
Abstract
Background
The higher level of neutrophil on admission has been reported to predict worse 3-month outcomes in ischemic stroke patients. Our study was to explore the dynamic changes of neutrophil and lymphocyte after r-tPA thrombolysis of ischemic stroke and the relationship with parenchymal hemorrhage (PH) and 3-month function outcome.
Methods
A total of 208 acute ischemic stroke (AIS) patients with intravenous thrombolysis were included and then received 3-month follow-up in the present study. Blood samples for neutrophil and lymphocyte counts were obtained on admission, at 24 h and at 7 days after r-tPA infusion. The associations of increase in neutrophil, lymphocyte, and neutrophil to lymphocyte ratio (NLR) with PH or 3-month poor outcome were examined by logistic regression.
Results
Increasing trends in the neutrophil and NLR were observed in AIS patients after r-tPA treatment. Increased level of neutrophil at 24 h after r-tPA infusion but not that on admission was associated with PH (OR = 2.86, P = 0.029) and 3-month poorer functional outcomes (OR = 2.67, P = 0.009). Moreover, patients were divided into four groups according to the percent change in neutrophil within 24 h following r-tPA treatment, and we found that there was a trend of incremental OR when compared higher increase group with lower ones.
Conclusions
Dynamic increase in neutrophil and NLR after stroke may predict PH and 3-month poor outcome in AIS patients receiving r-tPA treatment. Therefore, neutrophil and NLR may serve as activity markers for PH and 3-month poor prognosis in AIS patients with intravenous thrombolysis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Stroke becomes one of the most common diseases for mortality and morbidity of human being worldwide nowadays [1]. Most stroke survivors leave functional impairments which dramatically decline quality and independence of life [2]. A number of clinical trials have proved the efficacy and benefit of intravenous thrombolysis with recombinant tissue plasminogen activator (r-tPA) in acute ischemic stroke (AIS) patients within 4.5 h from symptom onset [3, 4]. Intravenous administration of r-tPA is now recommended as the primary choice for AIS patients within the time window; nevertheless, approximately half of the participants are still not independent or even died after 3 months. Therefore, although a few factors related to functional outcome of ischemic stroke patients treated with intravenous alteplase has been identified, detection of new risk factors is still necessary and important. Hemorrhagic transformation (HT) is claimed to be one of the major complications leading to poor functional outcomes after thrombolysis. The increased risk of hemorrhagic transformation following ischemic stroke was most likely attributable to the factor of reperfusion and the toxic effects of r-tPA [5].
In recent years, numerous studies have demonstrated that activated inflammatory process may play an important role in the functional outcomes and hemorrhagic transformation [6, 7]. When ischemic stroke occurs, inflammatory mediators such as chemokines and cytokines are released and then promote peripheral leukocytes infiltration. Among the peripheral circulating leukocytes, the neutrophils are firstly recruited to the ischemic area by binding various adhesion molecules in the early stages of ischemic stroke [8]. Moreover, they release matrix metalloproteinase-9 (MMP-9) and induce the damage of blood-brain barrier (BBB), which may induce the hemorrhagic transformation. In addition, the neutrophils have also been demonstrated to be involved in neurogenesis, angiogenesis, and neuroplasticity in neurological recovery stage [9, 10]. Therefore, the activation of neutrophil has been suggested to increase infarct size [11], hemorrhagic transformation, and worse neurologic outcomes [6]. On the other hand, as another type of leukocytes, the lymphocytes also play an important role in the progression of ischemic stroke. Previous studies have reported that lymphocytes count decreases following AIS and lower level of lymphocytes may contribute to poor functional outcome [8]. For example, as a subset of lymphocyte, specific T cell lymphocyte has been demonstrated to exert a neuroprotective effect on central nervous system [12]. Taken together, the neutrophils and lymphocytes may mediate inflammatory processes in different mechanisms after ischemic stroke.
Recent studies have suggested that the level of neutrophil on admission is associated with increased risk of hemorrhage transformation and can predict 3-month clinical outcome after r-tPA thrombolysis [6, 13]. In AIS patients, MMP-9-positive neutrophil infiltration results in disruption of the BBB and degradation of basal lamina type IV collagen [14]. All of these may contribute to the hemorrhage transformation and poor outcome in patients with ischemic stroke. Mao and colleagues observed that regulatory T cell lymphocyte abolish the r-tPA-induced elevation of MMP-9 and CCL2 after stroke, which decrease the risk of hemorrhage transformation [15]. More specifically, neutrophil-to-lymphocyte ratio (NLR) is regarded as a stable systemic inflammation biomarker [16, 17]. The ratio has also been reported to be correlated with short-term poor prognosis in ischemic stroke patients with r-tPA thrombolysis [18]. Nevertheless, these studies only examined neutrophil and lymphocyte before thrombolysis, but the comprehensive dynamic changes of neutrophil and lymphocyte and dynamic inflammatory process in patients with r-tPA thrombolysis have not been investigated.
As a particular type of hemorrhage transformation, parenchymal hemorrhage (PH) can be divided into PH-1 and PH-2. PH-2 is regarded as one of the major factors affecting the prognosis. Therefore, there is an increasing concern about the relation between dynamic changes of neutrophil, lymphocyte, as well as NLR, and the risk of PH and 3-month outcome in AIS patients with r-tPA treatment. In the present study, we aimed to explore the dynamic variation of the neutrophil and lymphocyte in ischemic stroke patients treated with intravenous r-tPA. More importantly, the further goal of current study was to evaluate whether these changes were associated with PH and functional outcome of AIS patients treated with intravenous thrombolysis.
Methods
Study population
A prospective, hospital-based observational study was operated. The study consecutively included consecutive ischemic stroke patients treated with intravenous thrombolysis from July 2016 to July 2018 in the First Affiliated Hospital of Wenzhou Medical University. Intravenous r-tPA (Boehringer Ingelheim, Germany, from 0.9 mg/kg to a maximum of 90 mg) was used with 10% of the total as a bolus within 4.5 h of stroke onset and the rest 90% by a 60-min infusion. The inclusion criteria for enrollment were as follows: (1) older than 18 years old; (2) diagnosis of acute ischemic stroke by neurologists according to the recommendations from World Health Organization [19]; (3) onset-to-treatment time within 4.5 h. The study exclusion criteria were according to AHA/ASA Guidelines [20] and follows: (1) evidence of infection at admission or any systemic infection that occurred during hospitalization; (2) a bridging therapy consisting of IV r-tPA followed by endovascular therapy (3) a history of cancer or autoimmune disease; (4) incomplete medical records and a missing of 3-month prognostic information. The present study was approved by the ethics committee of the First Affiliated Hospital of Wenzhou Medical University. All patients or their relatives signed the informed consent.
Clinical data and blood sample
Some baseline characteristics were collected as follows: age, sex, drinking, smoking, hypertension, diabetes, hyperlipidemia, onset to treatment time (OTT), systolic blood pressure (SBP) before thrombolysis and diastolic blood pressure (DBP) before thrombolysis. Stroke severity was assessed by a certified neurologist using the National Institutes of Health Stroke Scale (NIHSS) at admission and at 24 h, and 7 days after treatment with intravenous r-tPA.
Venous blood samples were obtained from all patients at admission, at 24 h, and 7 days after treatment with intravenous r-tPA. Total leukocyte, neutrophil, and lymphocyte counts were analyzed by the automated hematology analyzer (Sysmex Company, XE-2100, Japan). The NLR was calculated as the ratio of the neutrophils count over lymphocytes count, both obtained from the same blood sample.
Parenchymal hemorrhage and prognosis
All patients received a CT scan within the first 4.5 h of stroke onset. CT was repeated at 24 h, and another CT scan was done immediately in case of rapid neurological deterioration to evaluate the presence of parenchymal hemorrhage. Parenchymal hemorrhage was defined as hemorrhage in the cerebral parenchyma on the CT scan after cerebral ischemic infarction. As a type of hemorrhage transformation, parenchymal hemorrhage can be divided into PH-1 and PH-2. The prognosis after 3 months of AIS was estimated by the Modified Rankin scale (mRS) [21]. According to the mRS scores, the patients were divided into two groups: a good functional outcome for score 0 to 2 and a poor functional outcome for score 3 to 5 or death for the ischemic stroke.
Statistical analysis
The data managements and analyses were applied with SPSS for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA). P < 0.05 was considered statistically significant for all analyses. Categorical variables were presented as counts and percentages, and Fisher’s exact test or chi-squared tests were used as appropriate. Continuous variables not met normal distribution were descripted with median with 25th and 75th percentiles (interquartile ranges (IQR) and compared with Mann-Whitney U test. Normally distributed variables were presented with mean ± standard deviation (SD), and Student’s t test was applied to perform the comparison between two groups. Logistic regression was carried out to find the association between poor clinical outcome and parameters. Variables with a P value of < 0.1 in the univariate analysis were chosen into the multivariate analysis. Results were presented as 95% confidence interval (CI) with odds ratio (OR). According to the percentage change of neutrophil, we divided patients into four group and preformed multivariate analysis.
Results
Baseline characteristics of patients
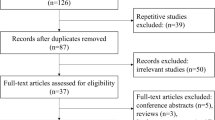
Out of 401 AIS patients treated with r-tPA, 193 patients were excluded due to occurrence of infection including lung infection (n = 62), urinary tract infection (n = 14), and septicemia (n = 4) during hospitalization, bridging therapy (n = 55), losing to follow up (n = 45), and a history of cancer or autoimmune disease (n = 13).
Therefore, we included 208 AIS patients receiving r-tPA (mean age 67 years old, 62% men) in the current study. The main baseline characteristics of patients are presented in Table 1, according to the presence or absence of PH, as well as the outcome at 3 months. We observed that patients with the presence of PH were more likely to suffer from neurological deficits and had more atrial fibrillation than those without PH.
The dynamic changes of neutrophil and lymphocytes following r-tPA treatment
The neutrophil and lymphocytes were obtained at three different time points: at admission, at 24 h, and at 7 days after r-tPA treatment. Figure 1 illustrates the changes in neutrophil, lymphocyte, and NLR at three different time points. Paired Wilcoxon signed-rank test in total participants revealed that neutrophil was significantly increased (median, 4.99 vs. 5.95) whereas lymphocytes were significantly decreased (0.73 vs. 0.71) at 24 h after r-tPA treatment (Fig. 1a, all P < 0.05). Similarly, the NLR was also significantly increased at 24 h after r-tPA infusion (6.97 vs. 8.63, P < 0.001). Nevertheless, neutrophil and NLR were significantly decreased at 7 days when comparing with those at 24 h (all P < 0.001), while lymphocyte was still significantly increased. Moreover, the present study observed that there was no difference in neutrophil count between the good and poor outcome groups at baseline (P = 0.887). At 24 h and at 7 days, neutrophil count was significantly higher in the poor outcome group compared to good outcome group (Fig. 1b, P < 0.001). As for the lymphocyte, there was no significant difference at admission (P = 0.17) and at 24 h (P = 0.25) following r-tPA between these two groups (Fig. 1c). At 7 days, lymphocyte count was significantly higher in the good outcome group compared with the poor outcome group (P < 0.001). Moreover, NLR at baseline between the good and poor outcome groups was not significant difference (P = 0.337). Furthermore, NLR was significantly higher in the poor outcome group compared to good outcome group at 24 h and at 7 days (Fig. 1d, P < 0.001).

Temporal profile (median and interquartile range) of neutrophil, lymphocyte, and NLR in stroke patients treated with r-tPA according to 3-month outcome (b neutrophil, c lymphocyte, d NLR). There was no significant differences in neutrophil, lymphocyte, or NLR on admission between patients with and without poor outcome. Comparing with good outcome group, patients in poor outcome group show higher levers of neutrophil and NLR at 24 h and at 7 days
The temporal profiles of the neutrophil and lymphocytes are presented according to the presence or absence of PH in Fig. 2. The neutrophil at admission did not differ between patients with and without PH (P = 0.661). An increasing trend of the neutrophil was observed in both groups (Fig. 2a). Nevertheless, the neutrophil in the PH group were significantly higher than those in the No PH group at 24 h (P < 0.001) and at 7 days (P = 0.012) after r-tPA. Additionally, there was no significant difference in lymphocyte at admission (P = 0.051), at 24 h (P = 0.154) and at 7 days (P = 0.473) after r-tPA between these two groups (Fig. 2b). Although the NLR at admission did not differ between patients with and without PH (P = 0.231), the NLR values in the PH group were significantly higher than those in the no PH group at 24 h (P < 0.001) and at 7 days after r-tPA (P = 0.041, Fig. 2c).

Temporal profile (median and interquartile range) of neutrophil, lymphocyte, and NLR in stroke patients treated with r-tPA according to PH (a neutrophil, b lymphocyte, c NLR).There was no significant differences in neutrophil, lymphocyte, or NLR on admission between patients with and without PH. Comparing without PH group, patients with PH show higher levers of neutrophil and NLR at 24 h and at 7 days
Prospective associations of neutrophil before and after r-tPA treatment with PH and stroke prognosis
Table 2 summarizes the results of the binary logistic regression analysis of PH and the 3-month outcome. The analysis using cell count before r-tPA treatment as a predictor did not find significant associations of neutrophil, lymphocyte, and NLR with PH or poor functional outcomes after stroke (all P > 0.05). In contrast, the analysis using cell count at 24 h after r-tPA treatment as a predictor showed that neutrophil level was obviously associated with parenchymal hemorrhagic (OR = 2.86, P = 0.029) and 3-month poor outcome (OR = 2.67, P = 0.009). Nevertheless, the changes of lymphocyte were not associated with hemorrhagic transformation and 3-month poor outcome. Moreover, NLR was significantly associated with increased risks for both outcomes (P < 0.05). Additionally, NLR at 7 days was also regarded as a predictor of 3-month outcome (OR = 3.64, P = 0.001). We found the age and NIHSS score also are independent predictors of the 90-day outcome, besides neutrophil and NLR after thrombolysis.
Subgroup analysis on the increase in neutrophil at 24 h after r-tPA treatment
In order to investigate the influence of dynamic changes in neutrophil on PH and 3-month unfavorable outcome, we further subdivided patients into four groups according to the percent change in neutrophil within 24 h after r-tPA treatment: decrease or no change reference group; 0< increase ≤ 25% group; 25%< increase ≤ 50% group; and increase > 50% group. Associations of the percent change in neutrophil within 24 h after r-tPA treatment with PH and stroke prognosis were showed in Table 3. An increase > 25% was found to be associated with an increased risk of PH and 3-month poor outcome when compared to the decrease or no change reference group. More importantly, there was a trend of incremental OR when compared higher increase group with lower ones. Patients with a neutrophil increase > 50% had numerically higher OR compared with patients with a 25%< neutrophil increase ≤ 50%.
Discussion
To the best of our knowledge, this is the first study to document the prognostic value of the dynamic changes of neutrophil and NLR in ischemic stroke patients treated with intravenous thrombolysis. The present study shows that the neutrophil and NLR are significantly elevated at 24 h after r-tPA thrombolysis. More importantly, these dynamic variations are independently associated with increased risks of PH and 3-month poor functional outcomes after r-tPA treatment in AIS patients. Besides the parenchymal hemorrhage, we also found dynamic changes of neutrophil, and NLR are independently associated with increased risks of hemorrhage transformation. Additionally, neutrophil and NLR on day 7 are also associated with poor outcomes in 3 months. Nevertheless, there is no statistically significant association between dynamic lymphocyte and parenchymal hemorrhage or 3-month poor functional outcomes. It also needs to be mentioned that the age and NIHSS score also are independent predictors of the 90-day outcome, which is consistent with previous studies.
In previous studies, higher neutrophil and NLR on admission were found to be independently associated with symptomatic intracerebral hemorrhages (sICH) and worse outcome at 3 months in patients with IV r-tPA treatment [22]. Duan and colleague also showed that the baseline NLR predicts 3-month functional outcome and sICH after endovascular treatment for acute anterior circulation large vessel occlusion stroke patients [23]. Nevertheless, the results of the present study suggested that neutrophil count and NLR, measured before r-tPA thrombolysis, are not reliable predictors of PH and prognosis in acute stroke patients undergoing systemic thrombolysis. The conflicting data presented above, which highlight a controversial role of early neutrophil count and NLR on the outcome, may result from the exclusion of patients with infections on admission in the present study. Moreover, infection has been demonstrated to affect stroke outcome in several different mechanisms. For example, infection may accelerate the inflammatory cascade and exceed central nervous system immune response [24]. Moreover, MMP-9 levels were found to be increased by the presence of infection and then enhance the ischemia-induced degradation of collagen IV, which may lead to the disruption of BBB [25]. Additionally, infection has also been observed to increase platelet activation and platelet-leukocyte aggregation [26, 27]. Therefore, the presence of infected patient may contribute to the difference in the predictive values of the neutrophils on admission for poor outcome at 3 months.
Numerous studies have demonstrated that inflammation response plays an important role in the formation and progression of ischemic stroke. When ischemic stroke occurs, a large quantity of leukocytes infiltrate in peripheral blood immediately [28]. Each subtype of leukocytes has a specific inflammatory function and may contribute differentially to the process of ischemic stroke [29]. Among peripheral circulating leukocytes, neutrophils are recruited to the brain ischemic area in the early phase of inflammation [9]. Brain infiltrating neutrophils release free oxygen radicals and inflammatory mediators and cause ischemic tissue damage by cellular necrosis and apoptosis [30]. Moreover, neutrophils release cytokines, chemokines, and adhesion molecules, resulting in BBB disruption and hemorrhagic transformation [31]. So far, many studies suggested that the high neutrophils and NLR are associated with stroke severity, hemorrhagic transformation [22], infarct volume [32], mortality, and clinical function outcome [33]. However, most of these previous studies focused on the neutrophils on admission but not the dynamic change of neutrophils levels. The present study observed that a higher increase of neutrophils within 24 h is independently associated with hemorrhagic transformation in acute ischemic stroke patients after IV r-tPA. The mechanisms underlying by which increased neutrophils within 24 h compromises outcomes remain to be fully elucidated. Higher level of neutrophils within 24 h may indicate more active inflammation statue. In animal experiment, MMP-9-positive neutrophil infiltration has been shown to contribute to an increased risk of hemorrhage after r-tPA treatment in middle cerebral artery occlusion (MCAO) rat models [34]. McColl and colleagues found the beneficial effect of treatments of preventing neutrophil infiltration on reducing MMP-9 released in the brain [35]. Additionally, the infarct volume of transient brain ischemia is found to be reduced when the infiltration of neutrophil is inhibited [36]. Moreover, inhibition of neutrophils also could reduce the BBB disruption and the rate of HT in ischemic stroke [34, 37]. In humans, MMP-9-drived neutrophil infiltration has been found to contribute to the BBB breakdown, basal lamina type IV collagen degradation, and HT [11]. Neutrophils are regarded as one of the main sources of matrix metalloproteinase-9. When neutrophils enter into brain, it can release MMP-9 which may act on tight junction proteins and then disrupt the BBB from the luminal side of the vessel [38]. Therefore, the inflammation process may contribute to the PH after ischemic stroke.
The present study also demonstrated that high neutrophils at 24 h are associated with 3-month poor outcome. Compared with favorable clinical outcome group, neutrophil count in the poor outcome group was significantly higher. The mechanisms underlying the relationship between high neutrophil and poor functional outcomes remain to be elucidated. Neutrophil has been demonstrated to release chemokines and cytokines and other molecules in inflammation process. Neutrophil can also disrupt the BBB by releasing MMP-9 [39] and increase reactive oxygen and nitrogen species [40]. Moreover, previous studies showed that BBB disruption, cerebral edema, and hemorrhagic transformation after ischemic stroke are highly associated with poor outcome and contribute to the morbidity and mortality of ischemic stroke. Patients with a neutrophil increase > 50% had numerically higher OR compared with patients with a 25%< neutrophil increase ≤ 50% in our study, which indicate the greater the neutrophil elevation within 24 h, the higher the possibility of hemorrhagic transformation and poor prognosis. Based on these findings, inhibition of neutrophil or neutrophil infiltration may be a reasonable peripheral target for clinical treatment of stroke.
There is accumulating evidence supporting that NLR, which reflects systemic inflammation and the balance between neutrophils and lymphocytes, was regarded as a reliable biomarker in acute ischemic stroke [16]. Consistent with previous studies, the present study demonstrated that higher level of NLR may predict 3-month poor functional outcome in AIS patients. For example, NLR on admission and within 24 h was a predictor of 3-month outcome in patients with first-ever AIS [17, 18]. The present study also examined the predictive ability of lymphocyte on PH and outcome in AIS patients with the r-tPA treatment. Nevertheless, the present study failed to observe any significant links to lymphocyte and 3-month functional outcome. Therefore, more work will be required to identify the reasons. It is well-established that inflammation response in the process of ischemic stroke is complicated. In addition to neutrophils and lymphocytes, other indicators of inflammation such as leukocyte and C-reactive protein (CRP) are also dynamically altered in stroke patients after thrombolysis [41]. CRP level measured within 24 h after stroke has been reported to predict 1-year functional outcome [42]. An increase in CRP during the first 24 h was also strongly associated with lack of clinical improvement and poor outcome in patients treated with r-tPA [43]. Another study showed that changes in leukocytes levels 24 h after intravenous thrombolysis could predict the short-term functional outcome of AIS patients.
It needs to be mentioned that there are still some limitations. In the current study, we finally recruited only 208 patients, and further study such as the association between neutrophil with PH-1 and PH-2 could not be addressed, and we would carry on including the patients. Additionally, we only examined neutrophil at three time points, and more time points of the examination would help to understand more precise dynamic change of neutrophil following IV r-tPA. Moreover, more work is required to explore the association between neutrophil with infarct volume. Furthermore, more studies are needed to characterize the underlying molecular mechanisms by which the neutrophil and NLR predict the PH and outcome in AIS patients with r-tPA treatment.
Conclusion
In conclusion, our results suggest that the neutrophil is a dynamic variable following the r-tPA treatment of AIS. Dynamic increase in neutrophil after stroke significantly and reliably predicts PH and 3-month poor outcome in acute ischemic stroke patients receiving r-tPA treatment. In light of our findings, neutrophil level after r-tPA treatment may be regarded as an activity marker for PH and unfavorable prognosis in AIS patients with intravenous thrombolysis. Therefore, inhibition of neutrophil may serve as a reasonable peripheral target for clinical treatment of stroke.
Abbreviations
- PH:
-
Parenchymal hemorrhage
- HT:
-
Hemorrhagic transformation
- AIS:
-
Acute ischemic stroke
- NLR:
-
Neutrophil to lymphocyte ratio
- r-tPA:
-
Recombinant tissue plasminogen activator
- MMP-9:
-
Matrix metalloproteinase-9
- BBB:
-
Blood-brain barrier
- OTT:
-
Onset to treatment time
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- NIHSS:
-
National Institutes of Health Stroke Scale
- MRS:
-
Modified Rankin scale
- SD:
-
Standard deviation
- MCAO:
-
Middle cerebral artery occlusion
- CRP:
-
C-Reactive protein
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- IQR:
-
Interquartile ranges
- sICH:
-
Symptomatic intracerebral hemorrhages
References
Sacco RL, Kasner SE, Broderick JP et al (2013) An updated definition of stroke for the 21st century a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke -Dallas 44(7):2064–2089
Meschia JF, Bushnell C, Bodenalbala B et al (2014) Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 45(12):3754–3832
Group IC, Sandercock P, Wardlaw JM et al (2012) The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet. 379(9834):2352–2363
Hacke W, Kaste M, Bluhmki E et al (2008) Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med
Jickling GC, Liu D, Stamova B, Ander BP, Zhan X, Lu A, Sharp FR (2014) Hemorrhagic transformation after ischemic stroke in animals and humans. J Cereb Blood Flow Metab 34(2):185–199
Zhu W, Guo Z, Yu S, Leys D, Bordet R (2015) Higher neutrophil counts before thrombolysis for cerebral ischemia predict worse outcomes. Neurology 85(16):1408–1416
Guo Z, Yu S, Xiao L, Chen X, Ye R, Zheng P, Dai Q, Sun W, Zhou C, Wang S, Zhu W, Liu X (2016) Dynamic change of neutrophil to lymphocyte ratio and hemorrhagic transformation after thrombolysis in stroke. J Neuroinflammation 13(1):199
Kim JY, Park J, Ji YC, Kim SH, Lee JE. Inflammation after ischemic stroke: the role of leukocytes and glial cells. Exp Neurobiol. 2016. 25(5): 241-
Herz J, Sabellek P, Lane TE, Gunzer M, Hermann DM, Doeppner TR (2015) Role of neutrophils in exacerbation of brain injury after focal cerebral ischemia in hyperlipidemic mice. Stroke 46(10):2916–2925
Perez-De-Puig I, Miró-Mur F, Ferrer-Ferrer M et al (2015) Neutrophil recruitment to the brain in mouse and human ischemic stroke. Acta Neuropathol 129(2):239–257
Tokgoz S, Keskin S, Kayrak M, Seyithanoglu A, Ogmegul A (2014) Is neutrophil/lymphocyte ratio predict to short-term mortality in acute cerebral infarct independently from infarct volume. J Stroke Cerebrovasc Dis 23(8):2163–2168
Schwartz M, Moalem G (2001) Beneficial immune activity after CNS injury: prospects for vaccination. J Neuroimmunol 113(2):185–192
Fang YN, Tong MS, Sung PH et al (2017) Higher neutrophil counts and neutrophil-to-lymphocyte ratio predict prognostic outcomes in patients after non-atrial fibrillation-caused ischemic stroke. Biom J 40(3):154–162
Rosell A, Cuadrado E, Ortegaaznar A, Hernándezguillamon M, Lo EH, Montaner J (2008) MMP-9-positive neutrophil infiltration is associated to blood-brain barrier breakdown and basal lamina type IV collagen degradation during hemorrhagic transformation after human ischemic stroke. Stroke. 39(4):1121–1126
Mao Leilei,Li Peiying,Zhu Wen et al. Regulatory T cells ameliorate tissue plasminogen activator-induced brain haemorrhage after stroke.[J] .Brain, 2017, 140: 1914-1931
Xue J, Huang W, Chen X, Li Q, Cai Z, Yu T, Shao B (2017) Neutrophil-to-lymphocyte ratio is a prognostic marker in acute ischemic stroke. J Stroke Cerebrovasc Dis 26(3):650–657
Qun S, Tang Y, Sun J et al (2017) Neutrophil-to-lymphocyte ratio predicts 3-month outcome of acute ischemic stroke. Neurotox Res 31(3):1–9
Pektezel M Yasir,Yilmaz Ezgi,Arsava E Murat et al. Neutrophil-to-lymphocyte ratio and response to intravenous thrombolysis in patients with acute ischemic stroke.[J] .J Stroke Cerebrovasc Dis, 2019, 28: 1853–1859
Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T (1980) Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ 58(1):113–130
Jauch EC, Saver JL, Adams HP et al (2013) Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Circulation. 8(3):870–947
Churilov L, Arnup S, Johns H et al (2015) An improved method for simple, assumption-free ordinal analysis of the modified Rankin scale using generalized odds ratios. Int J Stroke 9(8):999–1005
Maestrini I, Strbian D, Gautier S, Haapaniemi E, Moulin S, Sairanen T, Dequatre-Ponchelle N, Sibolt G, Cordonnier C, Melkas S, Leys D, Tatlisumak T, Bordet R (2015) Higher neutrophil counts before thrombolysis for cerebral ischemia predict worse outcomes. Neurology. 85(16):1408–1416
Duan Z, Wang H, Wang Z, Hao Y, Zi W, Yang D, Zhou Z, Liu W, Lin M, Shi Z, Lv P, Wan Y, Xu G, Xiong Y, Zhu W, Liu X, ACTUAL Investigators (2018) Neutrophil-lymphocyte ratio predicts functional and safety outcomes after endovascular treatment for acute ischemic stroke. Cerebrovasc Dis 45(5–6):221–227
Raymond S, Connie W (2016) Ischemia, immunosuppression and infection—tackling the predicaments of post-stroke complications. Int J Mol Sci 17(1):551–556
Muhammad S, Haasbach E, Kotchourko M et al (2011) Influenza virus infection aggravates stroke outcome. Stroke 42(3):783
Mccoll BW, Allan SM, Rothwell NJ (2009) Systemic infection, inflammation and acute ischemic stroke. Neuroscience. 158(3):1049–1061
Zeller JA, Lenz A, Eschenfelder CC et al (2005) Platelet–leukocyte interaction and platelet activation in acute stroke with and without preceding infection. Arter Thromb Vas Biol 25(7):1519
Barone FC, Hillegass LM, Price WJ, White RF, Lee EV, Feuerstein GZ, Sarau HM, Clark RK, Griswold DE (1991) Polymorphonuclear leukocyte infiltration into cerebral focal ischemic tissue: myeloperoxidase activity assay and histologic verification. J Neurosci Res 29(3):336–345
Kim J, Song T, Park JH, Lee HS, Nam CM, Nam HS, Kim YD, Heo JH Different prognostic value of white blood cell subtypes in patients with acute cerebral infarction. Atherosclerosis. 2012. 222(2): 464–467
Matsuo Y, Kihara T, Ikeda M, Ninomiya M, Onodera H, Kogure K (1995) Role of neutrophils in radical production during ischemia and reperfusion of the rat brain: effect of neutrophil depletion on extracellular ascorbyl radical formation. J Cereb Blood Flow Metab 15(6):941–947
Dirnagl U (1999) Pathobiology of ischaemic stroke : an integrated view. Trends Neurosci 22(9):391–397
Buck BH, Liebeskind DS, Saver JL, Bang OY, Yun SW, Starkman S, Ali LK, Kim D, Villablanca JP, Salamon N, Razinia T, Ovbiagele B (2008) Early Neutrophilia is associated with volume of ischemic tissue in acute stroke. Stroke. 39(2):355–360
Shi J, Peng H, You S, Liu Y, Liu CF (2018) Increase in neutrophil after r-tPA thrombolysis predicts poor functional outcome of ischemic stroke: a longitudinal study. Eur J Neurol 25(4):687–e645
Gautier S, Ouk T, Tagzirt M et al (2014) Impact of the neutrophil response to granulocyte colony-stimulating factor on the risk of hemorrhage when used in combination with tissue plasminogen activator during the acute phase of experimental stroke. J Neuroinflammation 11(1):96
Mccoll BW, Rothwell NJ, Allan SM (2007) Systemic inflammatory stimulus potentiates the acute phase and CXC chemokine responses to experimental stroke and exacerbates brain damage via interleukin-1- and neutrophil-dependent mechanisms. J Neurosci 27(16):4403–4412
Garau A, Bertini R, Colotta F, Casilli F, Bigini P, Cagnotto A, Mennini T, Ghezzi P, Villa P (2005) Neuroprotection with the CXCL8 inhibitor repertaxin in transient brain ischemia. Cytokine. 30(3):125–131
Li Z, Zheng GZ, Rui LZ, Mei L, Chopp M (2003) Effects of a selective CD11b/CD18 antagonist and recombinant human tissue plasminogen activator treatment alone and in combination in a rat embolic model of stroke. Stroke 34(7):1790–1795
Harris AK, Ergul A, Kozak A, Machado LS, Johnson MH, Fagan SC (2005) Effect of neutrophil depletion on gelatinase expression, edema formation and hemorrhagic transformation after focal ischemic stroke. BMC Neurosci 6(1):49
Ludewig P, Sedlacik J, Gelderblom M, Bernreuther C, Korkusuz Y, Wagener C, Gerloff C, Fiehler J, Magnus T, Horst AK (2013) Carcinoembryonic antigen-related cell adhesion molecule 1 inhibits MMP-9-mediated blood-brain-barrier breakdown in a mouse model for ischemic stroke. Circ Res 113(8):1013–1022
Dziedzic T (2015) Systemic inflammation as a therapeutic target in acute ischemic stroke. Expert Rev Neurother 15(5):523–531
Tiainen M, Meretoja A, Strbian D, Suvanto J, Curtze S, Lindsberg PJ, Soinne L, Tatlisumak T, Helsinki Stroke Thrombolysis Registry Group (2013) Body temperature, blood infection parameters, and outcome of thrombolysis-treated ischemic stroke patients. Int J Stroke 8(8):632–638
Napoli MD, Papa F, Bocola V (2001) Prognostic influence of increased C-reactive protein and fibrinogen levels in ischemic stroke. Stroke. 32(1):133–138
Gill D, Sivakumaran P, Wilding P, Love M, Veltkamp R, Kar A (2016) Trends in C-reactive protein levels are associated with neurological change twenty-four hours after thrombolysis for acute ischemic stroke. J Stroke Cerebrovasc Dis 25(8):1966–1969
Funding
This study was supported by the National Natural Science Foundation of China (81673144).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethical approval
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ying, A., Cheng, Y., Lin, Y. et al. Dynamic increase in neutrophil levels predicts parenchymal hemorrhage and function outcome of ischemic stroke with r-tPA thrombolysis. Neurol Sci 41, 2215–2223 (2020). https://doi.org/10.1007/s10072-020-04324-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-020-04324-6