
Abstract
Cerebral venous thrombosis (CVT) usually accounts for < 1% of all strokes. Global disparity and diversity in their demographics, etiology, clinical features, radiological presentation, and mortality have not been previously explored. A systematic search was performed for publications in PubMed using key words “cerebral venous thrombosis,” “Cerebral vein thrombosis,” and “Cortical vein Thrombosis.” A total of 600 relevant studies were abstracted with strict selection criteria, and a total of 7048 patient’s data were used for the final analysis. The frequency and relative frequency statistics were used to describe the data. Cases reported were Europe-3152, Asia-2722, North America-852, Africa-122, Australia-121, and South America-79. Overall male to female ratio was 1:2.2; among clinical characteristics, headache was the most common symptom and hematological factors were the most common etiology. Location of the thrombosis was described mostly in the transverse sinus. Intercontinental differences in relation to demographics, etiology, clinical features, radiological presentation, and mortality were identified. CVT can have significant disparity in their demographics, etiology, clinical features, radiological presentation, and mortality when compared from one continent to other. It is important for the worldwide physicians to recognize these differences and to follow the most recent guidelines, diagnostic methods, and treatment to insure the best outcome and prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background and objectives
Cerebral venous and sinus thrombosis (CVT) is a rare disease which accounts for < 1% of all strokes and usually affects adults at a young age in their third decade [1]. This disease has a wide variety of clinical symptoms which delays its diagnosis. Incidence of various presentation has been reported in the literature with headache as the most reported symptom [2]. The headache could be of an acute onset and indistinguishable from a thunderclap headache seen in subarachnoid hemorrhage [3, 4]. Other frequent CVT presentations include seizures (focal or generalized) which is seen more with CVT than in arterial stroke [2] and focal neurological deficits. If any of these presentations are coupled with headache, then CVT is becoming on the differential diagnosis [5].
There is a large number of conditions that are known for causing or predisposing CVT. International Study on Cerebral Venous Thrombosis (ISCVT) reported at least one identifiable risk factor in about 85% of their population and multiple risk factors in about 50% [2].
Neuroimaging advancement facilitated significantly in making and confirming the diagnosis of CVT [6,7,8]. Noninvasive methods like computed tomography venography (CTV) and magnetic resonance venography (MRV) are usually for performed first, while invasive direct cerebral venography is rarely required at present and usually reserved if the diagnosis of CVT is still doubtful. The treatment of CVT includes the use of anticoagulation, symptomatic treatment of intracranial hypertension, headache, seizure, focal neurological deficits, visual deficit, any other complications, and the treatment for the potential etiology.
There are only few epidemiological studies in the literature on the prevalence of CVT in different parts of the world [2, 9,10,11,12,13,14] of which the ISCVT has the largest cohort with 624 cases. Most of these studies analyzed a specific population in a specific geographical area. The literature is lacking on a large-scale analysis of CVT characteristics in patients from all over the world. The purpose of this paper is to highlight the differences of CVT between the different continents to aid medical care providers to recognize this disease faster in different parts of the globe.
Methods
We systematically searched PubMed for publication between 1966 and 2014 with a wide number of keywords such as “Cerebral venous thrombosis,” “Cerebral vein thrombosis,” and “Cortical vein Thrombosis.” The search strategy was developed in accordance with professional librarian instructions. We initially applied a language restriction to include only papers in English and studies were reviewed to check whether they contained information about human subjects. Altogether, we identified about 1100 potential articles using our initial search strategy. Then, we excluded articles after screening for duplicates, pediatrics of less than 18 years old, animal models, editorials, letters, short communications, and correspondence which did not have any patient information about demographics, presentation, diagnostics method, etiology, CVT location, treatment, and outcome. We included patients who were objectively confirmed to have CVT by accepted imaging methods (computed tomographic-venography, magnetic resonance imaging with magnetic resonance-venography, or conventional angiography). Finally, we retrieved 600 articles in full-text for detailed evaluation and verification in our systematic review with a total of 7048 patients. The number breakdown is as follows: case series with a total of 4978 patients (1535 males and 3443 females) and case reports with a total of 2070 patients (629 males and 1441 females).
We categorized the cases geographically, based on the population studied, into six continents: North America, South America, Europe, Africa, Asia, and Australia. We reviewed all the data to get CVT male/female ratio, presentation, diagnostic methods used, etiology, CVT location, therapeutic approach used, and eventually the outcome.
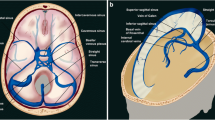
We categorized presenting symptoms into the following: headache, focal neurological deficits, seizures, systemic symptoms, visual deficits, and altered metal status. Etiologies were categorized into the following: systemic, hematological, hormonal, postpartum, malignancy, CNS, idiopathic, surgical, and miscellaneous (further description is provided in the supplementary material). Locations of CVT were categorized into the following: transverse-sigmoid-internal jugular (TSI) veins (as one category as most clots extend from one of these locations to the other), superior sagittal sinus (SSS), inferior sagittal sinus-straight sinus-vein of galen (ISS-SS-VOG), cavernous sinus, superficial and deep cortical, and internal cerebral veins. We looked at the use of Computerized Tomography (CT), Magnetic resonance imaging (MRI), and cerebral angiography for verifying the diagnosis. We categorized management of CVT into the following: anticoagulation, antiplatelet, antibiotics, lumbar puncture, steroids, shunting, and thrombolytic therapy. Outcome was categorized into the following: good (patients achieving complete recovery or very mild disability), moderate (patients with moderate disability), and poor (patients with severe disability or death).
We used descriptive statistics (frequency and relative frequencies) to report our findings. All statistics on male to female ratio, most common etiologies, most common presentations, most frequent location of CVT, most frequently used diagnostic method, and most commonly used therapeutic approach were stratified by continent.
Results
Out of the 7048 reported cases with CVT in the literature, 3152 were from Europe followed by 2722 from Asia and 852 from North America (Table 1). Overall male to female ratio was 1:2.2.
Africa
Africa had 122 reported patients in the literature of whom male to female ratio was 1: 5.1 which is higher than the reported overall average. Headache was the most common presenting symptom followed by focal neurological deficit and seizures (Table 2). The most common etiology was hematological, followed by systemic and postpartum etiologies (Table 3). MRI was the most used method diagnosing most CVT whereas cerebral angiography was used in 16% of the reported cases to make the diagnosis (Table 4). CVT was most commonly reported in the TSI veins, followed by the SSS (Table 5). Anticoagulation was the method of choice for treating CVT cases while the use of thrombolysis or shunting was not reported in any of these patients (Table 6). Good outcome was reported in 68%, while unfavorable outcome was reported in 29% of the patients (Table 7).
Asia
Asia had 2722 reported patients in the literature of whom male to female ratio was 1: 1.7. Headache was the most common presenting symptoms followed by focal neurological deficits and visual deficits (Table 2). Hematological etiologies were the most common followed by postpartum and systemic etiologies (Table 3). MRI was the most used method diagnosing most CVT whereas cerebral angiography was used in 17% of the reported cases to make the diagnosis (Table 4). CVT were most commonly reported in the SSS, followed by TSI veins. Anticoagulation was used in 77% of the cases while 2% underwent thrombolytic therapy; none of the patients had shunting as part of their management (Table 6). Good outcome was reported in 45% of the cases, while 46% had unfavorable outcome (Table 7).
Australia
Australia had 121 reported patients in the literature of whom male to female ratio was 1:2.5; the most common presentation was focal neurological deficits followed by headache and seizures (Table 2). Systemic etiologies were the most commonly reported, followed by hormonal and CNS etiologies (Table 3). MRI was the most used method diagnosing most CVT whereas cerebral angiography was used in 4% of the reported cases to make the diagnosis (Table 4). CVT was most commonly reported at the TSI veins, followed by the SSS. Anticoagulation was used in 92% of the cases while 8% underwent thrombolytic therapy; none of the patients had shunting as part of their management (Table 6). Good outcome was reported in 68%, while 26% had unfavorable outcome (Table 7).
Europe
Europe had 3152 reported patients in the literature of whom male to female ratio was 1:2.6; the most common presentation was headache, followed by focal neurological deficits and visual deficits (Table 2). Systemic etiologies were most commonly reported, followed by hormonal and hematological etiologies (Table 3). MRI was the most used method diagnosing most CVT whereas cerebral angiography was used in 12% of the reported cases to make the diagnosis (Table 4). CVT was most commonly reported at the TSI veins followed by the SSS. Anticoagulation was used in 81% of the cases while 3% underwent thrombolytic therapy and 1% underwent shunting (Table 6). Good outcome was reported in 52%, while 42% had unfavorable outcome (Table 7).
North America
North America had 852 patients reported in the literature of whom male to female ratio was 1:2.7. The most common presentation was headache, followed by focal neurological deficit and seizures (Table 2). Systemic etiologies were the most common followed by hormonal and hematological etiologies (Table 3). MRI was the most used method diagnosing most CVT whereas cerebral angiography was used in 13% of the reported cases to make the diagnosis (Table 4). CVT was equally reported at the SSS and the TSI veins as the most common location. Anticoagulation was used in 85% of the cases while 5% underwent thrombolytic therapy and 1% underwent shunting (Table 6). Good outcome was reported in 55%, while 30% had unfavorable outcome (Table 7).
South America
South America had 79 reported patients in the literature of whom male to female ratio was 1:1.1; the most common presentation was headache, followed by visual deficits and focal neurological deficits (Table 2). Hematological etiologies were most commonly reported, followed by hormonal and systemic etiologies (Table 3). MRI was the most used method diagnosing most CVT whereas cerebral angiography was used in 3% of the reported cases to make the diagnosis (Table 4). CVT was commonly reported in the TSI veins, followed by cortical veins. Anticoagulation was used in 57% of the cases while 1% underwent thrombolytic therapy and 1% underwent shunting (Table 6). Good outcome was reported in 60% of the patients, while 37% had unfavorable outcome (Table 7).
Discussion
Multiple national and hospital-based studies and reports have been published about CVT epidemiology and characteristics in different countries [2, 9,10,11,12,13], but to our best knowledge, none has gathered a large set of data that was reported in the literature to provide an overview and comparison about this disease characteristics based on the geographical area. Most physicians around the world base their experience with this disease on what is reported in the western literature without having enough data and publication to highlight the differences at their particular part of the world.
We were able to gather data for 7048 patients from all over the world, some continents had limited number of published data about CVT compared to other continents like Asia and Europe. We were able to identify multiple differences in these disease characteristics that would help physician to be able to identify this disease earlier to improve patients’ outcome.
Regarding male/female ratio, the overall ratio was 1:2.2 which is close to what the ISCVT reported [2], though we noticed that Africa had the highest ratio at 1:5.1 compared to the South America, and on the other hand, South America had the lowest ratio at 1:1.1. Among all CVT presenting symptoms, headache was the most commonly reported by the ISCVT [2], which held true across all continents as the most common presentation symptom with the exception in Australia where focal neurological deficits were the most common presentation. About two thirds of all presenting symptoms were headache, focal neurological deficits, seizures, and visual deficits.
At least one risk factor was reported in more than 85% of patients in the ISCVT, among which oral contraceptive use, prothrombotic conditions, and postpartum were the most frequently reported at 54, 34, and 14%, respectively [2]. We noticed different findings, such that hematological etiologies were the most common ones in Africa, Asia, and South America, while systemic etiologies were the most common ones in Australia, Europe, and North America. We also noticed that hormonal etiology was only common in Australia, Europe, and North America which might be attributed to the widespread use of oral contraceptives in these continents compared to the other ones.
MRI/MRV was the method used to ascertain the diagnosis in about half of the patients across all continents, except for Australia where the vast majority of cases were diagnosed via the use of MRI/MRV. CT/CTV was the second most common way of making the diagnosis, while the use of conventional angiography ranged from 3% in South America to 38% in Asia. After a lengthy search, we were not able to find articles to report the most frequently involved sinuses in CVT. We found, however, in our report that the TSI veins were the most common location for CVT in all continents, except in Asia where the SSS was the most common location. Cortical vein thrombosis was overall an uncommon location except in South America where 17% of the reported cases had CVT there.
The European Federation of Neurological Societies and the American Heart Association recommend the use of anticoagulation for CVT in patients without contraindications [15, 16]. The use of anticoagulation in different parts of the world was not previously reported; in this report, we found that it varied between the continents and was surprisingly low in South America at 57%. The use of direct thrombolysis varied between the continents, and the use of shunting was only reports from Europe, North, and South America.
Several prospective series [2, 17,18,19] have reported the prognosis of patients with CVT in which the overall rate of poor outcome (severe disability or death) at the end of follow-up in these studies was about 15%. In our analysis, we found that poor outcome was higher than 15% across all continents. Poor outcome was reported highest in Asia and Europe at 46 and 42%, respectively. This difference is mostly related to the nature of our data which included retrospective analysis, case series, and individual case reports for complicated patients. Best outcome on the other hand was reported in Australia at 68% of the patients.
Our analysis is limited by the nature of meta-analysis studies, and the limited number of reports in some continents compared to others that led to the inclusion of all available case series and individual case reports. Ideally, a multinational prospective study that includes sites from all over the world would be a better way to assess CVT characteristics and differences more accurately.
Our main goal from this paper was to highlight the key similarities and differences for the same disease in different areas of the world, as the biggest prospective cohort (ISCVT) participants’ sites were mainly in Europe and South America. We hope that this analysis will be a help for physicians all over the world to better understand and recognize CVT in their own area to achieve the best outcomes possible.
References
Stam J (2005 Apr 28) Thrombosis of the cerebral veins and sinuses. N Engl J Med 352(17):1791–1798
Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F (2004) Prognosis of cerebral vein and dural sinus thrombosis. Stroke 35(3):664–670
Sztajzel R, Coeytaux A, Dehdashti AR, Delavelle J, Sinnreich M (2001) Subarachnoid hemorrhage: a rare presentation of cerebral venous thrombosis. Headache: J Head Face Pain 41(9):889–892
Oppenheim C, Domigo V, Gauvrit JY, Lamy C, Mackowiak-Cordoliani MA, Pruvo JP, Méder JF (2005) Subarachnoid hemorrhage as the initial presentation of dural sinus thrombosis. Am J Neuroradiol 26(3):614–617
Jacobs K, Moulin T, Bogousslavsky J, Woimant F, Dehaene I, Tatu L, Besson G, Assouline E, Casselman J (1996) The stroke syndrome of cortical vein thrombosis. Neurology 47(2):376–382
Ford K, Sarwar M (1981) Computed tomography of dural sinus thrombosis. Am J Neuroradiol 2(6):539–543
Tsai FY, Wang AM, Matovich VB, Lavin M, Berberian B, Simonson TM, Yuh WT (1995) MR staging of acute dural sinus thrombosis: correlation with venous pressure measurements and implications for treatment and prognosis. Am J Neuroradiol 16(5):1021–1029
Lee SK (2003) Cerebral venous thrombosis in adults: the role of imaging evaluation and management. Neuroimaging Clinics 13(1):139–152
Kalbag RM, Woolf AL (1967) Cerebral venous thrombosis: with special reference to primary aseptic thrombosis. Oxford University Press
Bienfait HP, van Duinen S, Tans JT (2003) Latent cerebral venous and sinus thrombosis. J Neurol 250(4):436–439
Ferro JM, Correia M, Pontes C, Baptista MV, Pita F (2001) Cerebral vein and dural sinus thrombosis in Portugal: 1980–1998. Cerebrovasc Dis 11(3):177–182
deVeber G, Andrew M, Adams C, Bjornson B, Booth F, Buckley DJ, Camfield CS, David M, Humphreys P, Langevin P, MacDonald EA (2001) Cerebral sinovenous thrombosis in children. N Engl J Med 345(6):417–423
Coutinho JM, Zuurbier SM, Aramideh M, Stam J (2012) The incidence of cerebral venous thrombosis. Stroke 43(12):3375–3377
Lanska DJ, Kryscio RJ (2000) Risk factors for peripartum and postpartum stroke and intracranial venous thrombosis. Stroke 31(6):1274–1282
Saposnik G, Barinagarrementeria F, Brown RD, Bushnell CD, Cucchiara B, Cushman M, Ferro JM, Tsai FY. Diagnosis and management of cerebral venous thrombosis. Stroke. 2011 :STR-0b013e31820a8364
Einhäupl K, Stam J, Bousser MG, De Bruijn SF, Ferro JM, Martinelli I, Masuhr F (2010) EFNS guideline on the treatment of cerebral venous and sinus thrombosis in adult patients. Eur J Neurol 17(10):1229–1235
Ferro JM, Lopes MG, Rosas MJ, Ferro MA, Fontes J (2002) Long-term prognosis of cerebral vein and dural sinus thrombosis. Cerebrovasc Dis 13(4):272–278
Canhão P, Ferro JM, Lindgren AG, Bousser MG, Stam J, Barinagarrementeria F (2005) Causes and predictors of death in cerebral venous thrombosis. Stroke 36(8):1720–1725
Haghighi AB, Edgell RC, Cruz-Flores S, Feen E, Piriyawat P, Vora N, Callison RC, Alshekhlee A (2012) Mortality of cerebral venous–sinus thrombosis in a large national sample. Stroke 43(1):262–264
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This submission complies with the journal’s ethical responsibilities for the authors.
Conflict of interest
The the authors declare that they have no conflict of interest.
Statement of human rights and informed consent
For this type of study, formal consent is not required
Additional information
This paper has been accepted as a presentation in the 14th Annual meeting of the Neurocritical Care Society.
Electronic supplementary material
A supplementary material is provided that includes more frequencies for all presenting symptoms, etiologies, diagnostic methods, CVT location, management and outcomes. A detailed description of some of the categories in presentation and etiology also included.
ESM 1
(DOCX 25 kb).
Rights and permissions
About this article

Cite this article
Maali, L., Khan, S., Qeadan, F. et al. Cerebral venous thrombosis: continental disparities. Neurol Sci 38, 1963–1968 (2017). https://doi.org/10.1007/s10072-017-3082-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-017-3082-7