
Abstract
The incidence of sepsis is disproportionately higher in elderly adults, and age is an independent predictor of mortality. Retrospective analysis was conducted among patients admitted to the emergency department in a tertiary teaching hospital from January 2016 to June 2017. To study the prognosis determinants of sepsis among elderly patients attended in the emergency room of a tertiary care hospital. As secondary objectives, we aimed to describe the causes of sepsis, the general outcome, and the general characteristics of these patients. Two hundred thirty-five episodes data of patients admitted throughout the 15-month study period who were diagnosed with sepsis, severe sepsis or septic shock, were included. Throughout the study cohort, 51 patients (21.7%) fulfilled the criteria of severe sepsis or septic shock. All-cause mortality was 11 patients (4.7%) on day 14 and 27 (11.5%) on day 30. Prognosis factors associated with 30-day mortality were the following: albumin level < 2.6 g/dl (first quartile of the overall population), odds ratio (OR 3.26, 95% CI 12–9.41; p = 0.029), Charlson comorbidity index (OR 1.23, 95% CI 1.04–1.45; p = 0.012), C-reactive protein on admission (OR 1.04, 95% CI 0.99–1.08; p = 0.062), and non-adequacy of the initial antimicrobial therapy (OR 3.3, 95% CI 1.06–10.4; p = 0.039). Among elderly patients with sepsis, strong predictors of mortality such as albumin could be considered as part of prognosis and future potential interventions. Adequacy of antimicrobial therapy at admission must be one of the objectives in the treatment of sepsis, also in the elderly, since it is an independent predictor of mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aging is a heterogeneous process among individuals with different physiological response. There is a functional and repair capacity impairment. Infection and the altered response of the immune system in the elderly lead to an uncommon form of severe infection or sepsis [1, 2], making sepsis a life-threatening clinical condition which involves a profound systemic response to infection and results in serious, often irreversible, damage to cells and tissues [2, 3]. However, severe infection sometimes has atypical presentation in the elderly, making its recognition difficult and worsening prognosis [4].
The incidence of sepsis is disproportionately higher in elderly adults, and age is an independent predictor of mortality. Compared with younger patients with sepsis, elderly non-survivors of sepsis died earlier during hospitalization and elderly survivors presented great disability after the process [4]. Since this form of severe infection could have strong influence in prognosis of elderly patients, we aimed to study the determinants of sepsis outcome among elderly patients attended in the emergency room of a tertiary care hospital. As secondary objectives, we aimed to describe the causes of sepsis, the general outcome, and the general characteristics of these patients.
Patients and methods
Design
A retrospective analysis was conducted among patients admitted to the emergency department (ED) of a tertiary teaching hospital in Barcelona from January 2016 to June 2017. All adult in-patients aged > 65 years old with ICD-9 codification at discharge report for sepsis or septic shock (995.9X, 038.xx, 785.52) were included.
Clinical variables
Data on demographic characteristics, comorbidities, microbiology, and severity of illness at presentation were qualified by APACHE2, the presence of systemic inflammatory response syndrome (SIRS) criteria [5] and quick-SOFA [6].
Information on the clinical and analytical presentation of infection was also collected at day 0 (when the infection was suspected). This was possible due to the standardization of the blood analysis when sepsis is suspected in our hospital.
Levels of albumin were classified as marked hypoalbuminemia (< 2.6 mg/dL), mild hypoalbuminemia (2.7–3.5 mg/dL), and normal albumin (3.5–4.5 mg/dL).
Additional information about the infection such as the etiology, initial treatment, adequacy of empirical antimicrobial therapy (considered when an active antimicrobial agent was administered at the recommended dose), intensive care unit (ICU) admission, and microbiology results were also recorded.
Pathogens were considered multidrug-resistant (MDR) if they showed acquired non-susceptibility to at least one agent in three or more antimicrobial categories/families.
As principal outcome, we studied the role of inflammatory and nutritional markers as mortalitypredictors. Other secondary outcome were the 30-day moratlity rate.
The present study was conducted in accordance with the principles stated in the Declaration of Helsinki and was approved by the local ethical committee.
Statistical analysis
Univariate analyses were performed using the chi-square test or Fisher’s exact test and the Student’s t test and Mann–Whitney U test for comparison of categorical and continuous variables, respectively.
An exploratory multivariate analysis for analyzing predictors of in-hospital death at 30-day was performed. Multivariate analyses were performed by logistic regression.
The variables introduced in the logistic regression model were albumin levels at admission, CRP, Charlson comorbidity index, severe sepsis or shock, qSOFA > 2 at admission, APACHE2 at admission, SIRS criteria at admission, inadequate empirical treatment, and infection produced by a multiresistant bacteria. Along with other variables associated with mortality in a conservative univariate analysis at a level of significance of < 0.2, variables were selected using a backward stepwise process; a p value of < 0.1 was used to delete variables in subsequent steps. Interactions between empirical treatment and MDR bacteria, SIRS and qSOFA, were also studied. All analyses were carried out using Stata 14.0 I/C software package (Stata, Houston, TX, USA).
Results
Baseline characteristics
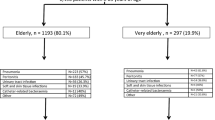
Two hundred thirty-five episodes data of patients admitted throughout the 15-month study period were included. Table 1 shows baseline characteristics. Regarding the infection acquisition sites, 169 (71.9%) community acquired infections, 36 (15.3%) were in-hospital acquired and 30 (12.8%) healthcare-related infections.
The most frequent sources of infection were urinary 126 patients (53.6%), respiratory 62 patients (26.4%), and intraabdominal 27 patients (11.5%).
Above all the microbiological tests performed, blood cultures were positive in 99 patients (44%).
The most common isolated microorganism was Escherichia coli in 100 episodes (42.6%), being 23 (23%) producers of extended spectrum beta-lactamases (ESBL) and representing 10% of total microbiological isolations. This was followed by Klebsiella pneumoniae isolates in 16 episodes (6.8%) being 4 of them (1.7% of the total) ESBL producers.
According to these results, empirical antimicrobial treatment was adequate in 196 patients (83.4%) of episodes. Non-adequate antimicrobial treatment was significantly higher in the non-survival group (14% vs 34%; p = 0.013).
All-cause mortality was in 11 patients (4.7%) on day 14 and 27 (11.5%) on day 30.
Variables associated with 30-day mortality
The results of the univariate analysis of the epidemiological, clinical, and laboratory factors associated with all-cause 30-day mortality in elderly patients with sepsis are described in Table 1.
No differences were observed in the frequency of MDR pathogens between survivors and dead patients 33 (15%) and 3 (11%), p = 0.504, respectively.
APACHE2 at admission was significantly higher in patients who died compared to those who survived (15 vs 12; p < 0.001), respectively.
After a backward stepwise variable selection, logistic regression showed that variables independently associated with 30-day mortality were the following (Table 2): albumin level < 2.6 g/dl (first quartile of the overall population), odds ratio (OR 3.26, 95% CI 12–9.41; p = 0.029), Charlson comorbidity index (OR 1.23, 95% CI 1.04–1,45; p = 0.012), PCR on admission (OR 1.04, 95% CI 0.99–1.08; p = 0.062), and non-adequacy of the initial antimicrobial therapy (OR 3.3, 95% CI 1.06–10.4; p = 0.039).
Discussion
We report that prognosis elderly patients with sepsis is determined by patients’ comorbidity, the concurrence of shock or severe sepsis, the prior nutritional status measured by serum albumin levels at admission, and importantly, the adequacy of antimicrobial therapy and the prior nutritional status measured by albumin levels at admission.
Though prior reports have described the association between hypoalbuminemia and mortality in conditions such stroke, myocardial infarction, or hip fracture [7,8,9,10,11], data available about albumin at admission and sepsis outcomes are scarce. In our series, low albumin levels on admission remained independently associated with mortality risk even when adjusting by known risk factors for increased mortality, including gender, age, smoking, alcohol, and comorbidities.
Albumin levels reflect the nutritional status, organic function, or prior physical activity of patients. However, the underlying inflammation status through increased interleukin-1 or tumor necrosis factor induces the decrease of albumin production by the liver [1, 12, 13] being co-responsible of the hypoalbuminemia seen since the early stages of sepsis.
Additionally, the hypothesis for the impact of albumin in infection prognosis is the fact that pharmacokinetics of antimicrobials could be altered by hypoalbuminemia (i.e., free plasma level antibiotics with high protein bounding could be significantly decreased due to an increased elimination) impairing antimicrobial levels in patients with low albumin. Since albumin levels on admission seem to be an important predictor of mortality in our cohort, further studies should be carried out to unveil this association.
In our series, non-adequacy of initial treatment on admission is independently associated with mortality, which has also previously reported [14]. In the same line, Leibovici et al. found decreased crude mortality rate among patients with bacteremia and septic shock when empiric treatment was adequate [15]. However, all these studies have in common that the population selected were young people with sepsis and, to our knowledge, no extensive large studies focused in elderly have been performed [14,15,16].
Noteworthy, similarly to other studies, we found a poor performance of the qSOFA score among our series. Askim et al. found that qSOFA failed to be a good-risk stratification tool to predict the 7-day and 30-day mortality [17]. Probably, qSOFA score should be used cautiously in the elderly population, at least until it will be prospectively validated.
Our study has several limitations: first, this is a retrospective design basing data on electronic chart review which have limited information, and some variables could not be controlled. Second, we did not have information regarding the baseline nutritional status of the patients, other than albumin levels. Hence, taking into account the observational design of the study, causation cannot be established.
In conclusion, the elderly population is a heterogeneous group where clinical presentation of severe infection presents a wide range of clinical pictures. Strong predictors of mortality such as albumin could be considered as part of prognosis and potential interventions. Adequacy of antimicrobial therapy at admission must be one of the objectives in the treatment of sepsis, also in the elderly, since it is an independent predictor of mortality.
References
Juneja D (2012) Severe sepsis and septic shock in the elderly: an overview. World J Crit Care Med 1(1):23
Martín S, Pérez A, Aldecoa C (2017) Sepsis and immunosenescence in the elderly patient: a review. Front Med 4(February):e1959
Capdevila JA, Diez LF, Artero A, Inglada L, Go A, Romero M et al (2018) The clinical impact of bacteremia on outcomes in elderly patients with pyelonephritis or urinary sepsis: a prospective multicenter study. PLoS One 13(1):e0191066
Martin GS, Mannino DM, Moss M (2006) The effect of age on the development and outcome of adult sepsis. Crit Care Med 34(1):15–21
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D et al (2003) 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 31(4):1250–1256
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M et al (2016) The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315(8):801–810
Famakin B, Weiss P, Hertzberg V, McClellan W, Presley R, Krompf K et al (2010) Hypoalbuminemia predicts acute stroke mortality: Paul Coverdell Georgia Stroke Registry. J Stroke Cerebrovasc Dis 19(1):17–22
Carter AM, Catto AJ, Mansfield MW, Bamford JM, Grant PJ (2007) Predictive variables for mortality after acute ischemic stroke. Stroke 38(6):1873–1880
Cho Y-M, Choi I-S, Bian R-X, Kim J-H, Han J-Y, Lee S-G (2008) Serum albumin at admission for prediction of functional outcome in ischaemic stroke patients. Neurol Sci 29(6):445–449
Plakht Y, Gilutz H, Shiyovich A (2016) Decreased admission serum albumin level is an independent predictor of long-term mortality in hospital survivors of acute myocardial infarction. Soroka Acute Myocardial Infarction II (SAMI-II) project. Int J Cardiol 219:20–24
Pioli G, Barone A, Giusti A, Oliveri M, Pizzonia M, Razzano M et al (2006) Predictors of mortality after hip fracture: results from 1-year follow-up. Aging Clin Exp Res 18(5):381–387
Churpek MM, Snyder A, Han X, Sokol S, Pettit N, Howell MD et al (2017) Quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores for detecting clinical deterioration in infected patients outside the intensive care unit. Am J Respir Crit Care Med 195(7):906–911
Akirov A, Masri-Iraqi H, Atamna A, Shimon I (2017) Low albumin levels are associated with mortality risk in hospitalized patients. Am J Med 130(12):1465.e11–1465.e19
MacArthur RD, Miller M, Albertson T, Panacek E, Johnson D, Teoh L et al (2004) Adequacy of early empiric antibiotic treatment and survival in severe sepsis: experience from the MONARCS trial. Clin Infect Dis 38(2):284–288
Leibovici L, Drucker M, Konigsberger H, Samra Z, Harrari S, Ashkenazi S et al (1997) Septic shock in bacteremic patients: risk factors, features and prognosis. Scand J Infect Dis 29(1):71–75
Behrendt G, Schneider S, Brodt HR, Just-Nübling G, Shah PM (1999) Influence of antimicrobial treatment on mortality in septicemia. J Chemother 11(3):179–186
Askim Å, Moser F, Gustad LT, Stene H, Gundersen M, Åsvold BO et al (2017) Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality - a prospective study of patients admitted with infection to the emergency department. Scand J Trauma Resusc Emerg Med 25(1):56–64
Author information
Authors and Affiliations
Contributions
IAB, RGF, SL, LS, OV, and RM designed the study. IAB and RGF collected data. RGF and IAB did the statistical analysis. RGF, IAB, SL, and LS prepared the manuscript. IAB, RGF, SL, LS, OV, and RM reviewed the manuscript. Robert Güerri-Fernández is a member of the European Society of Clinical Microbiology and Infectious Diseases—Study Group for Infections in the Elderly (ESGIE) and would like to thank ESGIE members for their stimulating support to write this article
Corresponding author
Ethics declarations
This study was submitted and approved by the IRB. No informant consent was needed.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Arnau-Barrés, I., Güerri-Fernández, R., Luque, S. et al. Serum albumin is a strong predictor of sepsis outcome in elderly patients. Eur J Clin Microbiol Infect Dis 38, 743–746 (2019). https://doi.org/10.1007/s10096-019-03478-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-019-03478-2