depend on physical features of the titanium coating and that in order to avoid thermal or physical damage to implant surface the irradiation treatment has to be carefully selected.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dental implants have opened new and often spectacular restorative treatment options for fully and partially edentulous patients; however, as the number of implants being placed continues to increase so does the number of implant-related complications. Understanding the etiology and treatment of these complications is thus essential to every clinician, especially if they perform implant placement or restorations. Peri-implantitis, one such complication that involves an inflammatory process affecting the implant-supporting bone [1, 2], can lead to implant loss if not treated or controlled. Recent studies have shown that peri-implantitis at different severity levels affects 11 to 47 % of the treated subjects 8 years after implant placement [2]. Because bacterial contamination of dental implants plays a central role in the development of peri-implantitis [3–5], several methods for decontaminating the implant surface have been developed. In particular, use of air-powered abrasive powder, citric acid, mechanical cleaning with metal and plastic curettes, or ultrasonic devices [6–8], in combination with local and systemic antibiotic, have been proposed for the treatment of peri-implantitis [9]. However, none of these methods can completely eliminate bacteria from infected implants [10, 11]. Instead, some of the currently used methods were reported to modify and even damage the implant surfaces, thus altering their osseo-conductive properties [12]. In the last decade, dental lasers commonly used in periodontics, i.e., CO2, Er:YAG, Nd:YAG, and diode lasers [13], have been reported to perform effective implant surface cleaning [14]. On the other hand, the effect of laser irradiation on the different implant surfaces is only partially understood and there are no standard decontamination protocols. In this context, a major issue is related to heating of the implant during irradiation, which can vary largely because of multiple factors including laser wavelength, instrument settings, and physical–chemical characteristics of implant surfaces. This is a key issue, as implant heating may rapidly exceed 50 °C which is commonly assumed as the tissue damage threshold [15]. Due to these many variables, inconsistent results of laser treatment of peri-implantitis are reported in the recent clinical literature [16].
The present study evaluated thermal effects and morphological alterations of different titanium discs irradiated with a diode laser (λ = 808 nm) upon different settings and operation modes. Our aim was to identify the optimal irradiation settings for the different implant surfaces in order to help design safe interventional protocols on patients with peri-implantitis.
Materials and methods
All experiments were performed on 6 mm wide and 2 mm thick titanium discs made of the material used to manufacture titanium implants (Nobel Biocare AG, Zürich, Switzerland). The base material was cold-worked titanium (Table 1) with four different surface treatments including the porous spark-anodized TiUnite surface corresponding to the osseous interface of the implants and three types of anodized, machined surfaces corresponding to different implant collar color codes. The three machined surfaces were metallic, yellow, and magenta, and are each characterized by a different color due to interference with varying thicknesses of the oxide layer (Fig. 1). All discs were ultrasonically cleaned in acetone, rinsed in distilled water, autoclaved at 120 °C for 15 min, and placed on a silicon-enriched cardboard to contain heat dispersion.

Characteristics of the four types of Ti discs used in the study. Upper panels visual appearance, lower panels scanning electron microscopy (magnification ×10,000). Thickness of the Ti oxide surface layer is also reported
The discs were irradiated with a diode GaAlAs laser emitting light at λ = 808 nm (Dental Laser System 4×4, General Project Ltd., Montespertoli, Italy) through a polyimide-coated silica-silica 600 μm optical fiber positioned perpendicular to the disc surface. For experiments in contact mode, the fiber tip was first initialized (“hot tip” technique) by activating emission over a sheet of black paper and then slid onto the disc surface during laser irradiation. In non-contact mode, the fiber tip did not undergo initialization and was kept at a distance of about 2–5 mm from the disc surface. The fiber was maintained in a fixed position or moved above the surface at a speed of 2.5 mm/s. The experiments were carried out with and without airflow cooling. The detailed laser irradiation parameters are reported in Table 2.
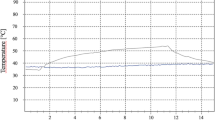
During laser irradiation, the temperature of the disc surface was monitored by a thermal camera (Ti9, Fluke Corp., Everett, USA) and a thermocouple (HGL 30 2 Channel Digital Thermometer K-type thermocouple, PeakTech, Ahrensburg, Germany). The thermal camera was locked at a 20-cm distance from the discs to avoid distance-related bias in the measurement. The discs were irradiated for 30 s and temperature was measured every 15 s until its return to the pre-irradiation values. Thermal images were processed with SmartView software (Fluke Corp.) to compose a thermal report and to extrapolate the maximum disc temperature. The Fluke Ti9 thermal camera has a −50 ± 270 °C measurement range: when the detected temperature exceeded the upper limit, the >270 °C indication appeared on the display. The temperature values obtained upon IR reading were compared with the thermocouple readings to ensure consistency of measurements. For each irradiation modality, the temperature trend was reported in a graph.
After irradiation, the discs were attached to scanning electron microscopy (SEM) stubs and sputter-coated with a 10-nm layer of platinum for SEM analysis to evaluate possible changes in the treated surfaces. Observations were performed with a Supra 40VP scanning electron microscope (Zeiss, Oberkochen, Germany).
Results
In each experiment, the maximum temperature values were reached in a very short time (1–10 s). Initially, as observed by thermography, heat was non-uniformly distributed on the disc surface, with a peak detected immediately in front of the fiber and its value being lower than that of the fiber tip. After 30 s irradiation, heat was uniformly distributed on the disc surface (Fig. 2).

Representative thermal image of TiUnite and yellow glossy discs subjected to laser irradiation in pulsed wave mode (45 μJ, 20 kHz, 7 μs), hot tip in contact mode, no airflow cooling, for 15 and 30 s
TiUnite discs
Independent of laser setup and irradiation mode, the TiUnite discs always reached the highest temperature values in comparison with the other disc types.
In contact mode irradiation with hot tip, the temperature values showed a similar trend for different laser settings, with the maximum values depending on beam power, pulse width, frequency, cooling source, and fiber movement speed (Fig. 3a). At laser switch-off, the disc temperature ranged between 200 and 50 °C, depending on the irradiation mode. Disc heating measurements with the thermocouple showed slightly lower readings than those measured by the IR thermal camera, which can possibly be attributed to the lack of a tight contact between the thermocouple probe and the TiUnite disc surface due to the disc’s marked roughness.

Diagrams showing the time course (0–180 s) of the temperature reached by TiUnite discs subjected to laser irradiation with different parameters
In non-contact mode irradiation with non-initialized tip and different laser settings, the maximum temperature values were lower than those measured in contact mode (Fig. 3b). When the fiber was maintained in a fixed position so that the laser beam irradiated the entire disc surface, the measured temperature was higher than in the protocol with the moving tip despite similar laser settings.
Treatment of the TiUnite discs with hot tip in contact mode and no airflow cooling yielded substantial heating ranging from 54 °C (continuous wave mode, 0.5 W) to 212 °C (pulsed wave mode, 45 μJ, 20 kHz, 7 μs, corresponding to 6.4 W peak power and 0.9 W average power). Among the laser settings tested, none allowed to maintain the temperature below the tissue damage threshold (50 °C). As expected, under airflow cooling, the temperature values were substantially lower and ranged from 45 (continuous wave mode, 0.5 W) to 207 °C (pulsed wave mode. 45 μJ, 20 kHz, 7 μs, peak power 6.4 W, average power 0.9 W).
In non-contact mode, the temperature also reached high values, sometimes higher than those measured in contact mode. This apparent paradox is likely due to thermodynamic phenomena on the surface. In non-contact mode and without cooling, no continuous wave mode setting allowed maintaining the temperature below 50 °C. Conversely, in pulsed wave mode, the temperature ranged from 48 (7 μJ, 20 kHz, 7 μs; peak 1 W, average 0.1 W) to 189 °C (45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). With airflow cooling, temperature lowered significantly and ranged between 42 (continuous wave, 0.5 W) and 71 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). With this modality, temperature could be easily held below the tissue damage threshold. The detailed safety parameters of laser irradiation for TiUnite discs are listed in Table 2.
Only for this particularly temperature-sensitive surface, an alternative irradiation method was evaluated. Specifically, a focalized zoom handpiece was used to laser-irradiate the whole disc surface, in non-contact mode and under air cooling, from a distance of 50 mm and with a beam diameter of 6 mm at the disc surface to completely cover the disc. This method allowed to significantly increase the laser power while maintaining low temperature. Using a 42 μJ, 20 kHz, 7 μs (6 W peak, 0.84 W average) laser settings, the measured temperature was 45 °C after 30 s. One possible explanation for this behavior could be the distance between the laser source, the disc and the lens system of the handpiece. In fact, even if the optical losses could cause lens heating, their dimensions reduce the temperature increment and the 50-mm distance from the surface further reduces the possible thermal irradiation of the target surface, which is only affected by the laser beam. Since there was no mechanical contact between the handpiece and the disc, and the resulting temperature was low, no SEM analysis was performed on this disc.
Metallic anodized, machined discs
Upon laser irradiation, metallic titanium discs showed slower and less intense heating, and faster cooling when compared to the other disc types. In contrast to the TiUnite discs, several combinations of laser beam power, pulse width and frequency settings allowed to maintain the disc temperature at low levels, even without airflow cooling.
Peak temperatures measured upon contact mode irradiation with hot tip and non-contact mode irradiation with non-initialized tip under different laser settings are shown in Fig. 4. Due to the high reflectivity of this particular surface, the IR thermal images sometimes included both the fiber tip and its reflection on the disc. During laser irradiation, the maximum temperature actually corresponded to the fiber tip because, as the fiber was slightly shifted, the temperature measurement suddenly decreased. Despite this bias, comparison of the IR measurements with the thermocouple readings showed that the two sets of values are largely in agreement. As expected, the temperatures measured with the fiber kept in a fixed position were slightly higher (+5 °C) than those detected with the moving fiber. In fact, with hot tip in contact mode and no cooling, the measured temperature ranged from 41 (continuous wave, 0.5 W) to 123 °C (pulsed wave: 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). During the tests executed in contact mode and airflow cooling, the temperature ranged from 41 (continuous wave, 0.5 W) to 69 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W).

Diagrams showing the time course (0–180 s) of the temperature reached by metallic glossy discs subjected to laser irradiation with different parameters
In non-contact mode and without cooling, almost all tested laser settings yielded low temperature increments. The measured values ranged from 38 (continuous wave, 0.5 W) to 52 °C (continuous wave, 2 W). In non-contact mode with airflow cooling, the temperature values ranged from 38 (continuous wave, 0.5 W) to 58 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). The detailed safety parameters of laser irradiation for metallic anodized, machined discs are listed in Table 2.
Yellow anodized, machined discs
Temperature measurement during laser irradiation was difficult on these discs because of a rather low IR emissivity that also appeared temperature-dependent. The values recorded by the IR thermal camera at the upper surface were very low, while those at the edge were higher and corresponded to the readings of the thermocouple. Since there is no information available regarding optical properties of the surface, the disc temperatures were deduced from the measurements on the edge. The temperature values achieved upon laser irradiation at different modes and settings were very low, especially when compared with the TiUnite discs, and did not exceed 50 °C, even in the absence of airflow cooling.
Figure 5 reports the peak temperatures measured upon contact mode irradiation with hot tip and non-contact mode irradiation with non-initiated tip with different laser settings. The measured temperatures were quite low but showed good correlation between the IR and the thermocouple readings. As previously observed for the metallic surface, the temperatures measured with the laser fiber kept in a fixed position were slightly higher than those detected with the moving fiber.

Diagrams showing the time course (0–180 s) of the temperature reached by yellow glossy discs subjected to laser irradiation with different parameters
The measurements performed with hot tip in contact mode without cooling showed temperature values ranging from 48 (pulsed wave, 10 μJ, 20 kHz, 20 μs; peak 0.5 W, average 0.2 W) to 135 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). No continuous wave settings were found suitable to hold the temperature below 50 °C. The measurements performed in contact mode with airflow cooling showed values ranging from 44 (20 μJ, 20 kHz, 11 μs; peak 1.8 W, average 0.4 W) to 88 °C (45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). In this case as well, no continuous wave settings were found to maintain the temperature below 50 °C.
In non-contact mode and no cooling, the temperature values ranged from 50 (15 μJ, 20 kHz, 10 μs; peak 1.5 W, average 0.3 W) to 78 °C (45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). No continuous wave settings were found suitable to keep the temperature below 50 °C. In non-contact mode and airflow cooling, almost all the tested laser settings yielded small temperature rise, ranging from 40 (continuous wave, 0.5 W) to 55 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). The detailed safety parameters of laser irradiation for yellow anodized, machined discs are listed in Table 2.
Magenta anodized, machined discs
The behavior of these titanium discs was intermediate between the TiUnite discs and the yellow machined disc. Under similar irradiation modes and settings, the measured temperatures were lower than those of the TiUnite discs but higher than those of the yellow ones. Thermocouple readings were generally slightly higher than those of the IR thermal camera pointing at the disc surface, but similar when the camera pointed at the disc edge. Intermediate thermal measurements between the TiUnite and the yellow discs were also obtained under airflow cooling.
Figure 6 reports the peak temperatures measured upon contact mode irradiation with hot tip and non-contact mode irradiation with non- initiated tip under different laser settings. In contact mode, the thermal image showed a central zone reaching a temperature higher than that of the remaining part of the disc, likely because of the increased IR emissivity of that zone.

Diagrams showing the time course (0–180 s) of the temperature reached by magenta glossy discs subjected to laser irradiation with different parameters
In hot tip contact mode and no cooling, no laser settings allowed to maintain the temperature below 50 °C. In fact, the measured temperature ranged from 53 (continuous wave, 0.5 W) to 163 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). In contact mode and airflow cooling, the temperature values ranged from 46 (continuous wave, 0.5 W) to 95 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W).
In non-contact mode without cooling, no laser settings allowed to maintain the temperature below 50 °C. In fact, the measured values ranged from 53 (continuous wave, 0.5 W) to 81 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). In non-contact mode with airflow cooling, the temperature values ranged between 38 (continuous wave: 0.5 W) and 58 °C (pulsed wave, 45 μJ, 20 kHz, 7 μs; peak 6.4 W, average 0.9 W). The detailed safety parameters of laser irradiation for magenta anodized, machined discs are listed in Table 2.
Morphological effects of laser irradiation on disc surfaces
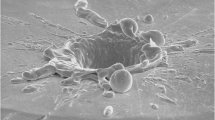
SEM examination showed that a simple dragging of the optical fiber tip over the disc surfaces, especially the TiUnite surface, even in the absence of laser emission, causes scratches of the superficial layer (Fig. 7). As expected, marked alterations of the titanium surfaces, consisting of deep grooves and microfusions, were observed upon laser irradiation in contact mode (2 W, continuous wave mode, airflow cooling; Fig. 7). By contrast, when the laser was set with the same emission parameters as above but used in a non-contact mode, the disc surfaces appeared undamaged.

Representative scanning electron micrographs of the four types of Ti discs used in the study. Upper panels the effects of dragging the fiber tip on the surface in the absence of laser emission consist in linear scratches. Lower panes deep grooves and microfusions appear upon laser irradiation in contact mode (2 W, continuous wave mode, airflow cooling). Arrows point at the edges of scratches and grooves (magnification ×10,000)
Discussion
The present findings demonstrate that the physical characteristics of the titanium surfaces lead to substantial differences in their laser energy absorption/reflection characteristics and hence susceptibility to heating and to heat-induced damage.
Diode lasers are increasingly used for the management of peri-implant diseases [14]; however, their use requires caution due to their marked thermal effects on metal targets. This caveat has recently been underscored by an in vitro study performed on titanium dental implants [17], which showed that a λ = 810 nm diode laser set at 2 W output energy in continuous wave mode generated a 10 °C temperature increase in 14 s of irradiation; on this basis, the authors concluded that pulsed wave mode and short irradiation times should be adopted for laser-aided implant surgery. The results of the present study confirm and extend this notion to encompass the possible thermal effects of diode laser on different titanium surfaces, which may be present on different implants or on different parts of the same implant. In particular, our findings clearly show that, upon similar laser irradiation parameters and modalities, the highest temperature values are reached on the TiUnite surface, corresponding to the endosseous implant portion. On the other hand, the glossy machined surface is markedly reflective, causing lesser heating and faster cooling than the TiUnite one. The present data show that the thicker the Ti oxide layer of the glossy discs (metallic < yellow < magenta), the lower the reflectivity and the higher the heating upon laser irradiation. Implant over-heating is a major issue during laser-aided surgery as it predisposes to exceed the tissue damage threshold [15] and induce severe injury of the peri-implant tissues. Moreover, high reflectivity of the glossy surfaces can raise safety concerns, because it may expose the surrounding tissues, as well as the patient and the operator, to undesired back-scattered laser radiation. On the other hand, it is evenly possible that the light scattered from the implant surface can be absorbed by chromophores of the adjacent periodontal tissues, promoting biostimulatory effects (analgesia, anti-inflammation, acceleration of gingival and bone tissue healing, etc.) which have been often reported as a major advantage of laser treatments [18].
Taken together, the present findings indicate that the TiUnite surface, owing to its peculiar micro-structure intended to optimize its osseo-conductive properties [19], is the most prone to laser-induced over-heating and damage, likely because of its physical characteristics that maximize absorption of radiation energy. On the other hand, the glossy machined discs, both natural metal and anodized yellow or magenta, show low IR emissivity, especially the yellow one, which appears to be temperature-dependent. The metal glossy machined discs also show high light reflectance, causing the IR camera to measure the temperature of the hot tip reflected onto the discs surface. All IR measurements were systematically verified with thermocouple readings to reduce possible experimental bias. Notably, the temperature measured with the thermocouple was in accordance with the values determined by the IR camera, especially at the edge of the discs. This observation, verified in different conditions and with different discs, allowed us to expedite the measurement process because we could rely on the IR thermal camera images.
As expected, maximum heating and subsequent cooling time are related to laser beam power and physical characteristics of the titanium surface. However, under pulsed wave irradiation, the discs displayed a sort of integrative capacity, yielding higher temperature values than those obtained upon continuous wave irradiation, even with a lower average output power. The cooling phase of the discs took about one minute. During this time, the disc temperature decreased uniformly to the initial values. This decay time varied with laser settings.
Of note, in non-contact mode with the same laser settings, when the fiber was held in a fixed position and the laser beam irradiated the entire disc surface, the measured temperature was higher in respect with the tests performed by moving the tip over the same surface. Likely, during fiber movement, the zones distant from the laser beam may have enough time to cool, or part of the laser beam falls outside the edge of the disc and does not contribute to total irradiation.
In most of the tested experimental conditions, the contact mode irradiation did not allow to maintain the disc temperature below the tissue damage threshold, unless the laser was equipped with an external airflow cooling device. These data underline the importance of an adequate cooling system for a safe use of laser in implant surgery.
A limitation of this study consists in the fact that the experiments were performed on new, clean discs in highly standardized laboratory conditions, which are substantially different from a real clinical situation requiring laser-aided implant surgery, in which the implant has a markedly different mass and surface geometry (e.g., threaded), is interlocked with the peri-implant tissues and can be covered by bacteria, blood, inflammatory cells, proteins and other debris. These conditions may affect the behavior of the implant upon laser irradiation. Therefore, caution is required when extrapolating the present findings to clinical practice. However, the present investigation explored multiple combinations of laser settings, irradiation modes and target titanium surfaces thus providing help to define the safest parameters to avoid thermal damage.
Conclusions
The present results suggest that the use of medical diode lasers on dental implants for the treatment of peri-implant disease requires appropriate cautions to avoid over-heating of the titanium surface and heat-induced injury of the surrounding tissues. Accordingly, preference should be granted to laser instruments that can be set in pulsed wave mode, in order to achieve high energy throughput while minimizing irradiation time, and equipped with an airflow cooling system. Particular attention should be paid when irradiating the exposed endosseous surfaces of implants, usually designed to optimize their osseo-conductive properties by means of micro-roughness, which can absorb laser energy and are prone to fast over-heating above the tissue damage threshold. Another clear notion emerging from the present findings is that laser irradiation parameters must be adjusted on a case-by-case basis. In fact, the strong dependency of laser-induced thermal effect on the physical features of the titanium surfaces clearly indicates that there is no unique, safe and effective irradiation modality suitable for all implants, but instead each implant type or even part of it requires its own appropriate laser settings and irradiation modes. To this end, the use of a feedback thermal probe, external or included in the laser device, is highly recommended.
References
American Academy of Periodontology (AAP) (2013) Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. J Periodontol 84:436–443
Koldsland OC, Scheie AA, Aass AM (2010) Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol 81:231–238
Rams PE, Link CC (1983) Microbiology of failing dental implants in humans: electron microscopic observations. J Oral Implantol 11:93–100
Belibasakis GN (2014) Microbiological and immuno-pathological aspects of peri-implant diseases. Arch Oral Biol 59:66–72
Nouneh RA, Waiaha JC, Hanes PJ, Lockwood P (2001) Effect of lipopolysaccharide contamination on the attachment of osteoblast-like cells to titanium and titanium alloy in vitro. J Oral Implantol 27:174–179
Renvert S, Samuelsson E, Lindahl C, Persson GR (2009) Mechanical non-surgical treatment of peri-implantitis: a double-blind randomized longitudinal clinical study. I: clinical results. J Clin Periodontol 36:604–609
Persson GR, Samuelsson E, Lindahl C, Renvert S (2010) Mechanical non-surgical treatment of periimplantitis: a single-blinded randomized longitudinal clinical study. II. Microbiological results. J Clin Periodontol 37:563–573
Sahm N, Becker J, Santel T, Schwarz F (2011) Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: a prospective, randomized, controlled clinical study. J Clin Periodontol 38:872–878
Salvi GE, Persson GR, Heitz-Mayfield LJ, Frei M, Lang NP (2007) Adjunctive local antibiotic therapy in the treatment of peri-implantitis. II: clinical and radiographic outcomes. Clin Oral Implants Res 18:281–285
Kontturi-Narhi V, Markkanen S, Markkanen H (1990) Effects of airpolishing on dental plaque removal and hard tissues as evaluated by scanning electron microscopy. J Periodontol 61:334–338
Drago L, Del Fabbro M, Bortolin M, Vassena C, De Vecchi E, Taschieri S (2014) Biofilm removal and antimicrobial activity of two different air-polishing powders: an in vitro study. J Periodontol 85:363–369
Figuero E, Graziani F, Sanz I, Herrera D, Sanz M (2014) Management of peri-implant mucositis and peri-implantitis. Periodontol 2000 66:255–273
Cobb CM, Low SB, Coluzzi DJ (2010) Lasers and the treatment of chronic periodontitis. Dent Clin North Am 54:35–53
Mailoa J, Lin GH, Chan HL, MacEachern M, Wang H (2014) Clinical outcomes of using lasers for peri-implantitis surface detoxification: a systematic review and meta-analysis. J Periodontol 85:1194–1202
Bornstein E (2004) Near-infrared dental diode lasers. Scientific and photobiologic principles and applications. Dentistry Today 23:102–108
Ashnagar S, Nowzari H, Nokhbatolfoghahaei H, Yaghoub Zadeh B, Chiniforush N, Choukhachi Zadeh N (2014) Laser treatment of peri-implantitis: a literature review. J Lasers Med Sci 5:153–162
Geminiani A, Caton JG, Romanos GE (2012) Temperature change during non-contact diode laser irradiation of implant surfaces. Lasers Med Sci 27:339–342
Rocci A, Rocci M, Rocci C, Scoccia A, Gargari M, Martignoni M, Gottlow J, Sennerby L (2013) Immediate loading of Brånemark system TiUnite and machined-surface implants in the posterior mandible, part II: a randomized open-ended 9-year follow-up clinical trial. Int J Oral Maxillofac Implants 28:891–895
Anders JJ, Lanzafame RJ, Arany PR (2015) Low-level light/laser therapy versus photobiomodulation therapy. Photomed Laser Surg 33:183–184
Acknowledgments
The authors are grateful to Dr. Peter Schüpbach, from Schüpbach Ltd. (Thalwil, Switzerland), for conducting the SEM investigation and to Dr. Emmanuel De Haller, Nobel Biocare Services AG, (Zürich, Switzerland), for valuable discussion on the experimental protocols.
This research was supported by a grant from General Project Ltd., Montespertoli (Florence), Italy. The authors report no conflicts of interest related to this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Giannelli, M., Lasagni, M. & Bani, D. Thermal effects of λ = 808 nm GaAlAs diode laser irradiation on different titanium surfaces. Lasers Med Sci 30, 2341–2352 (2015). https://doi.org/10.1007/s10103-015-1801-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-015-1801-y