
Abstract
A 56-year-old man presented to the clinic with episodic headaches for several years which had been worsening over a few months prior to the presentation. He described headache as sharp, stabbing pain around the left eye associated with nausea, vomiting, photophobia, and phonophobia lasting for hours associated with flushing on the left side of the face. The picture of his face during these episodes showed flushing of the left side of the face, ptosis of the right eyelid, and miosis (panel A). Flushing in his face would resolve with the abortion of the headache. At the time of presentation to the clinic, his neurological exam was only significant for mild left eye ptosis and miosis (panels B and C). Extensive workup including MRI brain, cervical spine, thoracic spine, lumbar spine, CTA head and neck, and CT maxillofacial was unremarkable. He had tried several medications in the past including valproic acid, nortriptyline, and verapamil without significant benefit. He was started on erenumab for migraine prophylaxis and was given sumatriptan for abortive therapy following which his headaches improved. The patient was diagnosed with idiopathic left Horner’s syndrome and his migraines with autonomic dysfunction would present with unilateral flushing opposite to the site of Horner’s presenting as Harlequin syndrome [1, 2].
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Case
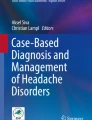
A 56-year-old man presented to the clinic with episodic headaches for several years which had been worsening over a few months prior to the presentation. He described headache as sharp, stabbing pain around the left eye associated with nausea, vomiting, photophobia, and phonophobia lasting for hours associated with flushing on the left side of the face. The picture of his face during these episodes showed flushing of the left side of the face, ptosis of the right eyelid, and miosis (panel A). Flushing in his face would resolve with the abortion of the headache. At the time of presentation to the clinic, his neurological exam was only significant for mild left eye ptosis and miosis (panels B and C). Extensive workup including MRI brain, cervical spine, thoracic spine, lumbar spine, CTA head and neck, and CT maxillofacial was unremarkable. He had tried several medications in the past including valproic acid, nortriptyline, and verapamil without significant benefit. He was started on erenumab for migraine prophylaxis and was given sumatriptan for abortive therapy following which his headaches improved. The patient was diagnosed with idiopathic left Horner’s syndrome and his migraines with autonomic dysfunction would present with unilateral flushing opposite to the site of Horner’s presenting as Harlequin syndrome [1, 2].

A Left facial flushing at the time of episodic headache (black arrows). B Partial ptosis and miosis in right eye (white arrow) (in ambient light). C Partial ptosis and miosis in right eye (white arrow) (miosis more obvious with ambient lights turned off)
References
Wasner G, Maag R, Ludwig J, Binder A, Schattschneider J, Stingele R et al (2005) Harlequin syndrome-one face of many etiologies. Nat Clin Pract Neurol 1(1):54–59
Lance JW, Drummond P, Gandevia SC, Morris J (1988) Harlequin syndrome: the sudden onset of unilateral flushing and sweating. J Neurol Neurosurg Psychiatry 51(5):635–642
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Informed consent for publication with pictures was obtained from the patient.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sharma, R., Khan, H. Harlequin syndrome. Neurol Sci 44, 2989–2990 (2023). https://doi.org/10.1007/s10072-023-06849-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-023-06849-y