
Abstract
Sepsis begins outside of the hospital for nearly 80% of patients and the emergency room (ER) represents the first contact with the health care system. This study evaluates a project to improve collection of blood cultures (BCs) in patients with sepsis in the ER consisting of staff education and completion of the appropriate BC pre-analytical phase. A retrospective observational study performed to analyse the data on BC collection in the ER before and after a three-phase project. The first phase (1 January to 30 June 2015) before the intervention consisted of evaluation of data on BCs routinely collected in the ER. The second phase (1 July to 31 December 2015) was the intervention phase in which educational courses on sepsis recognition and on pre-analytical phase procedures (including direct incubation) were provided to ER staff. The third phase (1 January to 30 June 2016; after the intervention) again consisted of evaluation. Before the intervention, out of 24,738 admissions to the ER, 103 patients (0.4%) were identified as septic and had BCs drawn (359 BC bottles); 19 out of 103 patients (18.4%) had positive BCs. After the intervention, out of 24,702 admissions, 313 patients (1.3%) had BCs drawn (1,242 bottles); of these, 96 (30.7%) had positive BCs. Comparing the first and third periods, an increase in the percentage of patients with BCs collected (from 0.4% to 1.3% respectively, p < 0.0001) and an increase in the percentages of patients with true-positive BCs (from 0.08% to 0.39% of all patients evaluated respectively, p < 0.0001) were observed. The isolation of bacteria by BCs increased 3.25-fold after project implementation. These results can be principally ascribed to an improved awareness of sepsis in the staff associated with improved pre-analytical phase procedures in BC collection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sepsis begins outside of the hospital for nearly 80% of patients and the emergency room (ER) represents the first contact with the health care system for patients with sepsis [1]. A correct triage assessment in the ER is required for prompt identification and subsequent completion of the 3-h bundle of care to reach the Surviving Sepsis Campaign objectives [2]. Blood culture (BC) collection is a key part of the bundles, and is fundamental in identifying the etiological bacteria and therefore administer to the patient an appropriate antibiotic treatment [2]. BCs should be obtained before any antimicrobial therapy and following appropriate pre-analytical procedures [3]. False-negative BCs are mainly due to antibiotic pretreatment or pre-analytical phase-related issues (i.e. suboptimal sample volume, an inadequate number of BC bottles cultured and delays in time to incubation) [3].
The aim of this study is to evaluate a project to improve BC collection in patients with sepsis in the ER consisting of staff education and completion of appropriate BC pre-analytical phase procedures.
Materials and methods
Study design and setting
This study describes a prospective intervention with a retrospective data collection and analysis, performed at Fondazione IRCCS Policlinico San Matteo, Pavia as part of a broader project developed in the ER, according to Surviving Sepsis Campaign international guidelines, to improve compliance with care bundles and standardise diagnostic and therapeutic intervention for early identification and fast treatment of septic adult patients (http://www.survivingsepsis.org/SiteCollectionDocuments/SSC_Bundle.pdf) [4]. The objective of this study was to analyse the data on BC collection in the ER (absolute number, percentage of positive BCs, species of isolated bacteria, appropriateness of collection) before and after project implementation.
The Fondazione IRCCS Policlinico San Matteo is a 900-bed tertiary-care teaching hospital in Pavia, Lombardy (Northern Italy). The onsite laboratory of microbiology receives BCs from all the wards, with a total of about 35,000 blood culture bottles processed each year. The microbiology laboratory opens on weekdays from 8 am to 8 pm and on week-ends or other holidays from 8 am to 4 pm.
The local project included three phases that were implemented as follows:
-
First phase (1 January to 30 June 2015): observation phase (before the intervention). Evaluation of data on BCs routinely collected in the ER and kept at room temperature until incubation in BACTEC located in the microbiology laboratory during opening times. During this period there were no specific formal procedures for BC collection.
-
Second phase (1 July to 31 December 2015): intervention phase. Education courses were provided to ER staff (physicians and nurses) on sepsis recognition according to the local sepsis algorithm and on pre-analytical phase procedures (including direct incubation in the BACTEC FX). ER nurses oversaw the incubating BCs.
-
Third phase (1 January to 30 June 2016): evaluation of the intervention (after the intervention). During this period, BCs were incubated in the ER when the Microbiology Laboratory was closed; otherwise, they were incubated in the Microbiology Laboratory. The BC bottles incubated in the instrument placed in the ER are moved to the one in the microbiology laboratory daily. The BD EpiCenter™ software provides data management, including the transfer of data relative to bacterial growths from the two different BD BACTEC™ blood culture systems.
Local sepsis algorithm at triage
A triage nurse evaluates vital parameters and consciousness according to MEWS [5], a score system to evaluate the occurrence of any risk factors for infections (i.e. age > 70, recent surgery, neoplasia, steroid treatment, solid organ transplantation, HIV infection, chronic kidney disease, chronic hepatic disease, diabetes, central venous catheter or urinary catheter, prosthetic cardiac valve, bedridden, previous infection, long-term care facility stay, recent hospitalisation and ongoing antibiotic treatment) and the presence of at least one sign and/or symptom of infections. A patient with MEWS ≥3 at triage plus one of the risk factors and/or symptoms of infection is classified as code red and is immediately subjected to physician evaluation. The physician performs the physical examination to identify septic foci (with radiology evaluation if required), haemogas analysis, biochemical markers (including C-reactive protein, procalcitonin and complete blood count) and blood cultures. Broad-spectrum antibiotic therapy is then prescribed.
Pre-analytical phase
Blood specimens were obtained at the bedside by nursing staff from the ER. The skin was disinfected with 2% chlorhexidine. The antecubital and median cubital fossa were the preferred sampling sites using sterile gloves. An ABD vacutainer safety lock blood collection set with pre-attached holder (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) was used. Each BC set consisted of two bottles (Bactec Plus Aerobic and Bactec Plus Anaerobic). Collection of two or a maximum of three sets of BCs was considered adequate. A volume of at least 10 ml of blood was suggested from adult patients for every single specimen (globally 40–60 ml of blood required), and multiple sampling was suggested whenever possible [3, 6]. A BACTEC FX (Becton, Dickinson and Company) automated blood culture instrument system, containing 40 BC bottles, was placed in the ER and was connected to the same EpiCenter software already in use in the microbiology laboratory.
Microbiology
Positive BC bottles were subjected to Gram-staining and sub-cultures were performed onto appropriate media: aerobic sheep blood agar plates, selective agar plates, and anaerobic Schaedler agar and 5% sheep blood plates (bioMérieux SA, Marcy-l’Etoile, France). They were incubated at 37 °C overnight. The organisms were identified by matrix-assisted laser desorption ionisation time-of-flight (MALDI-TOF) software Maldi Biotyper 3.1 (Bruker Daltonics, Bremen, Germany). The isolates were tested for antimicrobial susceptibility using the Phoenix 100 (BD) automated system or the disk diffusion method susceptibility test when appropriate, according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) clinical breakpoints (version 6.0) [7].
Positive blood cultures were defined according to Weinstein [8]. Coagulase-negative staphylococci, aerobic and anaerobic diphtheroids, Micrococcus spp., Bacillus spp., and viridans streptococci were considered contaminants if only one bottle was positive. The isolate was reported as a probable contaminant and susceptibility testing was not performed.
Statistical methods
Categorical variables were described by as numbers and percentages, quantitative variables by median and interquartile range. Chi-squared test or Fisher’s exact test as appropriate were used in univariate analyses for categorical variables; t test was used for continuous variables. Number and characteristics of BCs performed in the ER during the first and third periods were analysed. Analyses were performed using STATA 14.0 (Stata Corporation, 2016, 4905 Lakeway Drive, College Station, TX, USA). All the tests were two-sided at the 5% level.
Results
The before and after intervention periods were comparable for the number of patients evaluated and the period over the year (first 6 months of each year).
Before the intervention, out of 24,738 admissions to the ER, 103 patients (0.4%) were identified as being septic and had BCs drawn (359 BC bottles). Overall, 19 out of 103 patients (18.4%) had positive BCs with clinically relevant isolates (21 bacteria isolated) and 11 out of 103 (10.7%) patients had isolates considered to be contaminants and were excluded. Polymicrobial infections were detected in 2 cases. The median time to positivity for isolates from incubation was 11 h 33 min (range: 1 h 44 min to 27 h 18 min). After the intervention, out of 24,702 admissions to ER, 313 patients with MEWS ≥3 (1.3%) were identified and had BCs drawn (1,242 bottles). Of these 96 (30.7%) had positive BCs with clinically relevant isolates (109 bacteria isolated), and 18 (5.9%) were contaminants. Polymicrobial infections was detected in 13 cases. The median time to positivity for isolates from incubation was 13 h 22 min (range: 2 h 33 min to 79 h 35 min).
The number of patients admitted to the ER in the two periods was statistically comparable and their age and gender were also not significantly different (age 67 years [49–81] and 70 [52–81], before and after the intervention respectively, p = 0.3; 59.2% and 61% were male respectively, p = 0.7).
Comparing the periods before and after the intervention, the data show that awareness of sepsis was positively improved, as demonstrated by the increase in the percentage of patients with BCs collected (from 0.4% to 1.3% of all patients evaluated in the ER in the two periods respectively, p < 0.0001) and by the increase in percentages of patients with true-positive BCs (from 0.08% to 0.39% of all patients evaluated in the ER in the two periods respectively, p < 0.0001; Table 1).
Moreover, the pre-analytical phase was improved, as a decrease in the contaminated BC bottles was observed, from 15 out of 359 (4.2%) before the intervention to 21 out of 1,242 (1.7%) after the intervention (p = 0.01), and an increase was observed in patients with an adequate number of BC bottles collected, from 72 out of 103 (69.9%) to 275 out of 313 (87.9%) (p < 0.0001); in particular, solitary BC decreased from 30 out of 103 (29.1%) to 27 out of 313 (8.6%) (p < 0.001).
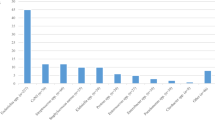
Data on the species isolated are reported in Table 2. In particular, before the intervention, 13 out of 21 (61.9%) Enterobacteriaceae (4 out of 13, 30.7% extended beta lactamase-producing bacteria [ESBL]); 2 out of 21 (9.5%) Staphylococcus aureus (1 out of 2 MRSA), were isolated.
After the intervention, 64 out of 109 (58.7%) Enterobacteriaceae (20 out of 64, 31.25% ESBL; 1 out of 64, 1.5% carbapenemase-producing), 12 out of 109 (11%) Staphylococcus aureus (2 out of 12, 16.6% MRSA), 8 out of 109 (7.3%) Streptococcus pneumoniae, 1 out of 109 (0.9%) Listeria monocytogenes, and 1 out of 109 (0.9%) Neisseria meningitidis, were isolated.
A significant number of bacteria species normally considered as fastidious bacteria, such as Streptococcus pneumoniae, Neisseria meningitidis, Streptococcus spp and bacteria that usually have slow growth curves as Pseudomonas aeruginosa grew on directly incubated bottles after the intervention, whereas they were not detected before the intervention.
Globally, throughout the whole of 2016, the number of isolates (217) and the range of bacteria were confirmed as shown in Table 2. These data further endorse the effectiveness of the project for sepsis recognition and management of the pre-analytical phase.
Discussion
The effect of an intervention to improve sepsis management in the ER, focused on education and proper BC collection and incubation, was retrospectively investigated in this study. The isolation of bacteria by BCs increased 3.25-fold after project implementation, consisting of staff education on sepsis recognition also using a score system (MEWS) and on adequate pre-analytical phase procedures in BC collection. These positive results were also consistent later in time, as the data collected throughout the whole of 2016 confirm this positive trend. An accurate collection of BCs is important as these samples represent the gold standard for identifying the pathogen(s) responsible for sepsis and allows for the implementation of an appropriate antimicrobial therapy for patients with sepsis [9]. Appropriate antibiotic treatment is in fact an independent factor predicting a positive outcome for patients with sepsis [10].
It is currently accepted that the rate of positive blood cultures is about 10–15% [3]. Using a computerised decision-support system to predict which patient will have a positive blood culture, the percentage of positive BCs varies between <3% in low-risk patients to 30% in high-risk patients with severe sepsis [11]. In our experience, roughly 30% of all BCs performed in ER turned out to be true-positive, a value in the higher range of positive BCs reported in the literature [12].
The strength of the results obtained from the described project can be principally ascribed to an improved awareness of sepsis in the staff associated with improved pre-analytical phase procedures. In the literature, different experiences are reported. An educational program consisting of training physicians and nursing staff from the emergency department, wards, and ICU in the definition, recognition and treatment of severe sepsis and septic shock improved compliance with the sepsis resuscitation bundles and improved the in-hospital sepsis-associated mortality, although only 50–60% of patients had BCs withdrawn before antibiotic treatment [13]. An intervention focused on rapid identification of patients by the triage nurse has shown a reduced time to antibiotics, but did not affect the percentage of positive blood cultures over time [14]. Other projects have been implemented on rapid BC incubation and have clearly shown benefits in terms of turnaround times of BC [9, 15].
In the present study, the training was focused both on sepsis recognition and on improving the pre-analytical phase to reduce the false-negative and false-positive results [3], in association with the rapid incubation of BCs. Major challenges in BC testing are low rates of true positivity due to antibiotic pretreatment before blood withdrawal, suboptimal sample volume, an inadequate number of BC bottles cultured and delays in time to incubation. It has been estimated that 0.3% to 15.3% of bottles containing bacteria or fungi are flagged as being negative by BC systems [3]. As sepsis begins outside the hospital in a large number of patients, collection of BC in the ER when critically ill patients are evaluated reduces the risk of false-negatives due to previous antimicrobial exposure and has been shown to reduce antibiotic overuse and costs in hospitalised patients [1]. A pre-analytical time before incubation longer than 2 h is an independent factor for false-negative results of BCs [16], as automated systems may fail to detect positive bottles entering the incubation system if microorganisms have already reached the stationary phase, or in the case of fastidious bacteria [16]. In our hospital, pre-incubation time for BCs in the ER before the implementation of the present project could vary between 1 and 18 h, in relation to laboratory opening and closing times. This situation is common in most laboratories across Europe [17]. Using incubators outside microbiology laboratories could be a relatively inexpensive intervention (less expensive than increasing opening times of the laboratories) that can be integrated into the existing procedures with relatively contained costs [15]. In our experience, the training on the correct procedures of the pre-analytical phase was also effective in reducing the number of contaminated BC bottles, which declined to less than 2%. The consequences of BC contamination and false-positive results are not insignificant, as they may lead to longer hospital stays, useless antimicrobial prescriptions and additional hospital costs [3].
Limitations of the present study include its observational retrospective nature and it being a single-centre study. It is therefore puzzling to ascribe the improvement to the intervention, although as two 6-month periods 1 year apart were compared, and the intervention phase was performed in the meantime, it seems reasonable to attribute the results to the intervention itself. A greater awareness by the staff of sepsis resulting from other forms of education (i.e. courses, conferences outside the hospital) could also have been responsible, in part, for the positive results. Another limitation of the present study is the absence of clinical data, such as data on the length of hospital stay and/or hospital-associated mortality that could have been helpful to better evaluate the effect of this intervention, as documented elsewhere [14]. The strength of these outcomes is the maintenance of the results in the months that followed.
Conclusion
As a single-centre study, these results may not be generalisable to all hospitals, a correct pre-analytical phase being fundamental to increasing the number of true-positives and reducing the rate of false-negatives. It is suggested that each hospital might apply the interventions to its own ongoing structure and organisation (mainly the positioning of a BC incubator in a place easily accessible to personnel during nights and holidays, and staff education).
References
Idrees M, Macdonald SP, Kodali K (2016) Sepsis early alert tool: early recognition and timely management in the emergency department. Emerg Med Australas 28(4):399–403. https://doi.org/10.1111/1742-6723.12581
Levy MM, Rhodes A, Phillips GS, Townsend SR, Schorr CA, Beale R, Osborn T, Lemeshow S, Chiche JD, Artigas A, Dellinger RP (2015) Surviving sepsis campaign: association between performance metrics and outcomes in a 7.5-year study. Crit Care Med 43(1):3–12. https://doi.org/10.1097/CCM.0000000000000723
Lamy B, Dargère S, Arendrup MC, Parienti JJ, Tattevin P (2016) How to optimize the use of blood cultures for the diagnosis of bloodstream infections? A state-of-the art. Front Microbiol 7:697. https://doi.org/10.3389/fmicb.2016.00697
http://intranet.sanmatteo.org/site/home/sistema-qualita/protocolli-aziendali/pdta---percorsi-diagnostico-terapeutici-assistenziali/articolo1005118.html “Percorso Diagnostico Terapeutico Assistenziale Per La Identificazione E IL Trattamento Iniziale Della Sepsi Grave E Dello Shock Settico Nell’adulto”
Vorwerk C, Loryman B, Coats TJ, Stephenson JA, Gray LD, Reddy G, Florence L, Butler N (2009) Prediction of mortality in adult emergency department patients with sepsis. Emerg Med J 26(4):254–258. https://doi.org/10.1136/emj.2007.053298
van den Bosch CM, Geerlings SE, Natsch S, Prins JM, Hulscher ME (2015) Quality indicators to measure appropriate antibiotic use in hospitalized adults. Clin Infect Dis 60(2):281–291. https://doi.org/10.1093/cid/ciu747
European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint tables for interpretation of MICs and zone diameters. Version 6.0, valid from 1 January 2016
Weinstein MP (2003) Blood culture contamination: persisting problems and partial progress. J Clin Microbiol 41(6):2275–2278
Bruins MJ, Egbers MJ, Israel TM, Diepeveen SH, Wolfhagen MJ (2017) Reduced length of hospital stay through a point of care placed automated blood culture instrument. Eur J Clin Microbiol Infect Dis 36(4):619–623. https://doi.org/10.1007/s10096-016-2837-z
Bouza E, Sousa D, Muñoz P, Rodríguez-Créixems M, Fron C, Lechuz JG (2004) Bloodstream infections: a trial of the impact of different methods of reporting positive blood culture results. Clin Infect Dis 39(8):1161–1169
Paul M, Andreassen S, Nielsen AD, Tacconelli E, Almanasreh N, Fraser A, Yahav D, Ram R, Leibovici L, TREAT Study Group (2006) Prediction of bacteremia using TREAT, a computerized decision-support system. Clin Infect Dis 42(9):1274–1282
Eliakim-Raz N, Bates DW, Leibovici L (2015) Predicting bacteraemia in validated models--a systematic review. Clin Microbiol Infect 21(4):295–301. https://doi.org/10.1016/j.cmi.2015.01.023
Ferrer R, Artigas A, Levy MM, Blanco J, González-Díaz G, Garnacho-Montero J, Ibáñez J, Palencia E, Quintana M, de la Torre-Prados MV, Edusepsis Study Group (2008) Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA 299(19):2294–2303. https://doi.org/10.1001/jama.299.19.2294
Rosenqvist M, Fagerstrand E, Lanbeck P, Melander O, Åkesson P (2017) Sepsis alert—a triage model that reduces time to antibiotics and length of hospital stay. Infect Dis (Lond) 49(7):507–513. https://doi.org/10.1080/23744235.2017.1293840
Kerremans JJ, van der Bij AK, Goessens W, Verbrugh HA, Vos MC (2009) Immediate incubation of blood cultures outside routine laboratory hours of operation accelerates antibiotic switching. J Clin Microbiol 47(11):3520–3523. https://doi.org/10.1128/JCM.01092-09
Venturelli C, Righi E, Borsari L, Aggazzotti G, Busani S, Mussini C, Rumpianesi F, Rossolini GM, Girardis M (2017) Impact of pre-analytical time on the recovery of pathogens from blood cultures: results from a large retrospective survey. PLoS One 12(1):e0169466. https://doi.org/10.1371/journal.pone.0169466
Schmitz RP, Keller PM, Baier M, Hagel S, Pletz MW, Brunkhorst FM (2013) Quality of blood culture testing—a survey in intensive care units and microbiological laboratories across four European countries. Crit Care 17(5):R248. https://doi.org/10.1186/cc13074
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest
Ethics approval
According to the local ethics review board, all patients signed at admission an informed consent for inclusion in observational studies at Fondazione IRCCS Policlinico San Matteo. The anonymity of the patients was respected and only laboratory data were used. The study was conducted under the auspices of the regional plan for sepsis management (DG Sanità Regione Lombardia, Decreto N.7517 del 5 agosto 2013; Strategie integrate per ridurre la mortalità ospedaliera associata alla sepsi grave). The study was designed and conducted in accordance with the Declaration of Helsinki.
Informed consent
None.
Additional information
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request
Rights and permissions
About this article

Cite this article
Mariani, B., Corbella, M., Seminari, E. et al. Evaluation of a model to improve collection of blood cultures in patients with sepsis in the emergency room. Eur J Clin Microbiol Infect Dis 37, 241–246 (2018). https://doi.org/10.1007/s10096-017-3122-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-017-3122-5