
Abstract
Current guidelines recommend performing echocardiography in all patients with Staphylococcus aureus bacteremia (SAB), but patients at very low risk of endocarditis may not benefit from this investigation. This study seeks to identify patients at very low risk of endocarditis. A retrospective single-center consecutive case series of patients with SAB was examined. Microbiological and echocardiographic data were used to identify patients with community onset, prolonged bacteremia, and intracardiac prosthetic devices. The diagnostic performance of these criteria for endocarditis as measured against transesophageal echocardiography (TEE) was calculated. 593 episodes of SAB were examined over a period of 6 years. 10 % were excluded from analysis due to death or discharge less than 48 h after the first positive blood culture or no admission to hospital, leaving 532 episodes for analysis. 64 % of the included episodes were investigated with echocardiography: 39 % with TEE and 26 % with transthoracic echocardiography (TTE) only. 16 % of the episodes investigated with echocardiography were demonstrated to have endocarditis. The rate of endocarditis was higher for episodes undergoing TEE (24 %) than TTE only (5 %). There were no instances of endocarditis amongst the 23 episodes investigated with TEE where none of the three risk factors were present. This group represented 57 % of the nosocomial (non-community-onset) episodes investigated with TEE. Patients with none of the three criteria examined in this study have a very low rate of endocarditis and may fall below the test threshold for echocardiography.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Current guidelines [1–3] recommend performing echocardiography in all patients with Staphylococcus aureus bacteremia (SAB) due to the risk of infective endocarditis (IE). However, as neither transesophageal echocardiography (TEE) [4, 5] nor prolonged antibiotic therapy [6] are without risk, there must exist a subset of patients with SAB in whom the risk of endocarditis is below the test threshold [7] and who do not benefit from echocardiography.
The published risk of endocarditis amongst patients with SAB ranges from 5 to 25 %, depending on the decade of publication, inclusion criteria, and echocardiography rates [8–13]. Risk factors predictive of IE amongst patients with SAB include duration of bacteremia [9, 10, 14], community acquisition [10], clinical signs of endocarditis [10], the presence of an intracardiac prosthetic device [11], dialysis dependency [14–17], metastatic infection [18–20], and an identifiable source of bacteremia [21, 22].
Two recent studies [12, 23] have suggested that it is possible to identify a subset of patients with SAB who have a very low risk of IE. Using different combinations of the above clinical criteria, the authors of these papers were able to identify subsets of patients with SAB who had a <4 % risk of endocarditis. These papers have been criticized for their low rates of TEE [13, 24] and used criteria that are difficult to apply early in the course of an episode of SAB.
We sought to identify patients with SAB who are at very low risk of endocarditis, using objective and available criteria, in a cohort with a higher rate of TEE than previous series.
Materials and methods
Patients and settings
Patients aged ≥18 years with Staphylococcus aureus isolated from blood cultures in the period 2008–2013 at an academic tertiary referral center were retrospectively identified from the hospital’s Microbiology Department database. Patients never admitted to hospital and those who died or were discharged within 48 h were excluded from the analysis.
Ethical considerations
The protocol was approved by the Melbourne Health Human Research Ethics Committee.
Data acquisition
All blood cultures (both positive and negative) collected from patients not meeting the exclusion criteria were organized into episodes of SAB. An episode commenced with the first positive blood culture and ended after a period of 14 days during which no blood cultures had been drawn.
The following data were retrospectively collected for each SAB episode: age, admission date and time, and date and time of discharge or inpatient death (all from the hospital patient management database); the date and time of each blood culture within an SAB episode, and the presence of oxacillin resistance for the first blood culture of an episode (from the Microbiology Department database). The duration of bacteremia was defined as the time of collection of the first blood culture until the time of the first negative blood culture where these data were available.
Echocardiography reports for all studies performed at our institution within 30 days of the first positive blood culture were reviewed. TEE was performed and contemporaneously reported by consultant cardiologists; transthoracic echocardiography (TTE) studies were performed by qualified echocardiographers and reported by consultant cardiologists on subsequent days. For all studies, the reporting cardiologist would have had access to the clinical information collected above (with the exception of total duration of bacteremia if ongoing) at the time of reporting. The following data were collected for each study: the date of performance, the study technique (TTE or TEE), the presence of valvular vegetations and their maximal dimension, the presence of an intracardiac prosthetic device, and the presence of paravalvular complications such as abscess or myocardial defect. Any finding labeled as endocarditis or as possibly representing endocarditis in the echocardiography report was considered as endocarditis for the purpose of data analysis. We did not seek to identify the presence of an intracardiac prosthetic device amongst patients not undergoing echocardiography.
Criteria set
We identified three previously reported risk factors for endocarditis which were unambiguous, easily available to clinicians early in the care of a patient with SAB, and objectively assessable in a retrospective manner. The three criteria analyzed were community onset (defined as the first positive blood culture occurring ≤48 h after hospital admission [25, 26]), prolonged bacteremia (defined as an interval between the first positive blood culture and the first negative blood culture greater than 72 h or any case where no negative follow-up blood culture was obtained [23, 27]), and the presence of an intracardiac prosthetic device (including valves, annular rings, congenital repairs, and rhythm management devices, but not central vascular access devices). We made no attempt to further separate community-onset SAB into the subcategories of “healthcare-associated” and “community-acquired” SAB [12, 28].
Statistical analysis
The primary statistical outcome was the diagnostic performance of the criteria set as measured against TEE findings in patients undergoing this examination. The sensitivity, specificity, positive predictive value, and negative predictive value of individual criteria, as well as the combined set for echocardiographic findings of endocarditis, are presented accompanied by modified Wald 95 % confidence intervals. This study was reported in accordance with the Standards for Reporting of Studies of Diagnostic Accuracy (STARD) [29].
Results
During the 6-year period studied, there were 593 episodes of SAB amongst 565 patients, comprising a total of 3,806 blood cultures. Of these patients, 542 had one episode of SAB, 19 had two episodes, three had three episodes, and one had four episodes. 103 episodes (17 %) were followed by inpatient death at a median of 7 days after the first positive blood culture (interquartile range, IQR, 2–15 days). Sixty-one episodes (10 %) were excluded from analysis due to death or discharge less than 48 h after the first positive blood culture or no admission to hospital, leaving 532 episodes for analysis.
The median age of the patients with analyzed SAB episodes was 64 years (IQR 48–77 years). The median number of blood cultures taken per episode was 6 (IQR 3–9). 454 episodes (85 %) included follow-up blood cultures taken more than 24 h after the initial culture. Of these, there were 432 episodes ending with a negative follow-up blood culture and 22 where a negative culture was never achieved.
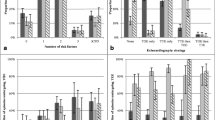
The median duration of bacteremia was 61 h (IQR 28–104 h) among the 446 episodes with a negative follow-up blood culture (i.e., where the duration of SAB was known). Figure 1 presents the duration of bacteremia for these episodes. Of these episodes, 184 (41 %) were demonstrated to be longer than 72 h. When episodes with no negative follow-up blood cultures were included (according to our definition), 269 (51 %) episodes were considered to have had prolonged bacteremia. In some episodes, the negative blood culture ending the defined period of bacteremia was taken days after the last positive blood culture, resulting in a very prolonged recorded duration of bacteremia.

Duration of Staphylococcus aureus bacteremia
317 (60 %) of the included episodes of SAB were community onset. 49 (23 %) of the 215 nosocomial episodes of SAB were due to methicillin-resistant Staphylococcus aureus, compared to 57 (18 %) of the community-onset episodes.
At least one intracardiac prosthetic device was present in 58 (17 %) of the episodes investigated by echocardiography. In total, there were 29 rhythm management devices (permanent pacemakers or implantable cardioverter defibrillators), 23 prosthetic aortic valves, 11 prosthetic mitral valves, five prosthetic tricuspid valves, and three repairs of congenital defects.
340 (64 %) of the included episodes were investigated with echocardiography: 157 (30 %) with TEE only, 136 (26 %) with TTE only, and 47 (9 %) with both techniques. 19 episodes were investigated with a second TEE, nine with a second TTE, one with a third TEE, and two with a third TTE. The last echocardiogram (which may have been the only study) was performed a median of 7 days after the first positive blood culture (IQR 4–10 days). Figure 2 shows the timing of the last echocardiogram relative to the first positive blood culture. Risk factors for endocarditis were highly prevalent amongst patients who were not investigated with TEE. 106 of 136 (78 %) episodes undergoing only TTE had one or more of the three risk factors assessed. 152 of 192 (79 %) episodes undergoing no echocardiographic assessment were either community onset or had prolonged bacteremia.

Timing of echocardiography (days after the first positive blood culture). TTE transthoracic echocardiography, TEE transesophageal echocardiography
Fifty-six (16 %) of the episodes investigated with echocardiography were demonstrated to have endocarditis. The rate of endocarditis was higher for episodes undergoing TEE (49 of 204, 24 %) than TTE only (7 of 136, 5 %). There were 24 episodes of left-sided native valve endocarditis, 13 cases of prosthetic valve endocarditis, 12 cases of isolated right-sided endocarditis, and seven cases of pacemaker-associated endocarditis. The median vegetation size was 14 mm (IQR 9–20 mm).
172 episodes were initially investigated with TTE; 160 of these studies were negative. Only 32 (20 %) of these episodes subsequently underwent TEE as suggested by current guidelines.
Table 1 presents the diagnostic performance of the risk factors for echocardiographic features of endocarditis. In the table, a true-positive represents an episode where the risk factor was present and endocarditis was demonstrated at TEE; a false-positive represents an episode where the risk factor was present but endocarditis was not. There were no instances of endocarditis amongst the 23 episodes investigated with TEE where none of the three risk factors was present. This group represented 57 % (23 of 54) of the nosocomial (non-community-onset) and 11 % (23 of 204) of all episodes of SAB investigated with TEE. In none of these episodes was echocardiography performed prior to the last positive blood culture.
When applied to all episodes undergoing echocardiography (including both TEE and TTE), the diagnostic performance of ≥1 risk factor was as follows: sensitivity 0.96 (0.87–1.00); specificity 0.18 (0.14–0.23); positive predictive value 0.19 (0.15–0.24); negative predictive value 0.96 (0.87–1.00). The diagnostic performance of the criteria did not differ significantly when episodes with unknown durations of bacteremia (i.e., no negative blood culture) were excluded, as there were only 27 such episodes investigated with echocardiography.
Discussion
We have shown that the absence of three previously reported, objective, and easily available clinical criteria identifies patients who have a very low risk of endocarditis as demonstrated by echocardiography. The use of these criteria, which are based on information collated as part of routine care, may allow the majority of nosocomial cases of SAB to be managed without echocardiography.
As noted above, the current guidelines recommend echocardiography for all patients with SAB on the basis that some of these patients will have endocarditis, and that TEE is highly sensitive for the condition. However, using the method of Pauker and Kassirer [7], it can be seen that the test threshold (the likelihood of disease below which testing is not of benefit) for any investigation cannot be zero unless the test is risk-free and either perfectly specific for the disease in question or the treatment resulting from a positive test is free of complications. Echocardiography (whether TEE or TTE) in SAB does not fulfil these criteria. Risk assessment strategies such as that proposed in the current study need not identify which patients with SAB have no risk of Staphylococcus aureus infective endocarditis (SAIE), but, instead, which patients have a risk low enough to fall below the test threshold. This threshold has not been clearly defined in the literature, but it is instructive to note that, in a previous analysis [30], a TEE-guided strategy only offered 16 quality-adjusted life days over routine short-course therapy (2 weeks) for SAB in a model where the endocarditis rate was assumed to be 6 % and relapse inevitable for endocarditis treated with short-course therapy.
Two recent studies have also sought to identify a low-risk cohort of patients with SAB using clinical criteria. Kaasch et al. [23] identified endocarditis in only 0.5 % of patients with SAB who did not have prolonged bacteremia (>4 days), a permanent intracardiac device, hemodialysis dependency, spinal infection, or non-vertebral osteomyelitis. Khatib and Sharma [12] found endocarditis in 3.7 % of patients without prolonged bacteremia (>3 days), an intracardiac device, a secondary focus of infection, or relapse within 100 days (the last two criteria were based on information that may not be available at the time of initial clinical decisions regarding echocardiography). These studies have been criticized for low rates of echocardiography (TEE having been performed in only 20 [12] and 23 % [23] of patients), raising the possibility of missed cases of endocarditis [13, 24]. In addition, Kaasch et al. [23] used 3-month clinical outcomes as a surrogate for echocardiographic endocarditis in patients not undergoing echocardiography. This method, based on the assumption that IE “would become clinically apparent after the discontinuation of antibiotics”, enhances the reported sensitivity of the criteria by introducing an insensitive alternate standard, as well as likely contributing to the low prevalence of IE in this study (4.3–9.3 %) when compared to TEE-only cohorts (24–29 % [8, 12, 13]).
We chose to assess the criteria set primarily in episodes undergoing TEE given the importance of a highly sensitive standard in a study seeking to identify patients at low risk of endocarditis. The rate of TEE in our series (performed in 39 % of episodes) was significantly higher than in the two previous studies reporting risk factors predictive of low endocarditis risk [12, 23].
In this study, episodes of SAB without any of the included risk factors account for the majority of patients with nosocomial SAB. In our series, this group comprises 11 % of all SAB undergoing TEE and 57 % of nosocomial SAB undergoing TEE. Perhaps due to the use of fewer criteria, the proportion of patients fulfilling none of the criteria proposed in this study is higher than that presented in Kaasch et al. [23], where only 28 % of nosocomial SAB were included in the low-risk group.
The incomplete echocardiography coverage demonstrated in our series confirms that clinicians in our hospital are not following current guidelines with regards to performing echocardiography in the majority of SAB episodes. Less than half of SAB episodes in our series were investigated with TEE, and very few episodes with an initial negative TTE went on to TEE as recommended [1–3]. One interpretation of this discrepancy is that clinicians lack awareness of the risk of IE amongst patients with SAB and the guideline recommendations. A second possibility is that clinicians are already using some form of risk stratification to decide between TEE, TTE, and no echocardiography. This is suggested by the difference between the rates of endocarditis in the TEE (24 %) and TTE (5 %) groups, a difference that is not explained by even the lowest published estimates of TTE sensitivity. Thirdly, some patients may have had clinically diagnosed uncomplicated endocarditis and been treated without the need for echocardiography, although we feel this would be uncommon in our setting. Finally, it is also possible that clinicians accept a miss rate for endocarditis that is not zero (the figure advocated by current guidelines). Previous cost-effectiveness analyses [30, 31] suggest that this miss rate should be in the order of 2–4 episodes of IE per 100 cases of SAB, a figure which would seem achievable with the use of criteria sets such as that presented in this study.
There are a number of limitations to our study. Firstly, the data set was generated in a retrospective manner, leading to the potential for biased data collection. However, the data used were uniformly available, objective (date/time of blood cultures, blood culture results, date/time of admission, and the presence of an intracardiac prosthetic device), and were recorded prospectively on preexisting read-only databases. The most subjective data point for each episode of SAB was the presence or absence of endocarditis, but, as described above, we collected these data in a conservative fashion to ensure that any bias was towards the reporting of endocarditis. Indeed, the two cases of endocarditis amongst the episodes undergoing TTE only without any of the three risk factors had a very brief period of bacteremia (a single positive blood culture) and 5–6-mm strand-like valvular lesions labeled as “possible endocarditis” by the reporting cardiologist. Neither of these lesions were further characterized with TEE. The criteria set as proposed is only capable of informing the likelihood of echocardiographic features of endocarditis and, therefore, the yield of echocardiography for an episode of SAB. There are likely to be cases where the diagnosis of endocarditis is made on the basis of other non-echocardiographic features. Similarly, the criteria are unable to inform the risk assessment for either metastatic complications or clinical outcomes in SAB, and cannot, in isolation, be used to assign patients to a short-course treatment regimen. We also acknowledge that, whilst there were no cases of echocardiographic endocarditis amongst the episodes without risk factors investigated with TEE, there were only 23 patients in this group.
In summary, we present three criteria—community onset, prolonged bacteremia, and the presence of an intracardiac prosthetic device—which, despite being more inclusive than previously published criteria sets, are able, by their absence, to identify patients with SAB who are at very low risk of endocarditis as demonstrated by echocardiography. We contend that patients with none of these criteria may reasonably be managed without echocardiography, although prospective studies designed to measure the clinical outcomes of this approach will be needed. Future guidelines should incorporate an assessment of endocarditis risk into recommendations regarding echocardiography in SAB.
References
Habib G, Hoen B, Tornos P et al (2009) Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J 30:2369–2413. doi:10.1093/eurheartj/ehp285
Murray RJ (2005) Staphylococcus aureus infective endocarditis: diagnosis and management guidelines. Intern Med J 35:S25–S44
Mermel LA, Allon M, Bouza E et al (2009) Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis 49:1–45
Daniel WG, Erbel R, Kasper W et al (1991) Safety of transesophageal echocardiography. A multicenter survey of 10,419 examinations. Circulation 83:817–821
Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D’Ambra MN, Eltzschig HK (2010) Safety of transesophageal echocardiography. J Am Soc Echocardiogr 23:1115–1127
MacKenzie M, Rae N, Nathwani D (2014) Outcomes from global adult outpatient parenteral antimicrobial therapy programmes: a review of the last decade. Int J Antimicrob Agents 43:7–16
Pauker SG, Kassirer JP (1980) The threshold approach to clinical decision making. N Engl J Med 302:1109–1117
Fowler VG Jr, Li J, Corey GR et al (1997) Role of echocardiography in evaluation of patients with Staphylococcus aureus bacteremia: experience in 103 patients. J Am Coll Cardiol 30:1072–1078
Chang FY, MacDonald BB, Peacock JE Jr et al (2003) A prospective multicenter study of Staphylococcus aureus bacteremia: incidence of endocarditis, risk factors for mortality, and clinical impact of methicillin resistance. Medicine (Baltimore) 82:322–332
Fowler VG Jr, Olsen MK, Corey GR et al (2003) Clinical identifiers of complicated Staphylococcus aureus bacteremia. Arch Intern Med 163:2066–2072
Das I, O’Connell N, Lambert P (2007) Epidemiology, clinical and laboratory characteristics of Staphylococcus aureus bacteraemia in a university hospital in UK. J Hosp Infect 65:117–123
Khatib R, Sharma M (2013) Echocardiography is dispensable in uncomplicated Staphylococcus aureus bacteremia. Medicine (Baltimore) 92:182–188
Incani A, Hair C, Purnell P et al (2013) Staphylococcus aureus bacteraemia: evaluation of the role of transoesophageal echocardiography in identifying clinically unsuspected endocarditis. Eur J Clin Microbiol Infect Dis 32:1003–1008
Fowler VG Jr, Justice A, Moore C et al (2005) Risk factors for hematogenous complications of intravascular catheter-associated Staphylococcus aureus bacteremia. Clin Infect Dis 40:695–703
Robinson DL, Fowler VG, Sexton DJ, Corey RG, Conlon PJ (1997) Bacterial endocarditis in hemodialysis patients. Am J Kidney Dis 30:521–524
Chang CF, Kuo BI, Chen TL, Yang WC, Lee SD, Lin CC (2004) Infective endocarditis in maintenance hemodialysis patients: fifteen years’ experience in one medical center. J Nephrol 17:228–235
Benito N, Miró JM, de Lazzari E et al (2009) Health care-associated native valve endocarditis: importance of non-nosocomial acquisition. Ann Intern Med 150:586–594
Jensen AG, Espersen F, Skinhøj P, Rosdahl VT, Frimodt-Møller N (1997) Increasing frequency of vertebral osteomyelitis following Staphylococcus aureus bacteraemia in Denmark 1980–1990. J Infect 34:113–118
Pigrau C, Almirante B, Flores X et al (2005) Spontaneous pyogenic vertebral osteomyelitis and endocarditis: incidence, risk factors, and outcome. Am J Med 118:1287.e17–1287.e24
Fery-Blanco C, Revest M, Alla F et al (2010) Vertebral osteomyelitis associated with infective endocarditis: characteristics analyzed within IE2008, a one-year population-based survey in France. In: Program and abstracts of the 50th Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC), Boston, MA, September 2010. American Society for Microbiology, abstract K2168
Miro JM, Anguera I, Cabell CH et al (2005) Staphylococcus aureus native valve infective endocarditis: report of 566 episodes from the International Collaboration on Endocarditis Merged Database. Clin Infect Dis 41:507–514
Crowley AL, Peterson GE, Benjamin DK Jr et al (2008) Venous thrombosis in patients with short- and long-term central venous catheter-associated Staphylococcus aureus bacteremia. Crit Care Med 36:385–390
Kaasch AJ, Fowler VG Jr, Rieg S et al (2011) Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus bacteremia. Clin Infect Dis 53:1–9
Soriano A, Mensa J (2011) Is transesophageal echocardiography dispensable in hospital-acquired Staphylococcus aureus bacteremia? Clin Infect Dis 53:10–12
Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM (1988) CDC definitions for nosocomial infections, 1988. Am J Infect Control 16:128–140
Centers for Disease Control and Prevention (CDC) (2014) CDC/NHSN surveillance definitions for specific types of infection. Available online at: http://www.cdc.gov/nhsn/PDFs/pscManual/17pscNosInfDef_current.pdf. Accessed 1 June 2014
Fowler VG Jr, Sanders LL, Sexton DJ et al (1998) Outcome of Staphylococcus aureus bacteremia according to compliance with recommendations of infectious diseases specialists: experience with 244 patients. Clin Infect Dis 27:478–486
Friedman ND, Kaye KS, Stout JE et al (2002) Health care-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med 137:791–797
Bossuyt PM, Reitsma JB, Bruns DE et al (2003) Towards complete and accurate reporting of studies of diagnostic accuracy: The STARD Initiative. Ann Intern Med 138:40–44
Rosen AB, Fowler VG Jr, Corey GR et al (1999) Cost-effectiveness of transesophageal echocardiography to determine the duration of therapy for intravascular catheter-associated Staphylococcus aureus bacteremia. Ann Intern Med 130:810–820
Heidenreich PA, Masoudi FA, Maini B et al (1999) Echocardiography in patients with suspected endocarditis: a cost-effectiveness analysis. Am J Med 107:198–208
Acknowledgments
The authors would like to thank A/Prof Michele Levinson who commented on previous versions of this manuscript and the Department of Microbiology at the Royal Melbourne Hospital for their assistance with the data extraction.
Conflict of interest
The authors declare that they have no conflict of interest.
Compliance with ethical standards
The authors declare that they have complied with ethical standards with respect to disclosure of conflict of interest and research involving humans (see text for further details).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Heriot, G., Yeoh, J., Street, A. et al. Echocardiography has minimal yield and may not be warranted in Staphylococcus aureus bacteremia without clinical risk factors for endocarditis. Eur J Clin Microbiol Infect Dis 34, 1231–1236 (2015). https://doi.org/10.1007/s10096-015-2352-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-015-2352-7