
Abstract
Objective
Repetitive Transcranial Magnetic Stimulation (rTMS) has been used to treat post-stroke upper limb spasticity (ULS) in addition to physiotherapy (PT). To determine whether rTMS associated with PT modulates cortical and spinal cord excitability as well as decreases ULS of post-stroke patients.
Methods
Twenty chronic patients were randomly assigned to either the intervention group-1 Hz rTMS on the unaffected hemisphere and PT, or control group-sham stimulation and PT, for ten sessions. Before and after sessions, ULS was measured using the modified Ashworth scale and cortical excitability using the output intensity of the magnetic stimulator (MSO). The spinal excitability was measured by the Hmax/Mmax ratio of the median nerve at baseline, at the end of treatment, and at the 4-week follow-up.
Results
The experimental group showed at the end of treatment an enhancement of cortical excitability, i.e., lower values of MSO, compared to control group (p = 0.044) and to baseline (p = 0.028). The experimental group showed a decreased spinal cord excitability at the 4-week follow-up compared to control group (p = 0.021). ULS decreased by the sixth session in the experimental group (p < 0.05).
Conclusion
One-hertz rTMS associated with PT increased the unaffected hemisphere excitability, decreased spinal excitability, and reduced post-stroke ULS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Upper limb spasticity (ULS) is an incapacitating post-stroke motor deficit since it significantly impacts activities of daily living due to functional loss, joint stiffness, and pain [1, 2]. The neurophysiological mechanisms for post-stroke ULS development are still poorly understood. Spasticity results of an increase in the excitability of the stretch reflex circuit which is regulated by excitatory and inhibitory descending signals of supra-spinal origin [3,4,5,6]. Since the motor cortex has an inhibitory control over spinal cord through the corticospinal tract [7, 8], it is acknowledged that cortical injuries could lead to loss of such control and an increase in spinal cord excitability, resulting in spasticity [9, 10]. Non-invasive brain stimulation therapies as repetitive transcranial magnetic stimulation (rTMS) could be used to increase the cortical excitability, resulting in a normalization of the motor cortex inhibitory control over spinal excitability [11, 12].
Previous studies have examined the efficacy of rTMS coupled with training in reducing ULS. Kakuda et al. [12] reported that 22 sessions of 1-Hz rTMS combined with occupational therapy reduced spasticity and improved motor function of stroke-affected upper limb. Similarly, Galvão et al. [13] noted a reduction of post-stroke ULS after ten sessions of 1-Hz rTMS coupled with physical therapy (PT). Conversely, Etoh et al. [14] showed no improvement of ULS after ten sessions of 1-Hz rTMS combined with 40 min of repetitive exercises. Additionally, despite a small improvement in upper limb measures, including spasticity, Rose et al. [15] concluded that 16 sessions of 1-Hz rTMS followed by 1 h of functional tasks did not lead to additional improvements in upper limb function of chronic stroke patients. Insights into how rTMS when combined with motor training acts on cortical and spinal excitability could be a key-factor for a successful implementation of rTMS as adjuvant therapy in neurorehabilitation.
Changes of the cortical and spinal activity that might underlie anti-spastic effects of rTMS are still poorly understood. To the best of our knowledge, only two studies [16, 17] have investigated the effects of 1-Hz rTMS over post-stroke spasticity through electrophysiological measures as Hmax/Mmax ratio (ratio between the maximum amplitude of the H-wave and the maximum amplitude of the M-wave). However, none of them coupled rTMS with training and both of them evaluated spasticity of lower limb.
Our study is rationally based on the theory of interhemispheric competition after stroke [18]. Healthy individuals have a balanced interaction between hemispheres. After a brain damage, this interaction becomes unequal due to a reduced activity of intracortical neuronal circuits of the affected hemisphere added to an excessive interhemispheric inhibition of the unaffected hemisphere. Considering such model, suppressing of the unaffected hemisphere excitability would reduce the interhemispheric inhibition and lead to an enhancement of descending inhibitory input through the corticospinal tract, followed by a decrease of the moto neuron excitability, resulting into a reduction of spasticity. We explored whether 1-Hz rTMS over the unaffected hemisphere of post-stroke patients associated with PT can modulate cortical as well as spinal cord excitability. In addition, the effects of such association over the ULS of patients was daily assessed during ten sessions.
Methods
Study design
A randomized, double-blind, sham-controlled trial with 4 weeks of follow-up was performed. Patients were randomly assigned into two groups: (i) experimental—rTMS and PT or (ii) control—sham rTMS and PT. A researcher not involved in the study performed the allocation sequence using a web-based computer software (www.randomization.com).
All patients and researchers who were involved in PT and evaluations were blinded to group allocations; only the researcher who administered rTMS was aware of the treatment group. This study was registered at ClinicalTrials.Gov (NCT01875536), was performed in accordance with the Declaration of Helsinki, and was approved by the local research ethics committee.
Participants
Participants were recruited through advertisements in a local newspaper, university website, and by screening outpatient clinics in local hospitals. Inclusion criteria were (i) ischemic/hemorrhagic stroke diagnosed by a neurologist and confirmed through CT or MRI, (ii) stroke onset ≥ 6 months and < 10 years, (iii) age between 40 and 75 years, (iv) wrist muscle tone score at modified Ashworth scale (MAS) [19] between 1 + and 2, and (v) absence of cognitive impairments, as determined by the Mini-Mental State Examination [20] (score > 20). Exclusion criteria were the following: (i) had clinical evidence of multiple brain lesions attested by physical examination and complementary imaging as CT or MRI, (ii) used antispastic drugs within the 6 months before enrollment, (iii) were pregnant, (iv) were using metallic implants or cardiac pacemakers, or (v) had a history of seizure or cerebral aneurysm. All patients gave written informed consent before starting the experiment.
Outcome measures
Interviews and clinical evaluations were carried out with all participants for collection of clinical data by an experienced blinded assessor.
Electrophysiological measures
Motor cortex excitability was determined by the intensity of the magnetic stimulator output (MSO), expressed as percentage of maximal stimulator output inducing motor-evoked potential (MEP) amplitude of 1 mV elicited by single-pulse TMS. TMS was performed using a magnetic stimulator (NEUROSOFT-Neuro-MS, Russian), connected to a 70-mm figure-8 coil positioned tangentially to the scalp at 45° from the midsagittal line over the primary motor cortex of the unaffected hemisphere. The coil was positioned at patient’s hotspot—the site where stimulation resulted consistently in the largest MEPs. Surface electromyography (EMG) recording was made from the first dorsal interosseous (FDI) muscle with Ag-AgCl surface electrodes. Responses were amplified and bandpass-filtered at 2 kHz. All data were digitized at an analog-to-digital rate of 5 kHz and further relayed into a laboratory computer using the Neuro-MEP-Micro software (Neurosoft Company, Russian). Motor cortex excitability was recorded at baseline and at each treatment session. Before each assessment, intensity was adjusted to elicit, on average, baseline MEPs of 1 mV peak-to-peak amplitude. The coil position was marked with a waterproof pen to guarantee identical position during the whole course of the study.
Excitability of the spinal cord was assessed through the variance in amplitude of the Hoffmann reflex (H-reflex). H-reflex measures excitability of motor neurons and that of the spinal cord indirectly and is used to evaluate spasticity [21]. H-reflex amplitude was normalized to the maximum muscle response using the Hmax/Mmax ratio. Conceptually, the Hmax/Mmax ratio reflects the proportion of motor neurons that are reflexly activated [22]. Hmax expresses the maximum amplitude, peak-to-peak, of the H-wave, and Mmax indicates that of the M-wave. Both indices were measured on the paretic side through peripheral electrical stimulation (rectangular pulses, 1-ms duration; frequency 0.2 Hz) of the median nerve and recorded by surface electromyography.
Electrodes were positioned as stated by Palmieri et al. [23]. Electromyographic data were collected at a sampling frequency of 2500 Hz, amplified, and bandpass-filtered (10–1000 Hz). H-reflex was measured at baseline, after ten treatment sessions (i.e., post-intervention) and at the 4-week follow-up.
Clinical measures
Before each session, Modified Ashworth scale (MAS) was recorded to determine spasticity of wrist flexor muscles in affected hand. This instrument is a 6-point scale that scores the average resistance to passive movements for each joint [24].
Interventions
Repetitive transcranial magnetic stimulation
rTMS of the motor cortex (1-Hz, 1500 pulses with an intensity of 90% of the rest motor threshold-MT [8]) was administered over the hotspot of FDI muscle of the unaffected hemisphere, three times per week—always before PT intervention—for a total of ten sessions. MT was defined as the lowest TMS intensity required to produce a MEP amplitude > 50 μV in at least six of ten trials. For each patient, coil position during rTMS sessions was defined by the place where MT was recorded.
In the sham rTMS, a coil disconnected from the stimulator was held over the scalp, while a second coil connected to the stimulator was positioned behind the patient’s head without touching the scalp. Patients were only exposed to acoustic stimulation and were not aware which of the coils were touching the scalp.
Physiotherapy
Thirty minutes of the PT program was applied immediately after stimulation with activities being adjusted according to patient’s functional capacity and focused primarily on upper limb rehabilitation. Specifically, the program had five objectives: (i) improve patient’s flexibility (stretching exercises of the flexors of wrist/fingers, biceps brachii, and pectoralis major and mobilization of the cervical muscles); (ii) improve strength (exercises of proprioceptive neuromuscular facilitation); (iii) improve coordination and balance; and (iv) improve patient’s mobility during transfers activities. All activities were based on recommendations of clinical practice guidelines for stroke patients [25].
Statistical analysis and data processing
Descriptive statistic was used to present demographic and clinical characteristics of participants. Groups were compared at baseline characteristics using an independent t test or chi-square test (χ2).
All data met the criterion for normal distribution (i.e., Kolmogorov-Smirnov test, p > 0.05). For cortical excitability, the MSO mean difference between each treatment session and first session was analyzed via repeated measures analysis of variance (rm-ANOVA), with Group (2 levels: experimental and control) as between-subjects factor, and Time (10 levels: from the first to the tenth session of treatment) as within-subjects factor. For spinal cord excitability, the difference in percentage of variance in the Hmax/Mmax ratio at post-intervention and at the 4-week follow-up was analyzed via rm-ANOVA, with Group (2 levels: experimental and control) as between-subjects factor, and Time (2 levels: post-intervention and 4-week follow-up) as within-subjects factor. Sphericity assumption was tested by Mauchly’s Test and adjustments were applied using a Greenhouse-Geisser correction. Pair-wise comparisons were performed for within- and between-subject analysis (Bonferroni corrections were applied).
To facilitate data analysis, MAS scores 1 +, 2, and 3 were assigned numerical values 2, 3, and 4, respectively. Since MAS data did not meet the criterion of normality, the difference in MAS scores between each treatment session and the first session was calculated and evaluated using Friedman test. Intra-group analysis was performed by Wilcoxon test, while comparisons between groups were analyzed by Mann-Whitney test. All analyses were performed using SPSS for Windows, Version 20 (Armonk, NY: IBM Corp). Statistical significance was set at p < 0.05.
Results
Participant characteristics and flow of the trial
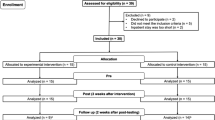
As shown in Fig. 1, out of a total of 148 patients who were screened for eligibility, 20 met study criteria and were randomized to the experimental (n = 10) and control group (n = 10). No difference was found between group at baseline (Table 1). No adverse events were reported by any of the participants.

Inclusion flow diagram
Electrophysiological measures
Figure 2 shows differences on cortical excitability; rm-ANOVA revealed an interaction effect between time and groups (F(9, 162) = 1.944; p = 0.049), while no significant main effect of time (F(9, 162) = 1.164; p = 0.33) and group (F(1, 18) = 3.212; p = 0.09) were found. Pair-wise comparisons using the Bonferroni corrections revealed a significant difference between groups at post-intervention (p = 0.044) pointing out to an enhancement of cortical excitability (i.e., lower values of MSO in the experimental group). MSO showed a decreased trend over the ten sessions in the experimental group. Pair-wise comparisons with Bonferroni corrections showed that this reduction was significant at the tenth session (p = 0.028).

Difference of output stimulator (%) between the first therapeutic session and each treatment session of experimental group (dashed line, circle) and control group (solid line, square). Data are shown as mean and standard error. *Represents significant difference between groups. Filled symbols represent significant difference from the first therapeutic session
Figure 3 shows differences in the spinal excitability measure throughout sessions. Two patients in each group were excluded from analysis due to poor reflex response. rm-ANOVA revealed a main group effect (F(1, 11) = 6088; p = 0.031). Bonferroni adjustment comparison showed significant difference on the Hmax/Mmax ratio between groups at 4-week follow-up (p = 0.021).

Variation (%) of Hmax/Mmax ratio from baseline in experimental group (dashed line, circle) and control group (solid line, square). Data are shown as mean and standard error. *Represents significant difference between groups
Clinical measure of spasticity
Figure 4 depicts changes in MAS scores throughout sessions. Friedman test revealed a significant difference in MAS scores between groups over time (χ2(9) = 24.35; p = 0.004). Pairwise comparisons with Wilcoxon signed-rank test showed a decrease of MAS scores from the third session (p < 0.05) when compared to baseline in the experimental group, pointing out to a decrease of spasticity. No significant difference was observed in the control group. Mann-Whitney test revealed differences between groups from the sixth session (p < 0.05).

Variation of Modified Ashworth scale score (MAS) from baseline of the first session before each therapeutic session in experimental group (dashed line, circle) and control group (solid line, square). Data are shown as mean and standard error. *Represents significant difference between groups. Filled symbols represent significant difference from the first therapeutic session
Discussion
To the best of our knowledge, this is the first double-blind RCT to investigate the effects of inhibitory rTMS coupled with PT on the cortical and spinal excitability, and as well as on the degree of ULS in stroke patients, for latter, tracking the effect daily during sessions. Our results suggest that rTMS coupled with PT decreases the level of ULS (beginning from the sixth treatment session) and the spinal cord excitability. Further, this association increases the cortical excitability in the unaffected hemisphere.
Effects of rTMS coupled with PT on cortical and spinal excitability
Based on the theory of interhemispheric competition [18], we have hypothesized that 1-Hz rTMS would decrease the excitability of unaffected motor cortex and restore the balance of transcallosal inhibitory circuits between the hemispheres, relieving the inhibition of the unaffected hemisphere and increasing the cortical activity of the affected hemisphere, as previously demonstrated [26]. However, we found that stimulation associated with PT increased the excitability of the unaffected hemisphere, as shown by the decrease of MSO in the experimental group. A possible explanation is that PT after effect interfered with prior inhibitory effect of 1-Hz rTMS reversing the suppressive effect of rTMS in facilitation. Supporting this view, studies in animals that have shown that physiological activity after induction of LTP/LTD can reduce, abolish, or reverse changes in synaptic plasticity [27,28,29]. This phenomenon has been also showed in human when two techniques of non-invasive brain stimulation were combined [30, 31]. Moreover, Huang et al. [32] have coupled inhibitory rTMS with motor training and observed that voluntary muscle contractions immediately after cortical stimulation increased the cortical excitability, reversing the suppressive effect of rTMS in facilitation.
Interestingly, increase in cortical excitability of the unaffected hemisphere was followed by decrease of Hmax/Mmax amplitude ration and spasticity. Indeed, the unaffected hemisphere seems to play a pivotal role in post-stroke rehabilitation [33]. In line with our results, earlier functional imaging studies have reported that an increased activity of the unaffected hemisphere might be related to the recovery of stroke patients [34, 35]. Also, Lotze et al. [36] reported that an inhibition of unaffected hemisphere areas can impair motor performance of the affected hand. Taken together, these findings suggest that the aim to strictly balance the interaction between hemispheres may be oversimplified [37]. Thus, other more complex models that take into account the lesion location and size, chronicity, and prior synaptic history should be investigated in order to advance in the developing of rTMS use as part of routine clinical practice.
Effects of rTMS coupled with PT on spasticity
Previously, we have shown that ten sessions of PT combined with inhibitory rTMS applied to the unaffected hemisphere are more effective than PT alone in reducing ULS in patients with chronic stroke [13]. Now, our results demonstrated that ULS significantly declines after the sixth session of treatment with rTMS and PT. This finding has an important clinical implication, suggesting that a minimum of six rTMS sessions are necessary in order to mitigate spasticity. Other studies have also reported antispastic effects of rTMS in neurological patients [38], but none has tracked the effects over time during treatment.
Since it is known that spasticity results from a hyperexcitability of the stretch reflex [39], we expected a reduction of spinal excitability along with MAS score decrease after treatment. Indeed, we noted such reduction throughout sessions only in the experimental group. Considering the decline in spasticity occurred from the sixth treatment session and a significant decrease of spinal excitability at follow-up, we suggest (i) the loss of muscular tone in response to passive stretching is not influenced merely by the decrease of the spinal excitability or (ii) the Hmax/Mmax ratio may lack clinical relevance when approaching spasticity. Indeed, the weak relationship between Hmax/Mmax ratio and clinical measurement for spasticity has been reported [40].
This study has some limitations. Firstly, some questions can be raised if an inclusion of patients with disease time ranging from 6 months to 10 years is not a time frame extremely wide. The time of development of paresis, as well as the amount of initial injury, can alter the final result of PT. Usually, better outcomes can be achieved when patients have high levels of adaptive neuroplasticity—such as at the first years after the stroke. Even though possible, the wide time frame used as inclusion criteria does not appear to have negatively impacted our results since 75% of patients (15 out of 20) had 5 years or less of disease. Additionally, age can be a key-factor for motor rehabilitation. Younger patients tend to respond in a better way than older ones. Once again, we used as inclusion criteria age between 40 and 75 years. It seems reasonable to assume that have in the same sample young and elderly patients could be a confounding factor, but 75% of our sample had 60 years or more. So, it can be assumed that they were more or less at the same motor capacity level.
Conclusion
We have demonstrated that 1-Hz rTMS over the unaffected motor cortex combined with PT decreased spinal cord excitability and ULS in chronic post-stroke patients. Besides evidence supporting the idea that rTMS combined with motor therapy may to be used in the management of spasticity, our study brings novel information on which manner this interaction occurs. This knowledge can be a key-factor for a successful implementation of rTMS as adjuvant therapy in stroke rehabilitation. Further studies with a larger number of patients may support the employment of rTMS in the PT arsenal.
Abbreviations
- rTMS:
-
repetitive transcranial magnetic stimulation
- ULS:
-
upper limb spasticity
- PT:
-
physical therapy
- MSO:
-
magnetic stimulator output
- CT:
-
computed tomography
- MRI:
-
magnetic resonance imaging
- MAS:
-
modified ashworth scale
- MEP:
-
motor-evoked potential
- MT:
-
motor threshold
- EMG:
-
electromyography
- H-reflex:
-
Hoffmann reflex
- Hmax:
-
maximum amplitude of the H-wave
- Mmax:
-
maximum amplitude of the M-wave
- FDI:
-
first dorsal interosseous
- RCT:
-
randomized clinical trial
- SPSS:
-
statistical package for social sciences
References
Harris JE, Eng JJ (2007) Paretic upper-limb strength best explains arm activity in people with stroke. Phys Ther 87(1):88–97
Cousins E, Ward AB, Roffe C, Rimington LD, Pandyan AD (2009) Quantitative measurement of poststroke spasticity and response to treatment with botulinum toxin: a 2-patient case report. Phys Ther 89(7):688–697
Burke D, Wissel J, Donnan GA (2013) Pathophysiology of spasticity in stroke. Neurology 80(3 Supplement 2):S20–S26
Barnes MP, Johnson GR (2008) Upper motor neurone syndrome and spasticity: clinical management and neurophysiology. Cambridge University Press
Gracies JM (2005) Pathophysiology of spastic paresis. II: emergence of muscle overactivity. Muscle Nerve 31(5):552–571
Priori AF, Cogiamanian F, Mrakic-Sposta S (2006) Pathophysiology of spasticity. Neurol Sci 27(4):307–309
Valero-Cabre A, Pascual-Leone A (2005) Impact of TMS on the primary motor cortex and associated spinal systems. IEEE Eng Med Biol Mag 24(1):29–35
Valle AC, Dionisio K, Pitskel NB, Pascual-Leone A, Orsati F, Ferreira MJ, Boggio PS, Lima MC, Rigonatti SP, Fregni F (2007) Low and high frequency repetitive transcranial magnetic stimulation for the treatment of spasticity. Dev Med Child Neurol 49(7):534–538
Goldstein EM (2001) Spasticity management: an overview. J Child Neurol 16(1):16–23
FAS V (1997) Alterações Centrais e Periféricas Após Lesão do Sistema Nervoso Central. Considerações e Implicações para a Fisioterapia. Braz J Phys Ther 2(1):19–34
Bolognini N, Vallar G, Casati C, Latif LA, El-Nazer R, Williams J, Banco E, Macea DD, Tesio L, Chessa C (2011) Neurophysiological and behavioral effects of tDCS combined with constraint-induced movement therapy in poststroke patients. Neurorehabil Neural Repair 25(9):819–829
Kakuda W, Abo M, Kobayashi K, Momosaki R, Yokoi A, Fukuda A, Ito H, Tominaga A, Umemori T, Kameda Y (2011) Anti-spastic effect of low-frequency rTMS applied with occupational therapy in post-stroke patients with upper limb hemiparesis. Brain Inj 25(5):496–502
Galvão SCB, dos Santos RBC, dos Santos PB, Cabral ME, Monte-Silva K (2014) Efficacy of coupling repetitive transcranial magnetic stimulation and physical therapy to reduce upper-limb spasticity in patients with stroke: a randomized controlled trial. Arch Phys Med Rehabil 95(2):222–229
Etoh S, Noma T, Ikeda K, Jonoshita Y, Ogata A, Matsumoto S, Shimodozono M, Kawahira K (2013) Effects of repetitive trascranial magnetic stimulation on repetitive facilitation exercises of the hemiplegic hand in chronic stroke patients. J Rehabil Med 45(9):843–847
Rose DK, Patten C, McGuirk TE, Lu X, Triggs WJ (2014) Does inhibitory repetitive transcranial magnetic stimulation augment functional task practice to improve arm recovery in chronic stroke? Stroke Res Treat 2014:305236
Rastgoo M, Naghdi S, Nakhostin Ansari N, Olyaei G, Jalaei S, Forogh B, Najari H (2016) Effects of repetitive transcranial magnetic stimulation on lower extremity spasticity and motor function in stroke patients. Disabil Rehabil 38(19):1918–1926
Naghdi S, Ansari NN, Rastgoo M, Forogh B, Jalaie S, Olyaei G (2015) A pilot study on the effects of low frequency repetitive transcranial magnetic stimulation on lower extremity spasticity and motor neuron excitability in patients after stroke. J Bodyw Mov Ther 19(4):616–623
Takeuchi N, Izumi S-I (2012) Maladaptive plasticity for motor recovery after stroke: mechanisms and approaches. Neural Plast 2012(2012):1–9
Bohannon RW, Larkin PA, Smith MB, Horton MG (1987) Relationship between static muscle strength deficits and spasticity in stroke patients with hemiparesis. Phys Ther 67(7):1068–1071
Brucki SM, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH (2003) Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr 61:777–781
Bakheit A, Maynard V, Curnow J, Hudson N, Kodapala S (2003) The relation between Ashworth scale scores and the excitability of the α motor neurones in patients with post-stroke muscle spasticity. J Neurol Neurosurg Psychiatry 74(5):646–648
Pinelli P, Di Lorenzo G (1989) Electromyographic assessment of spasticity. In: Electromyographic assessment of spasticity. Springer
Palmieri RM, Ingersoll CD, Hoffman MA (2004) The Hoffmann reflex: methodologic considerations and applications for use in sports medicine and athletic training research. J Athl Train 39, 268(3)
Charalambous CP (2014) Interrater reliability of a modified Ashworth scale of muscle spasticity. In: Classic papers in orthopaedics. Springer, pp 415–417
Van Peppen RP, Kwakkel G, Wood-Dauphinee S, Hendriks HJ, Van der Wees PJ, Dekker J (2004) The impact of physical therapy on functional outcomes after stroke: what’s the evidence? Clin Rehabil 18(8):833–862
Takeuchi N, Chuma T, Matsuo Y, Watanabe I, Ikoma K (2005) Repetitive transcranial magnetic stimulation of contralesional primary motor cortex improves hand function after stroke. Stroke 36(12):2681–2686
Zhou Q, Tao HW, Poo MM (2003) Reversal and stabilization of synaptic modifications in a developing visual system. Science 300(5627):1953–1957
Xu L, Anwyl R, Rowan MJ (1998) Spatial exploration induces a persistent reversal of long-term potentiation in rat hippocampus. 394(6696):891
Manahan-Vaughan D, Braunewell KH (1999) Novelty acquisition is associated with induction of hippocampal long-term depresssion. Proc Natl Acad Sci U S A 96(15):8739–8744
Fricke K, Seeber AA, Thirugnanasambandam N, Paulus W, Nitsche MA, Rothwell JC (2011) Time course of the induction of homeostatic plasticity generated by repeated transcranial direct current stimulation of the human motor cortex. J Neurophysiol 105(3):1141–1149
Cosentino G, Fierro B, Paladino P, Talamanca S, Vigneri S, Palermo A, Giglia G, Brighina F (2012) Transcranial direct current stimulation preconditioning modulates the effect of high-frequency repetitive transcranial magnetic stimulation in the human motor cortex. Eur J Neurosci 35(1):119–124
Huang Y-Z, Rothwell JC, Edwards MJ, Chen R-S (2008) Effect of physiological activity on an NMDA-dependent form of cortical plasticity in human. Cereb Cortex 18(3):563–570
Bütefisch C (2006) Neurobiological bases of rehabilitation. Neurol Sci 27(1):18–23
Riecker A, Gröschel K, Ackermann H, Schnaudigel S, Kassubek J, Kastrup A (2010) The role of the unaffected hemisphere in motor recovery after stroke. Hum Brain Mapp 31(7):1017–1029
Schaechter JD, Perdue KL, Wang R (2008) Structural damage to the corticospinal tract correlates with bilateral sensorimotor cortex reorganization in stroke patients. Neuroimage 39(3):1370–1382
Lotze M, Markert J, Sauseng P, Hoppe J, Plewnia C, Gerloff C (2006) The role of multiple contralesional motor areas for complex hand movements after internal capsular lesion. J Neurosci 26(22):6096–6102
Di Pino G, Pellegrino G, Assenza G, Capone F, Ferreri F et al (2014) Modulation of brain plasticity in stroke: a novel model for neurorehabuilitation. Nat Rev Neurol 10(10):597–608
Gunduz A, Kumru H, Pascual-Leone A (2014) Outcomes in spasticity after repetitive transcranial magnetic and transcranial direct current stimulations. Neural Regen Res 9, 712(7)
Mukherjee A, Chakravarty A (2010) Spasticity mechanisms–for the clinician. Front Neurol 1
Levin MF, Hui-Chan C (1993) Are H and stretch reflexes in hemiparesis reproducible and correlated with spasticity? J Neurol 240(2):63–71
Funding
KMS is supported by CNPQ-Brazil (grant number 308291/2015-8) and the research was supported by grant (number APQ-0357-4.08/13) from Fundação de Amparo a Ciência e Tecnologia do Estado de Pernambuco (FACEPE)-Recife-Brazil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
dos Santos, R.B.C., Galvão, S.C.B., Frederico, L.M.P. et al. Cortical and spinal excitability changes after repetitive transcranial magnetic stimulation combined to physiotherapy in stroke spastic patients. Neurol Sci 40, 1199–1207 (2019). https://doi.org/10.1007/s10072-019-03765-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-019-03765-y