
Abstract
Background and aims
Stroke is a leading cause of death and disability worldwide. However, our knowledge of the incidence of stroke for Saudi Arabian population is not known. Thus, we aimed to determine the pooled annual incidence of stroke in Saudi Arabia.
Summary of review
We conducted a comprehensive literature search of PubMed, Web of Science, and SCOPUS, without language or publication year limits. Outcomes of interest were stroke incidence rate for both first and recurrent. A total of five studies met the inclusion criteria for this review. The pooled annual incidence of stroke in Saudi Arabia was 0.029% (95% CI: 0.015 to 0.047) equivalent of 29 strokes per 100,000 people annually (95% CI: 15 to 47).
Conclusion
The findings indicate that there are 29 stroke cases for every 100,000 people annually for individuals residing Saudi Arabia. Our values were lower than those of other high-income countries. Establishing a nationwide stroke registry is warranted for monitoring and improving healthcare services provided to stroke survivors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite the medical and rehabilitation advances, stroke is still a leading cause of mortality and disability worldwide [1]. The World Health Organization defined stroke as “rapidly developing clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 h or leading to death, with no apparent cause other than that of vascular origin” [2]. Sustaining a stroke imposes a huge financial burden that impacts individuals as well as the health care system worldwide. The estimated cost of care for stroke survivors in the United States is approximately $34 billion each year and expected to increase [3]. In England, the economic cost of stroke is around £7 billion a year [4]. In Saudi Arabia, there are no available data about the cost of care for stroke survivors; however, cost is likely to be high given that the healthcare services are primarily government-funded.
There has been conflicting evidence regarding the incidence of stroke in Saudi Arabia. One study found the incidence of stroke to be 29.8 cases per 100,000 people [5], while another study found the incidence of stroke to be 43.8 cases per 100,000 people [6]. A third study conducted in a rural area of Saudi Arabia found the incidence of stroke to be 15.1 cases per 100,000 people [7].
There are claims that the rate of incidence of stroke is less than the western countries due to the younger age group in Saudi Arabia. However, this is primarily attributed to the limited data on the incidence of stroke in Saudi Arabia.
The majority of the available pertaining to the nationwide incidence of stroke are exclusive to a single community-based hospital where the attendees are a specified group of the community [6,7,8]. Examining these studies may help explain the variation in the findings. For example, there were differences in the methodologies used. Both were retrospective studies but the durations were different, with one study lasting 10 years [6] and the other study lasting 5 years [8]. While these studies were useful regionally, they do not give a full representation of the incidence of stroke in Saudi Arabia.
Determining the true incidence of stroke would help the health care systems to properly monitor the incidence of stroke nationwide, to audit the cost of care for stroke patients, and to generate solutions for preventing and reducing the incidence of stroke nationwide. Therefore, the aim of this study was to conduct a systematic review and meta-analysis to determine the pooled annual incidence of stroke among Saudi adults.
Methods
Protocol
The systematic review protocol was registered in PROSPERO (CRD42018094539). The presentation of the results from this systematic review and meta-analysis follows the PRISMA guidelines [9].
Eligibility criteria
Eligible studies for this review were (1) published as observational studies, (2) conducted in Saudi Arabia, and (3) included as a registry of stroke incidence rate of stroke either recurrent or first-time stroke.
Search strategy
We performed a computerized systematic literature search of PubMed, Web of Science, and SCOPUS up to September 2019, without language or publication year limits to capture all possible relevant titles. The key words and phrases (in different combinations) searched were stroke, cerebrovascular accident, CVA, hemorrhage, incidence, and ischemic stroke. The search was limited to studies conducted in Saudi Arabia. References listed in included studies were also used to identify additional eligible studies.
Study selection
Studies were evaluated for meeting the eligibility criteria. All studies conducted in Saudi Arabia that were examining the incidence of stroke were selected for review. The main reviewed outcome was stroke incidence rate. Screening of eligible studies was conducted by two of the authors (BA and AA). Disagreements regarding eligibility were resolved by a third reviewer (MA).
Data extraction and quality assessment
A double coding approach was implemented to extract data. Two of the investigators (BA and AA) extracted data using a standardized data extraction form. Any disagreements were discussed until a consensus was reached. The quality of included studies was assessed using the Newcastle-Ottawa Quality Assessment Scale [10]. The scale examined three areas including study group selection, group comparability, and outcome of interest. The final maximum score was 9 stars for the nonrandomized studies. A consensus between reviewers was reached in the case of any scoring discrepancies.
Data synthesis and analysis
A random-effects meta-analysis on annual stroke incidence in Saudi Arabia was conducted according to guidelines set forth by Lipsey and Wilson [11] as well as Barendregt et al. [12] Because the stroke incidence rates are close to zero numerically, the observed stroke incidence rates were transformed for meta-analysis using a double arcsine transformation so that the limits of the confidence intervals are between zero and one and so that the variance estimates are not distorted [12]. The double arcsine transformed data are presented in the forest plot for clarity of presentation. After conducting the meta-analysis, the pooled stroke incidence estimate is back transformed to a traditional percentage and then to the rate per 100,000 people annually for presentation to the reader.
Because of the small number of eligible studies, it is not feasible to use risk factors to account for between-study variance using meta-regression. Consequently, there is no way to empirically examine what accounts for between-study variance. The stated risk factors can be narratively reviewed so that future research studies and future meta-analyses can further explore the impact of the identified risk factors and stroke incidence when more studies are available. The meta-analyses were conducted in R [13].
Results
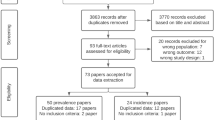
The literature search resulted in a total of 2268 studies (PubMed: 1052, Web of Science: 877, and SCOPUS: 339), of which a full text of 17 studies were identified and only 5 studies were eligible to be included in the meta-analyses. Figure 1 presents the complete selection process for this systematic review and meta-analysis. The main reason of the excluded studies is that studies did not provide numerical estimates on incidence of stroke.

Flowchart of the systemtic review and meta-analysis according to the PRISMA guidelines
The sample size in the included studies ranged between 164 and 1249 (mean age of 64.6 years, 60% male). All five included studies were cross-sectional and only examined the incidence of first stroke [14]. Only one study [14] was conducted in the western region of Saudi Arabia, and no studies have been conducted in the northern region of Saudi Arabia. The recruitment period for the included studies ranged from 12 months to 10 years. The total incidence rate per 100,000 people ranged from 13.9 to 57.6 (Table 1).
Using double arcsine units, the meta-analysis revealed a pooled estimate of 0.034 (95% CI: 0.024 to 0.043). The pooled estimate was statistically significant (Z = 7.09, p < 0.001). There was significant between-study heterogeneity (I2 = 98.97). Figure 2 presents the forest plot for these findings.

Forest plot of the observed stroke prevalence
Because double arcsine units are not intuitively interpretable, these can be back transformed to proportions and the incidence rate per 100,000 people annually. After converting the pooled estimate and confidence interval limits to proportions, the pooled estimate proportion was 0.029% (95% CI: 0.015 to 0.047). The stroke incidence rate per 100,000 people annually was 29 strokes per 100,000 people annually (95% CI: 15 to 47).
Discussion
This study aimed to determine the pooled annual incidence of stroke among people in Saudi Arabia. Our findings suggest that there are 29 stroke cases for every 100,000 people annually for individuals between mean age of 2.2 and 67.5 years.
A notable difference in the studies reviewed in this paper was the variability in the definition of stroke and diagnostic process of stroke. The majority of studies used the WHO definition of stroke or definitions that are closely similar to it [14, 15, 17]. This variation is expected due to the wide range of definitions in the literature. However, the inconsistency in the stroke definitions may lead to low internal validity and misleading results. For the diagnostic process, some studies used imaging approaches to confirm the stroke incidence such as computed tomography (CT) scan, magnetic resonance imaging (MRI), or angiography plus CT [14,15,16], whereas others used hematologic and biochemical investigation [6, 15]. One study used sign and symptoms of stroke as inclusion criteria and then utilized high evaluation procedure including CT and MRI for further investigation [17].
Four out of seven studies excluded people who were not from the targeted region based on the nationality [14,15,16,17]; however, Saudi visitors from different regions might be included. Three studies [6, 7] included all people who admitted to the hospital, but it is expected that several patients were transferred from outside the region or being a visitor. Thus, we recommend future epidemiological researches to consider the original region and length of stay in the analysis to clarify the incidence of stroke based on nationality and place of residence. In addition, all studies excluded previous stroke except three studies [6, 7] which might be not be ideal to account for the epidemiology of specific disease. Including all type of stroke and expanding the analysis to include sub-categories such as first stroke and recurrent stroke will help in understanding the nature of disease incidence.
The current study findings showed that the incidence of stroke is lower than other populations. Our results after excluding stroke in children revealed that only 32 stroke cases for every 100,000 persons annually. This incidence rate in the current study was much lower recent pooled estimates from different countries and regions [18]. Previous evidence has estimated the incidence of stroke in China to be 354 cases per 100,000 people compared to 32 cases in our study. Furthermore, the lowest estimate of stroke incidence between countries was in central Latin America, specifically El Salvador by 97 cases per 100,000 people, and this estimate is higher than our pooled incidence rate (only 32 stroke cases for every 100,000 persons). Therefore, the incidence of stroke is relatively in Saudi Arabia that is lower than other countries, and this requires further population-based studies to confirm our findings.
Considering environmental factor as a potential risk factor of stroke [19], two studies were conducted in the Southern region of Saudi Arabia [7, 16], one study in the Western region [14], two studies in the Eastern region [15, 17], and two studies in the Central region (one in the National Guard of the Central region [6]. There are total six provinces in Saudi Arabia with varied population rates, and we assumed that the results of this meta-analysis generalize to the majority of these provinces. However, due to low sample sizes and study sites, we recommend future epidemiological research to investigate the rate incidence of stroke on large databases using population-based cohort study that covers all regions in Saudi Arabia.
Aging is a risk factor of stroke [19], as most of the studies recruited wide range of ages and showed increasing in the incidence rate of stroke with aging [6, 7, 14,15,16]. These studies and our meta-analysis were consistent with different studies that are established in Europe [20], United States [21], Africa [22], Asia [23], and global burden [24]. A previous study showed that the lowest age-standardized incidence rate of stroke was in Saudi Arabia as this rate is lower than most studies established in Western countries [5]. We observed low incidence rate of stroke via adjusting pooled estimates in all seven reviewed studies. The low incidence rate of stroke might be due to low sample sizes in the included studies.
It is of importance to indicate that some studies used a wide range of time of recruitment [6, 15], which might eventually end up with larger number of incidences compared to short period studies within 5-year period [17] or < 2-year period [7, 14, 16]. We were not able to conduct sub-analysis based on data duration because of the low reviewed studies, and we recommend future studies to account for that.
Limitations
This meta-analysis only examined a small number of studies. Consequently, the results of this meta-analysis should be verified once there are more studies on the issue. Additionally, the small number of included studies prevented tests of publication bias from being used. Future meta-analyses on the incidence of stroke in Saudi Arabia should attempt to assess for publication bias in their findings. Although we used conservative approach in the meta-analysis [25] to overcome the issue of study heterogeneity, the findings of this meta-analysis should be interpreted with caution. The level of heterogeneity across study review might be related to study design, region of data collection, stroke definition, inclusion and exclusion criteria, and recruitment period. The design of studies reviewed in this paper is retrospective [6, 7], and prospective data [14, 16, 17] (i.e., one study used data retrospectively and prospectively). Both designs are suitable and reliable for observational studies; however, using longitudinal prospective design may overcome multiple issues such as selection bias and data entry errors [26]. The studies included in this paper were conducted in disparate regions across Saudi Arabia; hence, there may be differential base rates of stroke across the country. Finally, the occurrence of reported risk factors may be different between study samples, which may lead to differing levels of stroke incidence between studies.
Conclusion
This systematic review and meta-analysis is the first to describe the pooled annual incidence of stroke in Saudi Arabia. The findings of this study indicate that there are 29 stroke cases for every 100,000 people annually for individuals between mean age of 2.2 and 67.5 years. Establishment of nationwide stroke registry is warranted for monitoring and improving healthcare services provided to stroke survivors.
References
Mendis S, Puska P, Norrving B (2011) Global atlas on cardiovascular disease prevention and control. World Health Organ:2–14
Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T (1980) Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ 58(1):113–130
Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R et al Heart Disease and Stroke Statistics 2017 At-a-Glance. Circulation. 2017:1–5
Morse A. Department of Health: Progress in improving stroke care. Natl Audit Off Rep. 2010;(February)
Tran J, Mirzaei M, Anderson L, Leeder SR (2010) The epidemiology of stroke in the Middle East and North Africa. J Neurol Sci 295(1–2):38–40
al Rajeh S, Awada A, Niazi G, Larbi E (1993) Stroke in a Saudi Arabian National Guard Community: analysis of 500 consecutive cases from a population-based hospital. Stroke. 24(11):1635–1639
Ayoola AE, Banzal SS, Elamin AK, Gadour MO, Elsammani EW, Al-Hazmi MH (2003) Profile of stroke in Gizan, Kingdom of Saudi Arabia. Neurosciences 8(4):229–232
Almekhlafi MA (2016) Trends in one-year mortality for stroke in a tertiary academic center in Saudi Arabia: a 5-year retrospective analysis. Ann Saudi Med 36(3):197–202
Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (Chinese edition). J Chin Integr Med 7:889–896
Wells GA O’Connell D. B Shea. The Newcastle-Scale for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Ottawa Hosp Res Inst. 2011;
Lipsey MW, Wilson DB (2001) Practical meta-analysis. Appl Soc Res Methods Ser 49:264
Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T (2013) Meta-analysis of prevalence. J Epidemiol Community Health 67(11):974–978
(2019) R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing
Al-Shenqiti AM, Ibrahim SR, Khaled OA, Ali ARH, Ahmed MS (2017) Incidence of first time stroke: a Saudi experience. Eur Neurol 77(3–4):147–151
Al-Rajeh S, Larbi EB, Bademosi O, Awada A, Yousef A, Al-Freihi H et al (1998) Stroke register: experience from the Eastern Province of Saudi Arabia. Cerebrovasc Dis 8(2):86–89
Alhazzani AA, Mahfouz AA, Abolyazid AY, Awadalla NJ, Aftab R, Faraheen A et al (2018) Study of stroke incidence in the aseer region, southwestern Saudi Arabia. Int J Environ Res Public Health (2):15
Al-Sulaiman A, Bademosi O, Ismail H, Magboll G (1999) Stroke in Saudi children. J Child Neurol 14(5):295–298
GBD 2016 Stroke Collaborators (2019) Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 18(5):439–458. https://doi.org/10.1016/S1474-4422(19)30034-1
Giampaoli S, Hammar N, Adany R, De Peretti C (2007) Population-based register of stroke: manual of operations. Eur J Cardiovasc Prev Rehabil 14(SUPPL. 3)
Béjot Y, Bailly H, Durier J, Giroud M (2016) Epidemiology of stroke in Europe and trends for the 21st century. Presse Medicale 45:e391–e398
Cushman M, Cantrell RA, McClure LA et al (2008) Estimated 10-year stroke risk by region and race in the United States: geographic and racial differences in stroke risk. Ann Neurol 64(5):507–513. https://doi.org/10.1002/ana.21493
Connor M (2004) Prevalence of stroke survivors in rural South Africa: results from the Southern Africa Stroke Prevention Initiative (SASPI) Agincourt Field Site. Stroke. 35(3):627–632
Kulshreshtha A, Anderson LM, Goyal A, Keenan NL (2012) Stroke in South Asia: a systematic review of epidemiologic literature from 1980 to 2010. Neuroepidemiology 38:123–129
Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, Moran AE, Sacco RL, Anderson L, Truelsen T, O'Donnell M, Venketasubramanian N, Barker-Collo S, Lawes CMM, Wang W, Shinohara Y, Witt E, Ezzati M, Naghavi M, Murray C (2014) Global and regional burden of stroke during 1990-2010: findings from the global burden of disease study 2010. Lancet. 383(9913):245–255
Doi SAR, Barendregt JJ, Khan S, Thalib L, Williams GM (2015) Advances in the meta-analysis of heterogeneous clinical trials I: the inverse variance heterogeneity model. Contemp Clin Trials 45:130–138
Euser AM, Zoccali C, Jager KJ, Dekker FW (2009) Cohort studies: prospective versus retrospective. Nephron Clin Pract 113
Funding
This study was supported by the deanship of scientific research at Prince Sattam bin Abdulaziz University under the project # 2019/03/10805.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Alqahtani, B.A., Alenazi, A.M., Hoover, J.C. et al. Incidence of stroke among Saudi population: a systematic review and meta-analysis. Neurol Sci 41, 3099–3104 (2020). https://doi.org/10.1007/s10072-020-04520-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-020-04520-4