
Abstract
Background
Mild encephalitis/encephalopathy with reversible splenial lesion (MERS) is a clinical-radiological syndrome characterized by transient central nervous system symptoms and a reversible lesion in the splenium of the corpus callosum (SCC) on magnetic resonance (MR). We reported a case of adult-onset MERS with uncommon presentation and reviewed the existing literature.
Methods
We described a case of adult-onset MERS with uncommon symptoms and signs and performed a systematic review of case series including more than four patients of adult-onset (> 14 years old) MERS, from January 2000 to December 2022. We summarized the clinical, laboratory, imaging and therapy data.
Results
We included seven eligible studies for a total of 51 adult-onset MERS patients. Neurological manifestations were preceded by prodromal symptoms in most of the patients (88%), mainly with fever (78%). Headache was the most common symptom (50%), followed by seizures (22%) and disturbance of consciousness (22%). Inflammatory changes on cerebrospinal fluid were present in a half of patient, so defining encephalitis cases. Clinal recovery, was achieved in all patients but two with severe disturbance of consciousness who required ventilator support in the acute phase. MR showed isolated lesion in the SCC in 92% of patients, while 8% of patients showed also extracallosal lesions, all the lesions resolved or improved on follow-up imaging.
Conclusions
MERS is a form of encephalitis/encephalopathy with a broad range of central nervous system manifestation, often with mild symptoms, such as headache alone, that can lead to overlooked some cases, with an excellent prognosis in most patient.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mild encephalitis/encephalopathy with reversible splenial lesion (MERS) is a clinical-radiological syndrome with neurological signs and symptoms of Central Nervous System (CNS) and evidence of a transient lesion in the central portion of the splenium of corpus callosum (SCC) on Magnetic Resonance (MR) [1]. Clinical picture is heterogeneous and consists in encephalopathy/encephalitis manifestations such as seizures, disturbance of consciousness and delirium [2, 3], and milder symptoms such headache. A prodromal phase with fever, flu-like symptoms or gastro-intestinal disturbance often precedes the neurological manifestations [2, 4]. MR shows high signal intensity on fluid-attenuated-inversion recovery (FLAIR) and T2 weighted images on the SCC, reduced diffusion (hyperintensity on diffusion-weighted sequences -DWI- and low apparent diffusion coefficient -ADC- value), without enhancement after gadolinium infusion[1, 5, 6]. The clinical and imaging picture usually resolve within two-four weeks [1, 3]. MERS has been classified into two subtypes, based on the imaging features: MERS type 1 (isolated oval lesion in the center of the splenium) and MERS type 2 (the lesion in the splenium extends into the anterior part of the corpus callosum or into the cerebral white matter) [6,7,8], and has been associated with a number of systemic and brain pathological conditions, such as infections and antiepileptic drugs [9,10,11,12,13,14,15,16,17,18,19]. The majority of published studies reported on a pediatric population [4, 20, 21], whereas fewer studies investigated the clinical features of adult-onset MERS. During the Sars-Cov-2 pandemic many reports of Covid-related MERS in adults have been published[22, 23], but studies on MERS not related to Sars-Cov-2 remain scarce.
We report a case of adult-onset MERS not related to Sars-Cov-2 infection and conducted a systematic review of literature to summarize the current evidence about clinical manifestations, radiological findings, prognosis and therapy in adult patients.
Case report
A 21-years-old Chinese man presented at the Emergency Department complaining four days of fever, headache and myalgias. Laboratory examination revealed normal white blood cell count, C-reactive protein and urinalysis, with mild hyponatremia (131 mEq/l). Molecular oropharyngeal test for Sars-Cov-2 was negative. The physical and neurological examination were otherwise unremarkable. CT brain was negative and the patient was discharged at home.
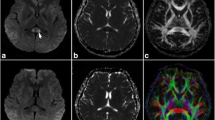
Four days later the patient presented again at the Emergency Department for fatigue, anorexia, headache, and lower abdominal pain, without fever. At the neurological examination he was alert, oriented, consciousness but restless, with involuntary movement at four limbs consistent with myoclonic movement, with postural and tactile stimulus activation and exaggerated startle response. Physical examination revealed hypogastric abdominal pain with sign of urinary retention at bladder ultrasound, in absence of urge to void and transurethral catheterization revealed residual urine. Blood exams reveled persistent mild hyponatremia (133 mEq/l), systemic inflammation markers were negative. The brain CT was unremarkable. The cerebrospinal fluid (CSF) examination showed increased protein content (1 g/dl) without cells, microbiological workup was negative. After few hours the patient had a clinical worsening developing visual hallucination, decrease of consciousness and meningeal irritation sign. A brain MR showed an isolated ovoidal lesion in the SCC, hyperintense on DWI, FLAIR, and T2-weighted images, hypointense on ADC sequences, without gadolinium enhancement (Fig. 1 A,B,C); no extracallosal lesions were detected. The patient was diagnosed as having a MERS, and administrated with bolus of methylprednisolone (1 g/d) for five days followed by tapering and intravenous acyclovir. The neurological symptoms gradually improved during the next days. EEG revealed mild slowing of basic activity with sporadic frontal slow waves, consistent with a diffuse encephalopathy. Serological tests for neurotropic viruses and bacteria were also negative. Autoimmunity tests as well as anti-sulfatide, anti-ganglioside, anti-myelin oligodendrocyte glycoprotein, anti-aquaporin-4 antibodies, anti-surface receptor and onconeural antibodies were negative. Another CSF sample was obtained with evidence of pleocytosis (64 cells/microL) without increased protein concentration, oligoclonal bands were observed. A follow-up MR was performed two weeks later showing a partial regression of SCC lesion with regression of restricted diffusion e mild hyperintensity on T2 images, without gadolinium enhancement. The SCC lesion was not present at a further MR performed a month and a half later (Fig. 1 D,E,F).

SCC lesion at onset of neurological symptoms, with hyperintensity on DWI (A), hypointensity in ADC (B) and hyperintensity on FLAIR (C) sequences and regression of the lesion at follow-up (D, E, F)
Methods
The systematic review was performed according to the Cochrane Handbook for Systematic Review of Interventions (https://training.cochrane.org/handbook) and results were presented following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations [24]. Data search, extraction, analysis, and interpretation were performed following a prespecified study protocol developed by the investigators (not registered or published).
Potentially eligible studies were identified through PubMed database, using the following search strategy: "Mild Encephalitis/encephalopathy with reversible splenial lesion" OR "cytotoxic lesions of the corpus callosum" OR "transient focal lesions in the splenium of the corpus callosum" OR "reversible splenial lesion syndrome" OR ((transient OR reversible) AND (splenium OR splenial) AND corpus callosum AND lesion), from January 2000 to December 2022.
We applied the following inclusion criteria: (1) English-written articles; (2) adult-onset of MERS (≥ 14 years) (3) case series with more than three patients; (4) final diagnosis of MERS type 1 and/or 2. We excluded: (1) case reports; (2) patients without symptoms/signs of CNS involvement; (3) unavailable follow-up MR; (4) pediatric cases; (5) Sars-Cov-2 associated MERS.
We extracted the following information: author, study country, age, gender, prodromal symptoms (fever, flu-like or gastrointestinal symptoms), CNS symptoms, etiology, auxiliary examination (blood chemistry with systemic inflammation markers and hyponatremia, EEG, CSF analysis, MR data), therapy and clinical and radiological outcome.
We reviewed each case and defined MERS as follows:
-
1-
Encephalitis/encephalopathy defined as acute onset of CNS signs/symptoms AND
-
2-
Reversible SCC lesion on MR
We used the terms encephalitis/encephalopathy in presence/absence of inflammatory changes (increased level of proteins and/or pleocytosis) on cerebrospinal fluid (CSF) examination, respectively.
We summarized raw numbers with sum, percentage, mean. All studies were case series, indicating low level of evidence and high risk of bias, thus we did not perform risk of bias assessment nor formal statistical testing.
Results
The initial search retrieved 450 results. We excluded 215 articles, 196 based on title and 19 not written in English. We then screened 235 records and excluded other 225 articles (14 case series in only children and 211 single case reports). Thus, we examined 10 full-text articles and excluded one study for missing relevant data, and two studies for unclear clinical assessment (absence of encephalitis/encephalopathy signs/symptoms). The study selection process is illustrated in Fig. 2. We included in the systematic review seven articles [1, 25,26,27,28,29,30], for a total of 67 patient, three studies excluded MERS type 2 [1, 26, 27]. Included studies were published from 2004 to 2019. We therefore reviewed single patient-level data where available and excluded 16 patients for the following reasons: 12 for age < 14 years, two for absence of sign/symptoms of CNS involvement (syncope, glossopharyngeal neuralgia), one for incidental SCC lesion without neurological symptoms, one lost to follow-up. We finally screened 51 adult-onset MERS patients. Of the seven case-series, five were from China, one from Japan and one from France, respectively 43 (84%) patients from Asia and 8 (16%) from Europe.

Preferred reporting items for meta-analyses (PRISMA) flowchart of study selection
The clinical and laboratory data are showed in Table 1, and Table 2. The mean age of onset was 28.9 ± 5.1 (range 14–60) years, 28 (55%) patients were male. Most of the patients (88%) experienced prodromal symptoms, mainly fever (78%) and/or flu-like symptoms (42%). Headache was the most frequent symptom of presentation and was present in 25 (50%) patients, in 10 (20%) was the only neurological symptom. Seizure and disturbance of consciousness were present in 11 (22%) patients, delirium was observed in 8 (16%) patients. Neurological signs were present in 7 (14%) patients as meningeal irritation, acute urinary retention was reported in two (4%) patients. Complete clinical recovery was observed in 96% of the whole population, mostly within two weeks. Two patients had unfavorable prognosis at four weeks (vegetative state and come).
A total of 47 (92%) patients performed a lumbar puncture, inflammatory changes were present in 56%, mainly with pleocytosis (23/47, 49%), nine (21%) patients had increased proteins, five (10%) with both. EEG was performed in 36 (71%) patients, of whom 19 (53%) had slow basic activity. Serum sodium level was available in 27 (53%) patients, ten (37%) had hyponatremia.
In 33 (73%) the etiology was unknown, 12 (27%) patients were reported as having a defined previous infection.
Imaging data of the included patients are shown in Table 3. All the patients received baseline and follow-up brain MR. An isolated lesion in the center of the SCC was detected in 92% (47/51), while four patients showed also extracallosal lesions, suggesting diagnosis of MERS-1 and MERS-2, respectively. Involvement of the anterior part of the CC was not detected. In 29 (57%) patients lesion shape was available and was mainly ovoidal (83%), in five (17%) patients the lesion extended irregularly into the lateral portion of SCC. MR lesions showed hyperintense signal on T2 sequences, and restricted diffusion on DWI and ADC sequences. No contrast enhancement was observed. Follow-up MR was performed with a mean of 25 (range 5–120) days after the baseline MR. A complete regression of the lesions was observed in 47 (92%) patients, four (8%) patients showed reduction in size and signal intensity of MR finding without complete resolution.
Treatment data are showed in Table 4. The treatment strategy was available for 43 (84%) patients, 26 (60%) received corticosteroids, 7 (16%) intravenous immunoglobulin, 30 (70%) antiviral therapy, 12 (30%) antibiotics, 22 (51%) received a combination therapy. Five patients did not receive any treatment and did not have any neurological sequelae.
Discussion
Reversible lesion of SCC has been associated with a variety of disorders, and in 2011 Garcia-Monco et al. merged the reversible splenial lesions syndrome (RESLES), with MERS included in the spectrum of RESLES [31]. Isolated reversible lesion of SCC on MR was reported for the first time in patients with epilepsy receiving antiepileptic drugs[32,33,34]. Afterwards, Tada et al. described the same MR finding in a case series of patients with encephalitis/encephalopathy caused by various infectious agents, and proposed this new clinical-radiological syndrome, namely MERS[1].
We presented a case of MERS in a young adult with uncommon clinical picture such as movement disorders (myoclonic movements at four limbs) and exaggerated startle response, without electroencephalographic findings suggestive for seizures. Other two cases of MERS with upper limb myoclonus and no electroencephalographic findings were reported[19, 28]. Our patient presented meningeal signs in association with urinary retention, which resembled the meningitis retention syndrome, which is characterized by aseptic meningitis and acute urinary retention, with benign and self-remitting course within few weeks, without brain lesions/involvement. Other few cases of MERS associated with meningitis retention syndrome[9, 25, 35,36,37] were reported, with MERS usually preceding or occurring simultaneously to urinary retention, in our case the encephalitic and the meningeal inflammation processes likely occurred at the same time.
Most MERS cases were reported in the pediatric population [5], where diagnostic criteria have been already formulated [5, 38], however, data on adults are scarce. In this systematic review we included only adult-onset (> 14 years) patients from case series and reviewed each case to include clinical and imaging features consistent with MERS. Our review suggested that clinical symptoms of CNS involvement may differ from children to adults, alluding to differences in immunity response[29]. The clinical spectrum was heterogeneous, however, we found that fever was the most common prodromal manifestation, as previously reported[1, 2, 4, 39]. While disturbance of consciousness, delirious behavior and seizures were frequent neurological manifestation in child-onset MERS[38], headache was the most common symptom of presentation in adult-onset, with one out of five patients presenting only with headache, which frequently was the only symptom reported. As headache is a common symptom in the general population and is frequent during fever, our review indirectly suggests that the incidence of SCC lesions on MR in adults may be underestimated.
We found that laboratory tests are not specific, however, some points deserve attention. We found that hyponatremia was present in around one third of patients with available serum sodium levels. Of note, all the three patients (including our case report) with acute urinary retention had hyponatriemia. Mild hyponatremia has been described in previous reports [40] and has been proposed as a contributing factor for MERS [29]. CSF analysis showed an aspecific inflammatory profile in more than a half of patients, with slight pleocytosis and mild protein increase, supporting the para/post infective nature of MERS. EEG findings were aspecific[3, 41] and suggested a general impairment of cerebral functions consistent with encephalitis/encephalopathy in around a half of patients.
Although the etiology is often unknown, various viral and bacteria pathogens have been reported as associated with MERS. We found that only in a minority of patients an infection was identified, most frequently viral infection, followed by bacterial infection. The cytokine-mediated cytotoxic edema[42] rather than the direct invasion of the pathogen has been proposed as pathogenetic mechanism since no causative agent is usually found in CSF, therefore the mechanism is supposed to be inflammatory-mediated, with a possible autoimmunitary response. SCC may be prone to cytotoxic edema due to the high blood supply, resulting from both the anterior and posterior circulation[43, 44], and the high density of cytokine and glutamate receptors [45]. The reversibility of the lesion is thought to originate from intramyelinic edema and inflammatory infiltrate [1].
According to the localization of the reversible lesion, MERS can be classified in type 1 and type 2, and we found a high prevalence of MERS-1. Although our results may reflect that the selected studies (three out of seven case series) did not include type 2 patients, MERS-1 seems to be more common compared to MERS-2. The splenial lesion is usually ovoidal/rounded-shaped and centered in the SCC, whereas and in a minority of patient the lesion extends to the lateral portion of SCC (the so-called “boomerang sign”). The SCC lesion presented a homogeneous high-signal on T2-WI/FLAIR, hyperintense on DWI with low ADC value, suggesting reversible cytotoxic edema, without contrast enhancement. All the lesions resolved or improved on follow-up imaging, supporting the transient and potentially reversible nature of the pathological process. However, according to Zhu et al.[26], occurrence of unfavourable outcome despite imaging lesion resolution suggests that MERS may not always have a mild course. Remarkably, severe disturbance of consciousness at onset was the clinical feature associated with ventilation support in the acute stage of disease, as previously suggested[26].
There is no consensus about the therapeutic strategy. The inflammatory process may support the use of corticosteroids, which could represent the only therapy once infective processes have been excluded, conversely, antibiotics or antiviral agents may be used when a specific pathogen is present. However, we found that six patients with mild clinical symptoms did not receive any treatment and had no neurological sequelae, suggesting that specific treatment may not be always necessary and supportive therapy could be the right strategy in milder cases.
In conclusion, our review suggests that MERS in adults is a form of encephalitis/encephalopathy with a broad range of central nervous system manifestations, often with mild symptoms, such as headache, and could follow unspecific symptoms such as fever. Laboratory tests are not specific, and the term encephalitis should be used when there are inflammatory markers in cerebrospinal fluid, which occur in around a half of patients, otherwise the term encephalopathy should be used. Hyponatremia may be present up to a third of patients and may help early diagnosis. We advocate that MERS in adults has a para/post infective origin, other encephalitis/encephalopathy with SCC lesions from known etiologies (e.g. antiepileptic drugs, metabolic disorders) should not be classified as MERS, rather the generic term RESLES should be adopted. The presence of an inflammatory lesion usually located in the SCC and reversible within a month is a key feature of diagnosis, with MERS-1 being the most frequent type. Further studies are needed to better characterize the clinical-radiological entity of MERS.
Data availability
Data supporting the results of the study are available upon reasonable request at the corresponding author.
References
Tada H et al (2004) Clinically mild encephalitis/encephalopathy with a reversible splenial lesion. Neurology 63(10):1854–1858
Takanashi J (2009) Two newly proposed infectious encephalitis/encephalopathy syndromes. Brain Dev 31(7):521–528
Fang Q et al (2017) Clinically mild encephalitis/encephalopathy with a reversible splenial lesion of corpus callosum in Chinese children. Brain Dev 39(4):321–326
Chen WX et al (2016) Reversible splenial lesion syndrome in children: Retrospective study and summary of case series. Brain Dev 38(10):915–927
Hoshino A et al (2012) Epidemiology of acute encephalopathy in Japan, with emphasis on the association of viruses and syndromes. Brain Dev 34(5):337–343
Takanashi J et al (2006) Widening spectrum of a reversible splenial lesion with transiently reduced diffusion. AJNR Am J Neuroradiol 27(4):836–838
Takanashi J, Hirasawa K, Tada H (2006) Reversible restricted diffusion of entire corpus callosum. J Neurol Sci 247(1):101–104
Takanashi J et al (2010) Differences in the time course of splenial and white matter lesions in clinically mild encephalitis/encephalopathy with a reversible splenial lesion (MERS). J Neurol Sci 292(1–2):24–27
Yuan J et al (2017) Mild encephalitis/encephalopathy with reversible splenial lesion (MERS) in adults-a case report and literature review. BMC Neurol 17(1):103
Thabet M et al (2022) Rituximab-induced mild encephalopathy with a reversible splenial lesion syndrome (MERS): An adverse effect to add to the list. Br J Clin Pharmacol 88(6):2969–2972
Heraud C et al (2022) Glial Fibrillary Acidic Protein (GFAP) Astrocytopathy Presenting as Mild Encephalopathy with Reversible Splenium Lesion. Neurol Ther 11(1):499–505
Saghir K., et al (2022) Anti-MDA5 antibody-positive dermatomyositis with mild encephalopathy with reversible splenial lesion: a possible rare association? Wien Med Wochenschr, 1–4
Mogi T et al (2017) Clinically mild encephalopathy with a reversible splenial lesion and nonconvulsive status epilepticus in a schizophrenic patient with neuroleptic malignant syndrome. Psychiatry Clin Neurosci 71(3):212
Ono R, Nishiguchi S, Kitagawa I (2022) Lithium intoxication-associated mild encephalitis/encephalopathy with a reversible splenial lesion: A case report. Bipolar Disord 24(5):551–552
Mawatari M et al (2018) Mild encephalitis/encephalopathy with a reversible splenial lesion due to Plasmodium falciparum malaria: a case report. Trop Med Health 46:37
Chopra P, Bhatia RS, Chopra R (2019) Mild Encephalopathy/Encephalitis with Reversible Splenial Lesion in a Patient with Salmonella typhi Infection: An Unusual Presentation with Excellent Prognosis. Indian J Crit Care Med 23(12):584–586
Nagpal K et al (2017) Chikungunya infection presenting as mild encephalitis with a reversible lesion in the splenium: a case report. J Neurovirol 23(3):501–503
Fu ML, Han N, Wang W (2021) Cytomegalovirus-Associated Mild Encephalopathy/Encephalitis With Reversible Splenial Lesion. Neurologist 26(5):172–174
Takahashi I, Yano H, Kinjo M (2020) Mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) following influenza virus infection. BMJ Case Rep. 13(5):e235461
Zhang X et al (2020) Reversible splenial lesion syndrome in children: clinical analysis and summary of a case series. J Int Med Res 48(4):300060520914202
Yildiz AE et al (2018) Mild encephalitis/encephalopathy with a reversible splenial lesion in children. Diagn Interv Radiol 24(2):108–112
Hayashi M et al (2020) COVID-19-associated mild encephalitis/encephalopathy with a reversible splenial lesion. J Neurol Sci 415:116941
De Oliveira FA, De Melo TF, Rocha-Filho PA (2020) Transient lesion in the splenium of the corpus callosum associated with COVID-19. Arq Neuropsiquiatr 78(11):738
Liberati A et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 6(7):e1000100
Pan JJ et al (2015) Mild encephalitis/encephalopathy with a reversible splenial lesion: five cases and a literature review. Neurol Sci 36(11):2043–2051
Zhu Y et al (2016) Reversible splenial lesion syndrome associated with encephalitis/encephalopathy presenting with great clinical heterogeneity. BMC Neurol 16:49
Zhang Z et al (2020) Mild Encephalitis/Encephalopathy with a Reversible Isolated Splenial Lesion (MERS) in Adult Patients: A Small Case Series. Eur Neurol 83(3):279–286
Grosset L et al (2021) Mild encephalopathy with reversible splenial lesion: Description of nine cases and review of the literature. Seizure 88:83–86
Gao X et al (2020) Clinical analysis of reversible splenial lesion syndrome in Chinese adults: A retrospective study of 11 cases. Medicine (Baltimore) 99(36):e22052
Xu W et al (2019) Clinical and Magnetic Resonance Imaging Features of Reversible Splenial Lesion Syndrome in Adults: A Small Case Series. Eur Neurol 82(4–6):86–92
Garcia-Monco JC et al (2011) Reversible splenial lesion syndrome (RESLES): what’s in a name? J Neuroimaging 21(2):e1-14
Kim SS et al (1999) Focal lesion in the splenium of the corpus callosum in epileptic patients: antiepileptic drug toxicity? AJNR Am J Neuroradiol 20(1):125–129
Maeda M et al (2003) Transient splenial lesion of the corpus callosum associated with antiepileptic drugs: evaluation by diffusion-weighted MR imaging. Eur Radiol 13(8):1902–1906
Mirsattari SM et al (2003) Transient lesion in the splenium of the corpus callosum in an epileptic patient. Neurology 60(11):1838–1841
Tascilar N et al (2009) Unusual combination of reversible splenial lesion and meningitis-retention syndrome in aseptic meningomyelitis. Clinics (Sao Paulo) 64(9):932–937
Kitami M et al (2011) Acute urinary retention in a 23-year-old woman with mild encephalopathy with a reversible splenial lesion: a case report. J Med Case Rep 5:159
Hidaka M et al (2021) (2021) Meningitis retention syndrome associated with complicated mild encephalitis/encephalopathy with reversible splenial lesion in a young adult patient: a case report. Oxf Med Case Reports 10:omab092
Mizuguchi M et al (2021) Guidelines for the diagnosis and treatment of acute encephalopathy in childhood. Brain Dev 43(1):2–31
Ka A et al (2015) Mild encephalopathy with reversible splenial lesion: an important differential of encephalitis. Eur J Paediatr Neurol 19(3):377–382
Takanashi J et al (2009) Encephalopathy with a reversible splenial lesion is associated with hyponatremia. Brain Dev 31(3):217–220
Kashiwagi M et al (2014) Clinico-radiological spectrum of reversible splenial lesions in children. Brain Dev 36(4):330–336
Tetsuka S (2019) Reversible lesion in the splenium of the corpus callosum. Brain Behav 9(11):e01440
Kakou M, Velut S, Destrieux C (1998) Arterial and venous vascularization of the corpus callosum. Neurochirurgie 44(1 Suppl):31–37
Kahilogullari G et al (2013) Arterial vascularization patterns of the splenium: An anatomical study. Clin Anat 26(6):675–681
Hassel B et al (2003) Glutamate transport, glutamine synthetase and phosphate-activated glutaminase in rat CNS white matter. A quantitative study J Neurochem 87(1):230–237
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All authors read and approved the manuscript, and the manuscript has not been submitted elsewhere nor published elsewhere in whole or in part.
Conflict of interest
All authors declare that they have no conflicts of interest.
Ethical approval
Given the nature of the article, a case report and systematic review, no ethical approval was required.
Informed consent
Written informed consent was obtained from the participant of the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chiara, R., Vanessa, P., Nazerian, P. et al. Adult-onset of mild encephalitis/encephalopathy with reversible splenial lesion (MERS): case report and systematic review. Neurol Sci (2024). https://doi.org/10.1007/s10072-024-07627-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10072-024-07627-0