
Abstract
Background
Natalizumab is an effective therapy in the treatment of relapsing-remitting multiple sclerosis; it induces lymphocytosis (NIL, natalizumab-induced lymphocytosis) and changes the peripheral lymphocyte pattern.
Methods
This study aims to evaluate NIL, peripheral blood lymphocyte subsets, CD4/CD8 ratio, and their impacts on JCV index and clinical data—No Evidence of Disease Activity (NEDA-3) and annualized relapse rate (ARR) in patients treated with natalizumab.
Results
Forty-one patients (33 women) were included in the study. The mean duration of follow-up on natalizumab treatment was 6.7 ± 3.2 years. Significant increases in relative lymphocytosis after 1 month, with a median of 40.4% (− 34.1 to + 145.5%) (p < 0.001), and after 1 year (49.0% (− 9.3 to + 127.6%)) (p < 0.001) were found. Significant differences were found after 1 month when comparing NIL between patients JCV-seroconverting (20.6% (− 17.7 to 72.7%)) and stable JCV-seronegative ones (43.5% (− 6.3 to +96.3%)) (p = 0.04). No significant difference NIL level was found between the patients exhibiting NEDA-3 status and those without it. ARR on natalizumab treatment correlated with CD4/CD8 ratio (r = 0.356; p = 0.021); patients who maintained NEDA-3 status over the whole treatment period exhibited a lower CD4/CD8 ratio (1.89 ± 1.08 vs. 2.5 ± 0.73; p < 0.04).
Conclusion
This contribution reports the CD4/CD8 ratio as a possible biomarker for better clinical efficacy of natalizumab in patients exhibiting a lower CD4/CD8 ratio. NIL did not correlate with long-term therapeutic efficacy in patients treated with natalizumab, but was demonstrated as lower in patients JCV-seroconverting in the course of follow-up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Natalizumab is a humanized monoclonal antibody targeting very-late-activating antigen-4 (VLA-4), a molecule involved in the migration of lymphocytes through the blood-brain barrier into the central nervous system (CNS). It has shown high efficacy in patients affected by relapsing-remitting multiple sclerosis (RRMS) in terms of a significant reduction in annualized relapse rate (ARR) and the risk of sustained disability progression by the standards of No Evidence of Disease Activity (NEDA-3) status, defined as an absence of relapses, progression, or new T2-hyperintense lesions on MRI [1, 2]. Its mechanism of action is based on the prevention of lymphocyte migration in the CNS, thus increasing the number of immune cells in the peripheral blood [3]. Natalizumab treatment, however, may affect lymphocyte subsets in various ways, as the α4β1 integrins are expressed differently on lymphocyte subtypes. It has been reported that memory subsets of B and T cells express higher levels of VLA-4 than naive forms [4, 5]. An increase may be observed in the absolute number of lymphocytes (natalizumab-induced lymphocytosis, NIL) in the blood count and, in particular, in a characteristic reversal of the relative leukocyte formula during treatment. The latter phenomenon is primarily due to lymphocyte sequestration in the peripheral circulation in reaction to the drug [6]. However, it is also related to VLA-4, which is expressed on all hematopoietic cells and is implicated in single-cell mobilization and migration of CD34 lymphocytes [7]. NIL has been considered a biomarker of the therapeutic efficacy of natalizumab, according to Signoriello [8].
Natalizumab treatment is associated with some risk of progressive multifocal leukoencephalopathy (PML), a rare subacute disease characterized by widespread loss of myelin arising out of reactivation of John Cunningham virus (JCV) [9,10,11,12,13]. Several factors, among them the duration of natalizumab treatment, prior use of immunosuppressants, and the presence of serum anti-JCV antibodies, may establish PML risk [14]. Anti-JCV antibodies occur in 50–70% of multiple sclerosis (MS) patients, while the anti-JCV antibody index has been reported as correlating with PML risk in seropositive patients [15,16,17,18,19,20,21]. Estimation of PML risk is an essential step for informed risk–benefit evaluation and treatment decisions in MS patients. Since JCV infection is a prerequisite for PML development, a two-step, enzyme-linked immunosorbent assay (ELISA) to detect anti-JCV antibodies has been developed to stratify PML risk (stratify test) [14].
Several studies have evaluated the peripheral lymphocyte pattern during natalizumab treatment, showing a disproportionate increase in peripheral subsets of lymphocytes and in CD4/CD8 ratio, both in the CNS and to a lesser extent in the peripheral blood [22,23,24,25]. Increased peripheral blood CD8+ T lymphocyte effector subset percentages are associated with JCV-DNA positivity [22]. Real-world evidence and observational studies are becoming increasingly attractive to researchers, since they reflect the usefulness of drugs in real life and have potential to disclose uncommon or rare adverse drug reactions and inclusive lab abnormalities. Therefore, real-world evidence can assist in evaluating a drug profile in clinical practice and in linking it with other clinical outcomes.
This study aims to evaluate NIL and lymphocyte pattern modification during natalizumab treatment in MS patients and its relationship with anti-JCV antibody index and the clinical efficacy of natalizumab treatment, in order to identify alternative, reliable immunological markers that may facilitate improvements in the safety and efficacy of therapy and guide tailored clinical decisions based on real-world evidence.
Patients and methods
Forty-one patients with RRMS, treated with natalizumab in the multiple sclerosis center of a large university hospital, were included into the study. They had all received at least 12 natalizumab infusions. All patients were over the age of 18 and their MS diagnoses were based on the 2017 McDonald criteria [26]. Exclusion criteria were the presence of autoimmune diseases other than MS and systemic steroids administered within 30 days before blood sampling. Patients treated with intravenous immunoglobulins or other blood products were not included in the study in the light of possible impacts on the antibody index [27].
Retrospective evaluations were made of leukocyte and lymphocyte blood counts before commencement of natalizumab treatment, after 1 month and 1 year of natalizumab treatment. NEDA-3 status and ARR in the whole cohort were evaluated.
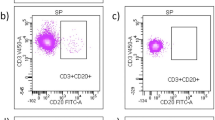
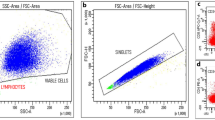
Lymphocyte subsets (CD3+, CD3+CD4+, CD3+CD8+) and CD4/CD8 ratio were prospectively obtained by flow cytometry in the whole cohort.
No informed consent was required since assessments and blood sampling were performed as part of a safety program for clinical practice. The research was approved by the local ethical committee.
Patients received natalizumab 300 mg intravenously every 28 days. Blood samples were collected by peripheral venous puncture before natalizumab infusion. The samples were always collected and analyzed by the same central laboratory. NEDA-3 status was evaluated on the basis of routinely recorded clinical data and 1.5-T magnetic resonance imagining (MRI). Expanded Disability Status Scale (EDSS) scores were obtained on a 3-month basis. The ARR was evaluated for the 2 years before natalizumab administration and then for the whole period of treatment. Clinical relapse was defined as the appearance of new neurological deficits or an exacerbation of existing ones lasting more than 24 h, in the absence of fever. An MRI scan was taken every year, while neurological examinations were performed every 3 months.
Anti-JCV antibody serological status and index were determined every 6 months by a two-step enzyme-linked immunosorbent assay (STRATIFY JCV DxSelect). An index value of less than 0.2 was considered anti-JCV antibody negative and of greater than 0.4 as anti-JCV antibody positive. Samples with an index between 0.2 and 0.4 were evaluated using a supplementary confirmatory test (second step). In the confirmation test, the patient sample was pre-inhibited with the coating antigen in solution and the pre-inhibited and non-inhibited aliquots of patient serum were tested. The results of the confirmation assay were reported as percentage inhibition and results higher than 45% were classified as anti-JCV antibody positive [28].
Flow cytometry analysis
The assessment of immune cell subsets in peripheral blood was performed by flow cytometry.
Whole peripheral blood collected in EDTA was used for multi-color flow cytometry immunophenotyping. A range of immunological subtypes, including CD3+ lymphocytes, CD3+CD4+ helper T lymphocytes, and CD3+CD8+ suppressor/cytotoxic T lymphocytes, were detected using KOMBITEST CD3 FITC CD8 PE/CD45 PerCP/CD4 APC (Exbio), and CD4/CD8 ratio was obtained. The flow cytometry assay was performed by BD FACSCanto II with SW Diva 1.3 analytics (BD Biosciences). The patients did not exhibit any relapse at least 3 months before blood sampling.
Statistical analysis
The normally distributed data are given as the mean and standard deviation (SD) (relative CD4 and CD8 lymphocyte count, CD4/CD8 ratio, absolute leukocyte and lymphocyte count, age, duration of natalizumab treatment) while the non-normally distributed factors (relative lymphocyte count, ARR, JCV index) are given as median and minimum/maximum. The relationships between lymphocytes, CD4/CD8 ratio, JCV index, and ARR were tested by means of Spearman’s rank-order correlation. Spearman’s correlation coefficients (r) and p values for each analysis were reported. Comparisons of groups of natalizumab-related patients were analyzed by the Mann-Whitney U test. The ANOVA test was used for differences in CD4/CD8 ratio arising out of comparison between groups of stable JCV-positive, stable JCV-negative, and JCV-seroconverting patients. SPSS (version 26, SPSS, Chicago, IL, USA) was used for data analysis. Results were considered statistically significant at the p < 0.05 level.
Results
Forty-one patients (33 women (80%)), with a mean age when natalizumab treatment commenced of 36.5 ± 7.5 years, and a mean disease duration before natalizumab treatment of 6.6 ± 2.9 years, were included into this study. The mean duration of follow-up on natalizumab treatment was 6.7 ± 3.2 years; 24 patients exhibited NEDA-3 status (58%) with a mean follow-up period of 7.1 ± 3.1 years, compared with 17 patients who did not exhibit NEDA-3 status (42%), with a mean follow-up period of 6.3 ± 3.4 years; no significant differences emerged in duration of natalizumab treatment duration (p = 0.47). Thirteen patients exhibited at least one relapse, 12 patients exhibited some disability progression (EDSS), and 16 patients showed some progression on MRI (new T2 or gadolinium-enhancing lesions) over the whole treatment duration.
Median ARR 2 years before natalizumab treatment was 1.5 (0.5–3); median ARR for the entire natalizumab treatment was 0 (0 to 2). Natalizumab significantly decreased ARR (p < 0.001). The baseline JCV index at the beginning of natalizumab treatment was positive in 21 patients (51%) with a median of 0.35 (0.1–4.16). Ten patients seroconverted (21%) over the follow-up period (7 to seropositivity; 3 to seronegativity). No patient experienced a PML during the follow-up period. A summary of the demographic and clinical features of the patients appears in Table 1.
Mean absolute leukocyte count before the first natalizumab infusion was 6.91 ± 2.13 × 10*9/L. Mean absolute leukocyte count 28 days after the first natalizumab infusion was 7.6 ± 2.4 × 10*9/L. Mean absolute leukocyte count 1 year after the beginning of natalizumab treatment was 7.61 ± 2.39 × 10*9/L. No significant increase in leukocytosis after 1 month (p = 0.09), and after 1 year (p = 0.07), appeared.
Significant increases in relative lymphocytosis after 1 month, with a median of 40.4% (− 34.1 to + 145.5%) (p < 0.001) and after 1 year (49.0% (− 9.3 to + 127.6%)) (p < 0.001) were found. No significant increase in relative lymphocytosis occurred from the first month to the first year of the treatment (8.5% (− 31 to + 79%)) (p = 0.12) (Fig. 1).

Box plots of absolute lymphocyte count before, then 1 month and 1 year after natalizumab treatment. Minima appear at the tips of the lower whiskers. The median marks the mid-point of the data and is shown by the line that divides the box into two parts. Maxima appear at the tips of the upper whiskers. Outliers are plotted as individual dots. Mean absolute lymphocyte count before first natalizumab infusion was 2.09 ± 0.74 × 10*9/L. Mean absolute lymphocyte count 28 days after the first natalizumab infusion was 3.24 ± 0.78 × 10*9/L. Mean absolute lymphocyte count after 1 year of the beginning of natalizumab treatment was 3.7 ± 0.89 × 10*9/L. There are significant increases in relative lymphocytosis after 1 month (p < 0.001), and after 1 year of natalizumab treatment (p < 0.001)
No significant difference in natalizumab-induced lymphocytosis (NIL) level was found between the patients exhibiting NEDA-3 status and those without it. The median increase in relative lymphocytosis after 1 month in patients exhibiting NEDA-3 status over the whole follow-up period was 40.5% (− 17.7 to + 105.7%) compared with non-NEDA-3 patients, for whom the figure was 40.3% (− 34.1 to + 145.5%) (p = 0.9): in relative lymphocytosis after 1 year in patients exhibiting NEDA-3 status (52.2% (− 9.3 to + 127.2%)) compared with non-NEDA-3 patients (46.8% (− 9.3 to + 127.2%)) (p = 0.56).
ARR during natalizumab treatment did not correlate with NIL after 1 month (r = 0.167; p = 0.3) and after 1 year (r = 0.213; p = 0.181).
Ten patients (24%) exhibited some seroconversion of JCV index (to seropositivity or seronegativity) during the follow-up period, and significant differences were found after 1 month when comparing NIL between patients JCV-seroconverting (20.6% (− 17.7 to 72.7%)) and stable JCV-seronegative ones (43.5% (− 6.3 to + 96.3%)) (p = 0.04) and also with the stable JCV seropositive-group of patients (50.4% (− 34.1 to + 145.5%)) (p = 0.03). NILs after 1 month in JCV-seroconverting patients were lower compared with patients of stable JCV serostatus (positive or negative) (46.8% (− 34.1 to + 145.5%)) (p = 0.024) (Fig. 2).

Box plots show that NIL after 1 month in JCV-seroconverting patients was lower compared with patients of stable JCV serostatus (positive or negative) (p = 0.024). Minima appear at the tips of the lower whiskers. The median marks the mid-point of the data and is shown by the line that divides the box into two parts. Maxima appear at the tips of the upper whiskers. JCV, John Cunningham virus; NIL, natalizumab-induced lymphocytosis
A significant difference emerged when comparing NIL after 1 year of natalizumab treatment in JCV-seroconverting patients (33.7% (+ 3.5 to 67.4%)) with stable JCV-seropositive ones (62.1% (− 9.3 to + 127.6%)) (p = 0.04) but not in the stable JCV-seronegative group of patients (46.3% (+ 14.6 to + 121.7%)) (p = 0.21). NILs after 1 year of natalizumab treatment in JCV-seroconverting patients were 33.7% (+ 3.5 to 67.4%) compared with patients of stable JCV serostatus (positive or negative) (54% (− 9.3 to + 127.6%)) (p = 0.11).
No significant correlations were found between JCV index and NIL after 1 month (r = − 0.025; p = 0.878) and NIL after 1 year (r = 0.033; p = 0.837).
No difference between groups was found in comparison of disease duration and natalizumab treatment duration.
Lymphocyte subsets (CD3+, CD3+CD4+, CD3+CD8+) and CD4/CD8 ratio were established by flow cytometry in the entire cohort after a mean interval of 6.8 ± 3.2 years of natalizumab treatment (mean age 43.2 ± 6.7 years). The mean relative CD4+ lymphocyte count was 63.2 ± 8.2%, and the mean relative CD8+ T lymphocyte count was 32.7 ± 7.9%. The mean CD4/CD8 ratio was 2.14 ± 0.94; this did not correlate with JCV index (r = 0.033; p = 0.82), natalizumab treatment duration (r = 0.107; p = 0.46), disease duration (r = 0.072; p = 0.618), or age of the patients (r = 0.054; p = 0.71). No significant differences in CD4/CD8 ratio were found in comparison of groups of stable JCV-positive (2.25 ± 1.05), stable JCV-negative (2.2 ± 0.98), and JCV-seroconverting patients (1.89 ± 0.58) (p = 0.59). No significant differences were found in comparison of groups of patients with stable JCV index (2.22 ± 1.02) compared with JCV-seroconverting patients (1.89 ± 0.58) (p = 0.4). Patients who maintained NEDA-3 status over the whole period of the natalizumab treatment exhibited a lower CD4/CD8 ratio (1.89 ± 1.08 vs. 2.5 ± 0.73; p < 0.04) and lower relative CD4+ T lymphocytes (60.9 ± 7.1% vs. 66.5 ± 8.4%) and higher relative CD8+ lymphocytes (34.7 ± 7.2% vs. 30.0 ± 8.0%). ARR on natalizumab treatment correlated with CD4/CD8 ratio (r = 0.356; p = 0.021).
Discussion
Natalizumab, the first monoclonal antibody for MS therapy targeting α4β1 integrin, is a highly active therapy for patients with severe relapsing MS. The current study aimed to establish reliable biomarker(s) for clinical efficacy and risk of JCV seroconversion in a cohort of 41 RRMS patients treated with natalizumab. A lower CD4/CD8 ratio correlated with better clinical response to natalizumab, while JCV-seroconverting patients suffered a lower level of natalizumab-induced lymphocytosis than patients with stable JCV index serostatus.
Among the limitations of this study, it must be accepted that it involved a relatively low number of subjects, a result of the single-center design. A further limitation may be found in the CD4/CD8 ratio, which was not evaluated longitudinally. The MRI protocol was not uniform (including gadolinium administration) over the follow-up in the whole cohort due to a retrospective study design.
The CD4/CD8 ratio was reduced in the CSF of PML patients receiving natalizumab [25], suggesting that a low ratio could be associated with a higher likelihood of the acquisition of pathogenic JCV variants that evade immune surveillance over time [29] and lead to PML. However, no significant correlation of CD4/CD8 ratio with JCV index emerged in this study. No significant difference between groups in terms of CD4/CD8 ratio and JCV stable positivity, negativity, or seroconversion was found.
The importance of lymphocyte subset modifications as a biomarker of natalizumab treatment efficacy in MS has been reported [8]; this corresponds with the data herein, indicating that natalizumab acts on immune cell circulation, altering T cell balance. The CD4/CD8 ratio should thus be monitored carefully in natalizumab-treated patients as a possible marker of response to this treatment. During such treatment, an inversion of the white blood cell count with lymphocytosis has been demonstrated [30] as a result of sequestration of lymphocytes [6], confirmed by an increase in NK cells, B cells, CD4+, and/or CD8+ T lymphocytes, with no change in the CD4/CD8 T cell ratio during treatment. In this study, it emerged that the CD4/CD8 ratio was lower in natalizumab-treated patients with better clinical response to immunomodulating therapy. A previous study suggests that this ratio difference increases in the first 12 months of natalizumab treatment [29].
The CD4/CD8 ratio might well be a possible biomarker for clinical efficacy in natalizumab treatment because patients exhibiting NEDA-3 status over the whole period of natalizumab treatment herein exhibited a lower CD4/CD8 ratio, and also patients with lower ARR had lower CD4/CD8 ratios, something that may indicate a better clinical effect of natalizumab in patients with lower CD4/CD8 (as a possible marker of efficacy of natalizumab).
Referring to the literature evidence [23] in the cohort studied herein, a significant difference was observed between the baseline percentage of lymphocytes and the percentage 4 weeks after the first natalizumab administration, an average increase of 40.4%, which might reflect the early biological action of the drug. No difference was observed in overall leukocyte blood count after the commencement of natalizumab treatment, which correlates with a selective lymphocyte effect [6].
Previous studies have suggested (e.g., Signoriello et al., 2015 [8]) that NIL may be a biomarker of therapeutic efficacy in patients with multiple sclerosis treated with natalizumab, and that the risk of a clinical or instrumental relapse may be higher in patients with a lower-than-expected NIL. High levels of lymphocytes during treatment reduced the risk of an early reactivation after treatment discontinuation [31], arising out of ongoing effects of lymphocytosis, especially by CD4+ and CD8+ lymphocytes, even after discontinuation of the drug. In the cohort herein, NIL did not correlate with long-term therapeutic efficacy in patients treated with natalizumab. No significant signs that NIL could be a reliable biomarker for natalizumab therapeutic efficacy emerged. The contrasting results of our study may be due to a different cohort—progressive-relapsing MS patients [8] were not included in this study, and also the cohort herein exhibited a higher increase of lymphocytes after 4 weeks (18.75% vs. 40.4%).
JCV-seroconverting patients showed lower NIL than patients with stable JCV index serostatus. These patients may be at higher risk of JCV seroconversion and possibly greater risk of PML. The relationship between natalizumab-induced lymphocytosis and JCV index, including the risk of seroconversion, has not yet been investigated in previous studies, so these data are unique. The patients who exhibited lower reactivity of the immune system, demonstrated by a lower level of NIL, lie in contrast with the higher proportion of JCV index seroconversion of these patients. The pathogenic mechanism and links between NIL and JCV index seroconversion are not yet fully understood.
Conclusion
This contribution reports the CD4/CD8 ratio as a possible biomarker for better clinical efficacy of natalizumab in patients exhibiting a lower CD4/CD8 ratio. Compared to the previous study [8], NIL did not correlate with long-term therapeutic efficacy in patients treated with natalizumab, but was demonstrated as lower in patients JCV-seroconverting in the course of follow-up.
References
Butzkueven H, Kappos L, Pellegrini F, Trojano M, Wiendl H, Patel RN, Zhang A, Hotermans C, Belachew S, on behalf of the TYSABRI Observational Program (TOP) Investigators (2014) Efficacy and safety of natalizumab in multiple sclerosis: interim observational programme results. J Neurol Neurosurg Psychiatry 85:1190–1197. https://doi.org/10.1136/jnnp-2013-306936
Puthenparampil M, Cazzola C, Zywicki S et al (2018) NEDA-3 status including cortical lesions in the comparative evaluation of natalizumab versus fingolimod efficacy in multiple sclerosis: therapeutic advances in neurological disorders. https://doi.org/10.1177/1756286418805713
Engelhardt B, Kappos L (2008) Natalizumab: targeting α4-integrins in multiple sclerosis. NDD 5:16–22. https://doi.org/10.1159/000109933
Camponeschi A, Gerasimcik N, Wang Y, Fredriksson T, Chen D, Farroni C, Thorarinsdottir K, Sjökvist Ottsjö L, Aranburu A, Cardell S, Carsetti R, Gjertsson I, Mårtensson IL, Grimsholm O (2019) Dissecting integrin expression and function on memory B cells in mice and humans in autoimmunity. Front Immunol 10. https://doi.org/10.3389/fimmu.2019.00534
Kim TK, Billard MJ, Wieder ED, McIntyre BW, Komanduri KV (2010) Co-engagement of α4β1 integrin (VLA-4) and CD4 or CD8 is necessary to induce maximal Erk1/2 phosphorylation and cytokine production in human T cells. Hum Immunol 71:23–28. https://doi.org/10.1016/j.humimm.2009.09.360
Frisullo G, Iorio R, Plantone D, Marti A, Nociti V, Patanella AK, Batocchi AP (2011) CD4+T-bet+, CD4+pSTAT3+ and CD8+T-bet+ T cells accumulate in peripheral blood during NZB treatment. Mult Scler 17:556–566. https://doi.org/10.1177/1352458510392263
Neumann F, Zohren F, Haas R (2009) The role of natalizumab in hematopoietic stem cell mobilization. Expert Opin Biol Ther 9:1099–1106. https://doi.org/10.1517/14712590903055011
Signoriello E, Lanzillo R, Morra VB et al (2015) Lymphocytosis as a response biomarker of natalizumab therapeutic efficacy in multiple sclerosis. Mult Scler J. https://doi.org/10.1177/1352458515604381
Bloomgren G, Richman S, Hotermans C, Subramanyam M, Goelz S, Natarajan A, Lee S, Plavina T, Scanlon JV, Sandrock A, Bozic C (2012) Risk of natalizumab-associated progressive multifocal leukoencephalopathy. N Engl J Med 366:1870–1880. https://doi.org/10.1056/NEJMoa1107829
Ferenczy MW, Marshall LJ, Nelson CDS, Atwood WJ, Nath A, Khalili K, Major EO (2012) Molecular biology, epidemiology, and pathogenesis of progressive multifocal leukoencephalopathy, the JC virus-induced demyelinating disease of the human brain. Clin Microbiol Rev 25:471–506. https://doi.org/10.1128/CMR.05031-11
McGuigan C, Craner M, Guadagno J, Kapoor R, Mazibrada G, Molyneux P, Nicholas R, Palace J, Pearson OR, Rog D, Young CA (2016) Stratification and monitoring of natalizumab-associated progressive multifocal leukoencephalopathy risk: recommendations from an expert group. J Neurol Neurosurg Psychiatry 87:117–125. https://doi.org/10.1136/jnnp-2015-311100
Olsson T, Achiron A, Alfredsson L et al (2013) Anti-JC virus antibody prevalence in a multinational multiple sclerosis cohort. Mult Scler J. https://doi.org/10.1177/1352458513477925
Tan CS, Koralnik IJ (2010) Progressive multifocal leukoencephalopathy and other disorders caused by JC virus: clinical features and pathogenesis. Lancet Neurol 9:425–437. https://doi.org/10.1016/S1474-4422(10)70040-5
Gorelik L, Lerner M, Bixler S, Crossman M, Schlain B, Simon K, Pace A, Cheung A, Chen LL, Berman M, Zein F, Wilson E, Yednock T, Sandrock A, Goelz SE, Subramanyam M (2010) Anti-JC virus antibodies: implications for PML risk stratification. Ann Neurol 68:295–303. https://doi.org/10.1002/ana.22128
Aladro Y, Terrero R, Cerezo M, Ginestal R, Ayuso L, Meca-Lallana V, Millán J, Borrego L, Martinez-Ginés M, Rubio L, de Andrés C, Miralles A, Guijarro C, Rodríguez-García E, García-Dominguez JM, Muñoz-Fernández C, López de Silanes C, Gómez M, Thuissard I, Cerdán M, Palmí I, Díaz-Garzón LF, Meca-Lallana J (2016) Anti-JC virus seroprevalence in a Spanish multiple sclerosis cohort: JC virus seroprevalence in Spain. J Neurol Sci 365:16–21. https://doi.org/10.1016/j.jns.2016.03.050
Bozic C, Richman S, Plavina T, Natarajan A, Scanlon JV, Subramanyam M, Sandrock A, Bloomgren G (2011) Anti-John Cunningham virus antibody prevalence in multiple sclerosis patients: baseline results of STRATIFY-1. Ann Neurol 70:742–750. https://doi.org/10.1002/ana.22606
Hegen H, Auer M, Bsteh G, di Pauli F, Plavina T, Walde J, Deisenhammer F, Berger T (2017) Stability and predictive value of anti-JCV antibody index in multiple sclerosis: a 6-year longitudinal study. PLoS One 12:e0174005. https://doi.org/10.1371/journal.pone.0174005
Kolasa M, Hagman S, Verkkoniemi-Ahola A, Airas L, Koivisto K, Elovaara I (2016) Anti-JC virus seroprevalence in a Finnish MS cohort. Acta Neurol Scand 133:391–397. https://doi.org/10.1111/ane.12475
Kolcava J, Hulova M, Benesova Y, Bednarik J, Stourac P (2019) The value of anti-JCV antibody index assessment in multiple sclerosis patients treated with natalizumab with respect to demographic, clinical and radiological findings. Mult Scler Relat Disord 30:187–191. https://doi.org/10.1016/j.msard.2019.02.019
Outteryck O, Zéphir H, Salleron J et al (2013) JC-virus seroconversion in multiple sclerosis patients receiving natalizumab. Mult Scler J. https://doi.org/10.1177/1352458513505353
Vennegoor A, van Rossum JA, Leurs C, Wattjes MP, Rispens T, Murk JLAN, Uitdehaag BMJ, Killestein J (2016) High cumulative JC virus seroconversion rate during long-term use of natalizumab. Eur J Neurol 23:1079–1085. https://doi.org/10.1111/ene.12988
Iannetta M, Zingaropoli MA, Bellizzi A, Morreale M, Pontecorvo S, D’Abramo A, Oliva A, Anzivino E, Lo Menzo S, D’Agostino C, Mastroianni CM, Millefiorini E, Pietropaolo V, Francia A, Vullo V, Ciardi MR (2016) Natalizumab affects T-cell phenotype in multiple sclerosis: implications for JCV reactivation. PLoS One 11:e0160277. https://doi.org/10.1371/journal.pone.0160277
Koudriavtseva T, Sbardella E, Trento E, Bordignon V, D'Agosto G, Cordiali-Fei P (2014) Long-term follow-up of peripheral lymphocyte subsets in a cohort of multiple sclerosis patients treated with natalizumab. Clin Exp Immunol 176:320–326. https://doi.org/10.1111/cei.12261
Stüve O, Marra CM, Jerome KR et al (2006) Immune surveillance in multiple sclerosis patients treated with natalizumab. Ann Neurol 59:743–747. https://doi.org/10.1002/ana.20858
Warnke C, Stettner M, Lehmensiek V et al (2014) Natalizumab exerts a suppressive effect on surrogates of B cell function in blood and CSF. Mult Scler J. https://doi.org/10.1177/1352458514556296
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, Correale J, Fazekas F, Filippi M, Freedman MS, Fujihara K, Galetta SL, Hartung HP, Kappos L, Lublin FD, Marrie RA, Miller AE, Miller DH, Montalban X, Mowry EM, Sorensen PS, Tintoré M, Traboulsee AL, Trojano M, Uitdehaag BMJ, Vukusic S, Waubant E, Weinshenker BG, Reingold SC, Cohen JA (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17:162–173. https://doi.org/10.1016/S1474-4422(17)30470-2
Kister I, Kuesters G, Chamot E, Omari M, Dontas K, Yarussi M, Subramanyam M, Herbert J (2014) IV immunoglobulin confounds JC virus antibody serostatus determination. Neurol Neuroimmunol Neuroinflamm 1:e29. https://doi.org/10.1212/NXI.0000000000000029
Lee P, Plavina T, Castro A, Berman M, Jaiswal D, Rivas S, Schlain B, Subramanyam M (2013) A second-generation ELISA (STRATIFY JCV™ DxSelect™) for detection of JC virus antibodies in human serum and plasma to support progressive multifocal leukoencephalopathy risk stratification. J Clin Virol 57:141–146. https://doi.org/10.1016/j.jcv.2013.02.002
Carotenuto A, Scalia G, Ausiello F, Moccia M, Russo CV, Saccà F, de Rosa A, Criscuolo C, del Vecchio L, Brescia Morra V, Lanzillo R (2017) CD4/CD8 ratio during natalizumab treatment in multiple sclerosis patients. J Neuroimmunol 309:47–50. https://doi.org/10.1016/j.jneuroim.2017.05.006
Sangalli F, Moiola L, Bucello S, Annovazzi P, Rizzo A, Radaelli M, Vitello G, Grimaldi LME, Ghezzi A, Martinelli V, Comi G (2011) Efficacy and tolerability of natalizumab in relapsing-remitting multiple sclerosis patients: a post-marketing observational study. Neurol Sci 31(Suppl 3):299–302. https://doi.org/10.1007/s10072-010-0344-z
Rossi S, Motta C, Studer V, Monteleone F, de Chiara V, Buttari F, Barbieri F, Bernardi G, Battistini L, Cutter G, Stüve O, Salvetti M, Centonze D (2013) A genetic variant of the anti-apoptotic protein Akt predicts natalizumab-induced lymphocytosis and post-natalizumab multiple sclerosis reactivation. Mult Scler 19:59–68. https://doi.org/10.1177/1352458512448106
Acknowledgments
Tony Long (Dalmellington) helped work up the English.
Funding
This work was supported by the Ministry of Health of the Czech Republic, ref. - RVO (FNBr, 65269705), and the project of specific research ref. MUNI/A/1325/2019 from the program of support of student projects at Masaryk University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
The research was approved by the local ethics committees.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kolcava, J., Hulova, M., Rihova, L. et al. The impact of lymphocytosis and CD4/CD8 ratio on the anti-JCV antibody index and clinical data in patients treated with natalizumab. Neurol Sci 42, 2847–2853 (2021). https://doi.org/10.1007/s10072-020-04897-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-020-04897-2